
Abstract
Key Points
Both static and dynamic stretching improve spinal flexibility in Belly Dance.
Dynamic stretching shows greater improvement in low back pain.
Combining static and dynamic stretches optimise spinal flexibility in Belly Dance.
Background
Low back pain (LBP) is among the most prevalent musculoskeletal disorders affecting athletes and physically active populations globally. 1 The prevalence and incidence of LBP vary substantially depending on sport-specific biomechanical demands, training intensity, and participant characteristics.2-4 Trompeter et al 4 conducted a comprehensive systematic review demonstrating that sports involving repetitive spinal loading, torsional forces, and impact show higher prevalence rates of back pain, which can lead to decreased performance, prolonged recovery, and early retirement from sport. Similarly, Maselli et al 5 reported that runners frequently suffer from LBP, often attributable to biomechanical overload and inadequate conditioning, highlighting the need for targeted preventative strategies in these populations. Spinal flexibility and mobility are critical components in optimising athletic performance and reducing the risk of injury, particularly LBP. 6 Reduced flexibility and impaired neuromuscular control have been consistently identified as significant contributors to the development and persistence of LBP in both athletic and general populations.7,8 Stretching interventions, including static stretching (SS) and dynamic stretching (DS), are widely implemented to improve flexibility and prepare athletes for activity.9-11 SS is characterised by sustained elongation of muscle tissue, which promotes increased muscle length and joint range of motion (ROM). 10 Conversely, DS involves movement-based stretches designed to mimic sport-specific motions, potentially enhancing neuromuscular readiness and functional flexibility.10,11 While both methods have shown efficacy in improving ROM, their comparative effects on spinal flexibility remain underexplored. 12
Belly Dance, also referred to as Oriental Dance, is a movement practice that uniquely demands high levels of spinal articulation and control through isolated torso movements that involve flexion, extension, rotation, and lateral flexion of the spine.13,14 This dance form has experienced significant growth globally and within South Africa, attracting a diverse population of participants. 15 The biomechanical requirements of Belly Dance necessitate adequate spinal mobility and core strength to facilitate safe and effective performance while minimising injury risk, particularly LBP. 16 Inadequate flexibility or conditioning may predispose dancers to musculoskeletal strain or chronic pain, negatively impacting their practice and quality of life. 17 Pelvic and abdominal movements serve as the biomechanical linkage between the spine and hips, playing a vital role in maintaining posture, balance, and voluntary motor control essential for Belly Dance technique.18-20 Joint mobility and muscle flexibility within these regions contribute directly to movement precision, performance quality, and injury prevention. 21 Flexibility is defined as the ability to move joints safely through their maximal ROM, a fundamental attribute influencing dancers’ technical proficiency and physical resilience. 22
Despite the acknowledged importance of flexibility training, limited research has investigated the effectiveness of SS and DS in improving spinal flexibility specifically among Belly Dancers. 19 This gap in the literature restricts the ability of dance educators and allied health professionals, such as physiotherapists and biokineticists, to design and implement evidence-based conditioning and rehabilitation programmes tailored to this population’s unique needs.20,23 Therefore, the present study aims to evaluate and compare the effects of static and dynamic stretching interventions on spinal flexibility in Belly Dancers. The findings are expected to inform targeted strategies for enhancing spinal health, reducing LBP risk, and optimising dance performance, thereby contributing valuable evidence to the fields of dance medicine and sports rehabilitation.
Hypotheses
Dynamic stretching (DS) will result in greater improvements in spinal flexibility compared to SS.
Static stretching (SS) and DS will reduce low back pain, with DS being more effective.
