
Abstract
Racial health inequities persist despite many attempts to correct them. Inadequate comprehension of racism obscures the ordinariness of racism in public health institutions. In addition to applying critical race theory (CRT) to the research and practice of public health, we argue that the struggle for health equity must also apply CRT toward the teaching of public health students. Adhering to conventional approaches in academic public health without grappling with their roots in Whiteness reproduces a public health workforce that is insufficiently equipped to address the complex, systemic issues underlying health inequities. By default, academic public health excludes the perspectives of scholars of color, relies too heavily on theories of individual behavior, and applies top-down teaching methods. To make durable changes, the rising generation of public health scholars and practitioners must understand how health equity fits within broader struggles for racial and social justice. Thus, we critique three responsibilities for teaching about public health: assigning readings, shaping analytical lenses with theories, and modeling change through andragogy. By questioning whose knowledge is legitimized when defining public health needs, whose lenses are used to prioritize solutions, and whose insights drive change, we can train a public health workforce more critical of racism, and more prepared to deal with the enduring reality of racial relations.
“Reality is not fixed, not a given. Rather, we construct it through conversations, through our lives together.”—Richard Delgado, 1989
In 2021, public health organizations throughout the United States declared racism “a serious public health threat” in response to the Movement for Black Lives (Walensky, 2021). However, Black, Indigenous, and People of Color (BIPOC) scholars have articulated this stance for decades (Williams & Collins, 1995). What stalls racism-conscious practice?
One postulation is the lack of training on racism (Shaw-Ridley & Ridley, 2010). Spurred by student-led efforts at the University of Washington, discussing racism as a challenge to health equity was formalized as a Master of Public Health (MPH) competency for accreditation by the Council on Education for Public Health in 2016 (Hagopian et al., 2018). Still, schools and programs of public health inadequately prepare graduates for anti-racist public health research and practice (Cross, 2018; Komro et al., 2018).
Critical race theory (CRT) prompts us to ask why racial health inequities persist. While Public Health Critical Race Praxis (PHCRP) guides the research and practice of public health (Ford et al., 2019), we argue that examining the teaching of public health students can broaden our understanding of the struggle for health equity. Guided by CRT of education (Delgado, 1989; Delgado Bernal & Villalpando, 2002; Yosso, 2005), we, as racial health equity scholars, question whose knowledge is taught in public health.
Racism, Whiteness, and CRT of Education
Racism systematically benefits White supremacy at the expense of BIPOC (C. P. Jones, 2018). This racial hierarchy is upheld, in part, by curtailed disciplinary self-critique (Bowleg, 2021; Liburd et al., 2019). We invoke the five tenets from CRT of education (Solórzano & Yosso, 2001) to elucidate academic public health’s entanglements with racism.
1. The centrality of race and racism and their intersectionality with other forms of subordination. CRT addresses racism as the primary form of oppression which, interacting with patriarchy and capitalism, stratifies access to education, wellness, and economic security. The challenge of training racism-conscious public health graduate students becomes clearer upon acknowledging long-held racist views in public health history. For example, public health concerns regarding the “hybrid of the most despicable, a mongrel of the most detestable that has ever afflicted the earth” (Volpp, 2000, pp. 801–802) justified bans on interracial marriage. Similar depictions of non-White people as biologically inferior substantiated eugenic policies, such as exclusionary immigration and forced sterilizations (Chowkwanyun, 2011; Stern, 2005). Thus, dismantling racism demands confronting contemporary public health fundamentals developed through racist legacies.
2. The challenge to dominant ideology. The racial hierarchy which positions White people above others is perceived as natural (Bonilla-Silva, 1997, 2012). Legal scholar Cheryl Harris (1993) described the essence of Whiteness as “the legal legitimation of expectations of power and control that enshrine the status quo as a neutral baseline, while masking the maintenance of white privilege and domination” (p. 1715). This baseline is achieved through “centering,” the dynamic where certain perspectives, most often those of White cismen (whose gender identity aligns with assigned sex at birth), are upheld as the “norm” by which others are compared (J. M. Jones, 1988).
CRT renders the hidden structures that maintain racial hierarchy more visible to facilitate their undoing. Defaulting to Whites as the “reference group” in disparities research implies White is normative (C. P. Jones et al., 1991) which obscures the health advantages conferred by White privilege (Sullivan, 2014). Consider the situation where a professor describes the readings on the Framingham cohort as “classics,” and then talks about Tongans as “culturally different” and “underprivileged.” Alternatively, they could have referred to White people and culture as “privileged” (Yosso, 2005). However, doing so feels odd because it disrupts the prevailing assumption that minoritized communities are deviant.
