
Abstract
Key Points
The 11+ Dance can induce physiological adaptations when performed daily before the ballet class, therefore may be used to complement current practice.
Clinically significant improvements in jump height and peak force were observed in the 11+ Dance group with no adverse effects.
The 11+ Dance is based on current evidence, is easy-to-use and therefore, can be utilized by dance teachers, strength and conditioning coaches, athletic trainers, and other practitioners who work with young dancers.
Introduction
The effectiveness of lower extremity injury prevention programs in team-sport athletes has been supported by numerous systematic reviews (24 studies, n ≈ 250,000). 1 However, there is currently no established injury prevention program for pre-professional dancers. Several injury prevention studies in youth football have indicated that the use of neuromuscular interventions induce meaningful motor performance in strength, sprint and power. 2 Neuromuscular training programs have been shown to improve performance in sport 3 and reduce overuse injuries. 4 Kaufmann et al. 5 conducted a cross-sectional online survey to clarify the warm-up habits in ballet dancers. The authors suggest that neuromuscular-based warm-ups are associated with less overuse injuries when compared to more traditional ballet warm-ups. There was no association between the type of warm-up and acute injuries. These findings are based on a small sample without a priori power calculation and injury incidence was based on self-reporting retrospective data, a method that has been shown to inflate injury rates. 6
Generally, injury prevention interventions focus on mitigating risk factors. These factors can be classified as intrinsic, extrinsic, and modifiable, non-modifiable. 7 Injury prevention interventions target the intrinsic modifiable risk factor such as muscular power and strength. 8 It is, therefore, reasonable to evaluate the effect of a newly developed program (11+ Dance) on motor performance. The 11+ Dance is a 30-minute training program that focuses on muscular endurance in the trunk musculature and the lower body, balance and proprioception together with take-off and landing technique. 9
The aim of this study, therefore, was to assess the effect of the 11+ Dance program on the following physiological parameters, countermovement jump (CMJ), reactive strength index (RSI), isometric mid-thigh pull (IMTP) and inter-limb asymmetry (ASYM) compared with a control group that carried out their normal routine led by their dance teacher.
Methods
Ethical approval was attained from the University of Wolverhampton ethics committee (Approval no. 117474).
A balanced randomization (1:1), parallel-group, controlled study design was used to address the aim of this study. The study was conducted with pre-professional dancers in fulltime training at a vocational ballet school.
The primary outcome was the maximum height of the CMJ, and the secondary outcomes were the RSI, IMTP, and ASYM. Adherence was measured through the attendance records that were updated daily for both groups. Adherence for both groups was defined as the percentage of total participation sessions. Participants who reported an injury were assessed by the in-house physiotherapist. Any recorded injury during the trial would then be reported as an adverse event. 10
A feasibility randomized controlled trial (RCT) (n = 22 participants, age = 17 ± 52 years) was initially conducted in order to assess the intervention fidelity and adherence and also the baseline-post test protocols. 11 A pilot RCT was then conducted for power and sample size calculation. Forty-two adolescent ballet (mean age = 13 ± 58 years) dancers volunteered to participate in the pilot study. The power and sample size calculation revealed (power of 80%, alpha of 5%) for a small effect .03, 110 participants were required. A total of 73 elite adolescent ballet dancers volunteered to participate in the main trial.
Participants
The participants from the pilot trial took part in the main trial and subsequently some of the participants were exposed to the intervention twice due to the randomization process. There was a wash-out period of 8 weeks between the pilot and the main trial. Out of these 73 participants, 39 had participated in the pilot study. To ensure the reported results were not affected from a potential learning effect we have used the data from the pilot trial (n = 42) and the New Starters (n = 34: 73main − 39pilot = 34) of the main trial for the analyses. The research protocol for both the pilot and the main trial was the same, however, the length of the trials was different. The pilot trial lasted 7 weeks (7 weeks × 5 sessions per week = 35 training sessions), whereas the main trial lasted 9 weeks (9 weeks × 5 sessions per week = 45 training sessions) (Figure 1). Informed consent was attained by all those who participated in the trial.