Methods
Research Design
A prospective, single-blind, multicentre, randomised controlled trial evaluated the effects of SS and DS interventions on spinal flexibility and low back pain in Belly Dancers. From January 2022 to April 2022, 75 participants were recruited from local dance communities in Gauteng Province, South Africa. Eligible participants were randomised into one of three groups: a static stretch group (SSG), a dynamic stretch group (DSG), or a control group (CG). The SSG and DSG group participants received supervised stretching interventions, while the CG continued their usual activities without additional structured stretching. The stretch routines prescribed to each of the two groups were carried out at selected dance schools, homes, gymnasiums, or any location the dancer preferred to use to complete their prescribed stretches. The pre-intervention workshop provided hands-on training and detailed guidance on stretching techniques, accompanied by written instructions and visual aids, which were distributed to each participant as a take-home resource. Pre-intervention workshops were completed under the guidance of trained biokineticist and certified Belly Dance instructors. Adherence was monitored through weekly check-ins, and participants were instructed in proper techniques during a pre-intervention workshop. Data were collected at baseline (January 2022) and after a 12-week intervention period (April 2022). The study design and protocol were approved by the University of Johannesburg’s Faculty of Health Sciences Research Ethics Committee, and written informed consent was obtained from all participants prior to enrolment. Biokinetics, as an emerging allied health profession in South Africa, is still expanding its scope of practice and research domains. This study represents a pioneering effort to integrate biokinetic principles into the culturally and physically unique context of Belly Dance. Given the novel exploratory nature of this pilot intervention and the absence at that time of established institutional requirements for clinical trial registration within this field, the trial protocol was not prospectively registered on a formal clinical trial registry. We recognise that prospective registration is a hallmark of methodological rigor and transparency in randomised controlled trials and are committed to adhering to this standard in all future studies. This study adheres to the CONSORT 2010 guidelines, with detailed reporting of randomisation procedures, participant flow, and outcomes.
Participants
The study used purposive and snowball sampling methods to recruit participants. Belly Dance instructors and students in Gauteng Province, South Africa, were contacted via email and asked to share the study’s online sign-up form within their communities. A total of 76 Belly Dancers (n = 76) participated, with an even distribution across the three groups. In Gauteng Province, there are approximately 150 registered Belly Dancers. Given this limited population, a recruitment target of 75 represented 50% of the potential population, ensuring a substantial and representative sample size while maintaining the feasibility of study execution. The final number of enrolled participants (76) slightly exceeded the target due to the inclusion of an additional eligible participant, further enhancing the robustness of the analysis.
Differential Diagnosis and Screening
To ensure participant safety and study validity, all potential participants underwent a clinical screening process to exclude serious pathology or conditions that could confound the study outcomes. Screening for red flags associated with LBP was conducted based on established physical examination protocols, 24 including assessment for unexplained weight loss, history of malignancy, recent severe trauma, neurological deficits, or signs of infection. Additionally, the clinical utility of commonly used screening questions was considered, acknowledging that “red flags” are not always definitive indicators of serious pathology. 25 Any participant presenting symptoms or signs suggestive of serious pathology was referred for further medical evaluation and excluded from the study. This rigorous screening process ensured the safety of participants and maintained the scientific integrity of the trial.
Recruitment and Randomisation
Participants were recruited through two primary methods. First, an email invitation was sent to a targeted network of Belly Dance instructors and community groups in Gauteng Province, South Africa. Second, an open call for participation was posted on social media platforms popular within the Belly Dance community. Recruitment occurred between October 2021 and December 2021, with a focus on engaging a diverse group of Belly Dancers actively involved in the community. 26
Participants were eligible if they (1) were aged 18 years or older, (2) had at least 1 year of continuous Belly Dance experience, and (3) cleared the Physical Activity Readiness Questionnaire (PAR-Q+) without contraindications to physical activity. Participants were excluded if they reported a history of recent musculoskeletal injuries, ongoing physical therapy, or conditions that could interfere with participation in stretching exercises. Eligible participants were assigned to one of three groups (SSG, DSG, or CG) using a process known as randomisation. This method involved creating a computer-generated sequence table to ensure a random and unbiased allocation of participants. Each participant was individually randomised into one of the three groups, maintaining a 1:1:1 allocation ratio to ensure an equal number of participants in each group. To prevent any potential bias and maintain allocation concealment, the group assignments were placed in sealed, opaque envelopes. These envelopes were prepared in advance by an independent researcher who was not involved in the recruitment or data collection process. The envelopes were only opened after the participant provided informed consent, ensuring that neither the participants nor the study team could influence group allocation before consent was obtained.