3. The commitment to social justice. CRT emphasizes dismantling racism and other root causes of inequities. By generating a shared understanding of reality, CRT facilitates the conditions to transform society (Delgado, 1989). Critical educators develop students’ critiques of oppression and motivation for social justice to collaboratively engage in transformational resistance (Solórzano & Bernal, 2001).
4. The centrality of experiential knowledge. CRT values lived experience. The margins refer to a social location wherein BIPOC communities generate unique perspectives on oppression and resistance (Hooks, 1990; Sweet, 2020). However, public health enthusiasm for collecting data from BIPOC communities overshadows support for investing in students from BIPOC communities as prospective researchers (Pasick et al., 2012). Notwithstanding modest increases in the percentage of BIPOC doctoral graduates, centering inimitable insights from BIPOC students and scholars in the predominantly White field of public health remains a struggle (Goodman et al., 2020; Pasick et al., 2012).
5. The transdisciplinary perspective. CRT provides sociopolitical and historical context to health inequities by drawing from multiple disciplines, including law, history, ethnic, and gender studies (Solórzano & Yosso, 2001). While civil rights, multiculturalism, and health disparities approaches superficially reform the status quo in law, education, and public health, respectively, the CRT perspective argues for radical transformation of these systems (Bell, 1980; Ford & Airhihenbuwa, 2018; Ladson-Billings & Tate, 1995; Solórzano & Bernal, 2001).
CRT of education clarifies how teaching conventionally centers Whiteness as the unquestioned standard. Its tenets inform our critique of common teaching responsibilities as everyday opportunities for advancing health equity. To eliminate racial health inequities, public health educators must deliberately transform teaching to value voices from the BIPOC community (Bowleg, 2021).
Transforming Teaching
We organize our critique around three ordinary responsibilities of public health educators—assigning readings, shaping analytical lenses, and modeling change through andragogy—as opportunities to name racism, question how it operates, and organize to dismantle it (C. P. Jones, 2018). First, educators select readings for syllabi which structures how students define public health needs. Because how one defines a problem guides strategies to respond, students’ aptitudes to identify racism as determinants of health hinge on including BIPOC authors and critical epistemologies that challenge dominant narratives in course reading lists. Second, educators shape how students analyze the causes of health inequities by curating which theories are taught. To interrogate how racism operates, students must critically interpret the mundane encounters between BIPOC and the systems that structure life (Gee et al., 2019). Third, educators model decision-making through andragogy, how they engage adult learners. To develop the commitment to justice and practical skills required to organize and strategize against racism, educators and students must cocreate classroom environments that amplify BIPOC students’ aspirations for change.
We urge educators to decenter Whiteness when not only teaching about racial health inequities but also throughout public health graduate training. That is, readings, theories, and andragogy represent everyday opportunities to transform teaching by learning from BIPOC scholars, community members, and students. Furthermore, “because those with the power to change institutions were also educated by these institutions . . . they . . . often perform their lives devoid of racial consciousness” (Patton, 2016, p. 234). Table 1 outlines how readings, theories, and andragogy serve as opportunities to either uphold the status quo (conventional competencies) or challenge it (CRT-informed competencies).
Comparison of Select Conventional and Critical Race Theory (CRT) Learning Competencies for Academic Public Health.
