
Abstract
Introduction
Community health workers (CHWs) are health promotion specialists who are trusted members of the community served and have a close understanding of the community’s needs and values. CHWs are a cost-effective and scalable workforce to promote health among men through tailored approaches. The purpose of the present review was to use the RE-AIM Framework to assess design, implementation, and outcomes of CHW-implemented health promotion efforts tailored for men to provide recommendations for future efforts.
Methods
The protocol was pre-registered with PROSPERO. The primary inclusion criteria were that the interventions were (a) implemented at least partially by CHWs, (b) conducted only among men, and (c) designed to improve a health-related outcome. PubMed, EMBASE, PsycINFO, CINAHL, Web of Science, and Global Index Medicus were searched using a librarian-generated search strategy. In all, 1,437 articles were uploaded to Rayyan and two reviewers blindly reviewed each article for inclusion. A total of 24 articles met the inclusion criteria.
Results
Most interventions (a) targeted men under 50 years, (b) were conducted among a subset of underserved men, (c) improved health outcomes, (d) community-based and informed, (e) atheoretical, and (f) had satisfactory retention rates. The roles and responsibilities of CHWs were varied. Attention was given to training of CHWs, but limited attention was given to how/if the CHWs were supervised.
Discussion
CHW-implemented interventions can improve health outcomes among men. Opportunities exist to build on past interventions, such as addressing mental health and incorporating prosocial aspects of masculinity. The results have implications for designing similar interventions.
Introduction
Surveillance data from the World Health Organization (WHO) indicates that women have a higher healthy life expectancy (i.e., the average number of years that a person can expect to live in “full health”) than men, that women live longer than men, and that many of the causes of unhealthy life expectancy and premature mortality among men are preventable (WHO, 2019). Efforts seeking to promote health and mitigate the impact of these preventable causes of premature mortality among men have been limited in their impact. Too few health promotion efforts are tailored for men (Griffith, 2016; Robertson et al., 2008; Treadwell & Young, 2013), despite widespread recommendations that efforts seeking to promote health among men should be tailored for men. This recommendation is supported by the 2001 WHO Madrid Statement—a statement that strongly recommended that health promotion efforts recognize the psychosocial differences in health promoting facilitators and barriers between women and men (WHO, 2001). This recommendation has been echoed by experts in men’s health (Baker, 2016; Baker et al., 2014; Ostlin et al., 2006; Teo et al., 2018; Weller & Campbell, 2009) and a comprehensive systematic review (Robertson et al., 2008).
Men are underrepresented in health promotion efforts that are not gender specific (Rounds & Harvey, 2019). For example, physical activity interventions whose inclusion criteria includes both men and women report much higher recruitment and retention (>80%) of women (Maher et al., 2014; Newton et al., 2014; Ryan et al., 2019; Whitt-Glover et al., 2014; Whitt-Glover & Kumanyika, 2009). While this has often led men to be characterized as a “hard to reach” population or as people who do not care about their health (Griffith et al., 2012, 2016; S. Robertson, 2006), qualitative and other empirical research suggests otherwise (Gough, 2013; Gough & Conner, 2006; Griffith et al., 2011, 2015). The limited attention to gender-tailoring of recruitment and intervention efforts may help to explain difficulties in the recruitment (Halbert et al., 2020; Robertson et al., 2008; Teo et al., 2018) and retention (Halbert et al., 2020; Maher et al., 2014; Ryan et al., 2019) of men in these efforts. These gendered patterns in health promotion intervention participation suggest that more attention is needed to understand and address how recruitment strategies, intervention approaches, intervention materials, and other health promotion components are gender and age appropriate (Griffith et al., 2012). Therefore, there is a need for interventions that are tailored to and for men by explicitly considering the psychosocial norms, beliefs, attitudes, and expectations that adult males experience. Developing interventions intentionally for men has the unique potential to boost recruitment, increase retention, and enhance the impact on men’s health promotion and men’s health outcomes.
Tailoring Efforts for Men
There is ample literature identifying and arguing for the need to understand the barriers to participation that impact health and health-promoting efforts among men, but the bulk of this research is at the Institute of Medicine’s (IOM) T0 stage of research (i.e., basic findings). This literature points to the underlying role of hegemonic or traditional masculinity (Seidler et al., 2016)—an idealized form of masculinity in a given place, time, and culture that reflects assumed norms and beliefs that are questioned and accepted as true (Courtenay, 2000). The Health, Illness, Men, and Masculinities is a theoretical framework that has been offered to help explain how these normative expectations shape men’s health and health behavior (Evans et al., 2011). This framework shifts the focus of understanding men’s health and health promotion away from the individual toward the sociocultural phenomenon of masculinity—a structural context that fosters and reinforces adverse health knowledge/views and practices through socially created gender norms (Griffith, 2020).
The direct and indirect impact of how men accept, reject, or reimagine aspects of gender ideals on men’s health and health promotion have been well-researched, but often men’s health patterns are attributed to characteristics of men rather than the structural conditions that shape their health (Griffith, 2016, 2018, 2020). Research indicates that men, compared to women, have low health-related knowledge (Beier & Ackerman, 2003) and a functional view of their body and health (Robertson et al., 2008). In addition, men are more likely to engage in adverse health practices—they are less likely to seek health-related help (Teo et al., 2016), less likely to engage in health promoting behaviors (Teo et al., 2016; Yousaf et al., 2015), and more likely to engage in health risk-taking behaviors (Harris et al., 2006). These adverse health knowledge/views and practices regarding health are modifiable (Griffith, 2016) and may serve as targets for tailored health promotion efforts among men, though attempts to translate research findings into clinical trials or health promotion efforts (i.e., IOM T1 stage and beyond) among men are limited in quantity and have been largely unsuccessful (Robertson et al., 2008).
