
Abstract
Diabetic foot ulcers (DFUs) impact a substantial proportion of patients with diabetes, with high recurrence rates, severe complications, and significant financial burden to health care systems. Adherence to treatment advice (e.g., limiting weight-bearing activity) is low with patients reporting dissatisfaction with the way in which advice is communicated. This study aimed to address this problem via the systematic development of a motivation communication training program. The program was designed to support diabetes-specialist podiatrists in empowering patients to actively engage with treatment. The development process followed an intervention mapping approach. Needs assessment involved observations of 24 patient–practitioner consultations within a diabetes-specialist foot clinic. This informed specification of a theory of change (self-determination theory) and relevant evidence-based communication strategies (drawing from motivational interviewing). The training program was developed iteratively with changes made following feedback from five diabetic foot health care professionals. The resulting training program, consisting of six one-hour face-to-face sessions over an 8-week period, was delivered to a further six diabetes specialist podiatrists, with five participating in postprogram telephone interviews to assess acceptability. Deductive thematic analysis of interview data revealed positive aspects of the training (e.g., valuable and relevant content), ideas for improvement (e.g., online resources and context-specific video examples), the acceptability of motivation strategies, and challenges putting the strategies into practice (such as time constraints and breaking old communication habits). This study contributes to our understanding of integrating motivation principles into routine consultations and holds potential for enhancing adherence to treatment recommendations in patients living with diabetic foot ulcers.
Background
Diabetic Foot Ulcers (DFUs) are a serious complication of diabetes that can lead to lower extremity amputation and premature mortality (Jupiter et al., 2016). The condition is associated with high health care costs (Cavanagh et al., 2012; Kerr et al., 2019) and has severe implications for patients’ health-related quality of life (Khunkaew et al., 2019). Patients with DFUs often experience limited physical and social functioning and nearly half are reported to experience depression (Jiang et al., 2020).
Patient adherence to treatment advice in the management of DFUs has been reported to be consistently low (Armstrong et al., 2003; Bus et al., 2016; Bus & Van Netten, 2016; Tanharo et al., 2018). Adherence to self-care behaviors (e.g., appropriate wound dressing, limiting weight-bearing activity, and wearing therapeutic footwear) is crucial in preventing and healing ulcers, with those not adhering presenting with higher rates of ulceration (Bus & Van Netten, 2016). Thus, interventions targeting patient adherence in this population are needed (International Working Group of the Diabetic Foot, 2019).
A key factor influencing patient adherence is the communication style of health care practitioners (Zolnierek & DiMatteo, 2009). Coffey et al. (2019) conducted a qualitative meta-synthesis focusing on the experiences of patients with DFUs. The results revealed that patients were dissatisfied with the way footcare advice was communicated to them. Patients reported inconsistencies in the advice they received, a lack of rapport and emotional support, and a general lack of understanding regarding how DFUs impacted their daily lives (Coffey et al., 2019). Similarly, a study by Searle et al. (2008) found one-third of interviewed patients felt they were not actively involved in decision-making during consultations and were hesitant to ask questions. Furthermore, Searle and colleagues (2008) interviewed podiatrists who expressed frustration and lack of support in their efforts to empower and establish collaborative partnerships with their patients. More recent research conducted by Hancox et al. (2023) interviewed patients regarding delivery of treatment advice specifically in relation to limiting weight-bearing activity. Patients reported that often treatment advice is delivered in a directive and generic manner and expressed a preference for a more person-centered approach with advice tailored to their specific needs via a process of collaborative problem-solving. Consequently, there is a pressing need for interventions to support health professionals in communicating with patients in a way that empowers them to actively participate in their treatment and adhere to recommendations.
Self-determination theory (SDT; Deci & Ryan, 1985; Ryan & Deci, 2017) is a framework that can be used to understand how the communication style of health care practitioners influences patient adherence to health behaviors. Central to SDT is the notion that satisfaction of individuals’ basic psychological needs for autonomy (choice and volition), competence (ability to perform the desired behavior), and relatedness (sense of belonging) fosters optimal motivation (Deci & Ryan, 2000). Individuals may be motivated to engage in health behaviors for more autonomous reasons (e.g., enjoyment, valuing benefits) or controlled reasons (avoiding letting oneself down or pressure from significant others) (Deci & Ryan, 2000). Some individuals may be amotivated (a lack of motivation) and have no intention of engaging. Increases in need satisfaction and autonomous motivation (but not controlled or amotivation) have been found to be associated with positive changes in health behavior (Ntoumanis et al., 2021) and long-term behavior change (Ng et al., 2012).
The communication style adopted by significant others (e.g., health care professionals) can influence the extent to which individuals’ basic psychological needs are satisfied, and in turn, the type of motivation underpinning engagement. An autonomy-supportive communication style (characterized by offering choice, rationale, and empathy) has been found to satisfy individuals’ basic psychological needs, promote more self-determined motivations, and be effective at increasing adherence to a variety of health-related behaviors: physical activity, tobacco cessation, medication adherence, and dental hygiene (Ng et al., 2012). Despite the potential for supporting adherence, no research has applied SDT in the context of DFUs.
Motivational interviewing (MI) is “a collaborative conversation style for strengthening a person’s own motivation and commitment to change” (Miller & Rollnick, 2012, p.12). MI interventions outperform traditional patient education methods where behavior change or adherence is the desired outcome for various health behaviors (Rubak et al., 2005).
