
Abstract
Objective
Adverse childhood experiences (ACEs), which refer to childhood traumatic events, have been identified as risk factors for tobacco use in adulthood. However, studies are limited on the effect of sex on the association of ACEs with e-cigarettes and dual use of e-cigarettes and cigarettes. This study explored sex differences in the association of ACEs with e-cigarettes, cigarettes, and dual use of e-cigarettes and cigarettes among adults in the United States.
Methods
This was a cross-sectional analysis of data from adults aged ≥18 years in the 2020 Behavioral Risk Factor Surveillance System (N = 62,768). ACEs, the independent variable, was a composite score assessed from 11 questions (with responses yes—1 or no/never—0) related to childhood emotional abuse, physical abuse, sexual abuse, and household dysfunction and categorized as 0 (reference), 1, 2, 3, or ≥4. The dependent variable, tobacco use patterns, included nonuse (reference), e-cigarette only, cigarette only, and dual use of e-cigarettes and cigarettes. Multinomial logistic regression was performed to test the interaction between sex and ACEs while controlling for potential confounders.
Results
Although we found no statistically significant interaction by sex, a greater number of ACEs were associated with higher odds of the different tobacco use patterns among females and males, with varying strengths of associations. Specifically, females who reported ≥4 ACEs compared with none had higher odds of e-cigarette (aOR [95% CI]: 3.58 [1.49–8.63]), cigarette (2.57 [1.72–3.83]) and dual use (3.25 [1.79–5.91]) relative to nonuse. Males with ≥4 ACEs had higher odds of cigarette (1.75 [1.15–2.65]) and dual use (7.64 [3.95–14.79]).
Conclusion
Our findings underscore the importance of developing appropriate, tailored trauma-informed intervention strategies for females and males. It is also important to consider ACEs in designing tobacco-specific preventive programs to curb initiation and promote cessation among U.S. adults.
Highlights
Explored sex differences in the association of ACEs with e-cigarettes, cigarettes, and dual use of e-cigarettes/cigarettes.
Sex did not significantly modify the association betweeen ACEs and the tobacco use patterns.
Greater number of ACEs were associated with higher odds of the different tobacco use patterns among females and males, with varying strengths of associations.
Appropriate trauma-informed intervention strategies for females and males should be considered when designing tobacco-specific prevention programs.
Introduction
Globally, and in the United States, tobacco remains a major cause of disease and disability (Cornelius et al., 2020; National Center for Chronic Disease Prevention and Health Promotion [NCCDPHP] (US) Office on Smoking and Health, 2014). In the past three decades, the United States has recorded significant declines in the prevalence of smoking in the general population (National Center for Chronic Disease Prevention and Health Promotion [NCCDPHP] (US) Office on Smoking and Health, 2014; Cornelius et al., 2020), and more focus is now targeted toward populations at the highest risk for persistent smoking. These populations comprise people who use substances, individuals with mental health problems, and those with co-occurring problematic substance use and poor mental health (Weinberger et al., 2020; Winhusen, 2017). Several studies have identified proximate risk factors that can increase the risk of both problematic substance use and poor mental health, which drive tobacco use (Rogers et al., 2022). One of these factors is adverse childhood experiences (ACEs) which includes events related to parental mental illness, domestic violence, alcoholism, emotional, physical, and sexual abuse in childhood (Hughes et al., 2017; Hughes et al., 2019; Krinner et al., 2020; Mersky et al., 2013; Rogers et al., 2022). ACEs can affect mental and behavioral health outcomes, including tobacco use, across the life course (Hughes et al., 2017; Rogers et al., 2022).
ACEs have been conceptualized as a series of stressors resulting from adverse childhood psychological, sexual, and physical abuse, as well as an experience of parental substance misuse, mental illness, domestic violence, and incarceration (Cosanella et al., 2019). Several studies have shown the association between ACEs and tobacco use (Anda et al., 1999, 2006; Bellis et al., 2014; Campbell et al., 2016; Cosanella et al., 2019; Felitti et al., 1998; Ford et al., 2011; Vander Weg, 2011). For example, one of the earliest studies on ACEs demonstrated that a high ACE score was linked with an increased likelihood of cigarette smoking in adolescence and chronic smoking patterns in adulthood (Felitti et al., 1998). The relationship identified in this study (Felitti et al., 1998), and subsequent studies might be explained by the self-medication theory, which suggests tobacco smoking may be a response to trauma and affective distress following exposure to ACEs (Baiden et al., 2022; Deighton et al., 2018; Dragan, 2020; Manyema et al., 2018). In addition, ACEs may trigger changes in the functioning and physiology of the brain leading to defective mood and behavioral self-regulation which heightens the vulnerability for maladaptive coping behaviors such as tobacco use (Anda et al., 1999, 2006; Ford et al., 2011).