There are empirical findings and a strong theoretical rationale to focus on peer-based health promotion efforts. Systematic reviews and qualitative research has found that men like intervention approaches where only men are present, and where they are able to learn from and engage with other men (Friedman et al., 2012; Griffith et al., 2013, 2014, 2018; Hooker et al., 2011; James, 2004; Valdez et al., 2021; Wong et al., 2012; Young et al., 2012). Several theories have been used justify peer-based efforts (e.g., Social Learning Theory, Social Inoculation Theory, Role Theory, and Communication of Innovations Theory) (Turner & Shepherd, 1999). Because masculinity is a socially created, learned phenomenon, leveraging peers to promote men’s health can be particularly effective (Gough & Novikova, 2020). Research shows that peer-related social control is significantly associated with health promoting behaviors among men (Houle et al., 2017). This is supported by qualitative interviews with men that indicate that peer-related social control influences men’s health-promoting behaviors through inspiration and positive role-modeling (Houle et al., 2017). In addition, it is known that men prefer to receive health-related information from peers with shared experiences and circumstances (Lefkowich & Richardson, 2018), and who are credible and relatable (Sharp et al., 2018).
Improving Men’s Health Efforts With Community Health Workers
Given the literature on masculinities, peer-based health promotion, interventions that only include men, and interventions that are designed explicitly for men, it is likely that health promotion efforts implemented using community health workers (CHWs) may be a viable strategy to promote men’s health. The CHW Section of the American Public Health Association defines CHWs as “frontline public health workers who are trusted members of and/or have an unusually close understanding of the community served.” That is, by definition, CHWs are peers with shared experiences and circumstances, in addition to being credible and relatable. The roles of CHWs are varied including providing culturally appropriate health education and information, providing coaching and social support, building individual and community capacity, and conducting outreach, among others (Rosenthal et al., 2021). CHW’s membership and understanding of the communities served have enabled them to be successful in promoting health among underserved and at-risk communities across the globe (Viswanathan et al., 2010). Their membership of the communities served is also particularly useful to health promotion efforts among men. That is because recruitment and participation (i.e., uptake) of men in health promotion efforts are improved if such efforts occur in places that are more congruent with men’s gender norms and where men routinely reside/frequent (Oliffe et al., 2020).
There is widespread evidence indicating that CHWs have been successful in improving numerous health outcomes such as stroke, heart disease, Type II diabetes, HIV, and asthma (Jack et al., 2017). The impact of CHWs goes beyond improving the health of underserved and at-risk communities. These efforts are also cost-effective. One study found that CHWs generated a net savings of $1,135 per patient which equated to a savings of $2.30 for every dollar invested into a CHW program (Findley et al., 2014).
Purpose of Present Review
Despite the robust literature that demonstrates the success of CHWs, no known systematic or scoping review has sought to understand the impact of CHW-implemented interventions to improve men’s health. This is surprising because CHW-implemented health promotion efforts are well suited to promote recruitment and retention of men in health promotion efforts, in addition to producing meaningful changes in the health of the participating men. The purpose of the present scoping review is to assess the design, implementation, and outcomes of CHW-implemented health promotion efforts that are tailored for men. The findings of this review were analyzed using the RE-AIM Framework (Glasgow et al., 1999). This addition to a scoping review provides us the ability to assess recent CHW-led interventions to improve health among men and to provide evidence-based recommendations for the development and implementation of future CHW-led health promotion efforts targeting men.
RE-AIM Framework
The RE-AIM Framework is one of the most frequently used frameworks in the field of implementation science that is used to plan and evaluate health promotion programming (Glasgow et al., 1999, 2019). The RE-AIM Framework contains five dimensions:
Methods
This scoping review protocol was prepared in accordance with the PRISMA Extension for Scoping Review’s (PRISMA-ScR) 22-item methodological checklist and the framework for scoping reviews proposed by Arksey and O’Mally (Arksey & O’Malley, 2005; Tricco et al., 2018), in addition to the PICOS (i.e., population, intervention, comparison, outcome, and study type) framework (Petticrew & Roberts, 2008). See Supplemental File 1 for the PRISMA-ScR checklist. Prior to extraction and synthesis, the protocol was registered with and published by PROSPERO, an international database of systematic reviews (Wippold et al., 2021b). The authors collaborated with a research librarian at the authors’ institution to ensure a comprehensive search strategy. The finalized search strategy is provided in Supplemental File 2. Articles were identified by searching CINAHL (EBSCO), EMBASE (Ovid), Global Index Medicus, PsycINFO (EBSCO), PubMed, and Web of Science (Clarivate).
Studies were included if: (a) the primary target population was adult men or trans-men (age 18 or above), (b) the intervention sought to improve one or more health indicators, (c) the intervention was entirely or partially implemented by CHWs, (d) the study included a quasi-experimental or experimental design, and (e) the article was available in English or Spanish. Studies were excluded that (a) targeted men/trans-men and women, (b) targeted men or trans-men and children, (c) were not entirely or partially implemented by CHWs, (d) did not report the outcomes of a health promotion intervention, and (d) were not available in English or Spanish. Interventions implemented by individuals designated with often-used synonyms for CHWs (e.g., lay health advisors, promotores) were also included because these individuals share characteristics, roles, and responsibilities with CHWs. See search strategy for these synonyms. There were no restrictions on publication dates or country of implementation.
