
Abstract
Korean Americans in the United States are more likely than other Asian ethnic groups to lack health insurance despite their high education and economic prosperity. According to the model of health service selection, immigrants’ perceptions of the health care system and health care behaviors in their host country are affected by sociocultural referents including premigration health care experience in the country of origin. This study explored Korean immigrants’ perceptions of health insurance and their intentions to purchase and maintain health insurance in the United States. We conducted in-depth interviews with 24 self-employed Korean immigrants who migrated from South Korea and were living in the Greater Los Angeles area in 2015. Participants generally had negative perceptions of U.S. health insurance in terms of cost, benefits, simplicity, and accessibility. Coupled with their positive experiences with the single-payer, universal health insurance in South Korea, respondents evaluated U.S. health insurance as not worth purchasing, and indicated they would not maintain health insurance once the individual mandate of the Affordable Care Act was abolished. On the contrary, respondents who immigrated prior to the establishment of the Korean universal health insurance in South Korea were relatively satisfied with U.S. health insurance and had maintained health insurance for substantial periods of time. Korean immigrants’ premigration health care experiences appeared to influence their decisions to purchase health insurance in the United States and their intention to maintain health insurance. The study findings highlight the necessity of tailored health education that takes into account sociocultural determinants of health coverage among immigrants.
Keywords
Introduction
Korean Americans—the fifth-largest ethnic subgroup among Asian Americans and one of the fastest-growing populations in the United States (Budiman, 2021; Budiman & Ruiz, 2021)—are more likely to be uninsured compared with other racial/ethnic groups in the United States (Carrasquillo et al., 2000; Kao, 2010; Nguyen et al., 2015). Such findings puzzle experts because Korean Americans tend to have higher levels of education and income than other racial and ethnic groups (Kao, 2010; Nguyen et al., 2015). Nguyen et al. (2015) found that while Korean Americans reported approximately 40% higher educational attainment, compared with Vietnamese Americans, Korean Americans also had higher rates of being uninsured (39.5%) than their Chinese (16.6%) and Vietnamese (11.7%) counterparts. Even after the implementation of the Patient Protection and Affordable Care Act (ACA), Korean Americans were still more likely to be uninsured among Asian American ethnic groups (Park et al., 2018).
Higher rates of self-employment are viewed as a possible explanation for the lower insured rates among Korean Americans (Huang & Carrasquillo, 2008; Nguyen et al., 2015) because access to affordable health insurance in the United States largely relies on employment-based health benefits (Davis & Branscome, 2011; Lieberthal, 2016). According to the 2007–2011 American Community Survey, about 20% of Korean immigrants were self-employed, which is substantially higher than other Asian ethnic subgroups including Vietnamese (13%), Chinese (8%), Asian Indians (7%), and Filipinos (4%) (Min & Kim, 2018). The higher rates of self-employment among Korean immigrants were associated with the lower rates of employer-sponsored health insurance coverage among Korean immigrants (53%) compared with Chinese (74%) and Vietnamese (62%) counterparts (Carrasquillo et al., 2000). However, Korean Americans’ lower rates of health insurance coverage remain unexplained even after adjusting for employment status, types of employment, and other factors including sociodemographic, immigration-related, and health-related characteristics (Cook et al., 2014; Kao, 2010). Cook et al. (2014) found that Korean Americans working in small businesses were 6.21 times more likely to be uninsured compared with Japanese Americans even after controlling for self-employed status and other confounding factors (e.g., education). In a related study, Korean Americans were found to have the lowest insured rates compared with other ethnic Asian subgroups across all employment sectors (Nguyen et al., 2015).
The unexplained variance in health coverage among Korean Americans could be explained by sociocultural determinants that construct ethnic-specific experiences of institutions, such as health care systems (Alegría et al., 2010, 2011). Leduc and Proulx (2004) found that immigrant families go through a multistage decision-making process influenced by sociocultural referents when seeking health care services. They propose a four-part health service selection model that includes (1) a search for information on health services, (2) an evaluation of available health services based on perceived attributes and the individuals’ beliefs and attitudes toward the services, (3) selection and use of a specific health service, and (4) a retrospective evaluation of the decision, which then may affect the subsequent use of health services. According to this model, the evaluation, selection, and adoption of health services among immigrants are largely based on their health care experiences in both the host country and the country of origin. Immigrants select and use specific health services by evaluating attributes of available health services in the host country with their recollection of service use in their country of origin. Specifically, depending on the perceived cost, accessibility, availability, and quality of health services in the country of origin, immigrants would be inclined or reluctant to use host-country health services (Choi, 2013b; Leduc and Proulx, 2004).