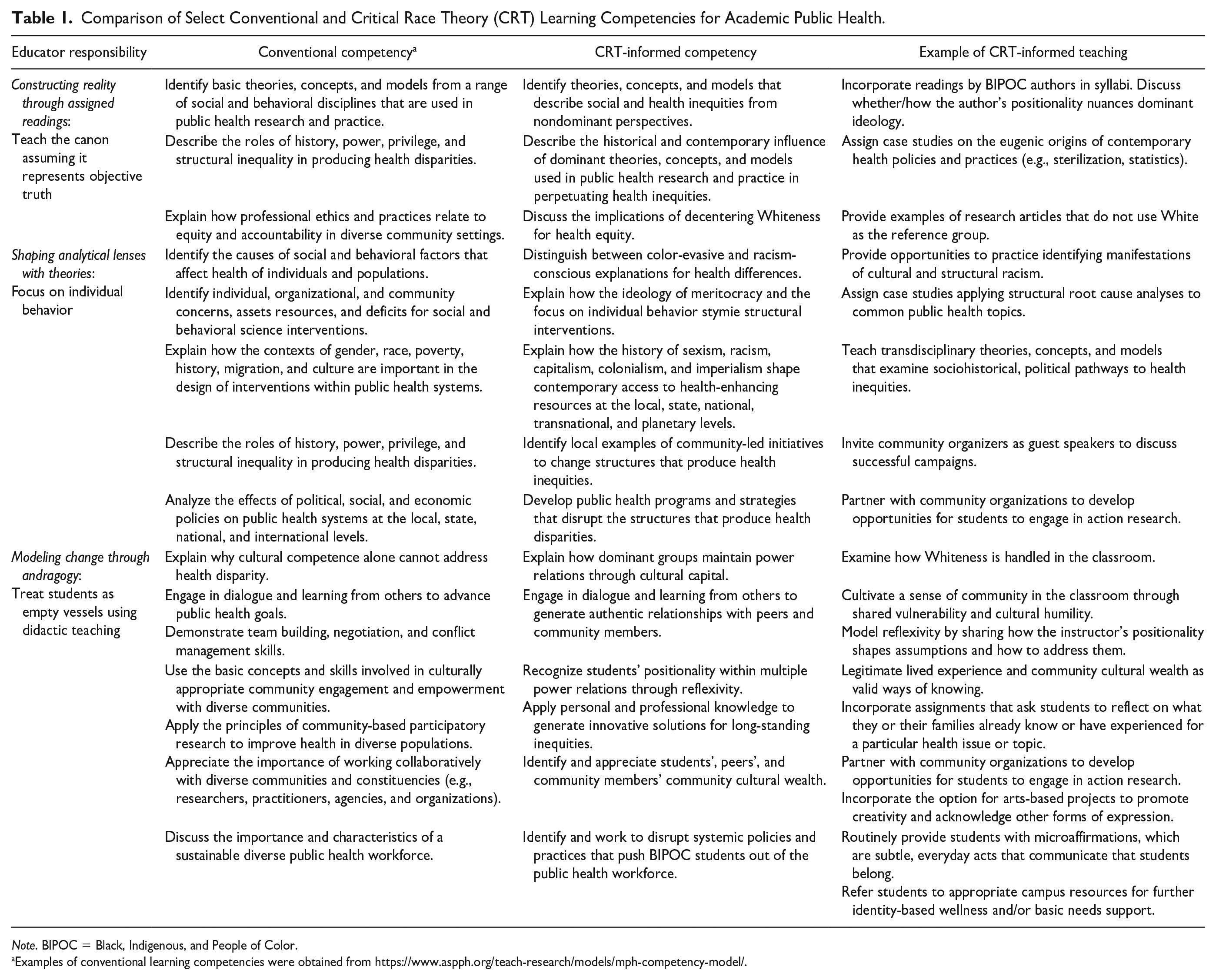
Note. BIPOC = Black, Indigenous, and People of Color.
Examples of conventional learning competencies were obtained from https://www.aspph.org/teach-research/models/mph-competency-model/.
Constructing Reality Through Assigned Readings
Class readings reinforce what is considered valued and normative in a field. In public health, reading lists transmit ways to think about public health needs (Schucan Bird & Pitman, 2020). When instructors assign readings, they exercise the power to set students’ foundational knowledge of public health. As intellectual currency, citations simultaneously facilitate the dissemination of some knowledge while restricting that of others (Bowleg, 2021).
Public health reading lists often cite established scholars who, given historical and ongoing racism and sexism in the academy, are most often White men (Ford & Airhihenbuwa, 2018; Zidani, 2021). The presumed superiority of Western knowledge has propagated through centuries of colonization, rupturing, denigrating, and erasing Indigenous ways of knowing (Smith, 2012). The “apartheid of knowledge” in academia “legitimates” mainstream knowledge while discrediting BIPOC epistemologies (Delgado Bernal & Villalpando, 2002). This cyclical devaluation of insights impedes progress in the pipeline of BIPOC educators, researchers, and authors (Bowleg, 2021; Yancey et al., 2007). Unequal opportunities to publish critical research and design related courses yield structural barriers to spreading BIPOC knowledge.