After conducting the search, results were imported into EndNote to identify and remove duplicates. The remaining titles and abstracts were uploaded to Rayyan—a reference managing software (Ouzzani et al., 2016). The titles and abstracts were independently screened by GMW and KAG against the eligibility criteria to identify studies for inclusion. Data extraction was guided and organized utilizing the RE-AIM Framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance)—a framework often used in the planning and evaluation of health interventions to ensure generalizability and facilitate the translation of research to practice (Glasgow et al., 1999). The following variables for data extraction were selected to align with each dimension of the RE-AIM framework: (1) Reach: participant age, inclusion criteria, and primary outcome(s); (2) Effectiveness: measure type (i.e., self-report and/or objective measures) and intervention results; (3) Adoption: intervention development, country of intervention, intervention setting, and theoretical framework or model; (4) Implementation: intervention dosage, CHW roles, CHW community embeddedness, barriers to intervention implementation, CHW title, training, and supervision, and study design; and (5) Maintenance: schedule of post-intervention data collection.
Results
A total of 2,857 articles were identified in the database searches, in which 1,420 duplicates were removed. The remaining 1,437 abstracts were uploaded to Rayyan and blindly examined by two reviewers (GMW & KAG) to assess inclusion. Reasons for the exclusion of articles during the full-text review included (a) the study included children, (b) there were multiple articles about the same intervention, and (c) the study was not based on an intervention (e.g., only focus groups conducted). This process resulted in 24 studies that met inclusion criteria for this scoping review. See Supplemental File 3 for PRISMA flowchart.
Reach Dimension
Data extracted that align with the Reach dimension were participant participant age, inclusion criteria, and primary outcome(s) (see Table 1).
Reach Dimension.
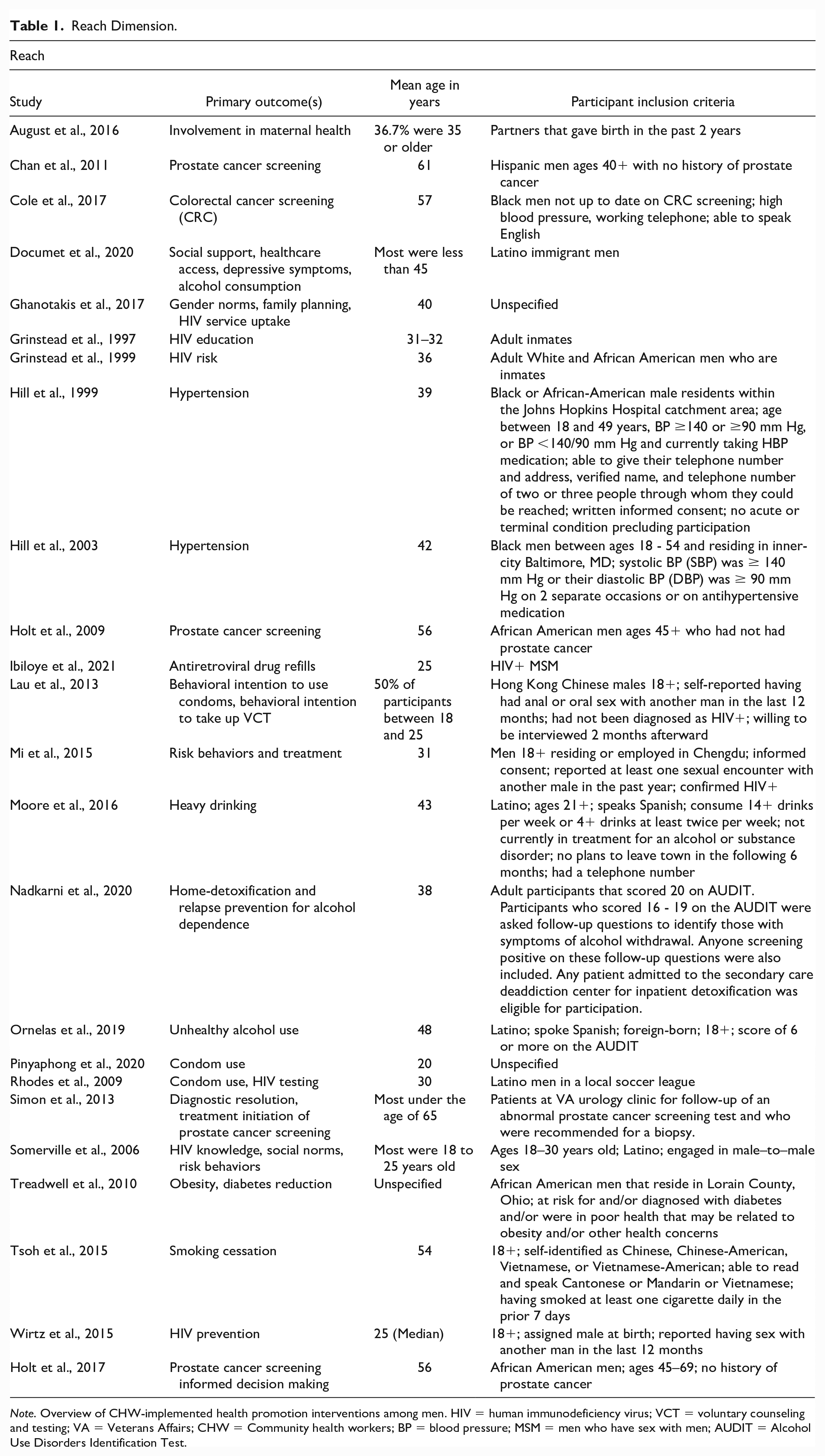
Note. Overview of CHW-implemented health promotion interventions among men. HIV = human immunodeficiency virus; VCT = voluntary counseling and testing; VA = Veterans Affairs; CHW = Community health workers; BP = blood pressure; MSM = men who have sex with men; AUDIT = Alcohol Use Disorders Identification Test.
