
Abstract
Background
Health behaviors, like diet, are influenced by a person’s culture and the society where they reside, contributing to the presence of health disparities within a unique region. Such disparities are evident in Central Appalachia where a unique cultural identity exists. Culture-based initiatives focused on improving food security and other nutritional challenges have had success in other diverse groups, yet similar interventions considering geographically tied culture, like Appalachia, are limited.
Aim
This study aims to identify specific aspects of Appalachian culture that address food insecurity to inform future initiatives that may improve adult dietary habits and food security status.
Methods
Qualitative data were collected from five focus groups in one rural Central Appalachian community in 2021 (n=59). Data were analyzed using Grounded Theory Approach.
Results
Four primary themes related to culture and food insecurity emerged: 1) Community decline and economic hardship 2) Shifts in multigenerational food traditions 3) Response to limited food access and 4) Value of social and familial units. Participants revealed adaptations they have made in the face of geographic isolation and poverty and the pride they take in providing for themselves and one another.
Conclusion
These findings indicate the people of Appalachia are unknowingly leveraging cultural practices to address food insecurity, yet the impact of these practices on nutritional status remains unknown. These results have implications for future studies and interventions in Appalachia which may have greater success by accounting for cultural influences compared to traditional approaches for reducing food insecurity in the region.
Culture is recognized as a combination of people, practices, and places that form a system of behavior and influence (Causadias, 2020). Cultures may develop based on race, class, ethnicity, gender, sexual orientation, religion, or geographic proximity. Health behaviors are influenced by a person’s culture and the society where they reside (Napier et al., 2014). These health behaviors include those which are tied to diet and may influence a myriad of health outcomes. It is imperative that interventions focused on improving food security and other nutritional challenges incorporate culture to be effective in achieving positive behavior change. This is particularly important when working in regions and subcultures that experience disproportionately high levels of health disparities. These disparities are apparent in the Appalachian region of the United States, where a geographic cultural identity has formed due to topographical remoteness.
Health disparities among cultural groups have been well documented (Milburn et al., 2019). Evidence suggests a correlation between cultural norms and a propensity for certain diet-related metabolic conditions (Thomas et al., 2004). Obesity and related chronic conditions are more prominent in Appalachia, and contribute to increased mortality, compared with other areas of the United States (Appalachian Regional Commission, 2019). Notably, those living in Central Appalachia, a subregion spanning four states and concentrated in eastern Kentucky, have experienced some of the highest rates of disparity and chronic disease for decades (Marshall et al., 2017). Residents of this subregion have higher obesity prevalence, cardiovascular disease mortality, and diabetes rates compared with non-Appalachian counties (Appalachian Regional Commission, 2019), all of which are exacerbated by food insecurity. In some Eastern Kentucky counties, food insecurity rates top 26% compared with the national average of 11% (Feeding America, 2020). Food insecurity brings specific barriers to healthy behaviors which further impacts the health status of these communities.
Multiple barriers exist that impede diet quality and increase food insecurity prevalence in Appalachia. Regional concerns include the high cost and time commitment associated with healthy cooking, limited nutritional knowledge, and fears surrounding new eating behaviors (Cardarelli et al., 2020, 2021; Hardin-Fanning & Ricks, 2017). Traditional Appalachian foods and procurement methods have been passed through generations in the face of poverty and limited access, which is reflected in the history of regional food culture, resourcefulness, and community pride related to self-sufficiency (Sohn, 2005; Veteto et al., 2011). To date, limited work has explored whether these adopted practices to address food insecurity in Appalachia are embedded within the localized culture by occurring naturally, or if they are formally embedded within the community by choice as a mechanism to address food insecurity.
The approach of incorporating community input and cultural preferences in health promotion efforts has been explored in a variety of cultural subgroups with success (Kagawa Singer et al., 2016). Culture-based interventions in communities of color found promising results in health promotion programs working directly with community members to craft specific messaging and materials (Fisher et al., 2007). Often, culture is used interchangeably with race and ethnicity with little exploration of geographically tied cultural aspects informing health promotion interventions. In Appalachia, the importance of community input for nutrition and food security-focused interventions has been recently documented (Cardarelli et al., 2020). Formative research has also revealed the importance of leveraging cultural assets in this geographic region for community-based interventions promoting healthy behaviors, (Kruger et al., 2012). Broad assumptions may be made that community-based interventions are culturally informed by nature; however, the angle of culture may not always be accounted for in community-based participatory research depending on who is contributing and the mechanism(s) for gathering information. There may be no difference between culturally informed and community-informed interventions, but focusing on one community challenge, like food insecurity, may help delineate the differences between the two if any exist.