Thus, a predominantly White faculty defaults to crafting syllabi which center publications authored by White scholars as the public health “canon.” For example, authors of assigned articles from two academic years of syllabi in a London MPH program overwhelmingly skewed toward institutions in the United States and United Kingdom (Price et al., 2022). Similarly, content analysis of 30 syllabi from top social/behavioral science MPH programs in the United States showed that all 15 of the most commonly taught theories were first-authored by White men and the two most commonly assigned behavioral theory textbooks were coedited by White women (Harvey & McGladrey, 2019). 1 Centering dominant perspectives naturalizes racist conditions and constrains students’ ingenuity (Kagawa-Singer, 2000).
What is excluded from syllabi also maintains health inequities (Petteway, 2020). To prepare students to critically identify public health issues, educators should prompt students to consider whose definitions of health are centered (Chandanabhumma et al., 2020; Delgado, 1989). Rather than assuming one universal truth, CRT appreciates the social construction of knowledge production and, relatedly, values BIPOC epistemologies (Ford & Airhihenbuwa, 2010). As Hill Collins (1990, p. 269) wrote, “[T]he significance of a Black feminist epistemology may lie in its ability to enrich our understanding of how subordinate groups create knowledge that fosters both their empowerment and social justice.” Because people at the margins of society uniquely understand oppression and resistance, educators should incorporate texts authored by BIPOC scholars that can inform pathways to health equity (Bowleg, 2021; Patton, 2016).
Racism-conscious educators can redistribute power by constructing syllabi for racial health equity rather than default to previously used materials. Table 1 provides examples of CRT-informed competencies and relevant teaching practices that promote disciplinary self-critique. Isolated modules on racism or infrequently offered electives are necessary but insufficient. Instead, BIPOC scholarship must be incorporated into curricula on numerous foundational public health topics, as illustrated in Table 2. In core courses, educators can illustrate key questions in the field without defaulting to the “canon” (Zidani, 2021) and encourage students to examine authors’ potential biases (Bowleg, 2017). Educators are responsible for transmitting ideas through syllabi; whose knowledge is legitimized?
Examples of BIPOC Scholarship on Foundational Public Health Topics.
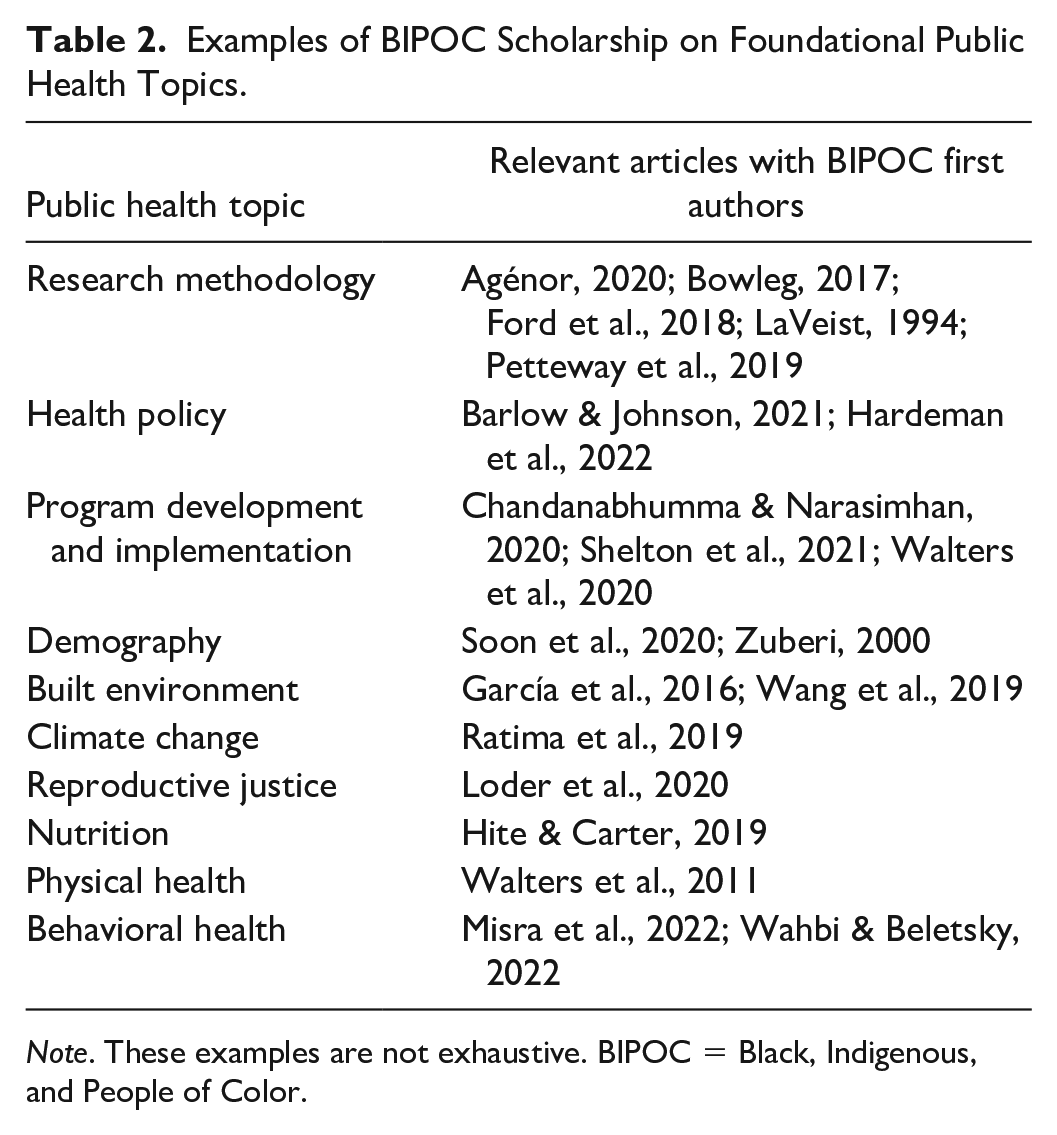
Note. These examples are not exhaustive. BIPOC = Black, Indigenous, and People of Color.