ACEs are prevalent, with 60% of adults reporting at least one ACE (CDC, 2015; Cosanella et al., 2019) during their lifetime, and the prevalence is concentrated in certain demographic groups (Rogers et al., 2022). For example, females have a higher prevalence of ACEs than males, particularly regarding sexual abuse (Rogers et al., 2022). Likewise, racial minorities and those residing in low-income neighborhoods have reported a higher prevalence of ACEs (Rogers et al., 2022). Thus, the relationship between ACEs and smoking is especially concerning because of the relatively high rates of ACEs exposure in the population and its concentration in select demographic groups (e.g., females), which can exacerbate the heightened risk of tobacco use.
Several studies have explored the relationship between ACEs and tobacco use and the moderating effect of sex and mainly report no significant differences (Cosanella et al., 2019; Grigsby et al., 2020; Mersky et al., 2013; Rehkopf et al., 2016; Topitzes et al., 2010). However, these studies have several limitations. First, some of these studies lack generalizability as they did not use a nationally representative sample (Cosanella et al., 2019; Topitzes et al., 2010). Second, an earlier study using a generalizable sample (Rehkopf et al., 2016) excluded sexual abuse from the measures of adverse childhood experience, and sexual abuse is highly correlated with ACEs among females. Finally, studies are sparse on the relationship between ACEs and e-cigarette use among adults. A prior study conducted among young women in Australia found a dose-response relationship between ACE score and e-cigarette use (Melka et al., 2019). With the decline in cigarette use and increase in alternative tobacco product such as e-cigarettes, the dual use of e-cigarettes and cigarettes are a prevailing pattern of tobacco use, given that some adults use e-cigarettes for cessation purposes (McRobbie et al., 2014; Rahman et al., 2015). There remains a gap in the literature on the extent to which the relationship of ACEs with e-cigarettes and the dual use of e-cigarettes and cigarettes differs by sex in a nationally representative sample after controlling for other demographic factors such as age and race/ethnicity. This study examines sex differences in the association of ACEs with e-cigarettes, cigarettes and the dual use of both products among adults in the United States using a nationally representative sample. The findings from this study are essential to public health, as it explores how sex might interact with the relationship between ACEs and tobacco smoking. Understanding this relationship can, in turn, shape targeted interventions with proper consideration for risk factors such as sex in tobacco control.
Methods
Study Population
We conducted a cross-sectional analysis of 62,768 adults from the 2020 Behavioral Risk Factor Surveillance System (BRFSS) public-use data files. A detailed methodology and sampling procedures of the BRFSS dataset have been previously explained (CDC, 2020). The BRFSS is conducted in the 50 states in the United States, the District of Columbia, and other U.S. territories. Briefly, the BRFSS is a cross-sectional survey designed and conducted by the CDC (2020) to collect data on chronic health conditions, health-related risk behaviors, and use of preventive behaviors from U.S. noninstitutionalized adults aged 18 years and older. Standardized questionnaires were administered to a representative sample of adults via landline telephone.
ACEs
ACEs, the independent variable, was assessed from 11 questions related to childhood emotional abuse, physical abuse, sexual abuse, and household dysfunction prior to 18 years of age. The items included (a) how often did a parent swear at you, insult you, or put you down? (b) How often did a parent or adult in your home physically hurt you (excluding spanking)? (c) How often did anyone ever touch you sexually? (d) How often did anyone make you touch them sexually? (e) How often did anyone ever force to have sex? (f) Were your parents divorced/separated? (g) How often did your parents beat each other? (h) Did you live with anyone who was depressed, mentally ill, or suicidal? (i) Did you live with anyone who was a problem drinker or alcoholic? (j) Did you live with anyone who served time or was sentenced to serve time in a prison, jail, or other correctional facility? (k) did you live with anyone who used illegal street drugs or who abused prescription medications? For each of the above questions, dummy variables were created, coded as “0” if the participant answered “never” or “no” and “1” if the participant reported in the affirmative. An ACE composite score was calculated using affirmative responses ranging from 0 to 11 and categorized as 0, 1, 2, 3, or ≥4, consistent with previous literature (Baiden et al., 2022; Craner et al., 2022; Felitti et al., 1998; Hu et al., 2021; Melka et al., 2019).