The study initially aimed to recruit 75 participants based on the sample size calculation, which was designed to detect a minimum effect size with 80% power and a significance level of 0.05. However, during the recruitment process, one additional participant who met the eligibility criteria expressed interest in joining the study. Given the alignment of this participant’s characteristics with the study requirements and the potential benefits of increasing statistical power, the research team included this individual, resulting in a final sample size of 76 participants. Participants were informed of their group assignment upon allocation. Given the hands-on nature of the intervention, it was not feasible to blind participants or facilitators to group assignments. Participants needed to be aware of their assigned stretching routine (static or dynamic) to perform the exercises correctly, while facilitators required knowledge of group allocation to provide appropriate guidance during the sessions. To reduce the risk of bias in outcome assessments, the data collectors were blinded to group assignments. This ensured that individuals measuring spinal flexibility and low back pain were unaware of the participants’ group allocation, maintaining objectivity and reducing potential measurement bias. Furthermore, the main investigator remained blinded to group assignments throughout the data collection and statistical analysis phases. Group allocation was disclosed only after all statistical analyses were completed, further minimising the risk of bias in the interpretation of results.
Intervention
The intervention for the SSG and DSG groups involved structured stretching routines, designed to improve spinal flexibility and reduce low back pain. Each group followed their respective stretching routine three times per week for a 12-week period. The SSG focused on SS, where each stretch was held for 30 seconds to target muscle elongation, while the DSG incorporated DS, involving controlled, repetitive movements that mimicked Belly Dance movements.
Participants were allowed to complete the 12-week programme at their selected dance schools, homes, gymnasiums, or any location the dancer preferred to use to complete their prescribed stretches. Although the pre-intervention workshop was supervised by a trained biokineticist and certified Belly Dance instructors, the majority of participants opted to complete the 12-week programme at their chosen dance schools, continuing under the guidance of the same instructors. Adherence to the intervention was monitored via weekly check-ins and attendance logs, and participants were encouraged to complete their sessions consistently. The Control Group (CG) did not participate in any specific intervention and continued their usual activities without a structured stretching programme. Upon study completion, participants in the control group were offered access to the stretching protocols as part of the study’s ethical commitment to equitable benefit.
Outcomes were measured at baseline and after the 12-week intervention period at local dance studios in Gauteng Province, South Africa. These settings were chosen for their relevance to the study population, as they are commonly used for Belly Dance practice. Baseline measurements were conducted by a qualified biokineticist, whose training covers the specific testing procedures used in this study. The primary outcomes included spinal flexibility (assessed through the Modified Schober’s Test, 13 Fingertip to Floor Test, 14 and Spinal Rotation Test 15 ) and low back pain (measured using the Oswestry Low Back Pain Index). Modified Schober’s Test measures lumbar spine flexibility by marking a point 10 cm below and 5 cm above the lumbar spine’s L5 vertebra. The participant is instructed to bend forward as far as possible while keeping their legs straight, and the distance between the two marks is measured to assess the extent of flexion. The Modified Schober Test demonstrated moderate validity (r = .59) with excellent interclass (r = .92) and intraclass (r = .96) reliability. 17 Its validity has been established in various populations, including those with low back pain and healthy adults. 13 Fingertip to Floor Test measures forward spinal flexion by recording the distance between the participant’s fingertips and the floor while standing. The participant is instructed to bend forward and reach as far down as possible while keeping their knees straight. The measurement is taken from the fingertips to the floor. This test has demonstrated good test-retest reliability (r = .8) and is considered a valid measure of spinal flexibility in clinical and research settings. 14 The Spinal Rotation Test assessed thoracic spine mobility by instructing participants to rotate their upper torso. The angle of rotation was measured using a goniometer, and the reading was cross-checked with the iPhone Compass app to ensure accurate measurements. The app provided a digital reading of the rotational angle, which was cross-checked with the goniometer to ensure consistency and accuracy. Both tools were used together to provide a reliable measurement of thoracic spine rotation. Furness et al 17 found that the Apple iPhone Compass app exhibited excellent reproducibility for intra-rater (0.96-0.98) and inter-rater reliability (0.87-0.89), and strong concurrent validity (r = .835, P < .001) compared to the Universal Goniometer when measuring thoracic spine rotation.