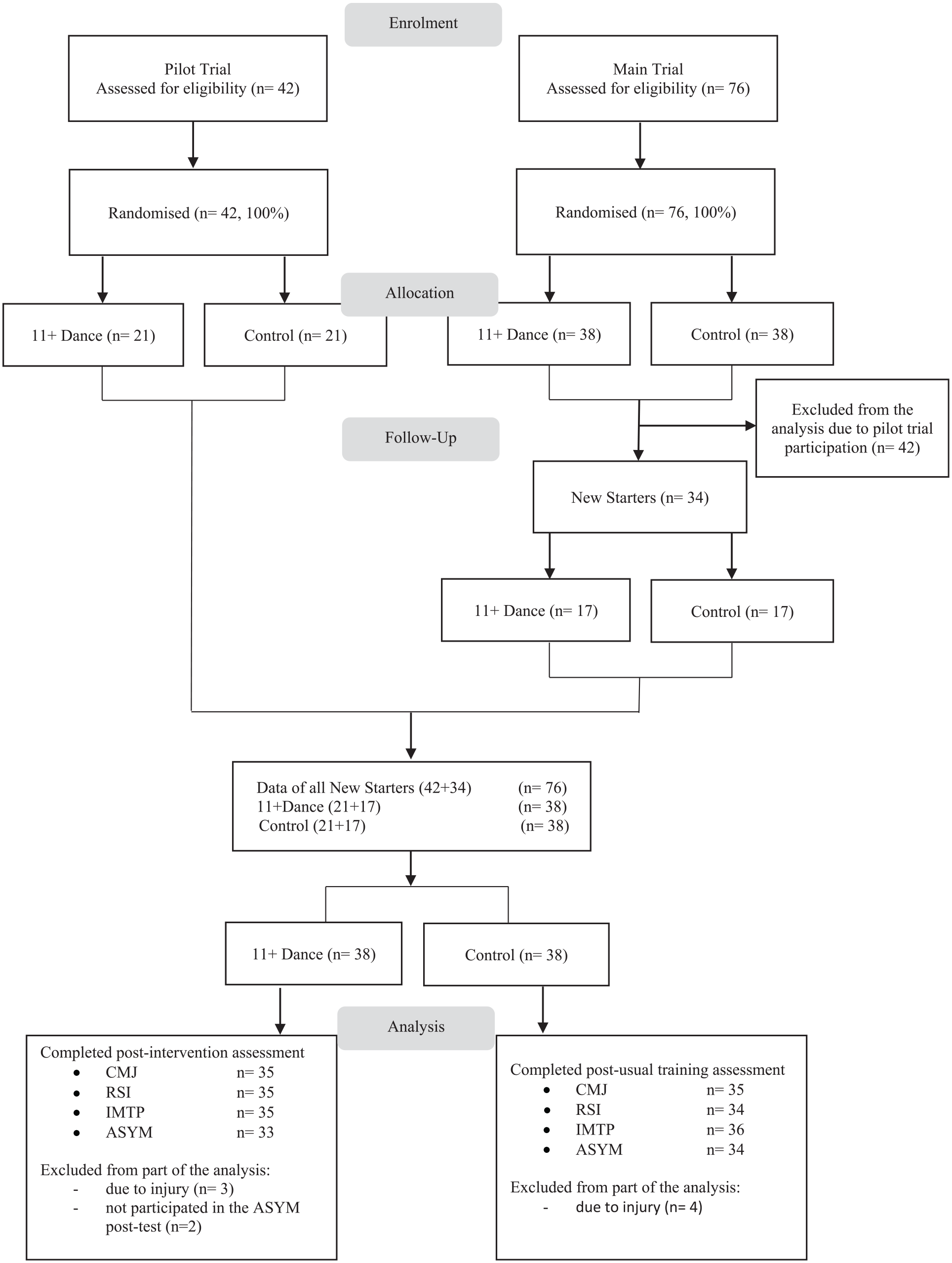
Pilot and main trial flow diagram.
Inclusion Criteria
All participants had to be injury free at baseline to be included in the study. Any participant who was unable to take part in the baseline testing and/or was diagnosed with an injury by the in-house physiotherapist was excluded from the analysis. The participants were all exposed to the same amount of dance hours per week (n = 19 h wk−1).
