
Abstract
Motivational interviewing is an evidence-based counseling approach. However, its learning processes and their influencing factors are understudied, failing to address the suboptimal use of motivational interviewing in clinical practice. A participatory action research was conducted in collaboration with 16 primary care clinicians, who encountered similar challenges through their previous counseling approaches. The study aimed to facilitate and describe the clinicians’ professional transformation through interprofessional communities of practice on motivational interviewing (ICP-MI). Data were collected using the principal investigator’s research journal and participant observation of four independent ICP-MIs (76 h) followed by focus groups (8 h). The co-participants performed inductive qualitative data analysis. Results report that learning motivational interviewing requires a paradigm shift from health experts to health guides. The learning processes were initiated by the creation of an openness to the MI spirit and rapidly evolved into iterative processes of MI spirit embodiment and MI skill building. The intrinsic influencing factors involved the clinician’s personal traits and professional background; the extrinsic influencing factor was the shared culture disseminating the expert care model. Previously described in a fragmented manner, motivational interviewing learning processes, and its influencing factors were presented as integrated findings. Considerations in elaborating effective MI training/implementation programs are discussed for clinicians, trainers, and decision-makers. Future areas of investigation are also highlighted calling forth the research community to contribute to knowledge advancement on health education in primary care.
Keywords
Introduction
In Canada, chronic diseases are the leading causes of death (Statistics Canada, 2021). Still, 80% of cardiovascular diseases and 40% of cancers could be avoided by adherence to healthy ways of living (World Health Organization, 2005). Accordingly, renowned models, such as the chronic care model (Wagner et al., 2001), recognize the crucial contribution of primary care (PC) clinicians’ proactive interventions in this field as chronic diseases are the most prevalent health condition encounter in this clinical setting (Smith et al., 2016).
Motivational interviewing (MI) is an evidence-based counseling approach that is highly disseminated in PC (Rochfort et al., 2018). Miller and Rollnick (2013) describe MI as a person-centered conversation style evoking and fostering patients’ intrinsic motivations about health behavior change. MI communication skills relate to asking open-ended questions, providing reflective listening, affirming patients’ self-efficacy, and offering solicited health education, which are based on relational abilities including compassion, acceptance, collaboration, and evocation. The MI method is initiated by an engagement process, which establishes a working alliance; it is followed by a focalization process, which collectively identifies the targeted behavioral health goal; then, comes the evocation process, which elicits/reinforces the patient’s personal motivations to adopt this behavior; and, ultimately, the planification process, through which the clinician consolidates the patient’s commitment to change by supporting it with an action plan.
Following an introductory training, PC clinicians frequently report feelings of discomfort and incompetence with the approach as they hold limited counseling knowledge and skills (Brobeck et al., 2011; Midboe et al., 2011; Östlund et al., 2015; Sargeant et al., 2008). Although introductory training is broadly provided and succeeds in initiating knowledge acquisition (Sӧderlund et al., 2011), learnings wear away over a 6-month period and rarely result in knowledge translation in practice (Schwalbe et al., 2014). Extensive training involving coaching/supervision activities would be required, yet such training programs are understudied (Schwalbe et al., 2014).
To address these knowledge gaps, this study aimed to facilitate and describe the learning processes and influencing factors of PC clinicians who had participated in interprofessional communities of practice on motivational interviewing (ICP-MI).
Methods
Research Design
A participatory action research (PAR) approach was conducted as described by Kemmis et al. (2014). This inquiry aims to facilitate professional development while dealing with professional/organizational challenges by implementing concrete actions targeted at co-participants’ practice/workplaces. The PAR approach serves to bridge gaps between research and practice through a singular perspective—as stakeholders directly concerned with the studied phenomenon engage in research as co-participants. To succeed in this endeavor, a cyclical process of reflection/planning/action phases is conducted until the co-participants are satisfied with their professional transformation through a minimum of three cycles (Kemmis et al., 2014). In this study, 10 cycles were completed over a year as illustrated in Figure 1 and the methodology used is detailed in another publication (Langlois et al., 2014).