The Oswestry Low Back Pain Index (OLBI) was used to measure the level of disability caused by low back pain in daily activities. The OLBI is a self-reported questionnaire consisting of 10 items, each related to a different aspect of daily functioning (eg, pain intensity, personal care, lifting, walking). Participants are asked to rate their level of discomfort or difficulty with each activity on a scale from 0 (no difficulty) to 5 (severe difficulty). The total score is then calculated, with a higher score indicating greater disability due to low back pain. The OLBI has been extensively used in research and clinical practice and has demonstrated high reliability (test-retest reliability >0.90) and validity in various populations, including individuals with chronic low back pain. It has been validated against clinical assessments of function and has been shown to correlate well with other measures of pain and disability. The OLBI is sensitive to changes in low back pain and has been used in multiple studies to assess the effectiveness of interventions aimed at improving back health. It has been shown to detect changes in disability over time following treatment interventions, including physical therapy and stretching exercises. Secondary outcomes included participant-reported improvements in flexibility and pain, as well as adherence to the prescribed stretching routines.
Data Analysis
All pre- and post-intervention data from the 12-week intervention were coded and summarised in an Excel spreadsheet. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 25.0, incorporating both inferential and descriptive statistics. In addition to P-values, effect sizes (Cohen’s d) and 95% confidence intervals (CIs) were calculated to assess the magnitude and precision of the differences between the intervention groups. The chi-square test examined the association between back pain and spinal flexibility, and the normality of continuous variables was assessed using the Shapiro-Wilk test. The non-parametric Kruskal-Wallis H test was used to compare the three intervention groups: the DSG, the SSG, and the CG. The Mann-Whitney U test was applied to compare differences within each intervention group, with the Bonferroni Correction used to adjust for multiple comparisons and mitigate Type 1 errors. P-values were tested against a significance level of .05/3 = .0167, due to the division of the original alpha-value by the number of analyses (the three intervention groups) on the dependent variable.
Results
Participants
In total, 76 potential participants were screened for eligibility (Figure 1). Of these, 76 met the inclusion criteria, which required participants to be at least 18 years old, actively engaged in Belly Dance for at least 1 year, and free of contraindications as assessed by the PAR-Q+ form. The 76 eligible participants were randomly assigned to one of three groups using a computer-generated randomisation sequence: the SSG (n = 25), the DSG (n = 26), and the CG (n = 25). Each participant was provided with instructions specific to their allocated group. The SSG and DSG participated in programme three times per week, while the CG continued their regular activities without a structured intervention. Throughout the 12-week intervention period, no participants withdrew from the study. Data from all 76 participants (SSG: n = 25, DSG: n = 26, CG: n = 25) were included in the final analysis, which was conducted following the intention-to-treat principle.

Flow chart.
The sample characteristics are depicted in Table 1. The mean age of the total sample (n = 76) was 34.24 (± 12.760). The SSG had the highest mean age of 37.64 years (± 14.4), followed by the DSG at 34.50 years (± 12.7), and the CG at 30.56 years (± 10.34). The age distribution was normal in both the SSG (P = .136) and DSG (P = .057), but not in the CG (P = .000). There were no significant differences in age between the three groups (P = .277).
Sample Characteristics.