Effectiveness Dimension
Data extracted that align with the Effectiveness dimension were measure type and intervention results (see Table 2).
Effectiveness Dimension.
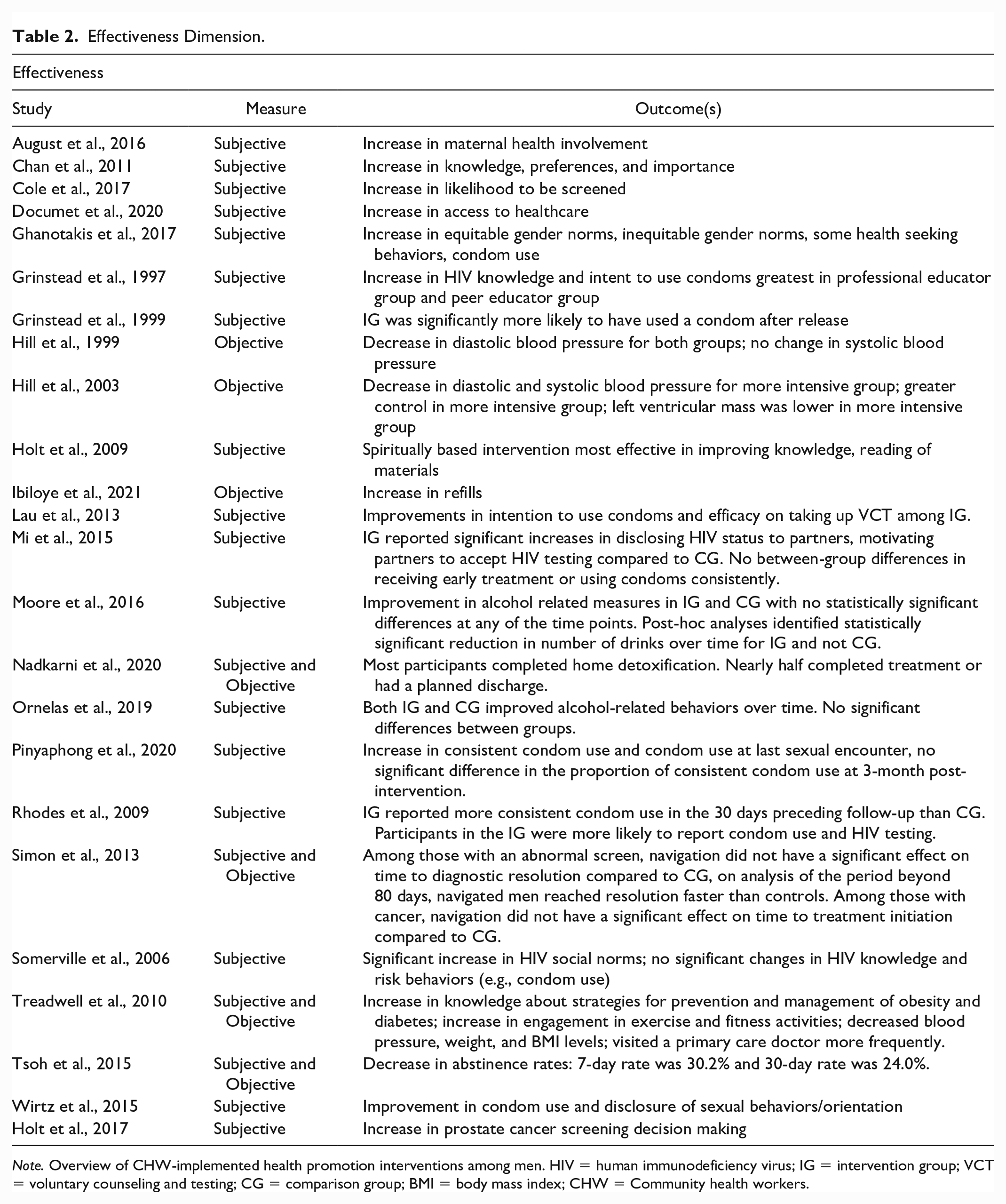
Note. Overview of CHW-implemented health promotion interventions among men. HIV = human immunodeficiency virus; IG = intervention group; VCT = voluntary counseling and testing; CG = comparison group; BMI = body mass index; CHW = Community health workers.
Adoption Dimension
Data extracted that align with the Adoption dimension were intervention development, country of intervention, intervention setting, and theoretical framework or model (see Table 3).
Adoption Dimension.