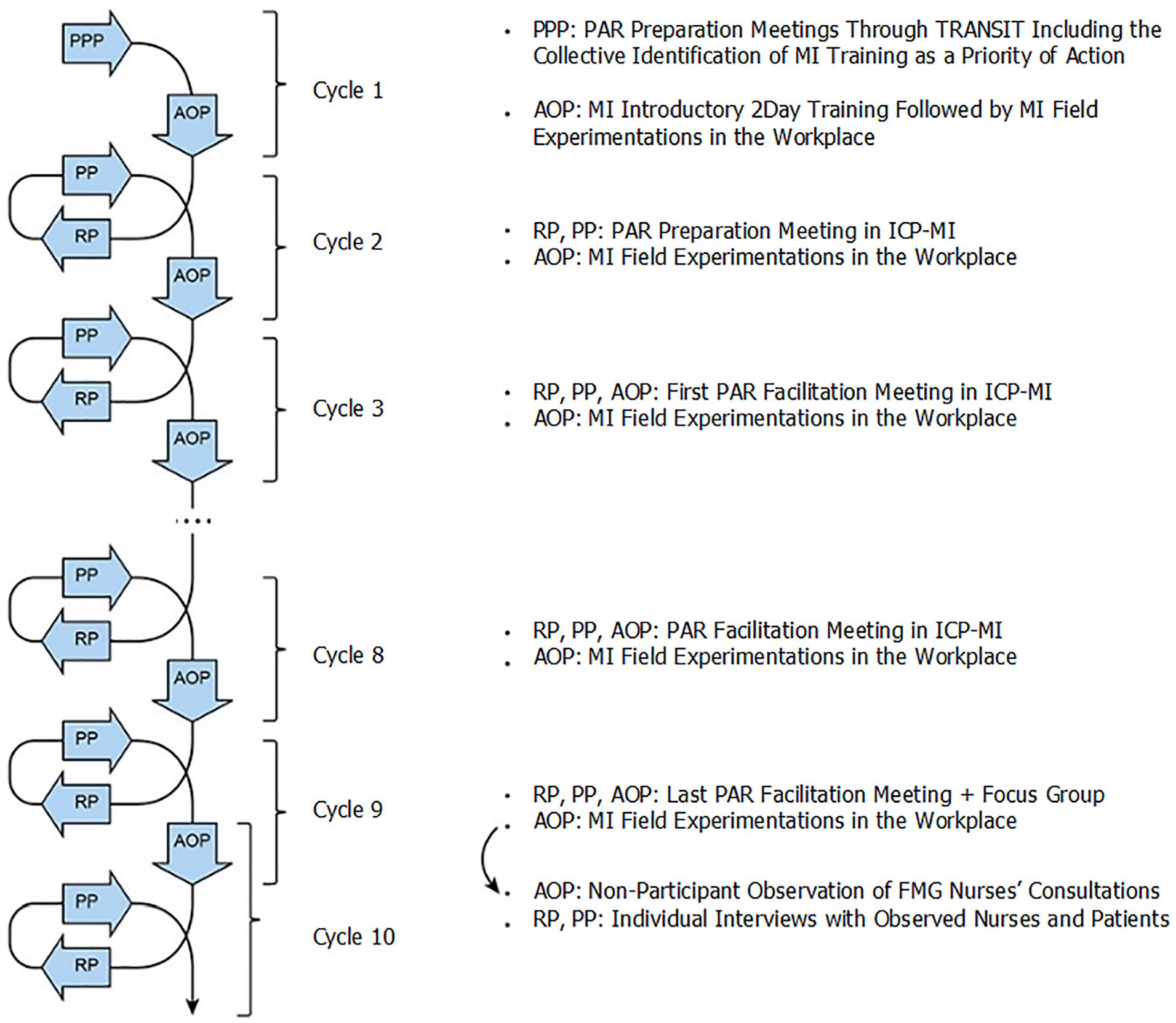
The cyclical process of this participatory action research.