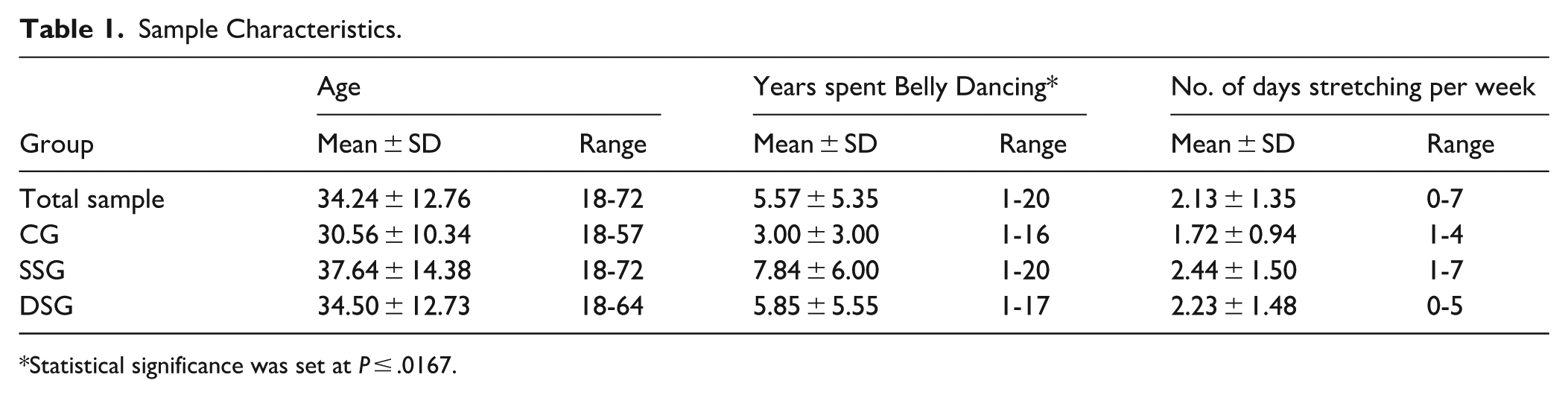
Statistical significance was set at P ≤ .0167.
Table 2 presents the pre- and post-intervention results of spinal flexibility measures among participants. For spinal flexion, significant improvements were observed in the DSG, with a mean difference of 0.54 (95% CI: 0.22; 0.86) and a moderate effect size of d = 0.54 (P = .001). This indicates a substantial increase in spinal flexion following dynamic stretching. In contrast, the SSG showed a non-significant improvement with a small effect size (d = 0.26), and the CG showed no significant changes, with a mean difference of −0.08 (95% CI: −0.29; 0.13) and a negligible effect size of d = −0.08.
Spinal Flexibility Measures.

Statistical significance was set at P ≤ .0167.
In spinal rotation to the left, both the SSG (P = .000, d = 0.85) and the DSG (P = .003, d = 0.25) showed significant improvements. The static stretching intervention had a large effect size (d = 0.85) with a mean difference of 9.24° (95% CI: 5.10; 13.38), while dynamic stretching showed a smaller effect (d = 0.25) with a mean difference of 4.08° (95% CI: 1.26; 6.90). The CG showed no significant change, with a mean difference of −0.48° (95% CI: −2.56; 1.60) and a negligible effect size (d = −0.03). For spinal rotation to the right, significant improvements were found in both the SSG (P = .001, d = 0.66) and the DSG (P = .000, d = 0.09), though the effect size for dynamic stretching was small. The static stretching group showed a mean difference of 7.00° (95% CI: 3.81; 10.19), indicating a moderate improvement. The CG showed no significant change, with a negligible effect size (d = 0.02).
In lateral flexion to the left, both the SSG (P = .003, d = −0.30) and the DSG (P = .001, d = −0.40) showed significant reductions in lateral flexion. The dynamic stretching group had a larger mean difference of −2.96° (95% CI: −4.07; −1.85), reflecting a more substantial change compared to static stretching, which showed a mean difference of −1.96° (95% CI: −3.01; −0.91). The CG showed no significant change, with a negligible mean difference of −0.04° (95% CI: −1.02; 0.94) and an effect size of d = −0.01. For lateral flexion to the right, significant improvements were observed in both groups, with the DSG showing the most notable reduction (P = .000, d = −0.76) and a mean difference of −5.42° (95% CI: −6.55; −4.29). The SSG also showed a significant reduction (P = .002, d = −0.43) with a mean difference of −2.72° (95% CI: −3.75; −1.69). The CG showed no significant changes, with a small effect size of d = 0.09 and a mean difference of 0.60° (95% CI: −0.29; 1.49).