MI and SDT are viewed as complementary approaches, with SDT serving as a theoretical framework for understanding how and why MI techniques facilitate behavior change (Deci & Ryan, 2012; Markland et al., 2005; Patrick & Williams, 2012; Vansteenkiste & Sheldon, 2006). Phillips and Guarnaccia (2020) conducted a systematic review of SDT- and/or MI-based interventions for prevention and treatment of type 2 diabetes. The authors identified 23 type 2 diabetes interventions (3 SDT-based, 20 MI-based), none of which focused on diabetes-specialist podiatrists. The effectiveness of the interventions was mixed, primarily due to variations in the quality of study design, methods, and treatment fidelity. To address these limitations, Phillips and Guarnaccia (2020) recommend the integration of the strong theoretical foundation of SDT with MI’s practice-orientated manuals and tools for assessing treatment integrity.
The purpose of this study, therefore, was to describe the development and acceptability of an SDT and MI-informed motivation communication training program for health care professionals (i.e., podiatrists) focused on facilitating discussions around motivation and adherence to treatment recommendations in patients with DFUs.
Methods and Results
Intervention Design Methodology
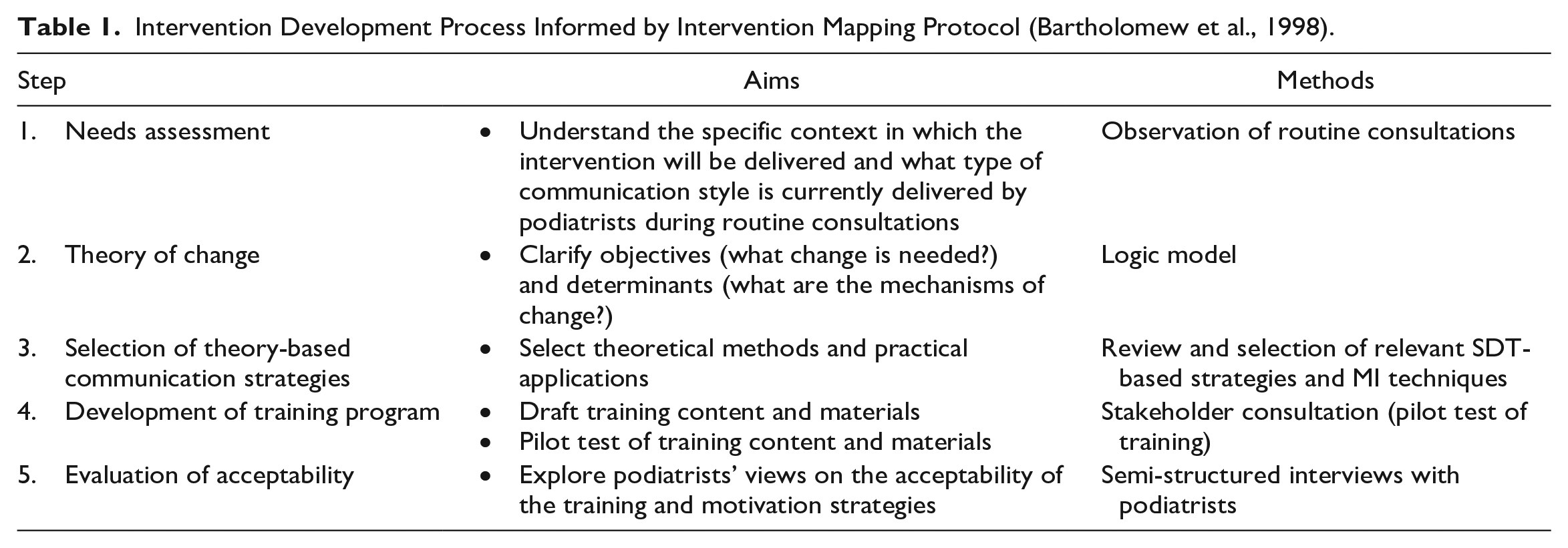
Aligned with the UK Medical Research Council guidance (Skivington et al., 2021), development of the training program was a pragmatic, dynamic, and iterative process that involved understanding the problem and context, involvement of stakeholders, drawing on existing theories and research evidence, undertaking of primary data collection (i.e., observation), and pilot testing to assess acceptability. The study was registered (ClinicalTrials.gov: NCT03853941) and approved by the East Midlands–Derby Research Ethics Committee (REC Number 18/EM/0162), in July 2018, and written informed consent was obtained from all participants. The training program was systematically planned following the first five stages of the Intervention Mapping protocol (Bartholomew et al., 1998). Table 1 provides an overview of the intervention development process.
Intervention Development Process Informed by Intervention Mapping Protocol (Bartholomew et al., 1998).
Step 1: Needs Assessment
The aim of Step 1 was to establish an understanding of what needs to be changed and the specific context for the intervention. As detailed in the introduction, patient-provider communication is an important factor influencing adherence in patients living with DFUs (e.g., Coffey et al., 2019; Gale et al., 2008; Hancox et al., 2023; Searle et al., 2008). Observation was undertaken to gain a detailed understanding of behavior change conversations in routine DFU consultations and the extent to which such discussions are aligned with SDT and MI approaches.
Observation
Design
The observational study was conducted in a secondary care, Diabetes Foot Clinic within the East Midlands. A nonparticipant observer (WJC, a Research Assistant trained in conducting observations) live-coded the communication style of podiatrists during routine DFU consultations between May and August 2019. Prior to the consultation, the observer explained they were a researcher interested in understanding more about patient–practitioner communication and were there to observe the consultation. Patient and podiatrist participant demographics (e.g., age, gender, and ethnicity) were collected using a short questionnaire.