Procedure
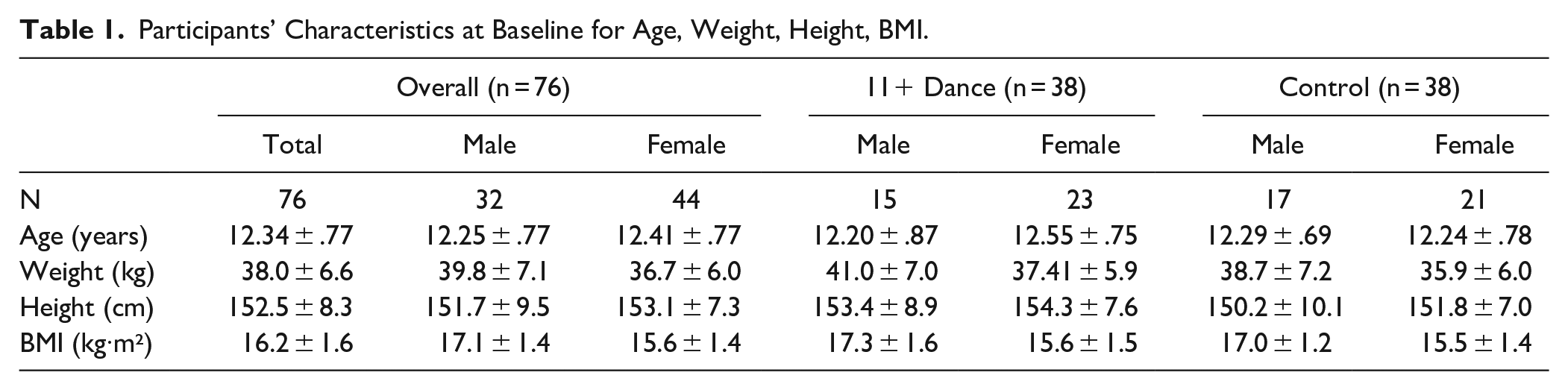
Anthropometric data, standing height (0.1 cm) and body mass (0.1 kg) were collected at baseline before breakfast and with minimum clothing (Table 1). The participants were randomly assigned to either the 11+ Dance or the Control group by an independent blinded researcher via a number-generator program after the baseline data collection. Baseline data were collected by the principal investigator whereas post-test data were collected by a blinded independent assessor. Testing for both groups commenced with a dynamic warm-up composed of 2 minutes of light cardiovascular exercise followed by dynamic stretches targeting the large muscles of the lower body. 11 All participants were familiar with the tests as they were routinely used as part of their fitness monitoring, typically 4 times per academic year.
Participants’ Characteristics at Baseline for Age, Weight, Height, BMI.
Equipment
Jump height for the CMJ and the reactive strength index (RSI) were measured with an Optojump Next system (Microgate, Bolzano, Italy, Version 1.10.19) and isometric lower body strength was measured through Powerlab (Ad Instruments, Dunedin, New Zealand).
Jumps
The participants performed 3 countermovement jumps (CMJ), and 3 drop jumps (DJ) from a 30 cm box in a non-fatigued state barefoot. For the DJ the instructions included; to initiate the move by stepping from the box and drop without pushing with the standing leg, while keeping their hands on the hips during the jump, touch the ground with both feet at the same time, and then immediately jump as high as possible. The verbal cues that were given were: “the floor is really hot, once you touch the ground jump as high as you can, as fast as you can.” If the contact time was ≥0.3 milliseconds the jump was discarded and the participant performed it again after the prescribed rest time. 12 The Optojump Next measures the flight time (FT) and contact time (CT) and through this calculated the jump height (JH) for the CMJ and the RSI was then calculated using the equation 13 :

Each participant had a 30 second recovery between CMJs, and 60 second recovery between the DJs. The highest bilateral CMJs were used for analysis and the mean jump height and contact time from the 3 jumps was used to calculate RSI.
Inter-Limb Asymmetry
The participants were instructed to stand upright, with their feet hip width apart, and keep their hands on their hips throughout the hop. To begin the test, the participants had to lift 1 leg off the floor to approximately mid-shin height of the standing leg. The participants performed a squat to a self-selected depth followed by a hop as high as possible. The participants were instructed to land on the same leg and avoid horizontal displacement which could have an effect on flight time. Any deviations meant that the jump was retaken after a 60-second rest period. The participants performed 3 unilateral CMJs on each leg. The calculation of the inter-limb asymmetry (ASYM) was assessed through the following equation 14 :

Isometric Mid-Thigh Pull
A 3 second isometric mid-thigh pull (IMTP) was used as the measure of lower body strength. Participants stood on a custom-made platform where a load cell (LCM Systems Ltd, UK) was anchored, and the signal was processed by Powerlab. On the other end of the load cell there was a chain and at the end of the chain a small bar that was placed at mid-thigh.