After the Immigration and Naturalization Act of 1965 abolished the restriction of immigration from Asian countries, the number of Korean immigrants in the United States dramatically increased over sevenfold from 39,000 in 1970 to 290,000 in 1980 (Gibson & Jung, 2006). From 1976 to 1990, Koreans were the third largest group of immigrants in the United States, following Mexicans and the Filipinos (Min, 2011). The strong growth continued over the next three decades, with more than 1.9 million Korean Americans living in the United States as of 2019 (Budiman & Ruiz, 2021). Unlike early groups of Korean immigrants who were predominantly low-skilled workers, more recent immigrants have tended to have higher levels of education and incomes (Esterline & Batalova, 2022). At the same time that significant numbers of Korean immigrants were moving to the United States, South Korea established the National Health Insurance program (KNHI)—a single-payer, universal health insurance—in 1977 and enforced universal coverage in 1989 (Jeong, 2011; Jones, 2010; Song, 2009). The Korean National Health Insurance (KNHI) scheme includes lower premiums, limited benefits, and high out-of-pocket costs for illnesses requiring intensive care (Jones, 2010). According to a 2017 report by the Organization for Economic Co-operation and Development (Organisation for Economic Co-operation and Development [OECD], 2017), out-of-pocket medical expenditures in South Korea accounted for 5.1% of final household consumption, double the U.S. average (2.5%). But since the KNHI in South Korea is a single-payer system and thus a monopolistic buyer of health services, it has effectively controlled health care costs by keeping out-of-pocket expenses relatively low and stable for outpatient services (Song, 2009). Thus, many healthy people in South Korea are generally satisfied with the KNHI, at least until they need more costly intensive care due to serious illnesses or injuries (Lee et al., 2008; Song, 2009). In addition, the KNHI in South Korea has very simple rules for using health insurance, so patients do not have to deal with administrative complexities that patients in the United States may encounter. For instance, in South Korea, there are no in-network or out-of-network providers because every health care provider is contracted by the KNHI. Patients in South Korea do not have to obtain or renew health care coverage on an annual basis, which is rarely the case in the United States.
Andersen (2008) argued that features of a macrolevel health care system affect individual-level behaviors regarding health care usage. System-level differences that Korean immigrants may face in the United States can create confusion and discomfort when seeking health care. Immigrants often bring cultural beliefs, values, and attitudes formed by interactions with the institutions in their home countries. Those cultural experiences—particularly related to health care system—may influence their decisions regarding how and when to use health services (Abel, 2008). Choi (2013a) found that differences in the health insurance systems between South Korea and the United States made it challenging for Korean immigrants seeking health care. That study, however, focused mainly on health care service use, leaving the decision-making process related to purchasing health insurance unexplored. To fill this gap, this study used the health service selection framework by Leduc and Proulx (2004) to explore how premigration experiences of self-employed Korean immigrants could shape their perceptions and decisions to purchase and maintain health insurance in the United States.
We focused on self-employed Korean immigrants because they represent a significant proportion of Korean immigrants in the United States and because of their structural and sociocultural vulnerability in purchasing health insurance in the United States. Research has found that social networks among self-employed Korean Americans, which are the major source of health information for this population (Kim et al., 2015), can limit their access to health-related information, including health insurance (Oh & Jeong, 2017; Xu, 2018), thus posing challenges for health authorities in reaching this population. Investigating self-employed immigrants would provide important policy implications as to how to design health education programs and outreach efforts to address cultural barriers to expand health insurance coverage among immigrants in the United States. Even though the overall health insurance coverage increased for Korean Americans after the implementation of the ACA, little is known about how newly insured immigrant groups perceived their health insurance and whether they will retain their health plans over the long term. In-depth understanding of potential influences of sociocultural factors of ethnic minorities including premigration health care experience on their access to health care will help us address existing health care disparities among immigrant groups. Thus, this study took a qualitative approach to explore the perceptions of health insurance among self-employed Korean immigrants and how the perceptions of health insurance affected their decisions to purchase health insurance and their intentions to maintain coverage.