Participants
Opportunistic sampling was used to recruit patient participants who met the inclusion criteria of adults (aged 18+ years) diagnosed with diabetes, and who currently had a DFU. Eligible patients were approached by a member of their usual care team who explained the nature of the study and what participation would involve and provided an information sheet. Patients were given a minimum of 24 hours to consider their participation before providing written informed consent.
Podiatrists working in the specialist Diabetes Foot Clinic, aged 18 and over, with at least 6 months of experience working within the NHS were invited to participate in the study. Eligible podiatrists were provided with an information sheet that informed them of all aspects pertaining to participation and given 24 hours or more before written informed consent was obtained.
Twenty-four patient consultations were observed. Participants included 18 males and 6 females, mean age of 60.8 (SD = 10.8, range = 35–81 years, 71% in their 50s or early 60s), and all participants were White British with English as their first language.
Fifteen podiatrists (12 female, 3 male, mean age = 45.7 years, SD = 12.2, range = 26–58 years) were observed. Most podiatrist participants were observed once or twice, one was observed five times. Podiatrists selected who was observed, depending on availability at the time of the patient’s appointment and clinical need.
Observation Measures
Observations were live-coded using the Behavior Change Counseling Index (BECCI; Lane, 2002). The BECCI was designed to measure practitioners’ use of MI-informed behavior change counseling techniques and has been found to demonstrate acceptable levels of reliability and validity (Lane et al., 2005). The BECCI uses 11 items, grouped into four domains, representing different MI skill competencies. Domain 1: Agenda Setting & Permission Seeking (Items 1 & 2, e.g., The practitioner invites the patient to talk about behavior change); Domain 2: The Why & How of Change in Behavior (Items 3–7, e.g., Practitioner uses empathic listening statements when the patient talks about the topic); Domain 3: Whole Consultation (Items 8–10, e.g., Practitioner acknowledges challenges about behavior change that the patient faces); and Domain 4: Talk about Targets (Item 11, Practitioner and patient exchange ideas about how the patient could change current behavior). Each item was rated on a five-point Likert-type scale (0 = not at all to 4 = a great extent). An estimate of the ratio of time spent speaking and the behavior change topics discussed was noted.
Aligned with SDT, three items were used to assess the extent to which the observer perceived the podiatrist to actively communicate with the patient in a need-supportive way (i.e., “practitioner actively fosters the patient’s autonomy by supporting their sense of control over their health behavior ‘practitioner actively fosters the patients’ feelings of competence by supporting the patient’s abilities and capabilities to master their health behavior” and the “practitioner actively relates to the patient with care and respect and shows an interest in aspects of their lifestyle that are important to them”). Items were rated on a five-point Likert-type scale (0 = not at all, 1 = minimally, 2 = to some extent, 3 = a good deal, 4 = a great extent).
Consultations were live-coded, and audio recording was not possible in the busy clinic environment due to concerns over privacy of nearby patients. The observer was trained in SDT and MI, read literature about behavior change in health care settings, for example, Rollnick et al. (2008), and completed the online BMJ module “Motivational interviewing in brief consultations” (https://new-learning.bmj.com/course/10051582). The observer also attended a six-hour MI training session, tailored to the context of the current study and designed and delivered by a Motivational Interviewing Network of Trainers trainer. This included fidelity training, whereby BECCI was used to code six video recordings of consultations using gradually more complex MI consistent techniques. Within this context, fidelity refers to the observer’s ability to recognize clinician strategies that are MI-consistent and codable using BECCI. Competency in using the BECCI was assessed by inter-rater reliability with two experienced coders to ensure a level of consistency (i.e., to score within one point of each other), prior to clinic observations. Throughout this process and during the clinic observations, the BECCI Coding Manual (Lane, 2002) was followed to ensure the accuracy of interpretation.
Data Analysis
Quantitative data was entered into SPSS software (v.24). Patient demographics (e.g., age and gender) and descriptive statistics were produced (e.g., mean scores for each BECCI item).
Results: Usual Care Observation
Patient–Practitioner Speaking Ratio
The mean consultation length was 40 minutes (SD = 24; range = 20–130). The ratio of practitioner-to-patient speaking is relevant because health care professionals are viewed as having more person-centered conversations if they speak less than the patient (Lane et al., 2005). In six consultations (25%), the practitioner spoke for more than half the time. In 16 consultations (67%), there was an even split in time talking between the patient and podiatrist. In two consultations (8%), the practitioner spoke for less than half the time.
Behavior Change Topics Discussed in Consultations
In eight consultations, no behavior change was discussed. In the remaining consultations, the topics discussed most often were adherence to footwear (n = 11), limiting weight-bearing (n = 5), medications (n = 3), and dressing adherence (n = 1).
Use of MI-Informed Techniques in Routine DFU Care
BECCI scores are displayed in Table 2. The techniques most used were showing sensitivity to talking about other issues and talking about current behavior. The least used were summaries, encouraging talk about behavior change, and empathetic listening statements.
Mean Scores for BECCI Items.