Given the effectiveness of culturally informed health interventions in other populations (Fisher et al., 2007), and the growing understanding of Appalachian culture (Denham, 2016), there is a need to explore how culture may address increasing rates of food insecurity and related health disparities in Central Appalachia. For the first time, to our knowledge, this study aims to identify specific aspects of Appalachian culture that are being used to address food insecurity in efforts to better understand future initiatives that may improve dietary habits and food security status while accounting for unique regional barriers.
Method
Data were collected via focus groups in May and June of 2021 in Martin County, Kentucky. The Institutional Review Board at the University of Kentucky approved all study materials and procedures (protocol #48905).
Setting
Martin County is a small Central Appalachian community, home to approximately 11,000 residents (United States Census Bureau, 2021a). Poverty levels within the county are almost three times the national average at 32%, compared with 15% in Kentucky and 12% nationally (United States Census Bureau, 2021b). As of April 2022, unemployment rates follow similar patterns at 7.3% in Martin County, 3.9% in Kentucky (KYstats, 2022), and 3.6% nationally (U.S. Bureau of Labor Statistics, 2022). The median household income for Martin County residents is US$30,320, well below that of Kentucky (US$54,074) and the United States (US$67,340) (United States Census Bureau, 2021b). Based on these three economic factors, Martin County is considered “distressed” within Appalachia (Appalachian Regional Commission, 2022). Food access indicators classify the county as low-income and low-access (USDA Economic Research Service, 2021), and trends indicate approximately 20% of the county are food insecure, including nearly one in four children (Feeding America, 2020). Twenty-two percent of adults under age 65 live with a disability (United States Census Bureau, 2021a).
Recruitment and Procedures
Participants were recruited from the community in partnership with the local Cooperative Extension Office and the Martin County Wellness Coalition. Both Cooperative Extension and a community Facebook page managed by a Coalition member advertised flyers on their social media pages in the spring of 2021. Physical flyers were also provided through the Extension office and a local newspaper. Adults over the age of 21 who had resided in Martin County for at least 1 year and were able to be physically active were intentionally recruited to participate.
All focus groups took place at the Martin County Extension Office in May and June 2021. Each of the five sessions included 10 to 14 participants and ranged between 58 and 69 min in length. Although some level of attrition was anticipated, a majority of participants who registered chose to attend the focus group sessions. The size of the focus groups was chosen to accommodate the high interest in participation while still assuring an appropriate environment for success. Written informed consent was obtained prior to beginning, and a US$40 gift card was offered as an incentive. Participants also completed a sociodemographic survey that included the following variables: age, race, gender, socioeconomic status, household size, education level, and food security status. Findings related to food security in this sample have previously been reported (Cardarelli et al., 2021).
A trained moderator oversaw each of the focus group conversations using a semi-structured moderator guide. The moderator made a concerted effort to ensure all participants that wished to participate in the discussion had the opportunity to do so. Four digital recording devices were used, and physical notes were taken by two to three researchers per session. Questions were asked regarding cultural influences on barriers to and motivations for healthy behaviors in the community, food access, food security, and implications of COVID on health behaviors.
Analysis
All demographic data were analyzed in Excel (Microsoft Office 365). Audio recordings were transcribed verbatim by researchers and graduate students. Investigators reviewed the transcripts and conducted thematic analysis using a grounded theory approach (Chun Tie et al., 2019). An inductive-deductive process was used to identify themes regarding cultural influences on health behavior which became the foundation for codes that were analyzed using NVivo (QSR International, Cambridge, MA, v. 12) in March and April 2022. Interrater reliability was measured after 20% of the transcripts were coded with 77% agreement between coders based on the Kappa coefficient in NVivo. The two coders independently applied the codes to the remaining transcripts. Final themes were then derived and agreed upon by investigators, and illustrative quotes were identified.
Results
Participants
Fifty-nine individuals participated in five focus groups. Table 1 provides the relevant sociodemographic information for participants. Participants were predominantly white women who had at least some college education. Although over half of the participants reported an annual household income below US$50,000, 49% reported receiving no formal food assistance.
Demographics of Focus Group Participants (n = 59), XXX County, STATE, 2021.