Shaping Analytical Lenses With Theories
Theory informs public health research and practice (Krieger, 2014). Although earlier health promotion initiatives focused on individual behavior change (Becker, 1986), health equity scholars recommend structural analyses to ascertain how upstream systems of power obscure multiple, complex pathways to health justice (Braveman & Parker Dominguez, 2021; Krieger, 2020). Choosing which theories to teach either stifles or enhances students’ abilities to connect structural racism to health inequities.
Individual behavior theories perpetuate Whiteness by utilizing dominant ideologies of meritocracy and color-evasiveness to explain population health disparities (Bonini & Matias, 2021; Kagawa-Singer, 2000; Neely et al., 2020). Among the 10 most commonly taught social/behavior theories in MPH programs, eight focus on individual factors (Harvey & McGladrey, 2019). Yet individual-level approaches are not well suited to address structural problems (Golden & Earp, 2012).
Controlling for individuals’ “race” stymies progress for measuring exposures to racism (Ford et al., 2019; LaVeist, 1994). Health equity experts theorize a throughline between power structures, differential access to resources, unequal exposure to harmful conditions, and physiological responses (Braveman & Parker Dominguez, 2021; Tsai et al., 2021). Yet explicit theory, structural or otherwise, is rarely invoked to explain empirical racial health inequities research in high-impact journals, limiting students’ access to nuanced analyses (Krieger et al., 2021; Mannor & Malcoe, 2022). To disrupt myths about individual responsibility for health, educators should incorporate transdisciplinary theories to reveal distal determinants, sharpen students’ analysis of Whiteness, and deepen appreciation for BIPOC epistemologies (Neely et al., 2020; Sabado-Liwag et al., 2022; Sun, 2014). Table 1 Row 2 suggests ways to incorporate such analytical lenses into teaching.
To improve conceptualizations of structural oppression, educators must teach students various analytical approaches using CRT lenses (Ford et al., 2019; Hagopian et al., 2018 C. P. (Jones, 2018; Neely et al., 2020). PHCRP provides an ordered process to guide racism-conscious empirical research and action-oriented practice for racial health equity (Ford & Airhihenbuwa, 2010). PHCRP scholars use tools from multiple disciplines to trace the roots of contemporary health outcomes, as noted in Table 3. Theories about structural determinants of inequity have been recommended elsewhere (Harvey, 2020).
Transdisciplinary Empirical Analyses of Public Health Issues.