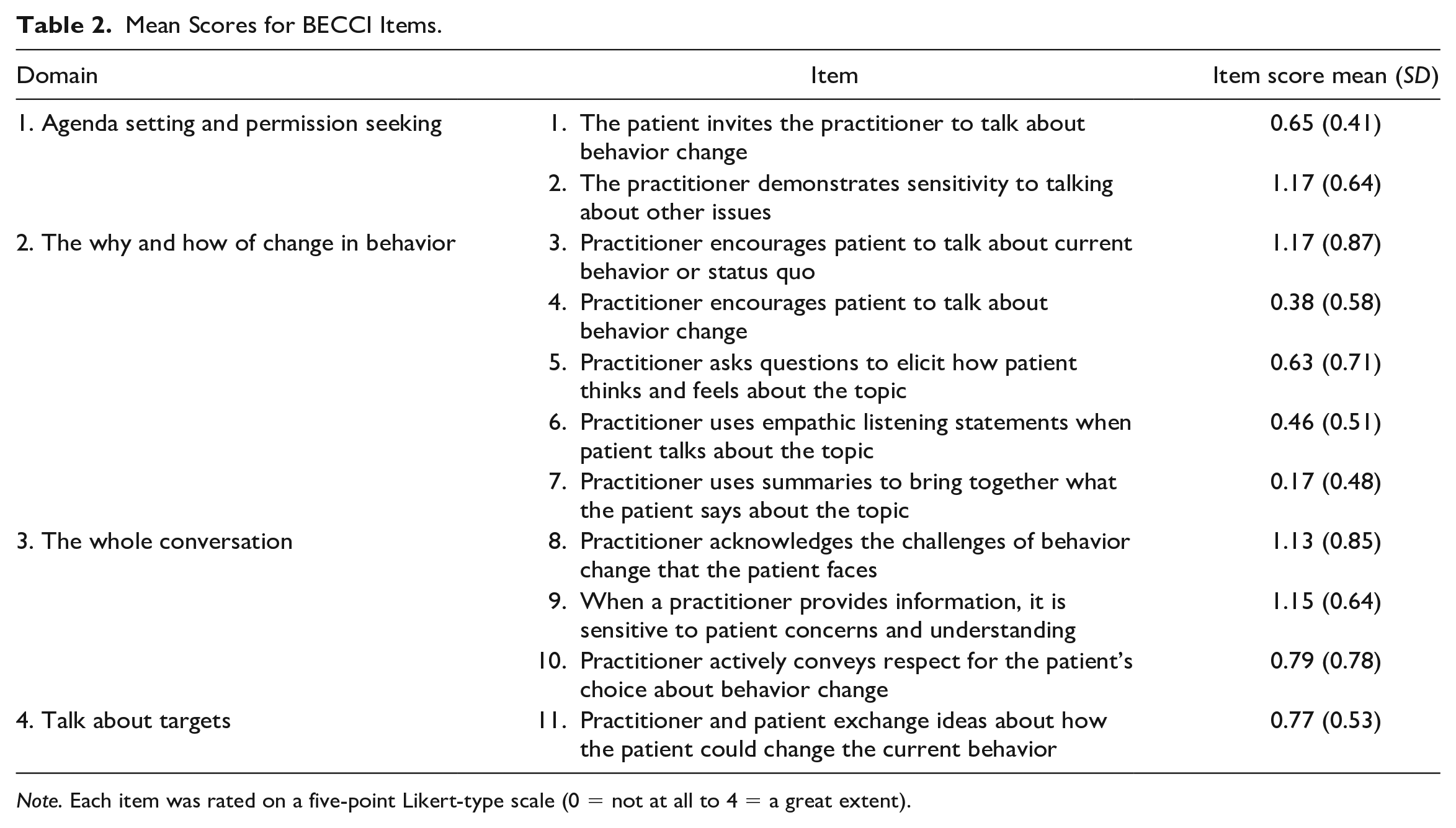
Note. Each item was rated on a five-point Likert-type scale (0 = not at all to 4 = a great extent).
Need-Supportive Communication
Need-support from the podiatrists while communicating with the patient was perceived to be minimal. The observer noted support for relatedness (mean = 1.75, SD = 0.85) to be higher than autonomy (mean = 1.17, SD = 0.76), and competence (mean = 1.21, SD = 0.88); however, all scores were modest.
Step 2: Theory of Change
The needs assessment in Step 1 identified opportunity for improvement in the patient-provider communication style. Based on the findings of Step 1, SDT (Deci & Ryan, 1985) was selected as the guiding framework for developing a communication intervention to promote adherence to treatment advice in patients with DFUs. See Figure 1 for a logic model illustrating the theory of change.