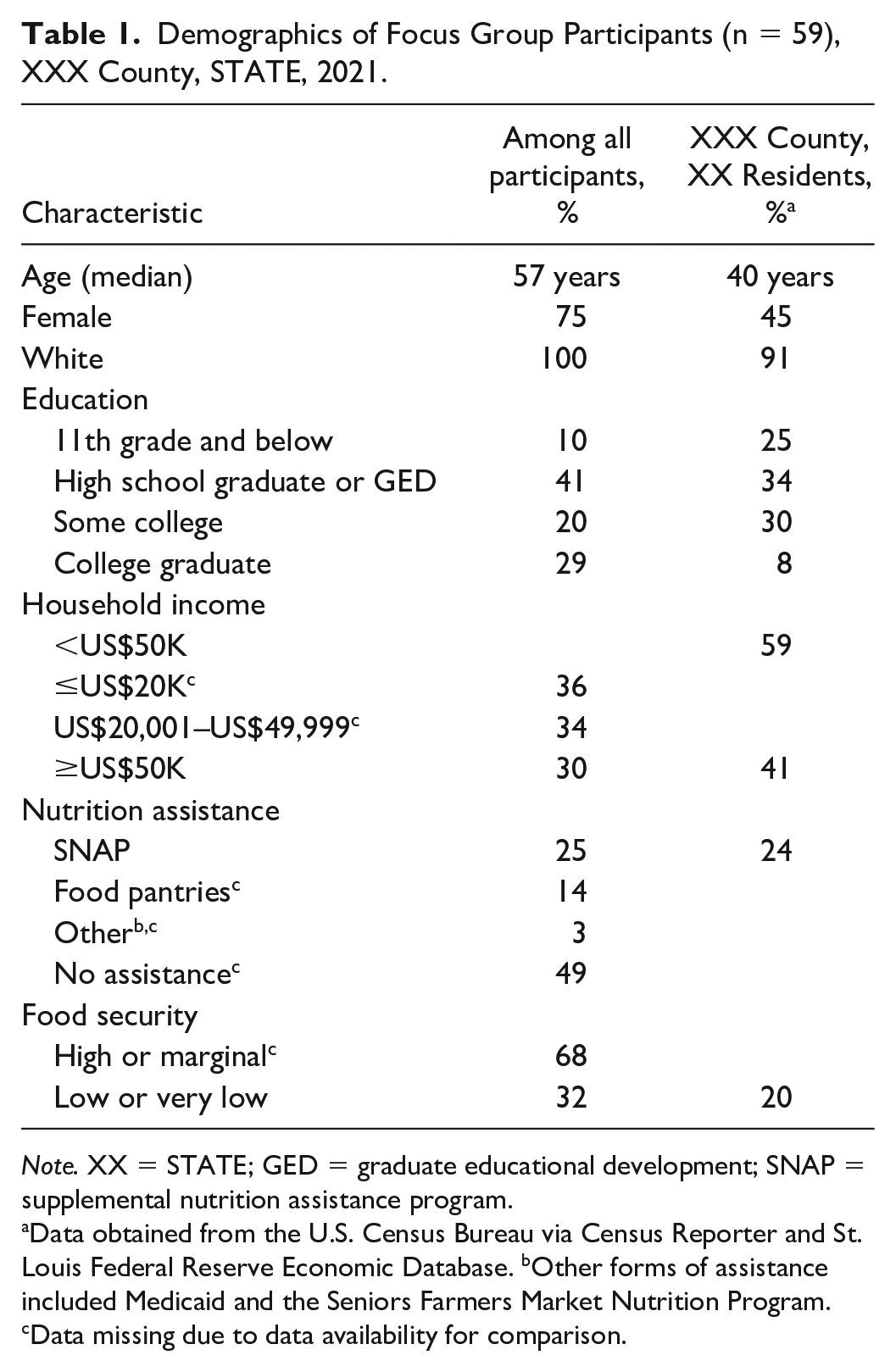
Note. XX = STATE; GED = graduate educational development; SNAP = supplemental nutrition assistance program.
Data obtained from the U.S. Census Bureau via Census Reporter and St. Louis Federal Reserve Economic Database. bOther forms of assistance included Medicaid and the Seniors Farmers Market Nutrition Program. cData missing due to data availability for comparison.