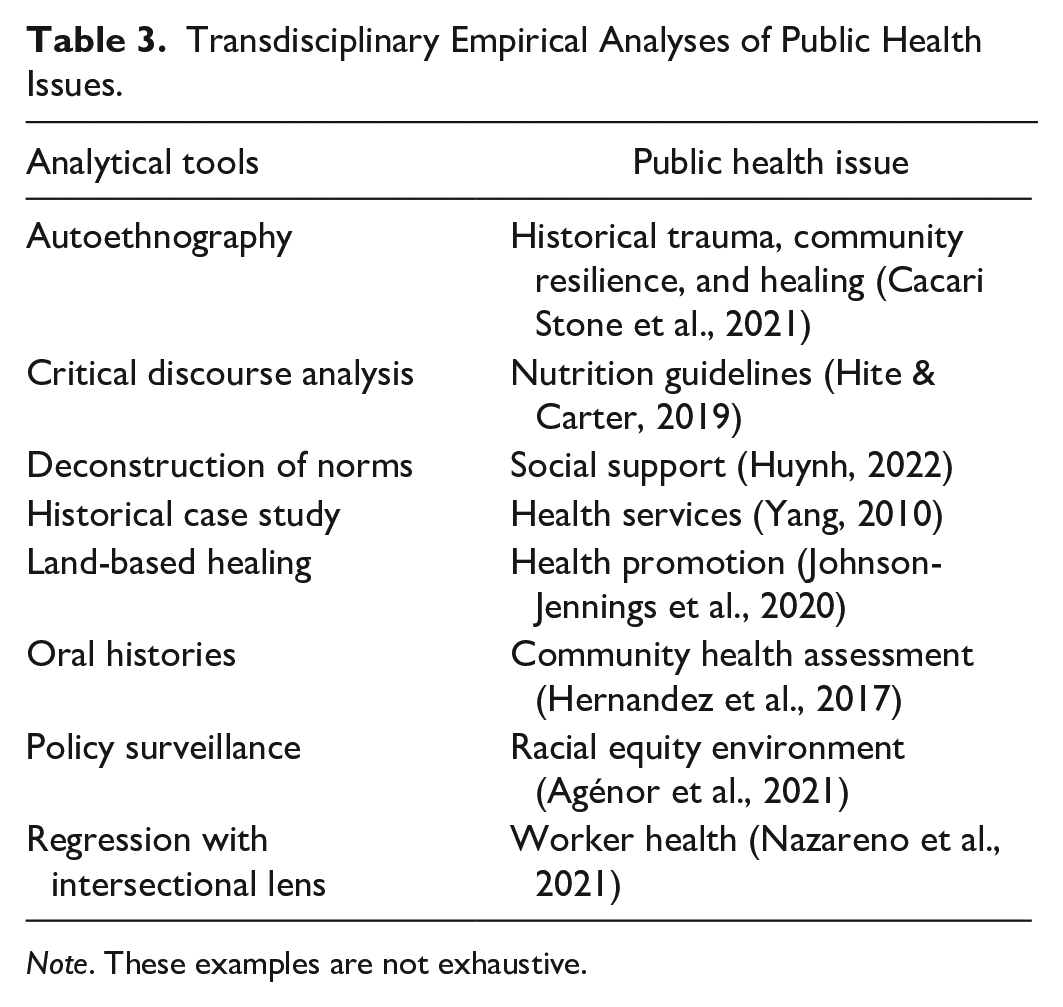
Note. These examples are not exhaustive.
Students can hone their cultural intuition to expose White supremacy in the ordinary lives of BIPOC (Delgado Bernal, 1998; Ford & Airhihenbuwa, 2010). Given the variants of racism (Davis, 2021), scholars of CRT in education have more precisely articulated its tenets for specific groups: LatCrit (Solórzano & Yosso, 2001), TribalCrit (Brayboy, 2005), AsianCrit (Iftikar & Museus, 2018), DisCrit (Annamma et al., 2017), and UndocuCrit (Aguilar, 2019). These branches distinguish racialized exposures to harm.
Public health students must also recognize how racism intersects with other systems of oppression (Agénor, 2020), including capitalism (Laster Pirtle, 2020), patriarchy (Bowleg, 2017), colonialism (Chandanabhumma & Narasimhan, 2020), and ableism (Annamma et al., 2017). For example, conventional public health may attribute elevated rates of obesity among low-income communities of color to limited access to well-equipped parks. While plausible, racial capitalism further unveils more than a century of urban planning decisions to privatize recreational spaces (e.g., single-family homes with backyards), destroy non-White communities (e.g., developing freeways through Black, Latinx, or Asian neighborhoods), and maintain disinvestment in public parks (e.g., property tax policies) (García et al., 2016). Supplanting home-based physical fitness education, the enhanced inquiry proposes anti-capitalist community organizing to sustainably invest in healthier neighborhoods for communities of color.