Methods
Participants
The present study included 24 self-employed Korean immigrants living in the Greater Los Angeles area. The Greater Los Angeles area has the largest Korean population in the United States (Esterline & Batalova, 2022). Respondents were invited to an hour-long individual interview in 2015 between March and June if they met eligibility criteria, including (1) speaking Korean as their primary language and (2) being self-employed for an extensive period. Respondents were recruited largely from local Korean ethnic churches, considering its representativeness as a social space for the study population (Min, 1992).
Table 1 provides characteristics of the participants, suggesting that our efforts to recruit the study sample from diverse backgrounds were successful. Respondents (n = 24) were 50% male and female, respectively, and the mean age was 50 years (SD = 9.7 years). The average monthly household income was US$5,643 (SD = US$2,530), and their average years of residence in the United States was 18.7 (SD = 9.1 years). More than half (62.5%) reported obtaining health insurance through California’s ACA Marketplace (Covered California) or California’s Medicaid program (Medi-Cal). In contrast, five respondents were still uninsured even after the ACA individual mandate that took effect on January 1, 2014.
Sample Characteristics and Overall Perceptions With Health Care Systems in South Korea and the United States.
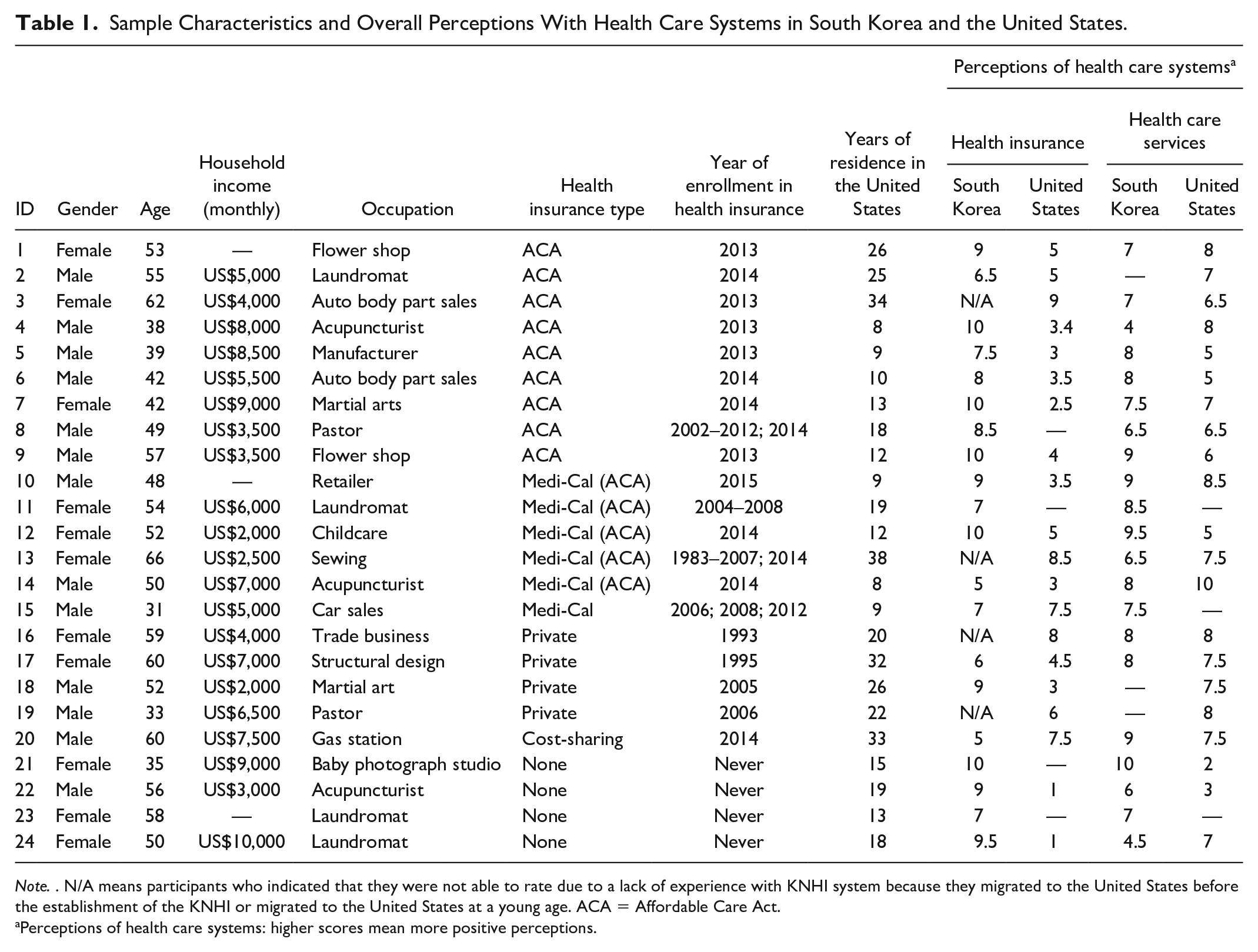
Note. . N/A means participants who indicated that they were not able to rate due to a lack of experience with KNHI system because they migrated to the United States before the establishment of the KNHI or migrated to the United States at a young age. ACA = Affordable Care Act.