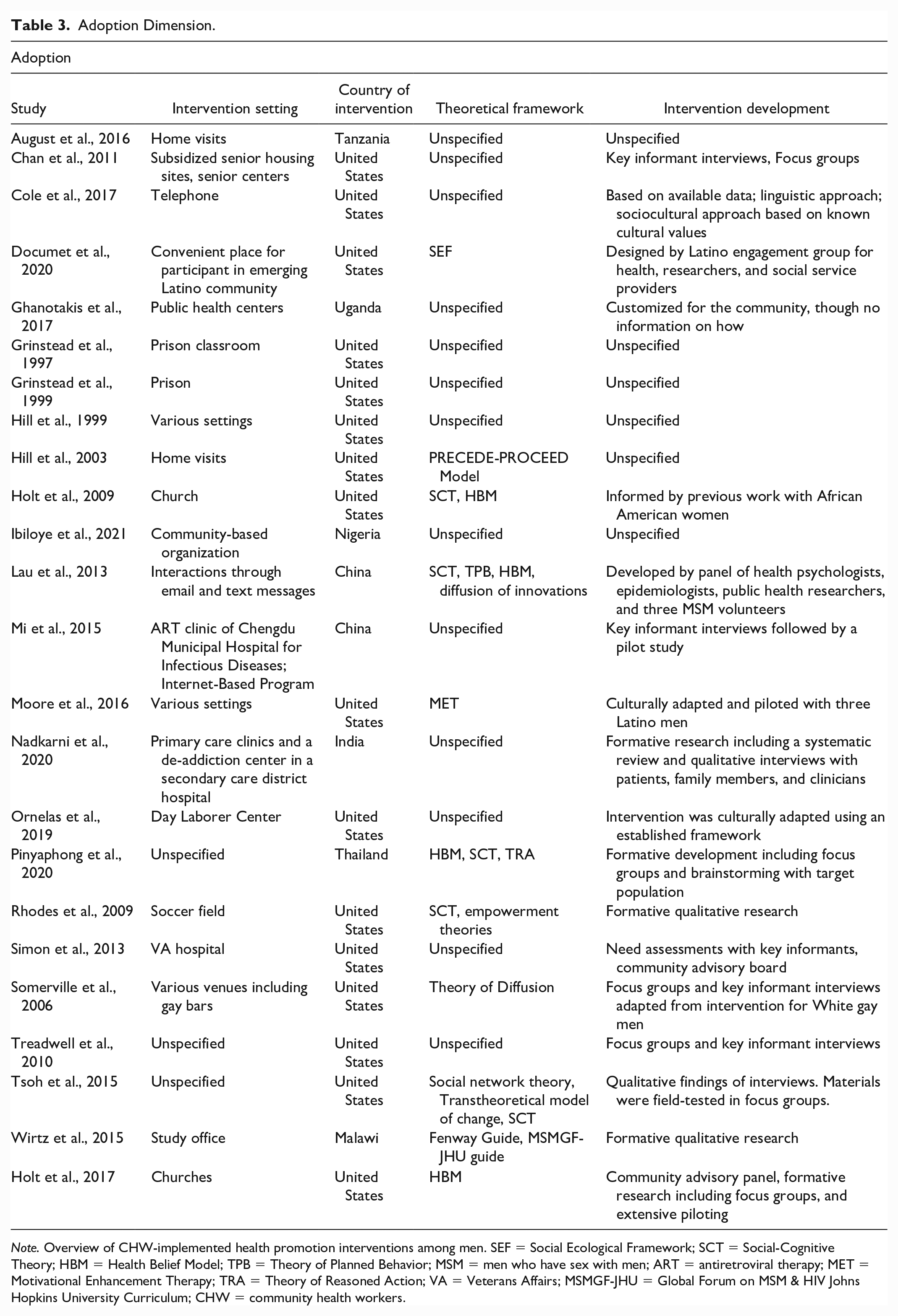
Note. Overview of CHW-implemented health promotion interventions among men. SEF = Social Ecological Framework; SCT = Social-Cognitive Theory; HBM = Health Belief Model; TPB = Theory of Planned Behavior; MSM = men who have sex with men; ART = antiretroviral therapy; MET = Motivational Enhancement Therapy; TRA = Theory of Reasoned Action; VA = Veterans Affairs; MSMGF-JHU = Global Forum on MSM & HIV Johns Hopkins University Curriculum; CHW = community health workers.
Implementation Dimension
Data extracted that align with the Implementation dimension were intervention dosage, CHW roles, CHW community embeddedness, barriers to intervention implementation, and CHW title, training, supervision, and study type (see Tables 4 and 5).
Implementation Dimension.