Research Context and Intervention
The study was undertaken in a suburban city near Montreal, Canada. It originated from a research program called TRANSIT. Using a participatory approach, TRANSIT participants, including patients, caregivers, clinicians, administrators, and researchers, collectively identified different priorities for action to improve chronic disease prevention/management in PC, including the need of MI training for clinicians (Lalonde et al., 2014). The study stems from this consultation.
The principal investigator (S.L.) facilitated the ICP-MIs being a PC nurse, doctoral candidate, and an MI network of trainers (MINT) member. Each ICP-MI entailed seven meetings over almost a year and, overall, 19 h of training. While considering the clinicians’ learning needs and preferences, ongoing coaching/supervision were delivered using case discussions, practical exercises, interactive quizzes, and analysis of MI videos. The collaborative design of the training program and the impact of ICP-MI on PC practices are presented in other publications (Langlois & Goudreau, 2022a, 2022b; Langlois et al., 2022).
Participants’ Recruitment
Before the study, 120 clinicians involved in the TRANSIT program were invited to attend a two-day training on MI provided by MINT members. Through purposive sampling among the 45 clinicians who participated in this introductory training, 16 clinicians were recruited in person or by email/telephone by the principal investigator once the study was approved by the affiliated health care center and the university ethics/scientific committees. Written informed consent were signed, and four ICP-MIs were then created. The inclusion criteria included: (a) participation in the TRANSIT program as a PC clinician, (b) attendance to an introductory MI training in the past 2 years through TRANSIT or an equivalent, and (c) availability/interest to participate in ICP-MI meetings. The complementary professional backgrounds of the co-participants strengthen the conduct of the study based on workplace learning in continuing interprofessional education (Kitto et al., 2012). Two clinicians dropped out mid-project for personal reasons. After PAR facilitation, 12 clinicians participated in focus groups after signing a declaration of informed consent presented in person by the principal investigator.
Data Collection
Data collection involved three methods: a research journal, participant observation, and focus groups.
The research journal is used in PAR to record the study-related pedagogical/methodological decision-making processes (Kemmis et al., 2014), serving to compile field notes during observational methods and support data analysis (Pope & Mays, 2020). The research journal was useful to: register important collaborative decisions taken by co-participants and the principal investigator’s doctoral supervisor (J.G.); the triangulation of data collection methods; and initiate data analysis.
Participant observation is frequently used in action research, being related to the principles of researcher–practitioner collaboration (Kemmis et al., 2014). The researcher acts as an external facilitator to explore the practitioners’ perspectives regarding the studied phenomenon and participate in the planning of the collective actions conducted to reach their professional empowerment (Kemmis et al., 2014). Participant observation was used during ICP-MI meetings, totalizing 76 h of observation; meetings were recorded and transcribed according to the methodological decisions collaboratively made by co-participants.
The focus group supports interactive exchanges among participants to describe a range of experiences/perspectives regarding the studied phenomenon (Pope & Mays, 2020). In PAR, it encourages power sharing between co-participants, facilitating its transformational process by stimulating critical reflection to reach professional/organizational change (Chiu, 2003). For this study, four focus groups (one/ICP-MI) were co-facilitated by the principal investigator and an external researcher once ICP-MI meetings ended. Each group discussion lasted for 45 to 60 min. A guide was elaborated to ensure consistency across groups and clarification of important aspects regarding the studied phenomenon. Introductory questions invited clinicians to elaborate on their learning journey followed by specific questions exploring the clinicians’ critical learning moments and specific learning challenges/facilitators.
Data Analysis
A general inductive approach, as described by Thomas (2006), guided data analysis. This approach is structured in five steps: immersion in the raw data, followed by data codification, segmentation, recontextualization, and conceptualization (Thomas, 2006). The data reduction process was supported by QDA-Miner software. The principal investigator worked collaboratively with her doctoral supervisor (J.G.) to perform intercoder reliability. As recommended (Kemmis et al., 2014; Thomas, 2006), all co-participants were invited to contribute to the last step of data analysis to validate the preliminary results and confirm data saturation. Six clinicians participated in this research activity during a 1-hour meeting. The researchers presented their data reduction process and moderated discussions to collectively determine the final research findings.