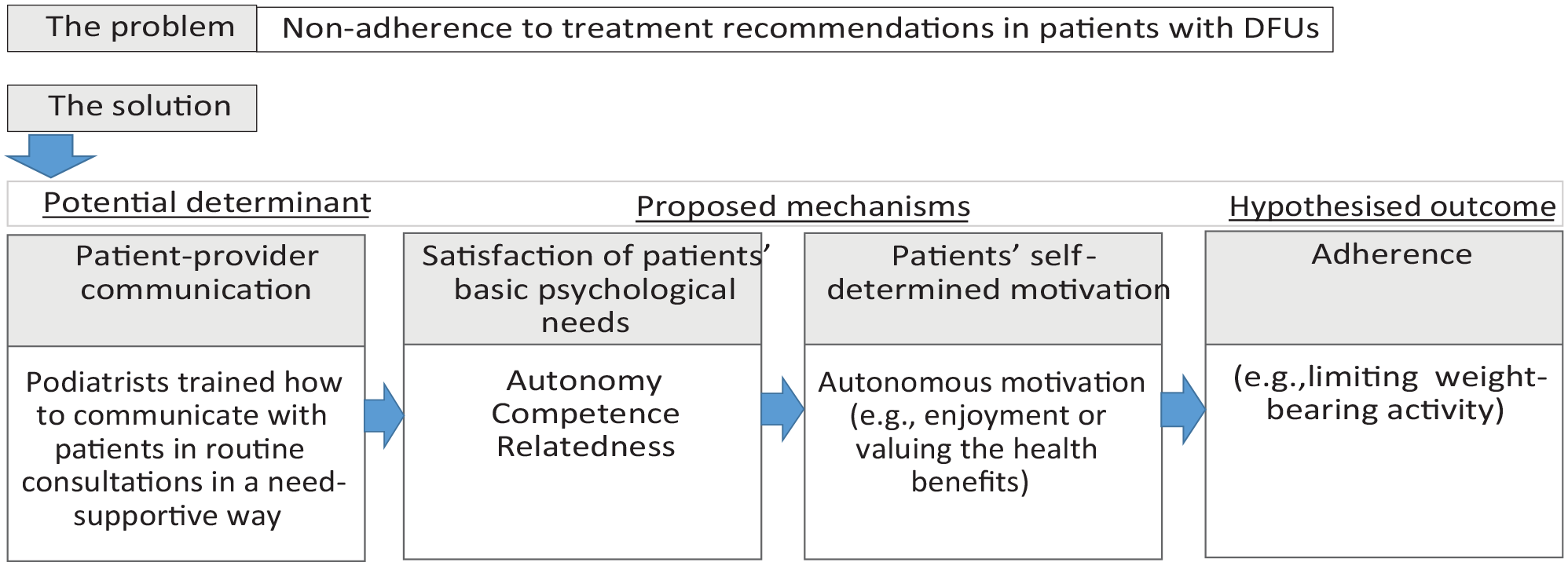
Logic Model Illustrating the Theory of Change Based on Self-Determination Theory (Deci & Ryan, 1985).
Step 3: Selection of Theory and Evidence-Based Communication Strategies
Motivation strategies, relevant to the specific context of a diabetic foot consultation (see Table 3), were selected from those in previous SDT interventions (i.e., Gillison et al., 2019; Ntoumanis et al., 2021). As with other applied SDT research (e.g., Coumans et al., 2020), MI techniques (e.g., open questions, reflections) were included as a means of promoting satisfaction of patients’ basic psychological needs. The selection of theory and evidence-based SDT strategies and MI techniques was informed by Stage 1 needs assessment findings, consultation with a patient and public involvement (PPI) group, health care professional advisory group, and guided by a proficient MI practitioner. Examples within the training were focused on discussions regarding patients’ limiting weight-bearing activity as this has been highlighted by podiatrists (health care professional advisory group) and patients (Hancox et al., 2023) as an area for improvement. However, the motivational strategies can be applied to other adherence-related conversations.
Motivation Strategies Organized by MI Process.
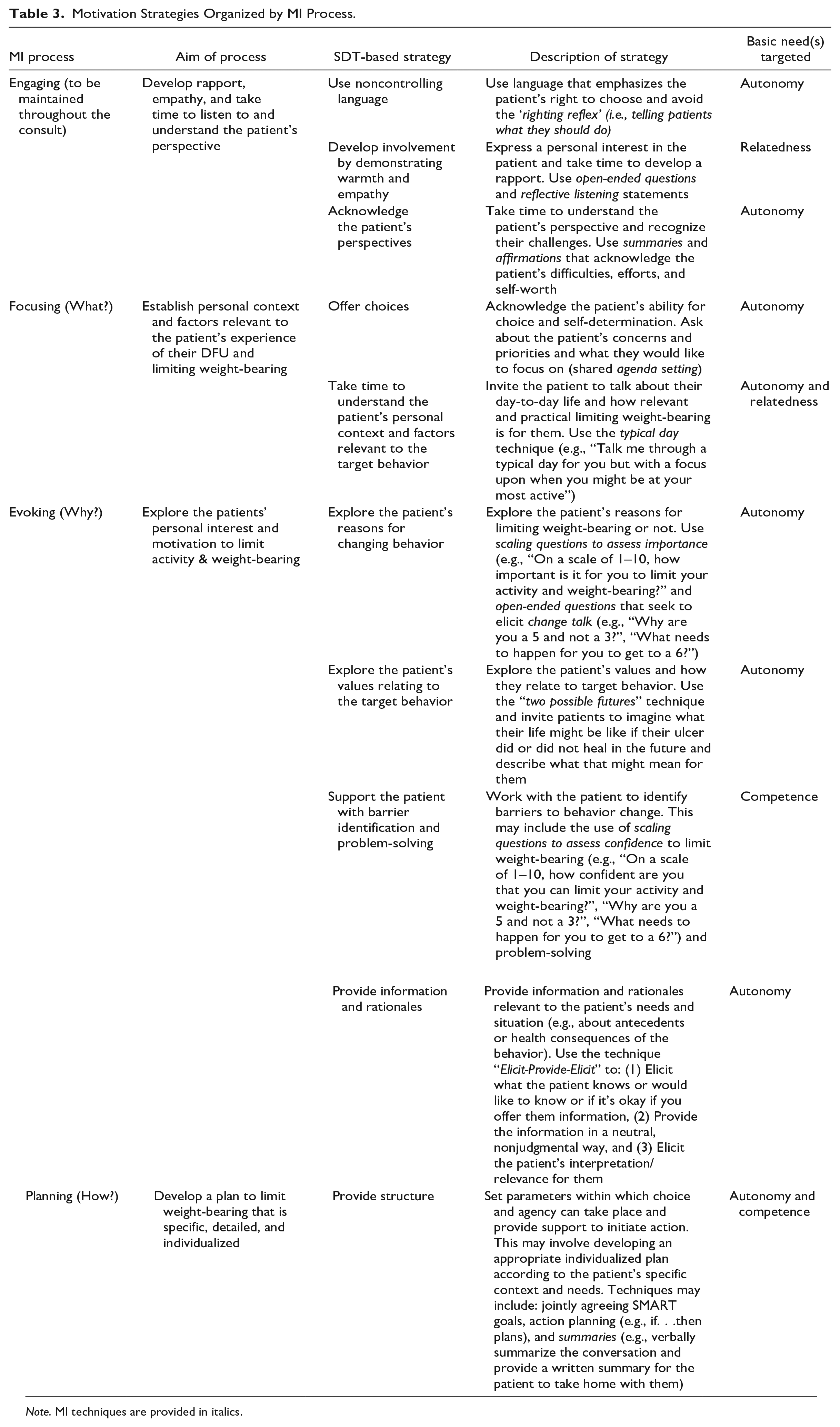
Note. MI techniques are provided in italics.