The results of the movement comparison post-test revealed several significant differences between the groups (Table 3). In spinal flexion, there were significant differences between SSG and DSG (Mean Difference = −0.87, 95% CI: −1.20; −0.54, P < .001), SSG and CG (Mean Difference = 0.52, 95% CI: 0.31; 0.73, P = .002), and DSG and CG (Mean Difference = 1.39, 95% CI: 1.08; 1.70, P < .001), with effect sizes indicating large effects in all comparisons. For spinal rotation to the left, the comparison between SSG and DSG approached statistical significance (Mean Difference = 5.35, 95% CI: −0.08; 10.78, P = .054), while the DSG versus CG showed a significant difference (Mean Difference = −7.48, 95% CI: −12.69; −2.28, P = .005). Spinal rotation to the right showed significant differences between SSG and DSG (Mean Difference = 7.06, 95% CI: 1.28; 12.83, P = .019), but no significant differences were found between SSG and CG or DSG and CG. For lateral flexion to the left, SSG versus CG showed a significant difference (Mean Difference = 2.92, 95% CI: 0.77; 5.08, P = .008), while the other comparisons were not significant. In lateral flexion to the right, no significant differences were found across any of the groups. These findings suggest that the dynamic stretching had the most substantial effects on spinal flexion and rotation, while the static stretching showed notable improvement in lateral flexion to the left.
Between Group Comparisons.
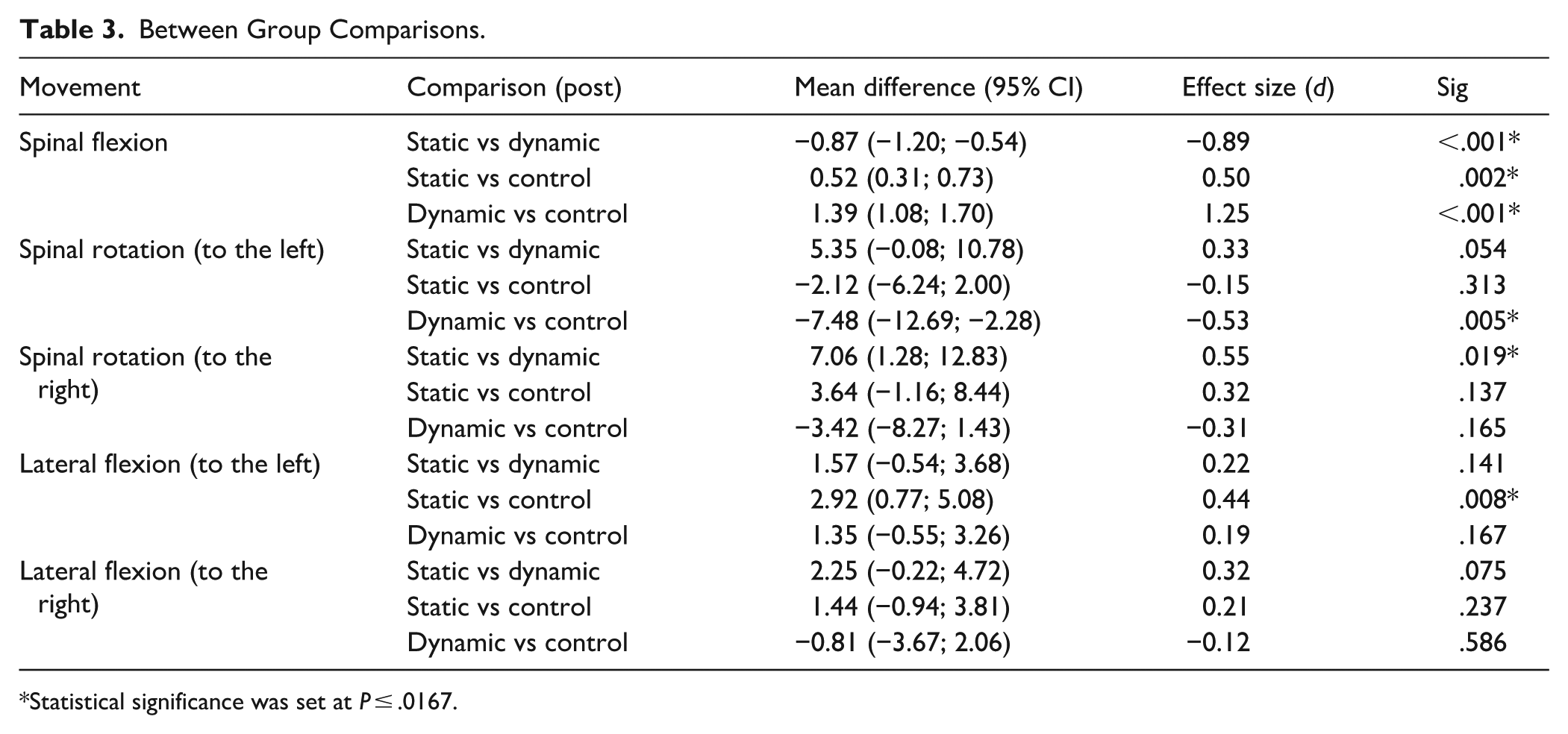
Statistical significance was set at P ≤ .0167.