Perceptions of health care systems: higher scores mean more positive perceptions.
Data Collection
After completing informed consent procedures, each respondent participated in a semistructured, in-depth interview. Respondents were asked a series of questions that focused on understanding (1) premigration/postmigration experiences of health insurance and health care services in South Korea and the United States, respectively, and (2) perceived barriers to and facilitators of purchasing health insurance in the United States. In addition, respondents were asked to rate their overall experiences with (1) health insurance and (2) health care services in both South Korea and the United States, using a scale of 1 to 10 (10 being the most positive). All interviews were conducted in Korean. Audio-recorded interviews were transcribed in Korean first and then translated into English by professional bilingual translators. The study was reviewed and approved by the Institutional Review Boards at University of Southern California.
Data Analyses
We used constant comparative methods rooted in Grounded Theory (Corbin & Strauss, 2008) to analyze the interview data. Two researchers (C.J. and H.O.) conducted independent open coding to identify themes based on the initial coding discoveries. The researchers then created separate lists of codes and categories relevant to the research questions. The two authors compared, matched, and discussed codes and categories derived from the independent open coding and reached consensus via thorough discussion. In addition to the qualitative analysis, we compared the evaluation scores that assessed how positively respondents perceived the overall attributes of health insurance and health care services in the United States and South Korea. A paired t-test was used to compare scores for health insurance and health care services between the United States and South Korea, respectively. An independent t-test was used to compare the levels of positive perceptions of U.S. health insurance between those who experienced KNHI and those who did not. The rejection level for a significance test was 0.05. Analyses were conducted using STATA 15.1.
Results
Perceived Characteristics of U.S. Health Insurance: Premigration Health Care Experience as a Sociocultural Referent
Respondents generally perceived the KNHI as superior to U.S. health insurance in terms of cost, benefits, simplicity, and accessibility. Most of the respondents who experienced the KNHI tended to use it as a standard to evaluate U.S. health insurance. One interviewee, for example, stated that “I think South Korea has really well-maintained health insurance. So, anytime, I tend to compare it with the one I have in the U.S.” (ID#1, female, 53years). During the interview, respondents frequently complained about perceived drawbacks of U.S. health insurance, using their experiences of health insurance in South Korea as a standard for comparison.
Cost
Respondents perceived health plan premium costs in the United States as much more expensive than those in South Korea, which appeared to be a critical factor in their decision not to purchase health insurance in the United States. For reference, the average monthly health insurance premiums for self-employed individuals in South Korea were around US$70 in 2016 (National Health Insurance Sharing Service, 2021), which was less than one-fourth of the average monthly premium (US$312) for an ACA marketplace plan in California for that same year (Kaiser Family Foundation, 2022). One respondent reported that she had expected to pay a similar premium for health insurance in the United States to the premium she had paid in South Korea. However, the health insurance premium in the United States far exceeded her expectation and was the main reason she did not purchase a plan. The first reason why I could not enroll in health insurance after we moved to America was that it was too expensive here. When we first came to the U.S. from South Korea, we expected it (the premium) would be about less than a hundred dollars [a month] at most. But when we moved here, the premium [for U.S. health insurance] was around several hundred dollars, so we could not enroll (ID#23, female, 58 years).
In addition to the premium costs acting as a barrier to acquiring insurance coverage, out-of-pocket costs in the United States were another barrier to seeking care. Despite being covered by insurance, respondents did not frequently use health care services in the United States as much as they did in South Korea due to the concern about copays or coinsurance, which were perceived as too expensive. Consequently, they dropped their health coverage by not paying the premium because they thought it was of no use. As a respondent explained, In South Korea, if you have your insurance card, you can go to any hospital. Even though there is co-payment, it only costs 1 or 2 dollars. It is like you get your services almost for free. When you go to a general hospital or go to a small, local hospital, you can just go without any difficulties [regarding cost]. That was really convenient (ID#1, female, 53 years).