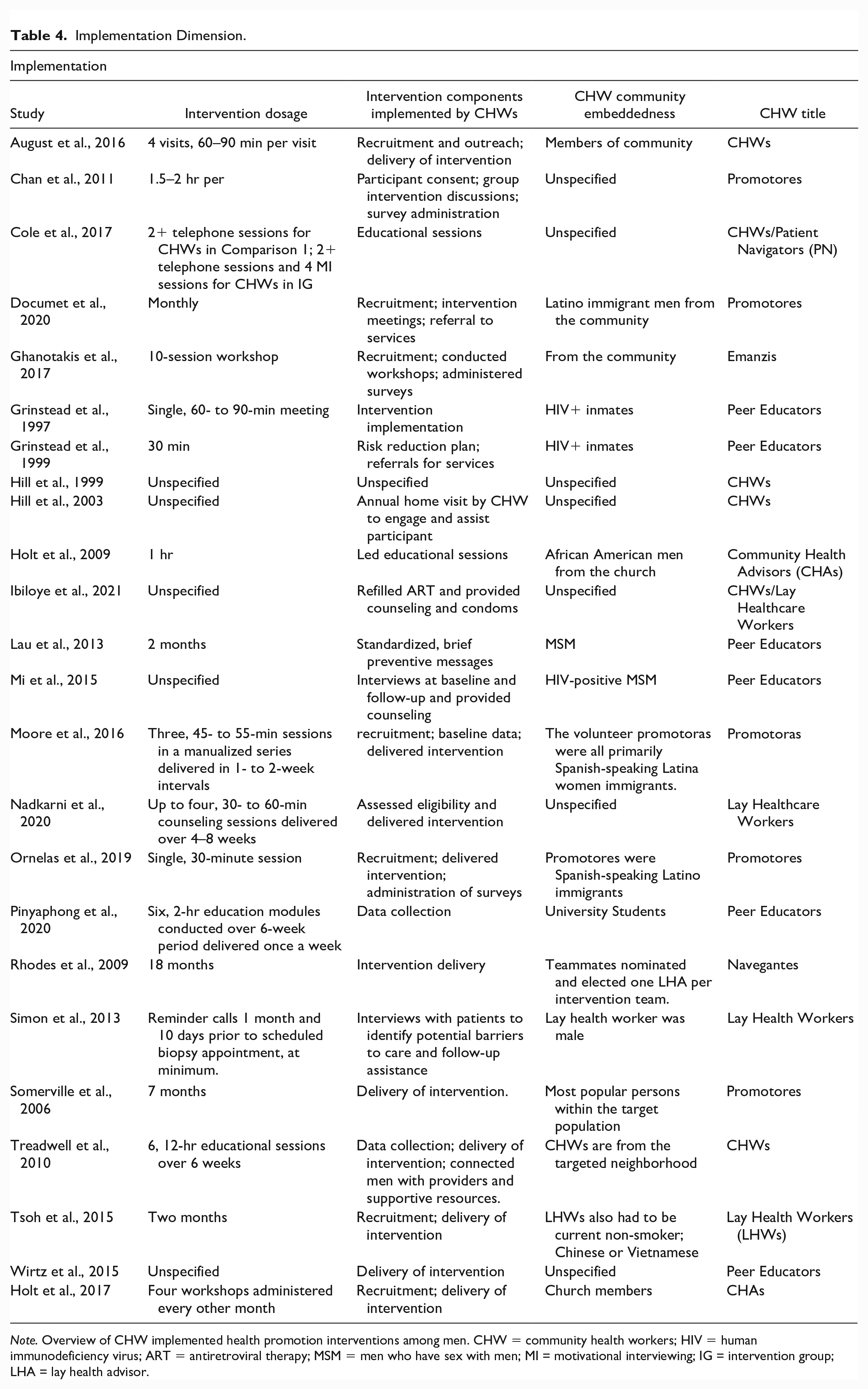
Note. Overview of CHW implemented health promotion interventions among men. CHW = community health workers; HIV = human immunodeficiency virus; ART = antiretroviral therapy; MSM = men who have sex with men; MI = motivational interviewing; IG = intervention group; LHA = lay health advisor.
Implementation (Continued) and Maintenance dimension.
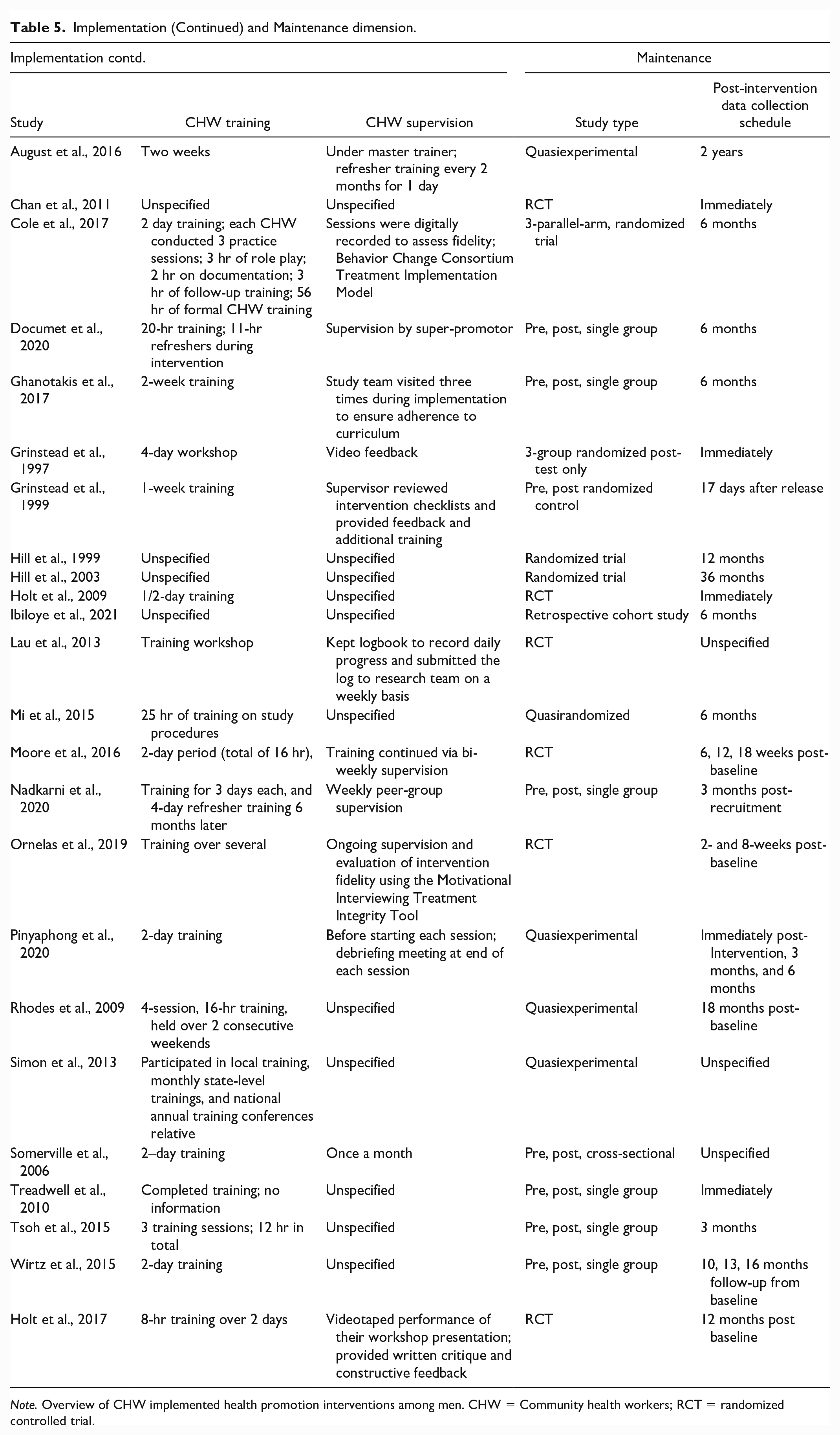
Note. Overview of CHW implemented health promotion interventions among men. CHW = Community health workers; RCT = randomized controlled trial.
Maintenance Dimension
Data extracted that align with the Maintenance dimension are schedules of post-intervention data collection of health outcomes (see Table 5).
Retention Rates
Retention rates for intervention groups were available for a total of 18 studies and ranged from 48.90% to 100%. Retention rates for comparison groups were available for a total of nine studies and ranged from 69.74% to 100%. It should be noted that time periods varied. See Supplemental File 4 for more information.
Discussion
This scoping review is the first to focus exclusively on health promotion efforts conducted by CHWs targeting various facets of men’s health promotion. Despite the fact that CHW programs date back to the 1920s and have a unique potential to promote men’s health, this scoping review found only 24 interventions that met the inclusion criteria (Perry et al., 2014). The data extracted from these studies were presented using the RE-AIM Framework to inform future efforts to promote health among men implemented by CHWs.
The reach of the interventions was varied as indicated by the mean age of participants, inclusion criteria, and recruitment and retention rates. Two noteworthy results with regard to reach emerged from the present review: (a) most of the CHW-implemented interventions targeted underserved men (e.g., Hispanic men, Black men, inmates, men who have sex with men) and (b) retention rates were satisfactory. Rigorous reviews have confirmed that CHWs are well-suited to promote health among underserved populations (Perry et al., 2014), and the present review confirms that CHW-implemented interventions can be effective in promoting health among underserved men. Furthermore, given that many health promotion efforts have difficulty retaining men, particularly underserved men, it should be noted that the retention rates were satisfactory. The overwhelming majority of the interventions were below the threshold that signals a high risk of bias from baseline to post-intervention evaluation (20% loss of participants from pre- to post-intervention (Schulz & Grimes, 2002).