Table 4 presents the results of the Wilcoxon Signed Rand test comparing pre-and post-intervention scores for the Oswestry Low Back Pain Index questionnaire across the difference groups. Pre-intervention, the mean score for the SG was 1.76 ± 2.79 (range 0-10), which decreased post-intervention to 0.64 ± 2.61 (range: 0-10) (P = .583). In the DSG, the mean score decreased from 4.0 ± 3.95 (range: 0-13) pre-intervention to 2.31 ± 0.90 (range: 0-9) post-intervention, with this improvement being statistically significant (P = .001). Conversely, the CG exhibited a pre-intervention mean score of 3.60 ± 2.93 (range: 0-12), which slightly increased post-intervention to 3.88 ± 3.11 (range: 0-11) (P = .800). It is important to note that these comparisons were compared to baseline measures within each group.
Low Back Pain Questionnaire.

Statistical significance was set at P < .0167.
Discussion
Participants in this study, drawn from Gauteng Province, South Africa, had a mean age of 34 years (± 12.76), with a range spanning 18 to 72 years. This demographic distribution aligns with prior international studies, such as those by Tiggemann et al 20 in Australia and Milner et al 21 in New Zealand, which similarly noted the cross-generational appeal of Belly Dance. As Moe 23 observes, older dancers in particular may experience enhanced mobility, psychosocial empowerment, and creative expression through participation in Belly Dance. The representation of varied age groups in the present study underscores the relevance of age-adapted movement interventions in clinical and rehabilitative contexts.
Low back pain (LBP) remains a significant musculoskeletal burden among dancers and athletes more broadly, with incidence rates documented in multiple systematic reviews.4,5 Given the biomechanical demands of Belly Dance, especially repetitive torso and pelvic articulations, optimal spinal flexibility is essential for injury prevention and performance maintenance. 21 Within this framework, the present study investigated the differential impacts of SS and DS stretching on spinal mobility and LBP severity. The findings demonstrated that DS was most effective in enhancing spinal flexion and lateral flexion, while SS yielded greater improvements in spinal rotation. These results are consistent with the literature: SS has been shown to enhance joint range of motion through prolonged muscle elongation,27-32 while DS promotes functional mobility and neuromuscular readiness through task-specific movement patterns.12,29 The clinical implication is clear, interventions should be selected based on the desired spinal movement outcome, and training regimens should be tailored accordingly.
Pain outcomes, as measured by the Oswestry Low Back Pain Index, indicated a 17% mean reduction across all groups, with the DS group showing a substantial 53.57% improvement, compared to 2.3% in the SS group. These data support previous research on the role of movement-based interventions in modulating pain and enhancing function in individuals with chronic LBP.33-37 Notably, França et al 35 and Chen et al 36 demonstrated significant functional improvements following stretching interventions in similarly affected populations.