Analytical transformation requires shifting perceptions of community members from “at-risk” study participants to collaborators with self-determined priorities (Smith, 2012; Tuck, 2009). As the experts of their own lives (Chandanabhumma et al., 2020), BIPOC community members should be involved in setting the agenda in academic public health, including informing curricular decisions (Hardeman et al., 2018; Perez et al., 2021). Public health programs are responsible for training students to recognize the determinants of health; whose lenses are used?
Modeling Change Through Andragogy
Educators’ interactions with students affect the latter’s capacity for change as future public health professionals (Chávez et al., 2006). Public health educators must not only facilitate knowledge acquisition but also, as an applied field, prepare graduates to cocreate the conditions for health equity (Komro et al., 2018). Whether “pedagogy” for children or “andragogy” for adults, teaching strategies affect students’ potential to change society (Freire, 2000; Solórzano, 2022). To encourage students’ agency, educators must make andragogical decisions that affirm, not dehumanize, as described in Table 1 Row 3.
Anti-racist andragogy refers to “instructional approaches in adult education designed to interrupt systems of oppression and challenge racist and discriminatory ideologies” (Sandifer et al., 2022, p. 1). Traditionally, Malcolm Knowles’ concept of andragogy acknowledges that adults bring a wealth of experience to the classroom, which shapes their comprehension of material. From an anti-racist perspective, this suggests that instructors should actively encourage students to reflect on their experiences as integral to dismantling racism.
Public health graduate educators, however, frequently utilize top-down, didactic methods that view students as empty vessels for depositing knowledge, a style critical education philosopher Paulo Freire referred to as “banking” (Chávez et al., 2006; Freire, 2000). This structure of teaching is inherently hierarchical, with professors serving as gatekeepers of knowledge and opportunities. For example, the presumed default is to send course syllabi as PDFs as opposed to collaborative, modifiable documents. The unidirectionality of power relations is normalized throughout the course (e.g., enrollment requisites, classroom engagement, standardized assignments, office hours).
Power dynamics typically maintain a culture of Whiteness that dehumanizes BIPOC students by divorcing content from lived experiences (Camangian & Stovall, 2022; Ladson-Billings, 1995). Engaged dialogue on epistemology enables students to interpret the world in context of their social identities and professional commitments. When educators fail to connect subject matter to students’ knowledge from their lives, BIPOC students’ assets frequently remain unrecognized (Delima, 2019; Yosso, 2005).
When White culture is synonymous with the norms in academic public health, students familiar with the dominant culture benefit (Utt, 2018). For example, “dispassionate” neutrality is often conflated with professionalism, socializing graduate students of color to silence their emotions to uphold the semblance of objectivity (Bowleg, 2021; Petteway, 2021; Solórzano & Yosso, 2001). Relatedly, requiring adherence to “academically acceptable English” prioritizes language that is “palatable to mainstream white society,” often diverging from BIPOC students’ preferred communication styles (Camangian & Stovall, 2022). In addition, environments lacking familiar sights, sounds, scents, and tastes contribute to feelings of exclusion (Chávez et al., 2006; Yancey et al., 2007). By teaching how they were taught, educators may unintentionally inflict psychological harm and distract students who respond by organizing others (Gwayi-Chore et al., 2021; McSorley et al., 2021).
In contrast, Freirean educators informed by CRT collaborate with students by incorporating humanizing activities toward social change (Camangian & Cariaga, 2021; Chávez et al., 2006). As a precursor to regarding students as cocreators of knowledge, educators must be mindful of their own relationships to power (Petteway, 2021; Rodney, 2016), specifically their complicity in upholding Whiteness (Aqil et al., 2021; Bonini & Matias, 2021). Reflecting on teaching philosophies and privileges can reveal underlying biases about what scholars look like, where they have been trained, and whose realities are deemed “unworthy of intellectual interrogation” (Camangian & Stovall, 2022; Posselt, 2018). Rejecting the caricature of the all-knowing professor, Freirean educators embrace collective dialogue as an ongoing process of learning alongside students with vulnerability, humility, and courage (Solórzano, 2022).
