
Abstract
Adolescents belonging to minority or marginalized groups often experience discrimination, which may negatively affect their mental and physical health. Using the dataset of the 2018 Health Behaviour in School-Aged Children (HBSC) study, we analyzed perceived discrimination based on various grounds in four minority groups of schoolchildren in Ireland: sexual minority youth, youth living with a disability or chronic condition, immigrant youth, and youth belonging to the Traveller community. To minimize the potential confounding effect of psycho-social contextual factors, we used a case-control matching approach, comparing minority groups with their non-minority peers matched by gender, age group, and social class. Minority groups were significantly more likely than their matched non-minority counterparts to report discrimination, not only on the basis of their minority status but also on other grounds. These associations varied in their effect size. We discuss educational and policy implications of the findings for reducing discrimination and structural stigma in school settings.
Keywords
Children and adolescents belonging to marginalized groups are more vulnerable to the negative consequences of discrimination than adults (Schmitt et al., 2014). Experiences of discrimination in adolescence are associated with poor psycho-social adjustment and academic performance (Hood et al., 2017). The grounds of discrimination include, among others, sexual orientation (Almeida et al., 2009), disability or chronic conditions (Heary et al., 2014), immigrant status or belonging to a racial minority (Mesch et al., 2008), and belonging to ethnic minority groups such as Roma (Kolarcik et al., 2015).
In Ireland, the Equal Status Acts 2000–2018 prohibit discrimination based on (1) gender, (2) marital status, (3) family status, (4) age, (5) disability, (6) sexual orientation, (7) race, (8) religion, and (9) membership of the Traveller community. According to a recent report (Department of Children, Equality, Disability, Integration and Youth [DCEDIY], 2022), nearly half (47%) of young people below 18 years in Ireland have ever experienced discrimination based on their age, while around 3% have been discriminated against based on belonging to the Traveller community. Prevalence of discrimination based on other grounds were between these two values. Discrimination manifested in various forms, including being shown less courtesy or respect, receiving poorer service than others, perceiving others thinking that they were not smart, or others acting as if they were afraid of them. Almost one in five of 17- to 18-year-old youth experienced being threatened or harassed. In some cases, gender, age, social class, or minority group was associated with the prevalence of discrimination, which warrants further analysis accounting for these sociodemographic characteristics. In this brief report, we present the rates of perceived discrimination on various grounds among minority and non-minority adolescents in Ireland. We used case-control matching to account for potential sociodemographic differences.
Method
Sample and Procedure
A nationally representative sample of 6,242 adolescents aged 12 to 19 (M age: 15.52 ± 1.22 years) was investigated. They participated in the 2018 data collection round of the Irish Health Behaviour in School-Aged Children (HBSC), a World Health Organization (WHO) collaborative cross-cultural study. The HBSC is an adolescent population health study conducted every four years in 51 countries in the WHO European Region and Canada, using a cross-sectional study design. A clustered sampling frame was used, with classrooms as the primary units. The survey utilized an anonymous questionnaire that adolescents completed in the classroom. Details of the HBSC methodology are reported elsewhere (Inchley et al., 2018; Költő et al., 2020). Parents and adolescents gave informed consent to participation. Participants were told that they were free not to answer any questions and/or to withdraw their participation at any time. The study was approved by the Research Ethics Committee of the University of Galway.
Measures
Sociodemographic Factors
Participants’ gender was assessed with a single item (“Are you a boy or a girl?” with response options “A boy” / “A girl”). In line with HBSC Ireland reporting practice (e.g., Költő et al., 2020), participants were assigned into three age groups: 12- to 14-year-olds, 15- to 17-year-olds, and those aged 18 or older. Social class was based on the occupation and employment status of their parents as reported by participants. These were classified into the categories used by the Irish Central Statistics Office (2016), and subsequently collapsed into three social class groups. The highest social classes included children of professional and managerial or technical workers. Children of non-manual and skilled manual workers were categorized into middle social classes. The lowest social classes included children of semi-skilled and unskilled workers.