Qualitative Findings
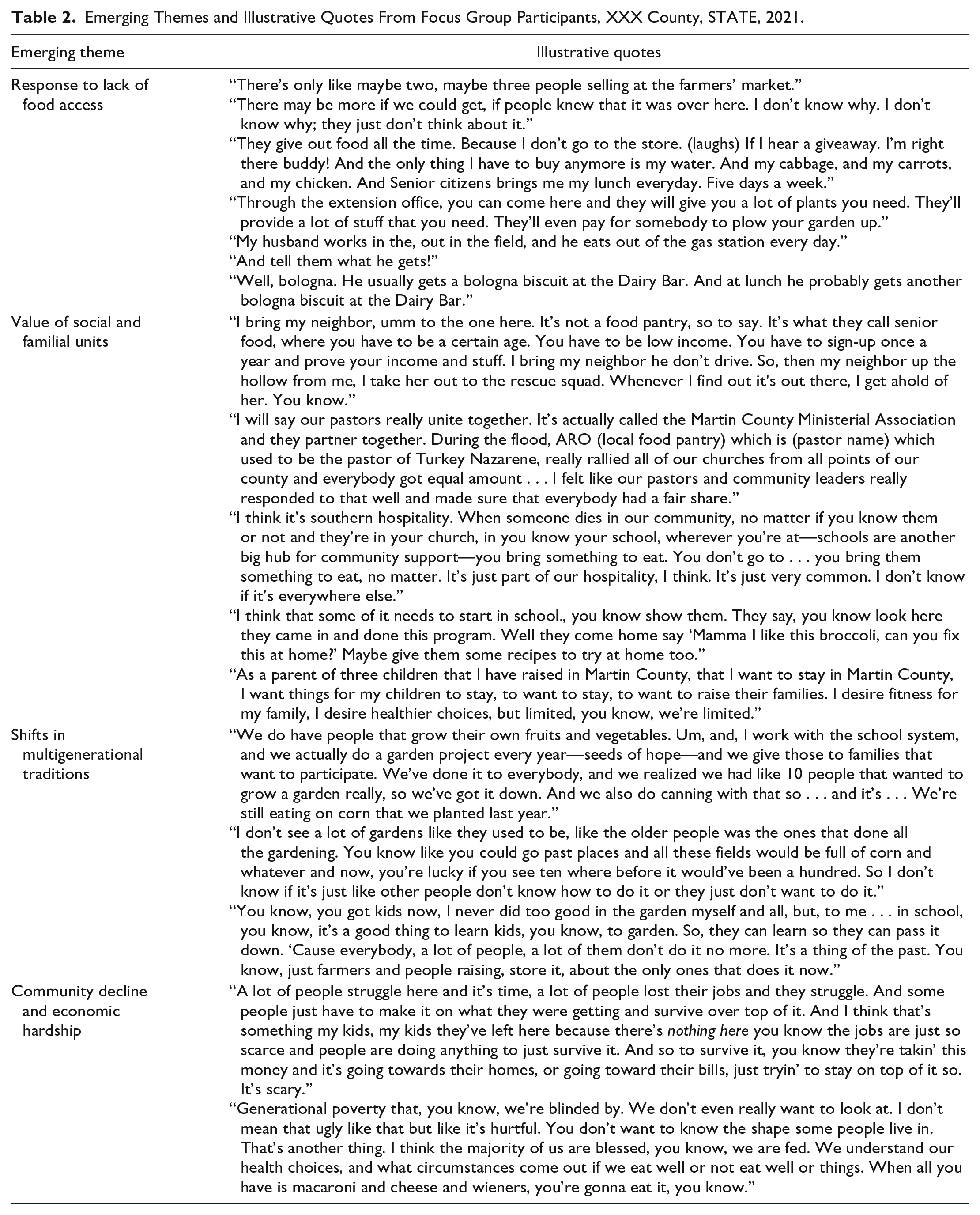
Four primary themes emerged that reflected cultural implications on health behaviors: (a) community decline and economic hardship, (b) shifts in multigenerational food traditions, (c) response to limited food access, and (d) value of social and familial units. Illustrative quotes for each theme are found in Table 2.
Emerging Themes and Illustrative Quotes From Focus Group Participants, XXX County, STATE, 2021.