Results
Clinicians’ Profiles
The clinicians’ profiles are detailed in Table 1.
Study Participants’ Profiles.
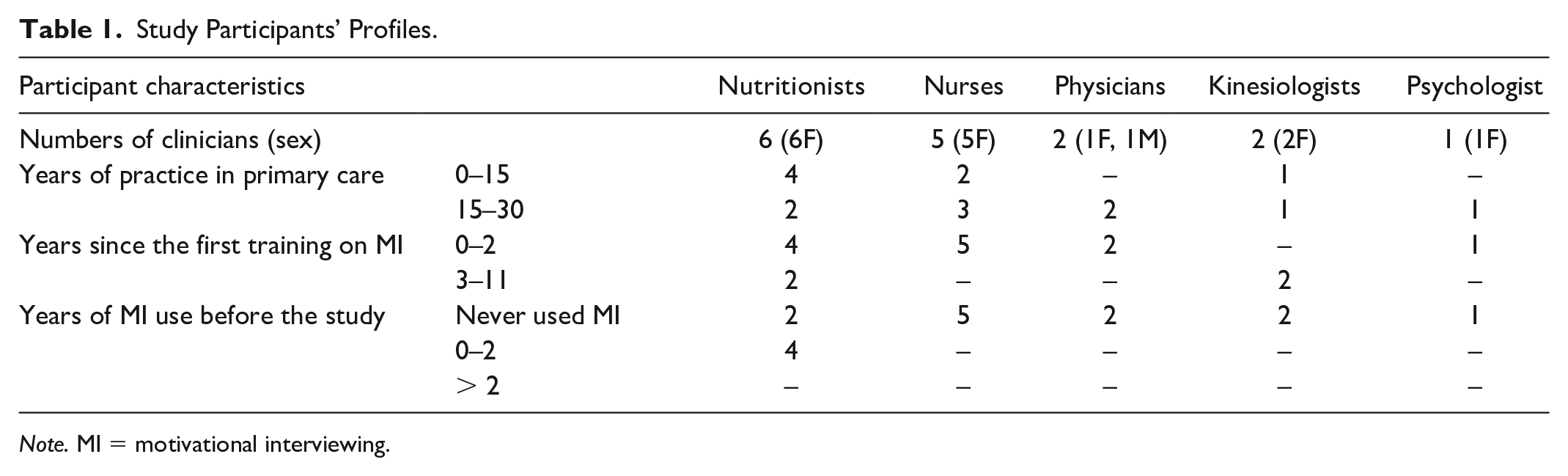
Note. MI = motivational interviewing.
MI Learning Processes and Influencing Factors
Globally, PAR co-participants experienced MI learning as evolving from health experts to health guides. This learning journey started with demystifying the MI spirit, as the fundamentals of the approach. Afterwards, they progressed to embody the MI spirit and build MI skills through iterative processes. Undertaking a paradigmatic shift and developing novel counseling abilities were the clinicians’ critical learning moments. Three influencing factors were reported that at times facilitated their learning processes but mostly complexified their learning journey: the clinicians’ personal traits, professional background, and a shared professional culture prevailing for a clinician-centered approach. Figure 2 provides an overview of the research findings. Observational data are then summarized and supported by quotations extracted from the participant observation of ICP-MI meetings and the focus groups.