Minority Status
Participants were asked which gender partners they were attracted to, with response options “Girls,” “Boys,” “Both girls and boys,” or “I am not attracted yet to anyone.” Girls attracted to girls, boys attracted to boys, and participants attracted to both-gender partners were categorized as sexual minority. This classification is routinely used in the HBSC network (e.g., Költő et al., 2021). Those who reported having a long-term illness, disability, or a medical condition diagnosed by a doctor were categorized as having a disability or chronic condition. Participants were asked in which country they were born. Those born outside of Ireland were categorized as first-generation immigrants. Participants who reported being a member of the Traveller community (an Indigenous ethnic minority in Ireland with distinctive cultural and nomadic practices) were categorized as such. These items are also routinely used in HBSC (Költő et al., 2020, 2021).
Perceived Discrimination
Participants were asked how often they were treated unfairly or negatively due to their age, gender, disability status, race, sexual orientation, religion, membership of the Traveller community or other reasons, on a scale ranging from never (1) to very often (5). For each of the eight grounds, responses were dichotomized into “never” versus “ever.” A textbox was provided in the questionnaire to describe “other” reasons.
Statistical Analysis
To eliminate the potential confounding effects of psycho-social contextual factors, an iterative case-control matching technique was employed. We attempted to match each minority participant (case) with another participant not belonging to the given minority group but having the same gender and belonging to the same age and social class group (match). Gender, age, and social class categories for matching were the same as described in the “Sociodemographic Factors” section. For each case, first, we searched for the match within the same classroom. If no match was found, we extended the search to the same school, then the same county, and finally the same region. If no match was found within the same region, the case remained unmatched.