The participants were asked to assume the position by self-selecting their hip and knee angles 15 while following the instructions, “place the chain between your feet, and your feet underneath your hips, to keep your knees soft, your back flat (neutral) and upright.” The height of the bar was recorded for the post-test assessment. They were then given the following instruction: “pull the bar with straight arms and push the platform away with your legs while maintaining your posture.” The participants were instructed to relax before the command “Pull!” to avoid the precontraction. 15 The pull lasted for 3 seconds, for 3 consecutive trials with 5 seconds rest between the pulls, and the peak force (N) was then recorded and was used for the analysis.
Intervention Group
The participants were asked to arrive at the gym at the start of their daily ballet class 5 times per week. The “11+ Dance” program consists of neuromuscular-based exercises. 9 The focus of the program is on muscle activation, local muscular endurance, balance and coordination, together with take-off and landing technique. The workout is split in 3 parts, Part 1: activation and local muscular endurance, Part 2: balance and coordination and Part 3: bilateral and unilateral take-off and landing technique (Supplemental Table A). The pool of the selected exercises used in the workout were split into 2 sessions which were alternated daily to minimize the risk of motivation loss through training monotony. 16 The coach who delivered the sessions had over 15 years of experience in coaching adolescent athletes.
Control Group
The participants performed exercises they would normally do with their dance teacher for 30 minutes before their ballet class. The 4 teachers, who had substantial experience (≥10 years) in teaching adolescent dancers, selected their own exercises, with no instructions from the principal investigator. Exercises included local muscular endurance, core musculature activation, balance and proprioception (Supplemental Tables B-E).
Statistical Analyses
Independent sample t-test was conducted to assess any potential between-group differences in the participants’ characteristics. Analysis was conducted based in the intention-to-treat principle. One-way Analysis of Covariance (ANCOVA) was conducted to test for a statistically significant difference between the 11+ Dance and the Control groups on CMJ, RSI, IMTP, and ASYM, controlling for the baseline scores and adherence. Effect sizes were calculated using partial eta square (
In the case of null findings in the primary and/or the secondary outcomes, equivalence testing was utilized to assess whether the intervention is equivalent or not with the usual training (control group). The 2 one-sided tests (TOST) procedure was used using standardized differences (eg, Cohen’s d) or raw differences (eg, 0.3 scale point on a 5-point scale). 17 The equivalence of the intervention is established when there is enough evidence that its efficacy is within Δ units from the Control group, 18 which means that the between-group difference is smaller than the smallest effect size of interest. 19 Δ Lower (ΔL) represents the minimum acceptable negative between-group difference for them to be considered equivalent whereas Δ Upper (ΔU) represents the maximum acceptable positive between-group difference for them to be considered equivalent. ΔL and ΔU are critical components in equivalence testing, defining the range within which differences are considered clinically insignificant. 18 The null hypothesis, therefore, is the presence of a true effect of ΔL or ΔU, and the alternative hypothesis is either the absence of an effect that is worthwhile to examine or the effect that is within the equivalence bounds. 17 For this study the equivalent bounds are set as ΔL = −.3 and ΔU = .3. 20 Alpha level was set at P < .05 and 90% confidence intervals. 18 When used together with null hypothesis significance tests (NHST), 4 outcomes are possible for a study: (1) statistical equivalence, whereby the effect is larger than ΔL but smaller than ΔU and no statistical difference from zero, (2) statistical difference from zero but not statistical equivalence, (3) statistical difference from zero and statistical equivalence or (4) neither statistical difference from zero nor statistical equivalence i.e. inconclusive outcomes. 17
Analyses were conducted using the statistical software Jamovi (version 1.0) retrieved from https://www.jamovi.org and in R (R Core Team, 2014) whereas figures were produced using the package TOASTER.
Results
No between-group statistical differences were observed for the participants’ characteristics. Three participants (8%) from the 11+ Dance group and 4 participants (11%) from the control group couldn’t complete part of the testing battery due to injury and therefore were excluded from the analysis of the tests they did not complete. Adherence for the 11+ Dance group was 72 ± 13% (range 6-35 sessions) and for the Control group 77 ± 9% (14-37 sessions). Participants included in the analyses completed at least 21 sessions, with only 2 participants in the control group completing 14 and 17 sessions. Reasons for not doing the workout were: illness, medical appointment, injury, or lack of time due to shorter ballet class. Participants in the pilot and main trial reported delayed onset muscle soreness (DOMS) during the first 2 weeks of the intervention. This information was gathered through informal conversations with the Principal Investigator. The soreness did not affect their daily practice and faded away as the participants got used to the new exercises. No adverse effects were reported from the control group.