Tobacco Use Patterns
Tobacco use patterns, that is, nonuse, current e-cigarette use only, current cigarette use only, and current dual use of e-cigarettes and cigarettes, were the dependent variable and were assessed from questions related to cigarette and e-cigarette use. Current cigarette use was assessed from the question of having smoked at least 100 cigarettes in their entire lifetime and if participants were smoking some days or every day (Cornelius et al., 2022). Participants who reported using e-cigarettes on some days or every day were classified as current e-cigarette users. Nonusers of either cigarettes or e-cigarettes were those who responded “No” to having smoked at least 100 cigarettes in their entire lifetime and “No” to the ever use of e-cigarettes. Dual use was defined as the concurrent use of both cigarettes and e-cigarettes.
Covariates
We included the following variables: age (18–24, 25–34, 35–44, and ≥45 years), race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Other, non-Hispanic Multiracial, and Hispanic), marital status (single, divorced/widowed/separated and married/partnered), income (< $25,000, $25,000 to <$50,000, ≥$50,000) and educational attainment (high school or below, attended college/technical school, graduated college/technical school). Additionally, we included past-month marijuana use and heavy alcohol consumption- Yes/No, current smokeless tobacco use (every day/some days, not at all), as prior research has shown associations with ACEs and substance use in adulthood (Kisely et al., 2020a, 2020b). We also included depression (“Ever told you had a depressive disorder, including depression, major depression, dysthymia, or minor depression”—Yes/No) and the number of days mental health was not good; which assesses stress, depression, and problems with emotions in the past 30 days; and was categorized in BRFSS as 0, 1–13, and ≥14 days (CDC, 2020).
Statistical Analysis
All analyses were performed using STATA version 17 (StataCorp LP, College Station, TX) and were conducted between May 2022 and April 2023. The characteristics of the study population were analyzed, and the weighted prevalence was reported overall and by sex. Unadjusted and adjusted multinomial logistic regression models were used to assess the associations of the tobacco use patterns (dependent variable, that is, nonuse [reference], current e-cigarette use, current cigarette use, and current dual use of e-cigarette and cigarette) with ACEs with “0” as the reference group (independent variable). We adjusted the models for demographic factors (age, race/ethnicity, education, income, marital status), past-month marijuana use, heavy alcohol consumption, current smokeless tobacco use, depression, and number of days mental health was not good. We tested for effect modification by sex and presented models stratified by sex. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported for the associations of ACEs with the tobacco use patterns. Sampling weights were utilized in all analyses to account for the complex features of the BRFSS survey design. The significance level was set at an alpha level of .05 and considered in the context of other evidence, such as the strength and magnitude of associations and measures of variability. Because BRFSS is publicly available de-identified data, it is deemed exempt from Florida International University Institutional Review Board (IRB) review.
Results
The characteristics of study participants (N = 62,768) varied by sex, as reported in Table 1, except for race/ethnicity and education. Females had a lower prevalence of e-cigarette use only (1.8% vs. 3.0%), cigarette use only (7.3% vs. 13.0%), and dual use (2.3% vs. 4.0%), compared with their male counterparts, respectively (p < .0001).
Characteristics of Study Participants.