Theme 1: Community Decline and Economic Hardship
Community decline related to a loss of job opportunities in the area was identified as a unique challenge to healthy behaviors. Participants explained that people have migrated away from the county seeking better employment opportunities, leaving older generations, and their community, behind. One participant noted:
You know our county used to be a big boomin’ town, but since we lost the mines, the coal mines, you know it’s gone down a whole lot. A lot of places have closed down, a lot of people have moved away you know because, it’s just hard here right now.
Participants also recognized the impact the limited economic opportunities may have on their children. One participant shared:
I got two girls and I wish they was back here, but they don’t like it. They both graduated . . . One graduated from college about four years ago . . . I was kind of hoping she’d come back here but she said there ain’t no jobs here.
The lack of industry and insufficient job opportunities have contributed to outmigration and economic decline in this community. This decline has influenced generational poverty, which was also recognized as a persistent barrier by participants, directly impacting food security and the ability to make healthy dietary choices.
Theme 2: Shifts in Multigenerational Food Traditions
Regional and traditional food-related behaviors and practices, like food preservation and gardening, are being lost, with participants noting these skills are no longer passed on to younger generations. One participant shared:
My grandmother always kept a garden, but it didn’t, like my mom and aunts and stuff didn’t develop that skill. That’s something I would love to be able to do, but, if there was a program like at the high school to maybe implement this stuff, it would keep going like after my generation.
Participants were eager to revive these traditional practices in younger generations. School-based gardens, along with personal efforts by community members to pass these skills along within their own families, were commonly mentioned. “I’m trying to educate my grandson, my great-grandson.” This participant further explained:
To eat healthier. He does help with a little bit of gardening. I started planting cucumbers for him when he was like three and he loved that. So, I don’t know. Kids, we have to start there to teach them you gotta live healthier, you gotta exercise, and you will be healthy.
Participants repeatedly expressed a desire to invest in future generations so they could provide for themselves and others.
Theme 3: Response to Limited Food Access
Due to limited grocery stores and supermarkets in the area, participants shared that other food access points were relied on, including non-traditional methods. Along with relying on faith- and community-based organizations to ensure food self-sufficiency, some reported regularly purchasing food from convenience stores. One participant shared:
I think just about every gas station around here has a space where they prepare food and serve it to, you know, to the community. Whoever comes in there to buy gas usually walks away with something to eat too.
Hunting was another procurement activity mentioned by participants, with one participant noting, “I think a lot, they do hunt a lot. When the hunting season’s coming up, they hunt turkey, they hunt deer, rabbit.” Participants shared that this practice generates enough meat to store for personal use and, if any extra remains, people share with their neighbors rather than letting anything go to waste. Others added that hunting was an activity in which youth were engaged from a young age.
Although available, participants shared that the local farmers market is often underutilized due to a lack of community members’ awareness and investment. Rather, home gardening was cited as a practice used by some residents to provide fresh food in the community. One participant explained:
I think a lot of people do the garden so that they can help other people . . . a lot of people will take their extra produce that they do get out of it and give it out to their families to help them along the journey of hardship and stuff. So, instead of throwing it away they’d rather give it away.
Significant barriers were also mentioned that hindered community members from gardening, including lack of awareness of community resources to support gardening, availability of seeds, and physical challenges in an aging population.
Theme 4: Value of Social and Familial Units
Participants conveyed a strong dependence on fellow community members and pride in the community’s ability to care for itself. The roles of social organizations, such as food pantries and senior citizen centers, and of individual community members in ensuring others had access to food and basic health services were articulated. Faith-based organizations were reiterated as a cornerstone of social connection and community support with one participant sharing, “During our flood that we just went through, our church has a food bank, and it went from 12 to 20 people to 50 to 75 just in the timeframe.” Other examples of community unification included providing transportation assistance and establishing food sharing networks among social units such as close neighbors.
Participants emphasized the importance of family units, focusing on youth within families as a motivator for positive health behavior change. One participant stated:
That’s how it is. If you get something for kids, the parents will take their kids. And that just about anything we do. Because our life’s around our kids. We make our kids happy and keep them healthy and things like that, parents usually jump on it . . .
In addition, participants wanted their children to stay and raise their own families in the area. Several participants explained that keeping multigenerational family units in the region was a highly valued priority. Despite the strong emphasis on family units, generational changes away from traditional behaviors within families were revealed.