Mean differences for both groups for all the assessed parameters are presented in Table 2.
Baseline and Post Intervention Mean Differences for CMJ, RSI, IMTP, ASYM for the 11+ Dance and Control groups.
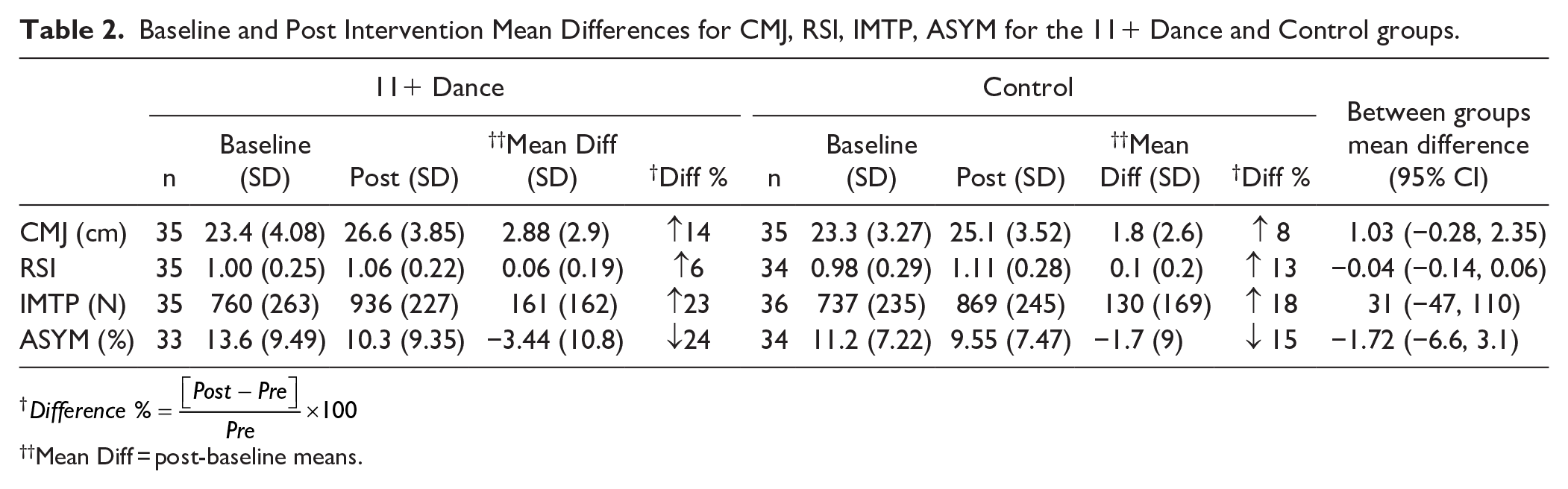
Mean Diff = post-baseline means.
The ANCOVA (between-group factor: group [11+ Dance, Control]; covariate: baseline scores and adherence) revealed no statistically significant effect of the 11+ Dance on CMJ, F(1, 66) = 3.52, P = .065,

(a) Equivalence analysis for CMJ; (b) Equivalence analysis for RSI; (c) Equivalence analysis for IMTP; (d) Equivalence analysis for ASYM.
The analysis showed no between-group differences for RSI F(1, 65) = 1.02, P = .316,
In the baseline and post-test the participants in the 11+ Dance and Control groups had similar results for the isometric mid-thigh pull, with no statistically significant between-group change F(1, 67) = 1.7, P = .197,
After the end of the intervention period, similar changes were observed in the inter-limb asymmetry in both groups. No between group differences in change were observed for ASYM F(1, 63) = .109, P = .743,
Based on the equivalence test and the null hypothesis test combined, it can be concluded that the observed effects for CMJ, RSI, IMTP, and ASYM are inconclusive, as they are not statistically different from zero nor statistically equivalent to zero.
Discussion
The main finding of this investigation was that no statistically significant performance differences were observed in any of the outcome measures between the 11+ Dance group and the Control group. Equivalence was not established therefore it cannot be stated whether the 11+ Dance is either superior or inferior to current training practices for the development of the selected physiological parameters. More specifically, both groups improved over time in the primary outcome (CMJ) and presented similar results for RSI, IMTP, and ASYM.