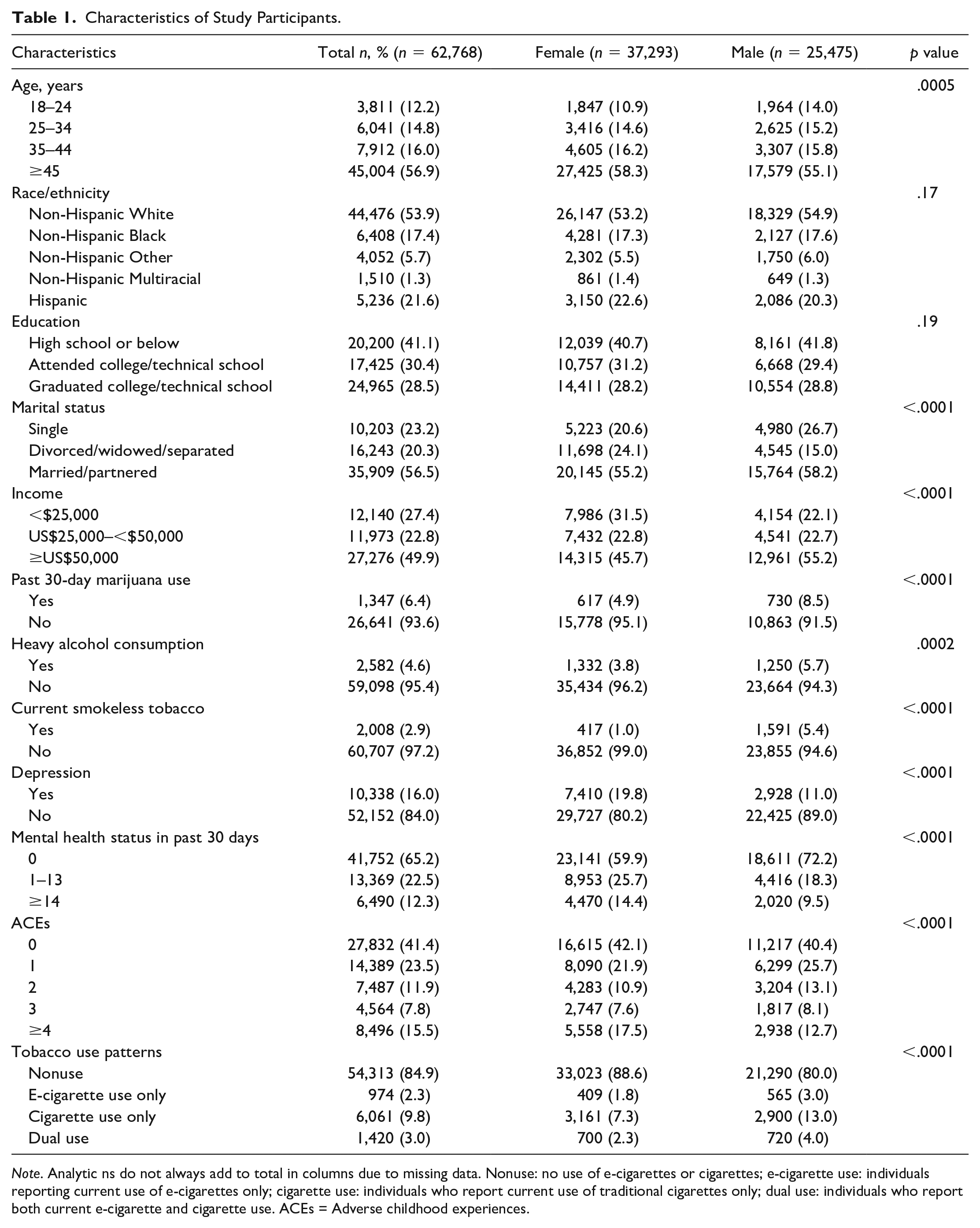
Note. Analytic ns do not always add to total in columns due to missing data. Nonuse: no use of e-cigarettes or cigarettes; e-cigarette use: individuals reporting current use of e-cigarettes only; cigarette use: individuals who report current use of traditional cigarettes only; dual use: individuals who report both current e-cigarette and cigarette use. ACEs = Adverse childhood experiences.