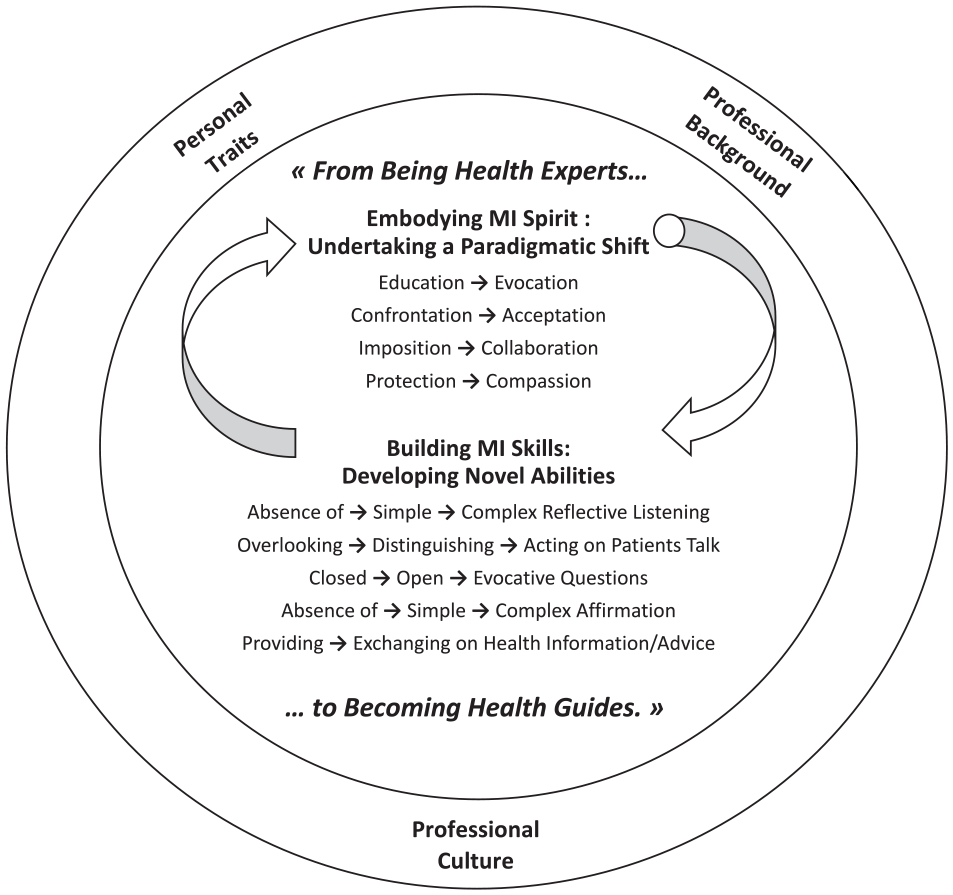
Motivational interviewing learning processes and influencing factors.
Embodying the MI Spirit: Undertaking a Paradigmatic Shift
The clinicians succeeded in learning the MI spirit by realizing their previous tendency to provide unsolicited and standardized health education, rather than evoking patients’ own ideas about change.
I am going to give you so much information that you are going to say “Eureka! I will do it!” So, I was in those old patterns and I was exhausted because there were no results. MI had lit something inside of me a long time ago in that regard. (AK)
Clinicians also became aware of past confrontational interventions as a benevolent attempt to convince patients to change behaviors. Through MI, they learned to accept the patients’ ambivalence with a nonjudgmental attitude. Although nurturing an unconditional positive regard for patients is fundamental, it was reported as challenging, especially when the patients’ behaviors challenged the clinicians’ values.
The tendency that we have, whether we are men or women, is to be . . . castrating! We believe that the thought of the other is not okay, and that our own is. When I have this in my mind, I must change my attitude. “Open yourself. Look at who’s in front of you. He is not there yet, it is okay.” (. . .) It’s the patients who are the experts. I give them back their autonomy of choice and power. (AN)
The clinicians’ endeavor to embody the MI spirit helped them to refrain from imposing health care decisions, instead evolving into collaborating with patients through a shared decision-making process.
I realize that respecting patients’ autonomy is crucial. I think more about this with my patients. I leave the choices to them, and I reaffirm their engagement in healthcare decisions. (BNJ)
Learning the MI spirit was described as a shift in the clinicians’ mind-set: from one related to the wish to protect patients from their lifestyle choices, to another related to the establishing of a therapeutic alliance and prioritizing patients’ welfare according to their unique perspective of health.
One sentence that struck me was that MI had sown seeds of change. This illustrates our need to let go and let the patients make their own choices while leaving the door open. The patients develop their life projects, and we must let go of wanting to save people from themselves. (CIL)
Building MI Skills: Developing Novel Abilities
Active listening was rarely used by clinicians before the study. Through MI, they developed their ability to listen carefully and to skillfully reflect the patients’ discourse to personalize counseling interventions.