The training content was structured using the four processes of MI: engaging, focusing, evoking, and planning (Miller & Rollnick, 2012) to provide podiatrists with a guide as to when certain strategies may be most relevant within the consultation process. The four processes are both sequential and recursive as the practitioner may need to return to prior processes as needed (Miller & Rollnick, 2012). Table 3 details each SDT strategy, the way it maps onto constructs of SDT, and the four processes of MI and relevant MI techniques.
Step 4: Development of Training Program
Training content and materials were drafted. The program covered both theoretical aspects (e.g., the importance of satisfying patients’ basic psychological needs and promoting self-determined motivation for long-term adherence) and practical need-supportive communication strategies (e.g., acknowledging patients’ perspectives). A mix of PowerPoint slides, video examples, small group discussions, and role-play activities were included.
The draft training program was piloted with five diabetic foot health care professionals (three podiatrists, one consultant podiatric surgeon, and one specialist registrar, mean years of experience = 15.32, range = 5–30). Two researchers, one experienced in delivering SDT interventions (J.H.) and the other experienced in delivering MI training to health care professionals (C.H.) led the one-day (five-hour) training session at an NHS hospital in the East Midlands. A questionnaire distributed at the end of the training revealed that health care professionals view the training as relevant to their job role (8.6/10) and enjoyable (9.2/10). They described feeling reasonably confident with integrating the skills learned into routine consultations (8.2/10), however, a few noted that they would need more practice time and reminders to support integration into practice. Practical strategies, such as scaling questions to assess patients’ importance and/or confidence regarding changing behavior, were described by health care professionals as the most useful aspects of the training. Health care professionals valued the chance to practice the communication strategies and discuss how what they say could be re-phrased in a more motivationally supportive way. In terms of improvements, feedback suggested it was “a lot to cover in one-day” and that multiple shorter sessions might be better.
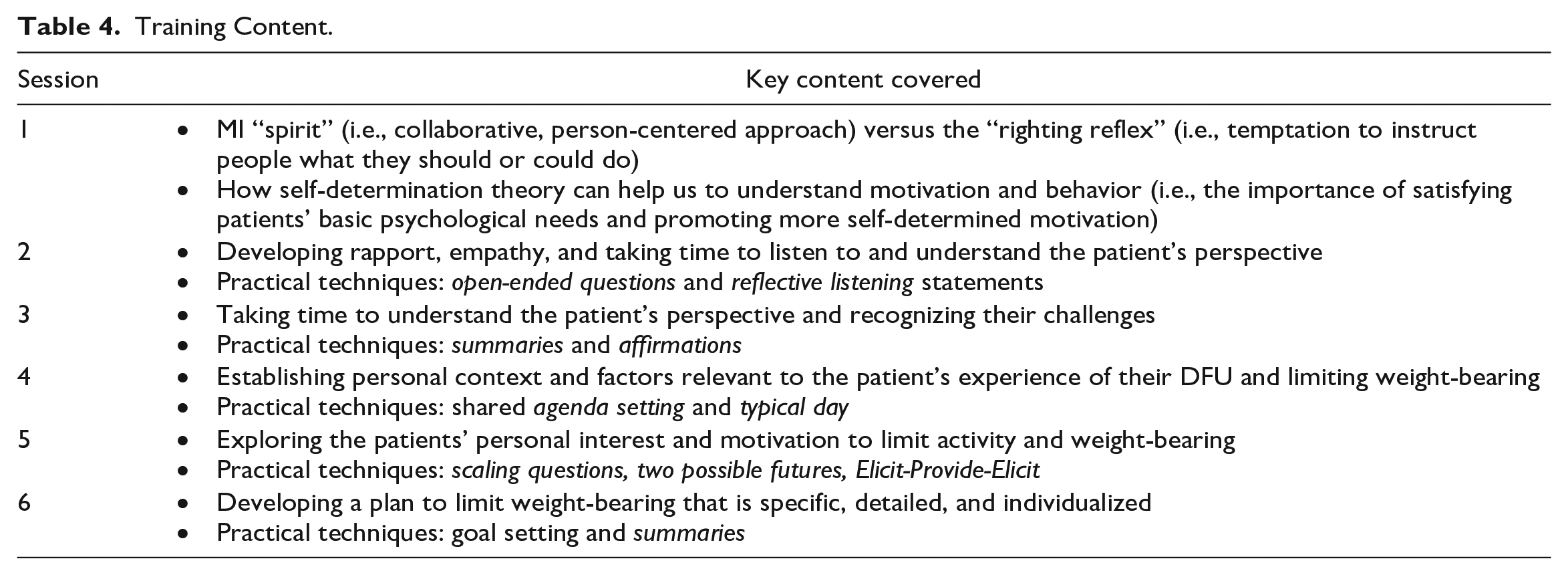
Following the pilot training, researchers met with three podiatrists working within the specialist diabetes unit in which the final training program would be delivered. Views were sought on practical aspects of training delivery (e.g., when, where, and how long). There was a preference for short training sessions delivered over multiple weeks. Thus, the final intervention consisted of 6 × 1-hour face-to-face training sessions delivered from 8 to 9 a.m. in a seminar room within the hospital where the podiatrists work. The training was delivered by two researchers (J.H. and C.H.) over an 8-week period (with the first four sessions delivered weekly, and the last 2 fortnightly) to enable podiatrists’ time to practice the motivation strategies between sessions. Participants were provided with a written summary of the practical strategies and audio recordings of key points covered in each training session. The focus of each training session is briefly outlined in Table 4.