Analyses were carried out in SPSS (Version 25). Chi-square tests were used to test the associations between minority status (yes / no) and the dichotomous discrimination variables (never / ever being discriminated against). Threshold of statistical significance was set at p < .05. To prevent the accumulation of Type I Error, p values were adjusted using the Holm–Bonferroni method (Holm, 1979). For each test, effect size (phi) is provided. In line with the guidelines of Cohen (1988), absolute values of phi ≤ .10 were interpreted as negligible, phi between .10 and .29 as small, phi between .30 and .49 as medium, and phi ≥ .50 as large. For all statistical tests, pairwise selection was used.
Results
Descriptive statistics are presented in Table 1. Around one tenth of the sample belonged to the sexual minority group; around 22% reported having a disability or chronic condition; around 15% were first-generation immigrants, and 2% belonged to the Traveller community. In the full sample, prevalence of ever feeling discriminated against ranged from 3% (based on Traveller status) to 51% (based on “other reasons”).
Descriptive Statistics (N = 6,242).
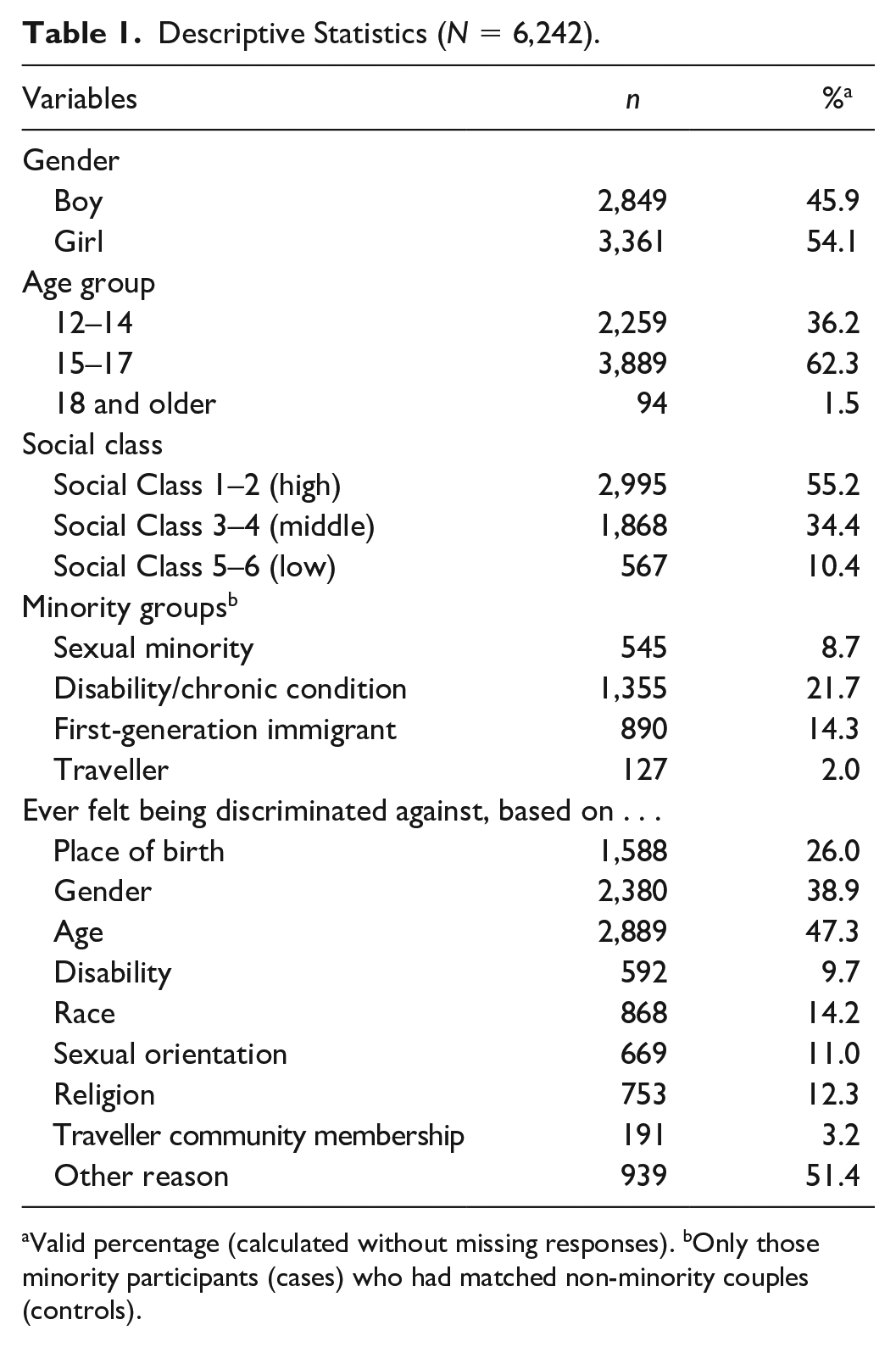
Valid percentage (calculated without missing responses). bOnly those minority participants (cases) who had matched non-minority couples (controls).
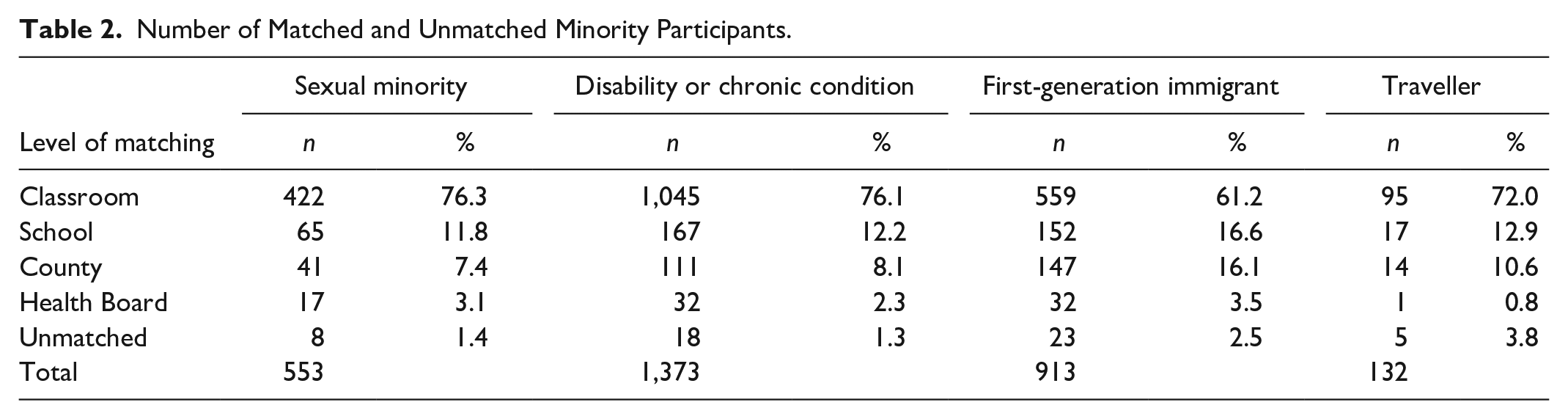
Table 2 shows the proportion of matching on different levels and unmatched participants. For each four groups, the largest number of non-minority counterparts (matched controls) were found in the classroom, and the smallest number within the same region. The proportion of unmatched cases ranged from 1.3% (disability and chronic conditions) to 3.8% (Travellers).