From a clinical management perspective, these findings advocate for the incorporation of both stretching modalities into dancer-specific training and rehabilitation protocols. Physiotherapists and biokineticists, in particular, should consider the functional specificity of each stretching technique when designing programmes. Moreover, the use of DS prior to dance activity may confer both preventive and therapeutic benefits, particularly in individuals with existing or recurrent low back discomfort.
Finally, it is important to note that commonly used red-flag screening questions for LBP may have limited utility in physically active populations. As highlighted by Andreoletti et al 24 and Premkumar et al 25 such screening tools often yield false positives or overlook benign musculoskeletal conditions. These limitations underscore the importance of differential diagnostic reasoning and functional assessment in guiding referrals and interventions within this cohort.
Strengths and Limitations
This study provides valuable insights into the effectiveness of both static and dynamic stretching in enhancing spinal flexibility and alleviating low back pain among Belly Dancers. The use of multiple outcome measures, including spinal flexibility tests and the Oswestry Low Back Pain Index, allowed for a comprehensive assessment of the intervention’s impact. Additionally, the inclusion of both a control group and two experimental groups strengthens the study design, providing a solid basis for comparison. However, several limitations must be acknowledged. First, the inclusion criteria, which required participants to have at least 1 year of continuous Belly Dance experience, restricted the eligible participant pool and may limit the generalisability of the results to novice dancers or broader physically active populations. Additionally, the use of convenience sampling within Gauteng Province may have introduced geographic and cultural bias, reducing external validity. The unsupervised nature of the home-based stretching routines presents another limitation, as variability in adherence and execution could have influenced intervention fidelity and outcomes. The Oswestry Low Back Pain Index, while widely used, is a self-reported measure and may be subject to recall bias and subjective interpretation. Moreover, while the study involved participants across a wide age range (18-72 years), subgroup analyses by age were not feasible due to sample size constraints. Future research with larger and more diverse samples could explore age-related differences in responsiveness to stretching interventions. Finally, although this study followed rigorous methodological principles, it did not undergo prospective trial registration, which is typically recommended for randomised controlled trials. At the time of study initiation, the research team was unaware of formal registration requirements. We acknowledge this as a limitation and recognise the importance of prospective registration for promoting transparency, replicability, and adherence to best research practices.
Clinical Implications and Future Directions
Expanding the sample size in future studies would improve statistical robustness, enabling more generalisable results. Research should also incorporate a wider variety of stretching routines targeting muscles crucial for lower back health and explore personalised programs to optimise spinal flexibility and minimise injury risks. Future work should investigate the long-term benefits of combined stretch routines, as well as the optimal frequency, duration, and sequencing of stretches in dance-specific contexts. Additionally, examining the psychological benefits of improved flexibility, such as enhanced self-esteem and artistic expression, could provide valuable insights into the holistic impact of stretching interventions on dance performance and well-being.
Conclusion
Low back pain is common among Belly Dancers, with Milner et al 21 identifying it as the most frequent injury in this population. Our study, using the Oswestry Low Back Pain questionnaire, shows that prescribed stretching routines effectively alleviate this condition. While spinal extension showed no significant improvement in flexibility, both the SSG and DSG demonstrated significant improvements in spinal flexion, rotation (left and right), and lateral flexion (left and right). The SSG showed greater improvement in spinal rotation, while the DSG exhibited higher gains in spinal flexion and lateral flexion. However, no single stretching modality was definitively superior, suggesting that a combined stretching regimen incorporating both static and dynamic stretches may offer the best results for improving spinal flexibility in Belly Dancers. These findings align with current dance research, which highlights the need for personalised, tailored interventions that address the unique demands of dancers. Integrating such interventions into dance training could improve performance, prevent injuries, and enhance dancer well-being.
Footnotes
Acknowledgements
The authors acknowledge Statkon at the University of Johannesburg for their contribution to data analysis.
Ethical Considerations
This study received ethical clearance from the Research Ethics Committee of the Faculty of Health Sciences at the University of Johannesburg (REC-1278-2021), prior to commencement.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
There is no identifying information related to the authors and/or their institutions, funders, approval committees, etc., that might compromise anonymity.