Benefits
Some of the respondents were aware of the limited benefits of KNHI for serious illnesses requiring intensive care: I guess one negative thing I can think of [about Korean health insurance] is that a serious illness needing intensive care is not sufficiently covered by the plan although small health issues are treated quickly and without a cost concern (ID#10, male, 48 years). However, most respondents believed the coverage of benefits that KNHI provides were still better than those in the United States. A respondent explained: I think there are so many treatments not covered by health insurance in the U.S. In South Korea, however, a really serious disease, even an incurable disease is eligible for coverage, not a lot though. But still, it is covered. But over here [in the U.S.], if you actually visit [hospitals], there are so many things that are not covered (ID#6, male, 42 years).
Simplicity
As opposed to the simplicity of the single-payer system in South Korea, respondents expressed dissatisfaction with having to consider too many options when buying health insurance in the United States. One respondent, who was accustomed to the KNHI in South Korea, complained about the difficulties of finding and applying for suitable health insurance plans in the United States: In [South] Korea, everything is governed and run by the government. Since there is a government-run agency, there will always be standards. [. . .] The system itself is very fair. On the other hand, the system here in the U.S. is personal and private. You need to do your own research and apply for plans appropriate for you. That is really hard. It is not easy at all. There are no standards (ID#9, male, 57 years). In addition to the complexity of health insurance options, limited English proficiency among self-employed Korean immigrants was perceived as a relevant barrier to finding adequate health plans. Some respondents were not able to understand written documents that explain the details of each plan. As described by one respondent, Language is another issue. It is also really tough for me to look it up by myself by reading really thick booklet in English (ID#6, male, 42 years).
Accessibility
Several respondents cited confusion about access to outpatient care covered by U.S. health insurance plans. They reported that patients in South Korea have more discretion to visit any specialist without referrals from primary care providers. In contrast, patients in the United States have to follow varied rules for seeking care from a specialist provider depending on the rules of their insurance plan. In the eyes of Korean immigrants, such a system appears inconvenient and time-consuming, and discouraged some from seeking needed care. A respondent explained, For HMO (Health Maintenance Organization), we have to choose a primary care physician and go see him [when we need care] . . . requiring referrals to seek care from a hospital. So, the whole process takes forever. [. . .] But in South Korea, if you want to go to any hospital, you can just go there [without referrals] (ID#9, male, 57 years).
Perceptions of Purchasing U.S. Health Insurance: “It Is a Waste of Money”
Poor Cost-benefit Ratio of U.S. Health Insurance as a Cultural Barrier to Enrollment
It was a common perception among the respondents that U.S. health plans are not cost-efficient, thus not worth purchasing. The high cost, yet limited or poor benefits, of health insurance in the United States was cited as the main force discouraging the respondents from purchasing health insurance. A respondent, who purchased a co-op plan instead of health insurance to avoid the individual mandate penalty, explained: In the U.S., the amount of premium that a family has to pay for health insurance is too much, and there are too many blind spots. As you know, many things are different, compared to Korean insurance. Because of too much monthly payment, I could not even think about enrolling (ID#20, male, 60 years). Instead of purchasing health insurance, respondents perceived other coping strategies to deal with acute symptoms as more cost-efficient—including cash payment for health services, over-the-counter medicine based on self-diagnosis, charity care, reliance on oriental medicine, or travel to South Korea for health care.
Due to the perceived poor cost-benefit ratio of U.S. health insurance, respondents tended to view buying health insurance in the United States as a waste of money: I feel like I am wasting my money because I do not go to a hospital often. I go to a hospital once per year or not at all. Basically, I am throwing away that money (ID#21, female, 35 years). Respondents also indicated that Korean immigrants may have culturally distinct beliefs regarding the importance of health insurance for health care. A respondent stated: Korean immigrants think it is a waste of money to use money on unnecessary things [like health insurance in the U.S]. Other immigrant groups may believe that money paid for health insurance should be spent anyway, instead of thinking that it is a waste of money (ID#18, male, 52 years).