Number of Matched and Unmatched Minority Participants.
Associations between minority status and ever being discriminated against are presented in Table 3. Members of the minority groups were significantly more likely than their matches to feel discriminated against on the basis of their minority status in each group. Effect sizes varied by group. Large effect sizes were observed for sexual minority and Traveller adolescents; a medium effect size was observed for immigrant adolescents; a small effect size was observed for adolescents with a disability or chronic condition.
Proportion Who Ever Felt Discriminated Against in Minority and Matched Non-Minority Participants, % (n).
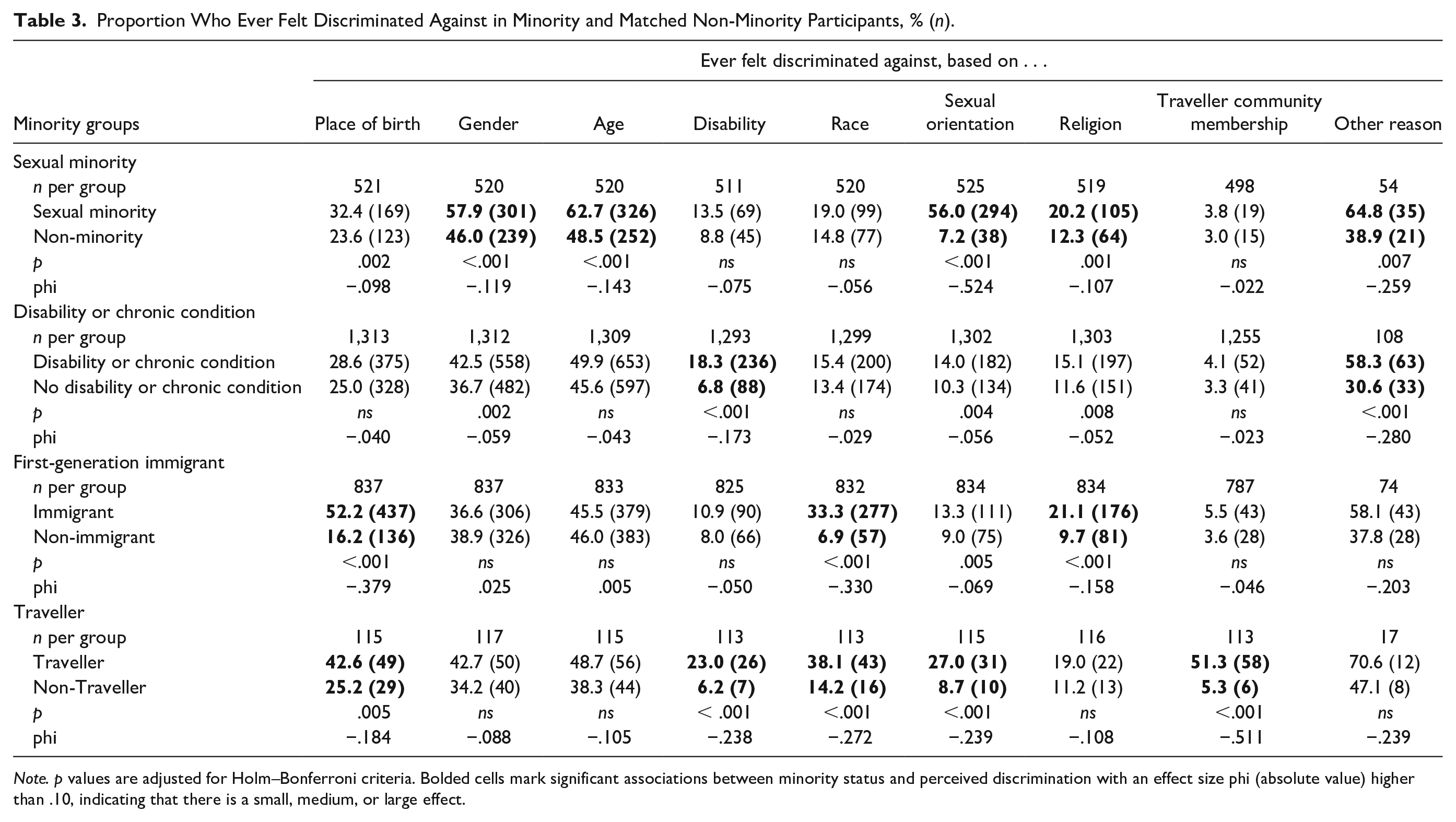
Note. p values are adjusted for Holm–Bonferroni criteria. Bolded cells mark significant associations between minority status and perceived discrimination with an effect size phi (absolute value) higher than .10, indicating that there is a small, medium, or large effect.
Members of minority groups were also significantly more likely than their non-minority matches to report discrimination based on grounds other than their minority status, all with small effect sizes. Compared their matched groups, sexual minority adolescents reported significantly higher rates of discrimination based on their gender, age, religion, and “other reasons.” Adolescents with a disability or chronic condition reported significantly higher rates of discrimination based on “other reasons.” Immigrant adolescents reported significantly higher rates of discrimination based on religion and “other reasons,” and those who were members of the Traveller community reported higher rates of discrimination based on place of birth, disability, race, and sexual orientation. There were some other statistically significant associations, but their effect sizes were negligible.
Discussion