Discussion
Our work corroborates the existing literature on the importance of respecting and honoring cultural traditions and practices in health promotion work (Kagawa Singer et al., 2016). However, our study provides a novel example illustrating that certain subgroups are addressing food insecurity and poverty indirectly through culturally relevant food practices. Participants in our study did not explicitly recognize their efforts as protective against food insecurity, suggesting that food insecurity, to an extent, is being addressed organically through cultural practices. Rather, their reasoning for these practices centered on assisting those in their community that are in need, illustrating their generosity and resourcefulness to ensure their community is cared for.
Appalachia has long been broadly characterized as a resilient and self-sufficient region (Denham, 2016), and the current findings make it clear that many of the practices that contribute to this reputation of resourcefulness are directly tied to food access and security. Residents in this community have adapted their food procurement practices, relying on unconventional methods of securing food self-sufficiency. However, this self-sufficiency does not equate to reduced food insecurity in the region (USDA Economic Research Service, 2022). As revealed previously, food insecurity is still a challenge for many residents in this area (Cardarelli et al., 2021; DeWitt et al., 2020). Current health disparities and chronic disease trends experienced in the region suggest that nutritional needs are not being met, contributing to poor health outcomes. It is imperative to continue to examine how cultural traditions and related practices may be used to address health disparities while further increasing food and nutrition security through the adoption and sustained use of health-promoting food behaviors.
The experiences of participants in this study reveal an undercurrent of cultural values which have formed around shared geography, religion, sense of individualism or collectivism, food procurement methods, and/or shared histories, consistent with previous work (Denham, 2016). These unique cultural factors have been heavily influenced by the economic, environmental, and social injustices pervasive in the region for decades (Engle, 2019) and create barriers to food security and other nutrition challenges within Central Appalachia. Although disparities were identified to varying degrees, the current study emphasized the resilience of the community and its culture that may be used to address nutrition-related health inequities. In Martin County, fruit and vegetable intake is low (Kentucky Health Facts, 2019). Although more than 1,400 varieties of fruits and vegetables are indigenous to the region, many traditional dishes center around starches, including beans, corn, and potatoes (Veteto et al., 2011). However, certain traditional methods of food procurement, such as gardening and food preservation skills, could be revitalized to increase the consumption of fruits and vegetables year-round.
Seemingly contradictory, participants noted that community members practiced gardening to provide for themselves and neighbors, while at the same time, gardening and other traditional practices were declining. Additional context was provided that these practices were primarily implemented by older community residents and these skills were being lost with generations and age-related physical challenges. As Engle et al. previously reported, in Central Appalachia, these gardening practices may be impacted by environmental injustices across the built, natural, health, and socioeconomic spheres, further influencing gardening efforts and providing multiple levels to intervene (Engle, 2019).
In this region, a strong identity of shared heritage is common, as many of the residents trace their Appalachian ancestry back by four or more generations (Denham, 2016). Multigenerational cultural adaptations have formed in response to difficult circumstances and chronic social injustices. This generational component was found to be a key motivator for behavior change among our sample, reinforcing the importance of tailored approaches. It was shared that identifying community organizations that prioritize youth may be an effective mechanism for eliciting positive behavior change. (Landry et al., 2021; Palar et al., 2019). Family-oriented nutrition programs that involve both parents and their children are more likely to result in desired outcomes (Murimi et al., 2018), though interventions focused on the inclusion of multiple generations are limited in Appalachia.
Other programs have attempted to leverage certain aspects of Appalachian culture to improve health outcomes with mixed success (Paskett et al., 2018). As revealed by participants in the present study, self-reliance, which is often mentioned as a hallmark of Appalachian culture, refers to the community, not necessarily individuals. In rural Appalachia, communities are closely tied to geography, where neighbors live in hollows or on mountains with restricted entry and access points due to topography and remoteness and rely upon one another for basic necessities. Previous work in this community highlighted a cultural value for assisting neighbors in need (Cardarelli et al., 2020), indicating the importance of social cohesion tied to geography. Although some progress has been made in nutritional confidence and self-efficacy, results have shown a limited impact on sustainable behavior changes (Torrence et al., 2018). Given our findings, health promotion interventions in this population should prioritize community-level programs, leveraging collectivism over individual initiatives and integrating cultural values into practice.