Limited In-network Providers Due to Language Barriers
A strong preference for Korean doctors among Korean immigrants due to linguistic barriers also seemed to underpin the negative cost-benefit ratio of U.S. health insurance perceived by many respondents. One respondent who had never been enrolled in health insurance plans justified her decision not to purchase health insurance by stating that: [Even with health insurance] I could not go to the hospital that I wanted. My English was poor so I had to go see a Korean doctor since I could not speak English well. But then, the insurance should be accepted by the Korean doctor. It did not work out due to many reasons (ID#21, female, 50 years). A new enrollee who purchased a health plan from a Marketplace also indicated that The inconvenience of Obama Care is that you have to go see a primary care physician. Even choosing a primary is hard because the network is so small. Since we’re Korean, we prefer Korean doctors, because of the language barrier and lots of Korean doctors are not part of the network (ID#19, male, 57 years).
Cultural Discrepancies in the Perceived Needs for Health Insurance by Generation
Differences in perceptions of health insurance may exist even between generations of Korean Americans. Korean Americans who were born and raised in the United States may have different perceptions of health insurance from Korean immigrants who were raised and socialized in South Korea. As one respondent explained, People who were born here or migrated very early in their ages from South Korea easily accept culture here in the U.S., because it is the only culture they have experienced. But people just like me, who migrated from South Korea after the age of 30 and had used benefits of Korean health insurance hate the health insurance over here. Korean immigrants from South Korea do not think the money for health insurance [in the U.S.] is something that they should pay. They think they are wasting their money (ID#5, male, 39 years).
Intention to Maintain Health Insurance
The perception that health insurance is not essential for health care appeared to negatively influence respondents’ intention to keep health insurance over the long term. Most of the post-ACA enrollees reported they purchased health insurance to avoid the penalty imposed by the individual mandates, not because they needed health coverage. One respondent mentioned: Well, it was mandatory, and I didn’t want to get fined. It’s not like I felt the need for it or anything (ID#4, male, 38 years). Another respondent indicated: the reason why I enrolled in this time was because I had to pay for penalty otherwise. I don’t think I did it for my health. I did not do it for a purpose of utilizing medical service. If I do get injured or sick, it’s cheaper to pay with cash than paying premium (ID#5, male, 39 years). The low perceived needs for health insurance along with the poor cost-benefit ratio of U.S. health insurance resulted in a lack of motivation to maintain health plans in the long term. The respondent, just mentioned earlier, expected that he would not maintain health insurance if the ACA’s individual mandate is abolished. He stated, When I become old and have to go to a hospital often, if then, I might go without feeling it is wasteful. But now, I am still at an age of thinking it is not worth it. [. . .] If Obamacare comes to an end, and if there is no mandatory enrollment, I think I would terminate it (ID#5, male, 39 years).
Quantitative Findings
Figure 1 presents scores indicating positive perceptions of health insurance and health care services in the United States and South Korea. Higher scores indicate more positive perceptions of health insurance or health care services. Respondents perceived Korean health insurance more positively (M = 8.2, SD = 1.7, and n = 20) than U.S. health insurance (M = 4.7, SD = 2.4, and n = 20), and the difference was statistically significant (t = −5.78, p < .001). With respect to health care services, on the contrary, no statistically significant difference was found between the scores for Korean health care services (M = 7.5, SD = 1.5, and n = 21) and those for U.S. health care services (M = 6.7, SD = 1.9, and n = 21). Interestingly, those who migrated to the United States before the KNHI was fully established or migrated to the United States at a young age (n = 4), thus having a lack of experience with the KNHI, perceived U.S. health insurance more positively. They also maintained health insurance coverage longer, even before the implementation of the ACA. As shown in Figure 2, the difference in the scores of respondents’ perceptions of U.S. health insurance between those respondents who experienced the KNHI (M = 3.9, SD = 1.9, and n = 20) and those who did not have sufficient experience with the KNHI (M = 7.9, SD = 1.3, and n = 4) was statistically significant (t = 4.00, p < .001).