Most of the interventions resulted in an ability to effectively improve the primary targeted health concern. With that being the case, it is significant that the vast majority of interventions were based on self-report data—an approach that can result in a high risk of bias, particularly if participants are not blinded to the outcome. The data also indicate that the vast majority of efforts targeted colorectal cancer screening or sexual health practices. Notably absent are efforts that target mental health concerns, given that holistic approaches have been advocated for some underserved groups of men (Wippold et al., 2021a). The results also indicate that most interventions were adopted in a community-based setting, which aligns with qualitative research indicating that men prefer community-based health programming (Oliffe et al., 2020). Significant results with regard to adoption were the (1) lack of theoretical framework/model for many of the interventions and (2) use of formative research among members of the target community to develop the intervention. The first represents a concerning limitation and the second represents a strength.
As with the other RE-AIM outcomes, the implementation of the interventions varied. The data indicate that the CHWs conducted a wide-range of intervention activities, ranging from participant recruitment to data collection. There are three noteworthy implementation-related findings. First, many interventions described the embeddedness of the CHW (i.e., how well the CHW’s demographics matched the demographics of the targeted participants). Research suggests that men prefer a higher degree of embeddedness (Lefkowich & Richardson, 2018; Sharp et al., 2018). Second, most of the CHWs were trained by the researchers and the trainings were well-described. Future similar interventions can build off these trainings. Third, there was limited information on the supervision of the CHWs once their roles as implementers started. The first and final implementation-related finding may be an artifact of limited space when reporting the results of the interventions in peer-reviewed journals, though suggest that more attention is needed to intentionally ensure CHW embeddedness and for ongoing supervision of CHWs during the implementation of the intervention.