MI helped me to make more reflections and more reinforcement; to let the patients talk about their way of seeing their problems. It helped me to better understand the situation and to intervene effectively. (DM)
Through MI, some clinicians also developed complex reflective listening skills, such as amplified reflections—that is, a summary of a person’s discourse translated into an overstatement. This skill serves to shift conversational directions while evoking the other side of ambivalence.
The patient tells me, “I do not move.” So I reflect, “Okay, you do not move at all.” And he corrects me, “Well, I don’t move . . . I move a little.” Aaah, it all comes out! I did not say “You know, it’s important to move. Blablabla!” Now, there is maturity in my interviews. And I finish by saying “Well, for someone who did not move, this is not bad at all!” (AK)
Developing mindful counseling practices was novel for clinicians. Through ICP-MI, they could discern and intentionally intervene to reinforce intrinsic motivations to change according to patient talk—that is, “Sustain talk and change talk are conceptually opposite—the person’s arguments against and for change.” (Miller & Rollnick, 2013, p. 165).
Before, I did not even ask myself these questions about motivational interventions. The person came to see me for a specific problem; I gave the theory, and that was it. (. . .) Recently, a patient said to me “I want to see my grandchildren grow up.” I see a different spark in my patients’ eyes as I evoke those motivations. (BNJ)
Learning to differentiate patient talk also prompted clinicians to skillfully guide motivational conversations in a stepwise manner.
I was already establishing S.M.A.R.T. goals with my patients before, but I was doing it too quickly, with people who were not ready to change. Therefore, I learned to listen carefully and assess the patients’ motivations to choose the appropriate timing to go forward with a plan. (BK)
Questioning was another suboptimal counseling skill observed at study onset as several clinicians mostly formulated closed questions. They learned to leave space for patients to express their thoughts and take their rightful place through open-ended and evocative questions.
Before, for the multimorbid patient, I used to tell myself, “I have my plan and we will cover hypertension first.” Now, I skip that part. Even if there is a lot to cover; my first questions are, “What brings you today? What is most important to you? What do you want to work today and what would you like to change?” (DN)
Most clinicians did not use strategies to consolidate the patients’ self-confidence to succeed in health behavior change. Formulating affirmations proved beneficial; once familiarized, clinicians even learned to help patients overcome adversity and discouragement.
It is surprising that we can find positive twists in challenging situations. I am more comfortable with the patients’ discomfort, their dissatisfaction related to pushing it a little further, and allow them to leave the consultation in a way that they feel more valued and confident. (DN)
Clinicians previously perceived the professional obligation to provide as much health information/advice as possible, but they realized that over-delivery often had the opposite effect. Through MI, they grasped the importance of exchanging solicited and tailored health education.
I know all what the patients would have to know and do, but the matter is to put that aside and ask them what they want to know, and to filter this information instead of dumping everything on them. Now, I do my duty, even much better, without having to say everything! (DN)
Influencing Factors: Building on Personal Strengths and Overcoming Power Structures
Having personal values correspondent with the MI spirit and demonstrating natural ease with MI skills were important facilitators of MI learning. However, some clinicians who presented these personal traits had to vigilantly avoid traps of identification/sympathy.
I am a person who is easily empathetic. I have a positive energy. I figured that I could focus on these strengths. (. . .) but I need to be aware of the distance I establish with my patients since I share similar past experiences with some of them. MI brings me closer to patients, so I need to be careful. (BNJ)
Clinicians’ professional backgrounds were also influential. Psychologists were perceived as more prepared to learn MI, as “It’s in their intervention time, their training, and their role.” The other clinicians experienced MI learning differently, as it was something completely novel.
We were all in the early stages of the approach. It was new, totally new! Of course, there were bits of MI that were already in our daily practice, without naming them. (. . .) But I was clumsy with MI at first! (BK)
Another aspect refers to past clinical experiences in acute care settings, where directive interventions are legitimately delivered in critical situations. This professional background consolidated the expert model of care for some participants.