Interactions of sex with ACEs were not statistically significant (e-cigarette only, p = .417; cigarette only, p = .154; dual use, p = .145). Table 2 shows the associations between ACEs and tobacco use patterns among females and males. In the unadjusted model, females with ACEs had higher odds of e-cigarettes, cigarettes, and dual use. For example, females with three ACEs and ≥4 ACEs had higher odds of e-cigarette use (OR: 9.68 [95% CI: 5.16–18.16] and OR: 13.15 [95% CI: 7.44–23.23]) compared with those without any ACEs. Similarly, females who reported three ACEs and ≥4 ACEs had higher odds of cigarette (OR: 1.68 [95% CI: 1.17–2.39] and OR: 2.88 [95% CI: 2.18–3.81]), and dual use (OR: 4.67 [95% CI: 2.17–10.07] and OR: 11.43 [95% CI: 5.86–22.28]), respectively. These associations were attenuated in the adjusted model; females with three ACEs and ≥4 ACEs had higher odds of cigarette (aOR: 2.11 [95% CI: 1.29–3.44] and aOR: 2.57 [95% CI: 1.72–3.83]), and dual use (aOR: 2.76 [95% CI: 1.30–5.86] and aOR: 3.25 [95% CI: 1.79–5.91]), respectively. Females with ≥4 ACEs had higher odds of e-cigarette use (aOR: 3.58 [95% CI: 1.49–8.63]). We found no statistically significant association for females with three ACEs and e-cigarette use (aOR: 2.43 [95% CI: 0.92–6.39]).
Association Between Number of Adverse Childhood Experiences and Tobacco Use Patterns.
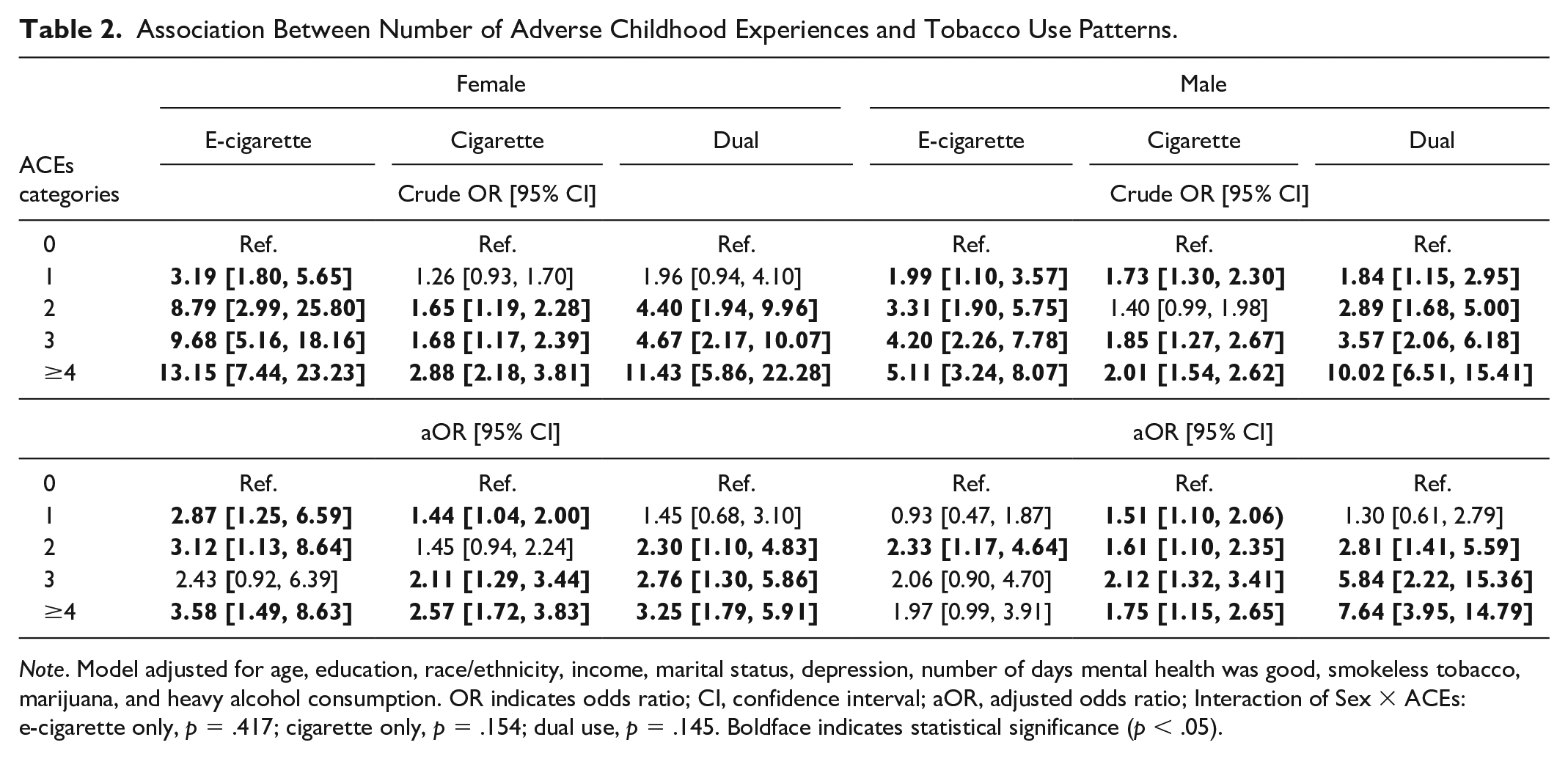
Note. Model adjusted for age, education, race/ethnicity, income, marital status, depression, number of days mental health was good, smokeless tobacco, marijuana, and heavy alcohol consumption. OR indicates odds ratio; CI, confidence interval; aOR, adjusted odds ratio; Interaction of Sex × ACEs: e-cigarette only, p = .417; cigarette only, p = .154; dual use, p = .145. Boldface indicates statistical significance (p < .05).