In addition to the recommendations embedded throughout this section (e.g., need for more rigorous designs and information on CHW supervision), there are ample literature-informed opportunities to enhance CHW-implemented interventions seeking to improve health among men. These opportunities include the need for multi-level interventions and interventions that explicitly help increase men’s awareness of how the ways they define and demonstrate their gender ideals have implications for their health. CHWs also are uniquely positioned to model manhood and other prosocial masculinities that can be sources of motivation to promote health. These two recommendations will contribute to sustainable health programming and acknowledge that health promotion is dynamic and ongoing. In addition, the last recommendation marks an intentional deviation from traditional deficit-based lens of men’s health.
Strengths and Limitations
The results and recommendations of this scoping review should be viewed in light of its strengths and limitations. The methods for data acquisition were rigorous—the authors pre-registered the protocol, consulted with a research librarian when creating the search terms, acquired articles from five search engines and one grey-literature search engine, and each article was blindly assessed for inclusion by GMW and KAG. Discrepancies were blindly resolved by SGF. In addition, evidence was synthesized by all authors, including DMG—an expert in men’s health promotion. Despite these strengths, there are some noteworthy limitations. First, the present review has the limitations often levied against scoping reviews. That is, the present review does not assess methodological rigor of the included interventions and does not quantitatively synthesize findings to calculate an overall effect—characteristics of systematic reviews and meta-analyses. Despite this being the case, the present scoping review provides a foundation for these other types of reviews. Second, only three studies reported an effect size, all of which were small. Third, the present review is likely limited by the publication bias. It is probable that national and international CHW organizations are conducting men’s health promotion efforts that are not published in peer-reviewed journals or grey literature repositories.
Implications and Conclusion
The results of the present review have implications for prevention and health promotion programs. First, implementation of CHW-led interventions may be a viable strategy to promote health and prevent adverse health outcomes among men—a group that has traditionally been underserved by health promotion specialists. Such interventions will benefit from gender tailoring to prosocial masculinities by assuming a strengths-based lens by incorporating and building on existing research that has identified health promotion facilitators among men. This approach constitutes a novel strategy to promote men’s health. Second, the training of CHWs in future efforts can build on training programs used by previous health promotion efforts, though it should be noted that attention should be given to the supervision of these CHWs. Finally, opportunities exist to address a diversity of health-related factors, including mental health, and determinants of health such as racism and discrimination.
Efforts are needed to improve healthy life expectancy among men. It is widely recommended that to improve recruitment, retention, and outcomes, such efforts must be tailored to the unique psychosocial factors that impact the health and health promotion of men. The present scoping review is the first to collate, summarize, and synthesize health promotion efforts for men that were implemented by CHWs—a workforce that aligns well with the health promotion preferences of men, are scalable, and cost-effective. The results of the present review highlight the importance of CHW-implemented health promotion efforts targeting men. Efforts implemented by CHW to improve health among men are scalable strategy that can promote recruitment, retention, and health-related outcomes.
Supplemental Material
sj-docx-1-heb-10.1177_10.1177_10901981231179498 – Supplemental material for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework
Supplemental material, sj-docx-1-heb-10.1177_10.1177_10901981231179498 for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework by Guillermo M. Wippold, Kaylyn A. Garcia, Sarah Grace Frary and Derek M. Griffith in Health Education & Behavior
Supplemental Material
sj-docx-2-heb-10.1177_10.1177_10901981231179498 – Supplemental material for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework
Supplemental material, sj-docx-2-heb-10.1177_10.1177_10901981231179498 for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework by Guillermo M. Wippold, Kaylyn A. Garcia, Sarah Grace Frary and Derek M. Griffith in Health Education & Behavior
Supplemental Material
sj-docx-3-heb-10.1177_10.1177_10901981231179498 – Supplemental material for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework
Supplemental material, sj-docx-3-heb-10.1177_10.1177_10901981231179498 for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework by Guillermo M. Wippold, Kaylyn A. Garcia, Sarah Grace Frary and Derek M. Griffith in Health Education & Behavior
Supplemental Material
sj-docx-4-heb-10.1177_10.1177_10901981231179498 – Supplemental material for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework
Supplemental material, sj-docx-4-heb-10.1177_10.1177_10901981231179498 for Community Health Worker Interventions for Men: A Scoping Review Using the RE-AIM Framework by Guillermo M. Wippold, Kaylyn A. Garcia, Sarah Grace Frary and Derek M. Griffith in Health Education & Behavior
Footnotes
Acknowledgements
The authors would like to acknowledge Ms. Kristina Schwoebel, MA, Sciences and Computing Librarian at the University of South Carolina for input and consultation on the search strategy.
Authors’ Contributions
Guillermo M. Wippold: Conceptualization, Methodology, Resources, Data Curation, Writing—Original Draft, Writing—Review & Editing, Supervision, Funding Acquisition; Kaylyn A. Garcia: Conceptualization, Methodology, Data Curation, Writing—Original Draft, Writing—Review & Editing, Visualization; Sarah Grace Frary: Conceptualization, Methodology, Data Curation, Writing—Review & Editing; Derek M. Griffith: Writing—Original Draft, Writing—Review & Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Guillermo M. Wippold was funded by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under award number K23MD016123. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Kaylyn A. Garcia has no financial disclosures. Sarah Grace Frary has no financial disclosures. Dr. Derek M. Griffith has no financial disclosures.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.