I was an emergency nurse, [and] where [I worked] it was action/reaction. [When] Listening to patients talk, sometimes I would like to say “Look, this is the goal. What should we do from here to get there? Okay let’s go!” I realized that it does not work like that in primary care. (CIM)
Moreover, the participating clinicians shared a professional culture that had a strong, yet insidious, impact on MI learning processes. This culture was described as widespread within various agencies and as explanatory for most of their learning challenges.
There is an urgent need for professionals to educate and give something. It goes back, it’s deep and almost visceral as we feel like we are doing our job when we give information and advice. It will definitely be a challenge for me to refrain from this impulse. (DN)
In PC, the frequent use of health care protocols and standardized tools was reported to encourage clinician-centered approaches. Through MI, clinicians feared that they would no longer meet professional/workplace requirements.
I have a computer template for hypertension, diabetes, cholesterol, etc. Before this training, I said to myself, “Before the patient leaves, I have to fill it all out! Otherwise, I would not have been a good nurse.” (. . .) If, for example, we sit down and I ask the patient what happened in the past few weeks, and then he started crying, before I would say to myself “I’m stuck! I will not be able to do my job!” (DI)
Most certified professional associations were also reported to disseminate standardized practices that failed to address patient-centered care. Participants felt puzzled upon facing the contradictions between these credible associations and MI.
I attended a Diabète Québec seminar. They said, “First meeting, you do this. At the second meeting, you are supposed to be there. The third meeting, blablabla.” You cannot integrate MI there! (. . .) But I realized that these imposed frameworks do not work for most patients. If I do not do MI, I will check all the boxes, but I will have to cover the same things all over again, because the patient was set aside. (CIL)
Developing counseling knowledge and skills related to MI was said to be a topic that is underdeveloped in undergraduate education, a reality that contributed to the culture of the expert model of care.
What I learned at the university; we were taught, “You meet patients, you give them an exercising program, you give it and you do that.” MI is not that at all! So it is a very different way of doing things! (AK)
Finally, the influence of professional orders may also have contributed to this culture.
I would fail my professional inspection if I were to provide MI and adapt my interventions to the patients’ preferences, without relying on the priorities underlined by my nutritional analysis. (. . .)I felt very incompetent in my job for a while because I did not work as recommended by our professional order. (BNM)
Discussion
Discussion of Research Findings
The study described four simultaneous processes of MI spirit embodiment, being the transition from education to evocation, confrontation to acceptance, imposition to collaboration, and protection to compassion. These processes illustrate the power structures that the clinicians unintentionally cultivated with their patients. Through ICP-MI, they mindfully realized and addressed this situation engaging in a paradigmatic change to progress from health experts to health guides. In the literature, overcoming the impulse to educate patients through knowledge transfer has been documented as a recurrent MI learning challenge for PC clinicians (Söderlund et al., 2011). Typical approaches to health education in PC are also documented as being predominantly authoritarian, characterized by the confronting of patients reluctant to adhere to health care advice which creates tensions among clinicians and patients (Graves et al., 2016; Sargeant et al., 2008).
To translate the MI spirit into practice, building MI skills is ineluctable. The research findings described the previous limited counseling practices of the clinicians. To our knowledge, no prior study has qualitatively detailed MI learning processes to build PC clinicians’ counseling skills, although underlying challenges have been reported in the literature. A strong discomfort and sense of incompetence among PC clinicians who were building their MI skills are reported, and PC nurses would be particularly challenged in that regard (Brobeck et al., 2011; Midboe et al., 2011; Östlund et al., 2015; Sargeant et al., 2008). This study, thus, supports the assumption that most PC clinicians present suboptimal counseling skills as they often deliver prescriptive health education fostering power imbalances and complexifying MI learning processes. This phenomenon underlines the need to provide/study extensive training program on MI for PC clinicians.