Results were qualitatively similar for males in the unadjusted model, where males with three ACEs and ≥4 ACEs had higher odds of e-cigarette use (OR: 4.20 [95% CI: 2.26–7.78] and OR: 5.11 [95% CI: 3.24–8.07]). Similarly, males who reported three ACEs and ≥4 ACEs had higher odds of cigarette use (OR: 1.85 [95% CI: 1.27–2.67] and OR: 2.01 [95% CI: 1.54–2.62]), and dual use (OR: 3.57 [95% CI: 2.06–6.18] and OR: 10.02 [95% CI: 6.51–15.41]), respectively. These associations were attenuated in the adjusted model; males with three ACEs and ≥4 ACEs had higher odds of cigarette use (aOR: 2.12 [95% CI: 1.32–3.41] and aOR: 1.75 [95% CI: 1.15–2.65]). Likewise, males with three ACEs and ≥4 ACEs had higher odds of dual use (aOR: 5.84 [95% CI: 2.22–15.36] and aOR: 7.64 [95% CI: 3.95–14.79]). We found no statistically significant associations among males for three ACEs and ≥4 ACEs with e-cigarette use (aOR: 2.06 [95% CI: 0.90–4.70] and aOR: 1.97 [95% CI: 0.99–3.91], respectively).
Discussion
This study examined the differences by sex in the association between ACEs and tobacco use patterns. Our findings suggest that females with an ACE score of ≥3 had significantly higher odds of exclusive cigarette and dual use (cigarette and e-cigarette), compared with those with an ACEs score of 0. Likewise, males with an ACEs score of ≥3 had higher odds of exclusive cigarette and dual use.
In this study, females had a higher proportion reporting an ACE score of ≥4 compared with males. Tobacco use patterns were consistently lower in females compared with males. These findings align with prior studies examining ACEs and tobacco use distributions by sex (Anda et al., 2006; Cosanella et al., 2019; Mersky et al., 2013; Rehkopf et al., 2016; Rogers et al., 2022). For example, Rehkopf et al. (2016) demonstrated that in the three dimensions of ACEs (physical abuse, parental mental illness, and parental alcohol abuse) examined in their study, females consistently reported more ACE-related events than males. However, our findings contrast with a prior study (Grigsby et al., 2020), which reported a stronger relationship among males between ACEs and e-cigarette use. Our results suggest no association between ACEs and e-cigarette use in males. The difference in results might be because of the variation in the populations sampled. We used a national adult sample from the BRFSS, while Grigsby et al., who identified a stronger relationship among males between ACEs and subsequent e-cigarette use, focused on adolescent and young adult college students in California (Grigsby et al., 2020).