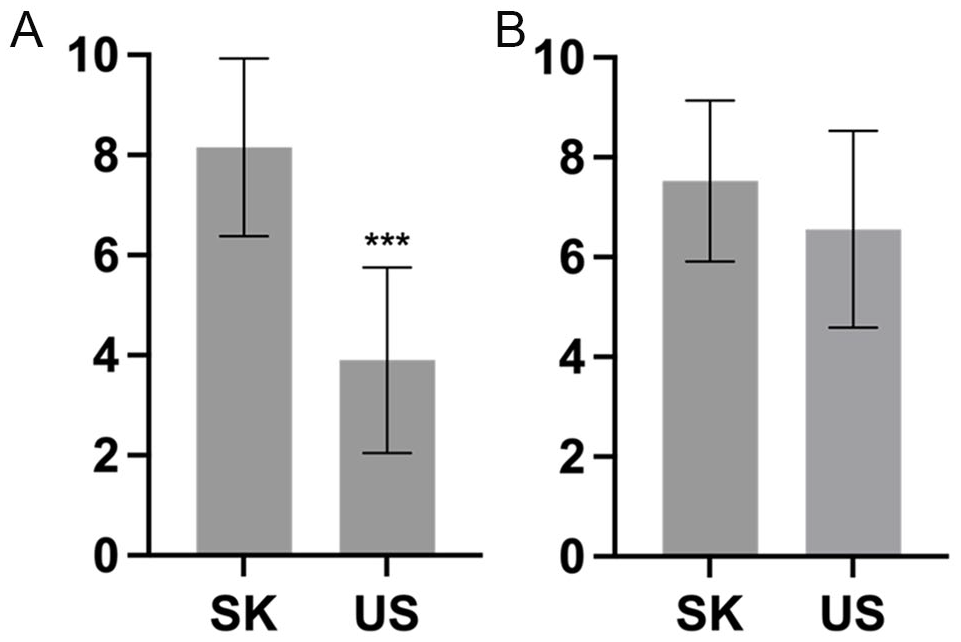
Levels of Positive Perceptions of (A) Health Insurance and (B) Health Care Services in South Korea and the United States.
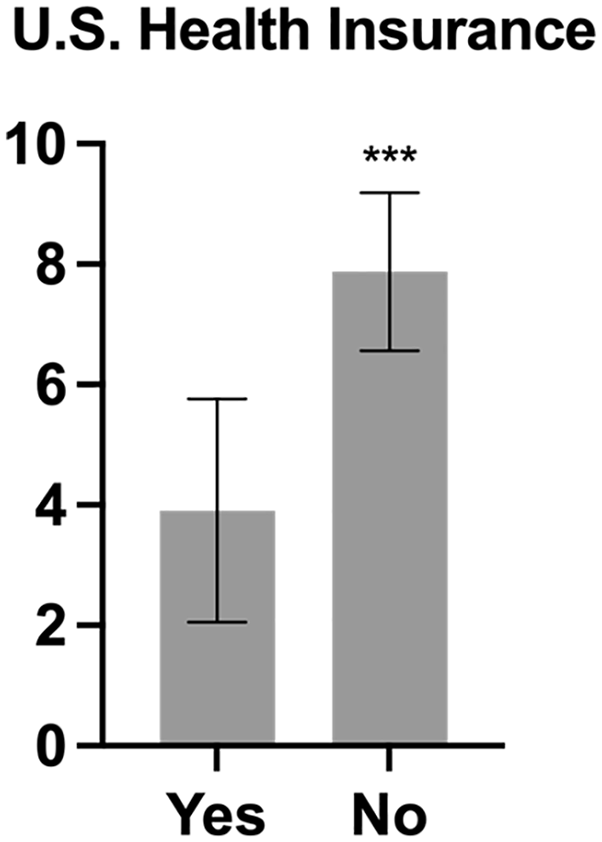
Levels of Positive Perceptions of U.S. Health Insurance by the Premigration Experience of KNHI.
Discussion
Guided by the health selection model delineating the roles of premigration experiences as a sociocultural referent in immigrants’ decision-making process regarding health care–seeking behaviors, the present study explored how premigration health care experiences among self-employed Korean immigrants affect their perceptions of health insurance in the United States and their intention to purchase and maintain health insurance. Our findings demonstrated that Korean immigrants had culturally shaped ideas about health insurance, seemingly internalized from past experiences with the KHNI, a single-payer and universal health care system. Korean immigrants’ perceptions of what health insurance should offer do not seem to match what actual health insurance plans offer in the United States. As with previous literature (Choi, 2013b; Leduc & Proulx, 2004; Portes et al., 1992), premigration experiences in the countries of origin played a critical role in the interpretations of the quality and degree of satisfaction with health insurance, use of health services, and health care behaviors. As shown in the data, respondents who migrated after the KNHI was implemented expressed dissatisfaction about the rules and processes for seeking care in the United States by referencing previous health care experiences during the premigration period. Those who did not have sufficient experience with the KNHI showed relatively higher levels of satisfaction with U.S. health insurance. Apparently, such negative attitudes toward U.S. health insurance among participants impeded their purchase of health insurance, while encouraging them to rely on prior coping strategies for acute symptoms when uninsured (Choi, 2013a; Oh & Jeong, 2017).