To engage in the reflexivity required to contribute a shared understanding of health inequities (McSorley et al., 2021), students should be liberated from rote demonstrations of knowledge. Narrative storytelling may resonate more deeply among students with strong oral traditions; indeed, testimonios have been framed as a critical race strategy for addressing segregated knowledge (Huber, 2009). Reflection journals and arts-based projects creatively integrate students’ professional and political voices (Griffith & Semlow, 2020; Lightfoot et al., 2021; Petteway, 2021). The insights generated through these activities could inform collaborative training opportunities for action research financially supported by local public health organizations (Blenner et al., 2021). Health equity cannot be achieved in silos (Galea & Vaughan, 2019). Educators are responsible for training students to ensure the public’s health; whose insights are driving change?
CRT challenges claims of neutrality. Educators should abandon conventional approaches to teaching public health to unleash our collective potential to dismantle White supremacy. Transformation may begin with discomfort (Chávez et al., 2006), particularly among those who benefit from Whiteness (Leonardo & Porter, 2010). Unlearning oppressive ideologies may feel strange and unsettling, given the myriad of societal norms which elevate educators above students, naturalize racial hierarchies, and depoliticize death. Ultimately, the goal for transforming teaching is humanization, changing relations by changing standards of who is seen as fully human (Leonardo & Porter, 2010) and embracing discomfort and struggle as necessary for growth (Rodney, 2016). Racism-conscious teaching commits to broadening perspectives, advancing structural analyses, and sustaining transformative resistance.
Public Health Implications
Public health training must evolve to match transformations in public health practice. For example, equity-focused measures have been incorporated into the 10 essential public health services for health department accreditation (The Futures Initiative, 2020). For community health improvement process development, departments must demonstrate engagement with multiple community organizations and review local impacts on exclusionary policies (e.g., redlining) and disinvestment (Public Health Accreditation Board, 2022). To train the critical, anti-racist professionals needed to equitably assure these services, we need critical, anti-racist health workforce development (Bonini & Matias, 2021; French et al., 2020; Maglalang & Rao, 2021; Ramirez-Valles et al., 2022; Tsai et al., 2021).
Relatedly, the socialization of health professionals should be incorporated into research on structural determinants of health inequity. That is, health equity scholars could monitor trainees’ preparedness for equity. For example, course syllabi could be analyzed to detect differences in assigned readings (e.g., author race, research paradigms, and theories). What is taught could be compared across institutional types (e.g., minority-serving institutions), assessed longitudinally (Price et al., 2022), or juxtaposed against local demographic composition (Lucy et al., 2020). Schools and programs in public health have begun to transparently discuss struggles and innovative approaches for centering equity in curricular policies (Hagopian et al., 2018; Perez et al., 2021; Seiler et al., 2022). Training program evaluations should operationalize concepts from CRT of education (e.g., microaffirmations, community cultural wealth, transformational resistance) to garner support for humanizing andragogy (Neely et al., 2020; Pasick et al., 2012; Solórzano, 2022).
Public health educators must acknowledge the futility of using White logic and White methods to change health inequities produced by Whiteness (Bowleg, 2021; Patton, 2016; Stewart, 2003). Instead, we need a public health workforce that can define needs informed by BIPOC scholarship, substantiate analyses through the material realities of BIPOC lives, and collectively build new futures inspired by BIPOC aspirations. A CRT approach to teaching would provide students with the knowledge, analytical skills, and collaborative networks necessary for organizing anti-racist partnerships for racial health equity (Mitchell et al., 2022; Neely et al., 2020).
Transforming teaching for health equity is not a prescription for specific readings, theories, or course assignments. Rather, by critically questioning whose knowledge is legitimized when determining public health needs, whose lenses are used to prioritize solutions, and whose insights drive change, we can train a public health workforce more critical of racism, and more prepared to deal with the complexities and contradictions of racial relations. To manage the serious public health threat of racism, we must commit to asking ourselves, whose knowledge heals?
Footnotes
Acknowledgements
Erin Manalo-Pedro is grateful for the humanizing mentorship and critical guidance from Walter R. Allen, Daniel G. Solórzano, and their respective research apprenticeship courses. The authors would also like to thank the members of Gilbert C. Gee’s lab group for feedback on prior versions of this manuscript and Chandra L. Ford and the Center for the Study of Racism, Social Justice, and Health for encouraging disciplinary self-critique as a route to health equity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.