Furthermore, our study found no significant moderating effect of sex on the relationship between ACE scores and tobacco use patterns. The current findings align with most studies that indicate no sex differences in the association between ACEs and tobacco use (Anda et al., 1999; Choi et al., 2017; Grigsby et al., 2020; Mersky et al., 2013; Rehkopf et al., 2016; Topitzes et al., 2010). These findings can be explained by the self-medication theory, which posits that an individual’s response to emotional or psychological distress and their choice to use a particular substance is based on their subjective affect regulation (Khantzian, 1997) and findings may also be due to differences in coping approaches and resilience between the sexes. Prior studies suggest that males are more likely to engage in externalizing behaviors to cope with affective distress, leading to medicating with substances like tobacco (Gajos et al., 2023; Rogers et al., 2022). Conversely, females are more likely to experience (or report) internalizing symptoms that can increase affective distress, which is also medicated with tobacco use (Matud, 2004; Mel’endez et al., 2012). Another plausible explanation is that the association between ACEs and smoking, as moderated by sex differences, might be related to specific ACE categories. However, the current study aggregated ACEs scores (0, 1, 2, 3 and ≥4) and did not adjust for differences in ACE categories. Thus, potential sex-specific relationships might have been missed in this study. Nevertheless, the literature suggests that people who experience stress and anxiety use nicotine/tobacco products for mood modulation (Cosci et al., 2011). Therefore, those who are exposed to ACEs may use nicotine/tobacco products to control their undesirable mood states later in life, regardless of their sex.
Our results can potentially support prevention programs aimed at screening for ACEs in the population. In addition, the high prevalence of ACEs, particularly severe experiences of ACEs with scores of three or more, suggests the importance of designing interventions with sex-sensitive messaging to increase awareness and preventive practices to mitigate ACEs at the household and community level. Therefore, these interventions that prevent ACEs may help to further curb tobacco use. Similarly, because individuals with a history of ACEs may have traumatic origins for their tobacco use, interventions among tobacco users may help address underlying trauma (Alcalá et al., 2016). Also, future longitudinal studies can explore how sex differences might moderate the relationship between ACEs at different developmental stages and subsequent tobacco use in the US population and globally.
This study has some limitations. First, because of the cross-sectional analysis, we are unable to draw causal conclusions between ACEs and the tobacco use patterns examined in this study, though it is important to note that the ACEs variable assessed events that occured in the past. Future studies that utilize multiple waves may be useful in establishing a temporal association between ACEs and the tobacco use patterns examined. Prior longitudinal studies on ACEs and cigarettes found similar associations as observed in the current study (Kisely et al., 2020a). Second, responses were self-reported, so may be subject to recall bias, which may result in an underestimation of the ACEs and the true strength of the association between ACEs and tobacco use patterns. Nevertheless, although the validity of self-reported ACEs needs to be explored further, self-reported tobacco status correlates highly with serum cotinine levels (Caraballo et al., 2001). Third, ACEs are often portrayed as count variables given their complexity and it may not reflect their severity or impact (Craner et al., 2022). Likewise, categorizing ACE variables (such as the maltreatment variables) originally asked as frequencies are debatable as to whether an ever or never experience is the best measure, as results suggest that measuring maltreatment severity may be a more optimal approach (Litrownik et al., 2005). Finally, the BRFSS survey is limited to adults who are not institutionalized and have access to a phone; therefore, it excludes those who were incarcerated or homeless who may be more vulnerable to ACEs, thus, limiting the generalizability of this study. Despite these limitations, this study contributes to the existing literature by examining sex differences in the relationship between ACEs and tobacco use among a sample of U.S. adults and has significant implications.
Conclusion
In conclusion, this study adds to the literature examining the effect of sex on the relationship between ACEs and tobacco use. Our findings validate the link between ACEs and tobacco use, specifically, exclusive cigarette and dual tobacco use in adulthood in a nationally representative sample in the United States. Although we found no moderating effect of sex on ACEs and tobacco use, our results build on prior studies by going further to examine the relationship between ACEs and dual use (concurrent cigarette and e-cigarette use), which is increasingly prevalent among young adults in the United States. In addition, we explored a broad measure of ACEs using 11 constructs that are validated in the BRFSS. Overall, these findings support the importance of screening for ACEs and developing specific interventions with consideration for both females and males. Interventions that take into account the influence of ACEs on tobacco use behaviors are critical, given the risk for dependency and addiction associated with tobacco use, to reduce tobacco-related morbidity and mortality in the overall population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Z.B. was supported by FIU-Research Center in Minority Institution (Grant U54MD012393-01). Other authors have no funding to declare.