Proportionally, unmatched cases among Traveller participants were almost threefold (3.8%) than among participants living with a disability or chronic condition (1.3%). Families of the Traveller youth are most likely to belong to the lowest social classes, for whom often no matched controls could be found. This probably contributed to the relatively large proportion of unmatched Traveller participants.
Adolescents belonging to minority groups are more likely than their matches to be discriminated on the basis of their minority status, as well as on other grounds. This may reflect a “negative halo” or “horn effect,” where a person who has a characteristic seen as undesirable, is attributed with other negative features (see Költő et al., 2021).
In some cases, these additional grounds of discrimination seem rather unequivocal. For instance, that immigrant adolescents experience more discrimination based on their religion than their non-immigrant peers can be explained by the fact that in Ireland, the majority of people of Irish descent identify as Catholic, while many people from immigrant families have other faiths (Conner, 2019). Similarly, Traveller adolescents may be more likely to experience discrimination based on disability due to the fact that members of the Traveller community are more likely than non-Travellers to have poor health (Quirke et al., 2020).
Other associations—such as sexual minority youth being more likely than their non-minority peers to report discrimination based on their religion, or Traveller participants being discriminated against based on their sexual orientation—are not so easy to explain. We believe these findings can be interpreted using the theoretical approach of structural stigma, by which culturally embedded notions of normativity lead to minority individuals being implicitly understood as undesirable or inferior, compared with the majority (Almeida et al., 2009; Heary et al., 2014). Other theoretical models that are helpful to understand discrimination in adolescents include the social rejection and social discount approaches. These models attribute perceived discrimination to social status and its collective devaluation (Mesch et al., 2008).