Our findings suggest that high uninsured rates among Korean Americans are not only triggered by individuals’ rationales for maximizing economic returns based on their own cost-benefit analysis, but also driven by their culturally established beliefs about what health insurance should offer. The mismatch between an imaginary, ideal health insurance plan, and actual health insurance plans available in the United States could be exacerbated by self-employed Korean immigrants’ limited access to information regarding health insurance. The self-employed Korean immigrants were found to be surrounded by ethnically and occupationally homogeneous social networks, which may limit their access to a fuller range of information related to health insurance and may reinforce culturally embedded norms with regard to purchasing health insurance (Oh & Jeong, 2017).
It is noteworthy that perceptions of a health care system can be biased by limited personal experiences and thus one’s understanding of a health care system (including the role of health insurance) might not reflect the health care system’s objective features. Despite the KNHI system’s higher out-of-pocket spending (for serious illness) compared with the U.S. system, a majority of respondents reported that copayments in South Korea were less expensive than in the United States. This is true but only for routine outpatient care, where copayments in the KNHI may be as little as $1–$5 U.S. dollars.
Such a contradictory result may also be attributable to the healthy immigrant effect, the phenomenon that immigrants are generally healthier than the native-born in the host countries (Kennedy et al., 2015). It is plausible that relatively healthy Koreans migrated to the United States and were satisfied with the KNHI having not experienced the limited benefits for serious illnesses within the South Korean health care system. In addition, they would have experienced very low out-of-pocket costs for routine outpatient care adding to a positive image of the KNHI. Healthy Korean immigrants, pressured to select self-employment by various socio-structural barriers to mainstream employment (Min, 1984), face expensive health insurance plans on the individual market that come with limited benefits and very high out-of-pocket costs for routine care, thus leading to very negative perceptions of U.S. health insurance. From this perspective, it is critical to understand that self-employed Korean immigrants may encounter additional sociocultural, psychological barriers to purchasing health plans in the United States, compared with other immigrant groups who may have relatively positive perceptions and attitudes toward U.S. health insurance, especially if other immigrant groups were more likely to experience employer-based or public plans such as Medicaid or Medicare.
Study limitations should be noted. The recruitment of respondents (Korean immigrants) was based on specific employment (self-employed) and geographic (greater Los Angeles area) criteria to better understand the experiences among Korean immigrants adapting to the U.S. health care system. As such, interpretation of the results should be limited to this population and cannot be generalized to other immigrant experiences. In addition, the cross-sectional study design does not allow us to establish causal inferences between premigration and postmigration experiences of the health care systems in respondents’ home and host countries. The study does not fully account for health status—which is closely related to the need for health services—and health service utilization history of the respondents, that may have influenced respondent’s perceptions and experiences of the health care systems in either country. Taken together, these factors may be related to patients’ willingness to pay for health insurance and their attitudes toward purchasing health insurance in the United States. Thus, cautious interpretation of the study’s findings is required. That said, the associations identified in the qualitative interviews were supported by the quantitative analyses in the present study.
This study makes an important contribution to the literature with findings that suggest immigrants’ premigration health system experiences affect their perceptions, attitudes, and behaviors in host country’ health care systems. More research is needed to understand how culturally determined values, norms, and beliefs affect how immigrant groups adapt to a new health care system. Study findings suggest it may not be enough to merely provide health insurance information to immigrant groups to increase their health insurance coverage. Rather, health educators should consider how specific culturally embedded beliefs and norms about health insurance (based on premigration experiences) could affect behaviors regarding health insurance enrollment for immigrant populations. Educational interventions for self-employed Korean immigrants, for example, might include information on the purpose of health insurance, benefits, financial security, and how to access services, in addition to basic information on insurance plans.
Footnotes
Compliance With Ethical Standards
All procedures performed were in accordance with the ethical standards of the institutional human research ethics committee (University of Southern California: UP-15-00175) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability
Data from this study are available on request to the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hamovitch Center for Science in the Human Services at the USC Suzanne Dworak-Peck School of Social Work [grant number: not applicable].