Regarding the influencing factors of MI learning processes, we drew similar conclusions to those found in the scarce literature on the topic; especially regarding the limited training of PC clinicians in counseling, except for psychologists (Brobeck et al., 2011; Graves et al., 2016; Midboe et al., 2011; Östlund et al., 2015). The other factors are original findings and could have in common the dissemination of a clinician-centered approach in PC, which could owe to the protocolization of clinical practices encouraging standardized rather than personalized interventions in health education (Poitras et al., 2018) and in PC globally (Couturier et al., 2009). This finding illustrates the persisting power imbalances in our health care systems. We did not encounter any publication addressing the role of influential instances on MI learning processes such as professional orders and universities, although this research path appears central to demystify the tensions experienced by the participating clinicians while learning MI. It highlights the importance of fostering the dissemination/investigation of patient-centered care from political/decisional to clinical/practical spheres in PC.
Theoritical Reflection
The model of eight stages for learning MI, elaborated by Miller and Moyers (2006), was contrasted to the current research findings. According to this model, learning MI evolves from (1) the valuing of the MI spirit; (2) the use of patient-centered skills; (3) the recognition of change talk and resistance; (4) the evoking/reinforcing of change talk; (5) the rolling with resistance; (6) the developing of a change plan; (7) the consolidating of patient commitment to change; and (8) the flexible switching between MI and other interventions. The study adds an empirical and dynamic viewpoint that serves to conceptualize MI learning as processes, rather than stages. We came to the same conclusion that presenting an openness to the MI spirit is a starting point; however, the seven other steps of this model focused on the building of MI skills. Our findings, instead, present the learning of the MI spirit and skills as iterative and continuous processes. A paradigmatic shift underlying the MI spirit embodiment was detailed previously. Regarding the MI skills, the clinician’s ability to apply patient-centered skills (stage 2), to recognize/reinforce change talk (stages 3, 4, and 7), and to roll with resistance (stage 5), were gathered into one category of findings related to patient talk. As for the developing of a change plan (stage 6), it was not a critical learning moment observed during the study. Instead, clinicians rather learned to wait for the right timing to elaborate action plans while listening to patient talk. Finally, blending MI with other interventions (stage 8) is presented in Miller and Moyers’s model as the last stage of MI learning. In this study, we had its onset at the beginning of the training and distinguished MI implementation from MI learning, as presented in another publication (Langlois & Goudreau, 2022b).
Study Limitations
Clinicians’ involvement in the identification of the studied phenomenon and in data collection was extensive. Although, they partially collaborated with data analysis and the dissemination of research findings. Considering that these methodological choices were openly discussed among the co-participants, they are not the result of power imbalances, which PAR approach aims to overcome (Kemmis et al., 2014). We also acknowledge that participants presented great interest in learning MI as they voluntarily engaged in ICP-MI after attending introductory training, which creates a selection bias. Hence, results may not be largely transferable to any PC setting and may have influenced the conduct of the study in creating a ripple effect enabling MI learning.
Conclusion
In PAR, the aim is to stimulate historical consciousness and collective actions to resolve unsatisfying professional practices through a cyclical and empowering process (Kemmis et al., 2014). This study detailed the professional transformation that PC clinicians undertook through MI learning processes facilitated in ICP-MI, which were conceptualized as a paradigmatic shift from health experts to health guides. Influencing factors were presented including a shared professional culture of clinician-centered care that diverges from the MI principles while prevailing power structures in our health care systems. Clinicians, trainers, and decision makers can reflect on these findings to improve patient-centered counseling practices in PC; researchers are also call forth to investigate MI learning to guide the diffusion of this clinical innovation.
Footnotes
Acknowledgements
The authors acknowledge the contribution of all the PC clinicians who took part in this study. They also thank Lyne Lalonde and all the members of research team “Équipe de recherche en soins de première ligne de Laval” who collaborated in this PAR.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Recreation and Sports (Québec, Canada)—LP 250 048 633 CA, the Fondation de l’Ordre des infirmières et infirmiers du Québec, the Fonds Pfizer-FRQS-MSSS sur les maladies chroniques (Fonds de Recherche du Québec en Santé, Ministry of Health and Social Services of Quebec, Canada), the CIHR—TUTOR-PHC fellowship program, the Université de Montréal, and the Fondation Cité de la Santé de Laval.