Training Content.
Step 5: Acceptability of the Training Program
The training was delivered to six diabetes specialist podiatrists (1 male, 5 female; mean age = 35.83, SD = 11.41, all White British) working in a specialist Diabetes Foot Clinic in the East Midlands, UK (a different NHS Trust to the pilot training) from August 16 to October 4, 2019. Inclusion criteria were aged 18 and over and have at least 6 months of experience working within the NHS. On average podiatrists had worked in the NHS for 9 years (range = 4–17 years) and had been in their current role for 5 and half years (range = 1–17 years). Three podiatrists attended all six training sessions (100%). One podiatrist attended 5/6 sessions (83%) and two attended 4/6 sessions (67%). Reasons for missing sessions included holidays and illness. Those missing sessions were encouraged to listen to the provided audio-recorded summary.
Semi-structured interviews were conducted within 2 months of the end of the training to explore podiatrists’ views on acceptability of the training program and motivation strategies. All six podiatrists who took part in the training were invited to be interviewed. Interviews were conducted via telephone by an independent consultant researcher not involved in delivering the training program, to reduce the risk of social desirability bias.
An interview guide (see Supplementary Material A), developed by C.H. and J.H., was used to explore podiatrists’ thoughts on and experiences of receiving the training, implementation of strategies in practice, and suggestions for improvements. Interviews lasted approximately 30 minutes and were audio-recorded, transcribed verbatim, and anonymized. Data were analyzed in NVivo (version 12) using a deductive thematic analysis (Braun & Clarke, 2006) based on the content of the interview guide and motivation strategies (see Table 3). Analysis was conducted by J.H. (a researcher trained in qualitative analysis). Although J.H. was involved in delivering the training program, when analyzing the data J.H. took a neutral stance, taking into consideration the range of opinions expressed by interview participants and using supporting quotes to illustrate the interpretation of the data and support confirmability. Following familiarization with the data through “active reading” of transcripts, initial codes were generated. Codes were then collated into potential themes which were discussed with all authors. Detailed field notes and a clear audit trail of analytic decisions were kept to maximize transparency and ensure credibility and quality.
Five out of six podiatrists agreed to participate in a semi-structured interview. Four main themes were identified: positive aspects of the training, ideas for improvement, acceptability of motivation strategies, and challenges in putting the strategies into practice. A brief outline of each theme is provided below. Further details including subthemes and illustrative quotes are provided in Supplementary Material B.
Positive Aspects of the Training
Podiatrists liked that the training was delivered over multiple sessions enabling time to practice between sessions. However, it was suggested that longer sessions (e.g., 1.5 hours) would be preferable. The small group format was described as supportive, enabling participants to feel involved and contribute. Trainers were viewed as approachable and sharing of “real life” examples was valued. Podiatrists liked the mix of activities (e.g., videos, role-play) and learning resources (e.g., handouts). Those missing sessions found the audio-recorded summary helpful for catching up on the content. The podiatrists valued the opportunity to reflect on their approach to motivating patients and found the specific strategies helpful. Overall, the training was viewed as valuable and relevant for a wide range of health care professionals.
Suggestions for Improvements
It was suggested that online resources for easy access would be beneficial. Podiatrists explained a tailored handout for patients with a summary of what was discussed regarding behavior change, and video examples of strategies in the specific context of DFUs would also be helpful.
Acceptability of Motivation Strategies
The only technique that was considered as not appropriate for the patient population was the “no change” version of the two possible futures strategy which invites patients to imagine what their life might be like in 6 months’ time if their ulcer did not heal. Podiatrists explained that for patients who have had the ulcer for years, the technique appeared to reinforce their negative view that no matter what they do their ulcer will not heal. Instead, asking patients the “change has occurred” version of this strategy, whereby patients are invited to think about what it would mean for them if their ulcer healed, was viewed more favorably.
Challenges of Putting the Strategies Into Practice
Challenges experienced putting the strategies into practice included: time pressures and competing demands during consultations, other health care professionals using a more directive communication style, avoiding the righting reflex (i.e., wanting to tell the patient what to do), breaking the habit of asking closed questions, confidence using the strategies and perception that some patients will not change no matter what health care professionals say.