In response to challenges in traditional food access, such as limited grocery stores and supermarkets, many cultural food behaviors have shifted due to necessity, resilience, and self-sufficiency. Although some adaptations have led to less nutritious food choices, such as prepared foods from gas stations, residents of Martin County also leverage traditional food practices and other aspects of their culture to provide for themselves and their fellow community members by relying on formal and informal networks. Tracing back generations, hunting is tied to the culture of residents in the region (Special Collections Research Center, 2011). Although this practice was recognized as an activity for recreation and familial connectedness, it also provides a nutritious protein source and enables residents to maintain traditional processing, preparation, and preservation methods. Educational programs could be tailored to Appalachia by incorporating food procurement methods unique to the region. Better understanding of food access points and cultural preferences for food is highly informative for novel nutrition education approaches. For example, the Kentucky Nutrition Education Program developed education materials and affordable recipes centered around wild game that could be utilized by limited-resource families to reduce food insecurity (College of Agriculture, Food, and Environment, 2019). This type of program incorporates familiar recipes, locally available ingredients, and traditional cooking methods to provide families with resources for ensuring food sufficiency and promote healthy home-cooked meals.
Since the time of this study, several interventions and initiatives, derived from the community, have been culturally tailored and implemented. To address the expressed needs of skill building and the need for motivation in youth, partnerships were established with a local after school program at the middle school and one elementary school. This project will increase exposure to gardening practices via indoor hydroponic gardening systems (Anderson & Swafford, 2011; Corveleyn et al., 2020) and provide fresh produce for families. To build on existing community support and leverage social cohesion, a community garden was established at a local faith-based organization to increase access to fruits and vegetables at no cost to those from the community (Barnidge et al., 2013; Stluka et al., 2019). Finally, to work across generations in families and social units, Cooperative Extension programming has been expanded to increase access to fresh produce and increases capacity for gardening, food preparation, and food preservation skills among local growers is the existing Grow Appalachia program (Grow Appalachia, 2022). This program is designed to address food insecurity while also supporting local growers in entrepreneurship and enhancing social enterprise which addresses community decline. Collectively, these approaches are designed to support ongoing community collaboration emphasizing nutrition-based lifestyle behavior change to improve dietary habits and food security while accounting for unique regional barriers. Future studies will examine food security levels in the community after the implementation of these culturally tailored approaches.
Limitations
Like many qualitative studies, our study population was not randomly selected and was a small sample size, recruited through a purposive sampling approach. Study findings may not be applicable or reproducible in all Appalachian or rural communities, but provide evidence that culture, traditions, and local history perpetuate health behaviors and is unique to each community. Our sample is primarily older females with higher levels of education than the rest of the county; therefore, we cannot confirm that experiences shared are representative of the entire community. Participant responses may have been influenced by a social desirability bias. Finally, while it was not a major theme, the findings were undoubtedly influenced by the ongoing COVID-19 pandemic and the challenges it presented rural, remote communities.
Implications for Future Practice
Aligning interventions aimed at reducing health disparities and food insecurity with cultural norms and practices may be a novel approach for increased adoption and sustainability of health-promoting behaviors in Central Appalachia and other rural areas. More geographic subcultures exist beyond Appalachia, and tailored initiatives which consider and integrate cultural influences may have greater success than traditional approaches when striving to reduce these disparities. In our study, community members are unknowingly leveraging cultural practices to address food insecurity. These novel findings provide a unique mechanism that allows public health practitioners and nutrition educators to develop and adapt programming to address food security that is better suited for the communities in which they work. From this study, we are unaware of how these cultural adaptations impact nutrition status; therefore, future studies should examine strategies that target both food and nutrition security in efforts to reduce nutrition-related health disparities. Future strategies that bolster cultural practices, target food insecurity, and enhance nutrition security simultaneously should be considered.
Supplemental Material
sj-docx-1-heb-10.1177_10901981231175360 – Supplemental material for Exploring Food-Based Cultural Practices to Address Food Insecurity in Rural Appalachia
Supplemental material, sj-docx-1-heb-10.1177_10901981231175360 for Exploring Food-Based Cultural Practices to Address Food Insecurity in Rural Appalachia by Lauren Batey, Emily DeWitt, Dawn Brewer, Kathryn M. Cardarelli and Heather Norman-Burgdolf in Health Education & Behavior
Footnotes
Acknowledgements
The study team is grateful for the ongoing support of this work provided by the Martin County Cooperative Extension Office and the Martin County Wellness Coalition. They thank Brittany Cox, J.B. Pitts, and Rachel Gillespie for their assistance in data transcription.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the Centers for Disease Control and Prevention Division of Nutrition, Physical Activity, and Obesity (DNPAO), Cooperative Agreement number 1NU58DP0065690100.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.