Implications for Policy and Practice
Given the ample evidence of the negative consequences of perceived discrimination on health and well-being, especially for adolescents (Schmitt et al., 2014), anti-discrimination policies and interventions that reduce social exclusion and bullying need to be implemented. The Irish government seems to be attentive to the frequent occurrence of discrimination, as reflected in both Irish law and policy strategy (DCEDIY, 2022). Increasing cultural awareness, tolerance, and empathy can make a difference for the inclusion of minority youth in society. Teachers, youth workers, and service providers need to be trained on how to cater for the needs of all minority young people. Their training should cover biased perception and stigma as well as skills on how to intervene when required. Abreu et al. (2016) pointed out the valuable role of school counselors in providing support, prevention, and education in reducing oppression in the school environments for sexual and gender minority youth. The authors found that LGBT+ (lesbian, gay, bisexual, and transgender) youth had significantly better mental health in schools where anti-bullying policies explicitly ban bullying and harassment based on someone’s sexual orientation or gender identity than in schools without such explicit policies. These insights may be extended to discrimination and bullying that target other minority groups.
Strengths and Limitations
We believe that the nationally representative sample and the established methodology of the HBSC study give strength to our findings. The case-control matching strategy that sought matched controls within the same classroom first may have been able to parse out confounding effects not only for sociodemographic factors, but also those stemming from the clustered sampling technique employed by HBSC.
However, there are some limitations. First, the analysis does not account for multiple minority statuses—that someone belongs to a certain minority group does not imply that this is the only way they are marginalized. Likewise, matched non-minority participants could be members of another minority group. Part of the intersecting marginalization is that girls and adolescents of lower socioeconomic status might experience more discrimination than boys and adolescents from more affluent backgrounds. While the case-control matching accounts for these effects, further studies need to carry out similar analyses disaggregated for genders and socioeconomic groups (if subsample sizes allow meaningful comparisons). Second, we did not ask participants about who treated them unfairly, in what context, and we limited our analysis to describing prevalence of discrimination. More work is needed to better understand the context, mechanisms, and impacts of discrimination. Third, data were collected from adolescents in schools. Rates of school completion in Ireland are high (> 90%), but those from minority groups and those experiencing discrimination are more likely to leave school early. Thus, is it important to consider the data presented as representing schoolchildren and not all adolescents. Number of participants in the Traveller subsample and their matches was particularly small, which prompts us to interpret those findings with caution. Fourth, there are various other marginalized groups (e.g., young carers, homeless youth, or those living in institutional care) who also face social exclusion, discrimination, and social stigma. Further studies are needed to understand their experiences of discrimination. Finally, we have used a binary categorization (boy/girl) to classify gender of participants and their sexual attraction, which neglects the lived experiences of trans and other gender minority adolescents. The international HBSC research network is currently in the process of developing measures to categorize sexual and gender minority youth in a more inclusive fashion.
Conclusion
Adolescents in Ireland who belong to minority groups (sexual minority youth, having a disability or chronic condition, youth with immigrant background or belonging to the Traveller community) are more likely than their non-minority peers to perceive discrimination. Discrimination due to their minority status is especially salient. However, in all groups, there is at least one additional ground of unfair treatment that disproportionately affects the given minority group. This might reflect a “negative halo” or “horn effect” and warrants urgent interventions and policy changes. Further studies are needed to better understand context of and causal mechanisms behind the discrimination experienced by adolescents.
Footnotes
Authors’ Note
The Health Behaviour in School-Aged Children (HBSC) is an international study carried out in collaboration with WHO/EURO. The International Coordinator of the 2017–2018 survey was Joanna Inchley (University of Glasgow, Scotland) and the Data Bank Manager was Oddrun Samdal (University of Bergen, Norway). The Principal Investigator of HBSC Ireland is Saoirse Nic Gabhainn (University of Galway, Ireland). For details of HBSC international, see http://www.hbsc.org. For details of HBSC Ireland, see ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Health Behaviour in School-Aged Children (HBSC) study in Ireland was funded by the Department of Health.
Ethical Approval
The study was approved by the Research Ethics Committee of the National University of Ireland Galway.