Discussion
The aim of this study was to describe the development and acceptability of a motivation communication training program for diabetes-specialist podiatrists focused on supporting adherence discussions. The training program was theory and evidence-based and developed in a systematic way considering the specific context. Observation was undertaken to gain an understanding of the communication style currently used by podiatrists during routine consultations. Findings suggest that while some MI-consistent techniques are used, there is an opportunity for improvement in quality and consistency. These findings reinforced the need for the development of a communication training program for this population. Observation highlighted areas for improvement (e.g., use of summaries, reflective listening statements, and satisfaction of patients’ basic psychological needs) which informed training development.
The training program was positively received by podiatrists. Suggestions for improvements (e.g., longer sessions, online resources) will be explored and if feasible incorporated in future iterations of the training program. A particular challenge noted by podiatrists was other practitioners entering the consultation and using a more directive communication style. Podiatrists expressed the training would be relevant for a wide range of health care professionals. Widening the scope of the training to include all health care professionals within the multidisciplinary team may address support for a more consistent and cohesive motivational approach with patients.
The only motivation technique considered not appropriate was the “no change” version of two possible futures. Wagner and Ingersoll (2008) have cautioned this MI technique, which aims to develop discrepancy, is consistent with a negative reinforcement model (e.g., change is needed to escape a negative future). Such an approach may evoke introjected motivations, characterized by pressure to act to resolve negative emotions (e.g., shame or fear), which are not considered conducive to long-term behavior change. Moreover, podiatrists in this study noted the technique to be particularly problematic with those who had been a patient for a long time as it reinforced their already negative emotions. It has been suggested (Neipp et al., 2021; Wagner and Ingersoll, 2008) that, instead, the focus should be on moving toward a positive future state (such as is imagined in the “change has occurred” version of the two possible futures). This approach is more aligned with SDT and promotion of autonomous motivation with an emphasis on how individuals can proactively seek a better future.
Time pressures and competing demands were described by podiatrists as a further challenge to integrating the strategies routinely into practice. Many of the podiatrists interviewed worked in both clinic (hospital outpatient) and community settings and explained strategies were easier to implement in community settings. Often community visits are longer, with more consistency in which practitioner visits and fewer distractions. Podiatrists typically engage in casual rapport-building conversations while treating the ulcer and replacing dressings and therefore are uniquely placed with the opportunity to have all-important behavior-change conversations with patients (Gabbay et al., 2011). However, they typically do not receive formal training in motivation communication approaches. To address this gap in training provision, future research could explore the implementation of the training program within community settings.
Strengths and Limitations
A key strength of the study was the systematic and rigorous approach to intervention development with a key focus on tailoring to the specific context. Observation of the current motivation communication style used by podiatrists enabled identification of key areas for improvement and maximized the likelihood that intervention would be relevant and enhance current practice. Furthermore, involvement of stakeholders throughout the development process aided the refinement of content, format, and delivery of the training to optimize acceptability (Skivington et al., 2021).
A limitation of the study is acceptability of the training being tested with a small sample (n = 6) of podiatrists, limiting the generalizability of findings to more diverse populations. The observed patient sample also lacked diversity (mainly male, White ethnicity, aged over 65). Although this sample is representative of the wider patient population living with DFUs (Public Health England, 2022), recruitment of a more heterogeneous sample (e.g., inclusion of ethnic minority patients) should be explored in future research. Another limitation of the present study is the lack of exploration of patients’ views on receiving care from podiatrists who have undergone the training, a noteworthy avenue for future research. The present study focused on health care communication, and other barriers to patient treatment adherence (e.g., lack of pain, depression; Hancox et al., 2023) could be addressed in future research.
A proof-of-concept study, using a nonrandomized, controlled before-and-after design, to assess the training’s impact on podiatrists’ communication and patient behavior has been submitted elsewhere (Hancox et al., in press). Furthermore, we intend to address the limitations identified in a larger cluster randomized controlled trial which will aim to establish the feasibility and effectiveness of the intervention more widely.
Conclusion
Patient adherence to treatment recommendations is crucial in both preventing and treating DFUs. However, patients encounter challenges in this regard, expressing dissatisfaction with the patient–practitioner relationship and the way treatment advice is conveyed, which serves as a significant barrier. To our knowledge, this is the first study to test the acceptability of an SDT-based and MI-informed training program with this population. This research makes an important contribution to the literature by advancing the understanding of the practicalities of translating motivational principles in routine consultations with patients living with DFUs. Findings relating to the challenges experienced by podiatrists when integrating the motivation strategies into practice can be used to improve future training.
Supplemental Material
sj-docx-1-heb-10.1177_10901981231216744 – Supplemental material for Development of a Motivation Communication Training to Aid Diabetes-Specialist Podiatrists With Adherence Discussions
Supplemental material, sj-docx-1-heb-10.1177_10901981231216744 for Development of a Motivation Communication Training to Aid Diabetes-Specialist Podiatrists With Adherence Discussions by Jennie E. Hancox, Wendy J. Chaplin, Charlotte Hilton, Katie Gray, Fran Game and Kavita Vedhara in Health Education & Behavior
Supplemental Material
sj-docx-2-heb-10.1177_10901981231216744 – Supplemental material for Development of a Motivation Communication Training to Aid Diabetes-Specialist Podiatrists With Adherence Discussions
Supplemental material, sj-docx-2-heb-10.1177_10901981231216744 for Development of a Motivation Communication Training to Aid Diabetes-Specialist Podiatrists With Adherence Discussions by Jennie E. Hancox, Wendy J. Chaplin, Charlotte Hilton, Katie Gray, Fran Game and Kavita Vedhara in Health Education & Behavior
Footnotes
Data Availability
Data is available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project was funded by the National Institute for Health Research (NIHR) School for Primary Care Research (project reference 399). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.