No studies on adolescent dancers appear to have examined the effects of neuromuscular training on muscular power, explosiveness, muscular strength, and inter-limb asymmetry, therefore direct comparisons are not possible. Even though the mean difference of baseline-post change between the 2 groups was not statistically significant in CMJ, the clinical significance of a 14% and 8% improvement in 7 to 9 weeks, for the 11+ Dance and Control groups respectively is not negligible. A meta-analysis (26 studies, n = 1.024,
Neither group revealed statistically significant change for the RSI. The observed 6% (0.06 units) and 13% (0.13 units) increase for the 11+ Dance and Control group respectively may not be clinically significant either. It has been suggested that decrements in RSI of 0.15 units may be a meaningful change threshold in elite junior athletes, whereas anything less than this may simply be “noise” in the data. 22 The participants of the current study performed rope skipping, a low intensity activity, in order to primarily raise the body temperature, heart and respiration rate, blood flow and joint viscosity, but also to promote a stretch-shortening-cycle stimuli. 23 A recent rope skipping study by García-Pinillos et al. 24 reported improvements in CMJ (3%, P < .001) and RSI (0.3%, P < .001) after a 10-week rope skipping training program for the intervention group. It is noteworthy, however, that not all the participants had the same skill level when performing this task and may affect the ground reaction force and peak force. 25 Two teachers utilized rope skipping in their training, which may have affected the between-groups difference, and may have been a contributing factor for the jump-height improvements in both groups as rope skipping was not part of the usual training before the start of the trials. The total number of the rope-skipping foot-contacts was not calculated for this trial. We speculate that the lack of RSI improvements for the 11+ Dance group may have been associated with the daily training dose of skipping. In addition, post testing commenced the day after the intervention was completed, therefore fatigue may have been a factor that needs further investigation.
The IMTP mean difference was not statistically significant for both groups at the end of the trial. A reliability study on the use of the IMTP with adolescent dancers revealed that the minimal detectable change for this population is 12%. 26 The clinical significance, therefore, of the 23% and 18% in the 11+ Dance and Control group respectively is worth mentioning. Even though it has been suggested that the size of the gains in strength and power are probably dependent on the assessment and the training mode being similar, 27 the use of an isometric strength test indicates strength improvements in both groups. The only isometric exercises in both groups were the plank and its variations, whereas the rest of the exercises were dynamic. Research suggests that the IMTP correlates to dynamic athletic tasks. 28 Increases of muscular strength have been observed in injury prevention studies, however, strength is usually assessed with isokinetic strength protocols for the quadriceps and hamstrings.2,29
The inter-limb asymmetry (ASYM) change difference was not statistically significant. It decreased by 24% and 15% in the 11+ Dance and Control group respectively. Prior to the intervention the mean for both groups was <15%. It has been previously suggested that a 15% asymmetry threshold may be a critical threshold for increased injury risk prediction for athletic populations. 30 We speculate that regular exercise may have a positive effect on muscle asymmetries in adolescents with low training age. As there are no normative data for inter-limb asymmetry and its association with injuries in dance, it is unclear whether the observed asymmetry decrease in both groups is clinically significant and needs to be investigated further.
The results of this study suggest that daily low intensity bodyweight supplementary training may be inducing physiological adaptations in adolescent dancers as observed by the reported DOMS for the 11+ Dance group, however, the selected test battery may not have been sensitive enough to detect all the potential changes from the exercise interventions. The positive effects of neuromuscular training on landing kinematics have been previously reported.3,31 Whilst speculative, it may be that the combination of all the exercises (strength, balance, plyometrics) may promote a level of neuromuscular control not detectable by the selected tests.
It has been suggested that the higher the volume of neuromuscular training, the higher the effect, 32 however, studies with neuromuscular training incorporate 2 or 3 sessions per week as part of the training sessions the participants normally have. In the current trial, the participants trained daily, therefore, they needed to warm-up every day. Even though the selected exercises were split in 2 sessions, and they were rotated daily, the sessions had similarities. The dosage, therefore, needs to be investigated further for optimal results. In the absence of a true control group, the observed improvements for both groups raise the question whether they are due to exercise induced adaptations, the reduction of dance load (n = 2.5 h week−1), or the combination of both.
Contrary to sports, dance training is driven by movement proficiency rather than physiological parameters such as maximum jump height, or muscular strength development. Whilst improving physiological parameters has anecdotally been the current trend for the dance industry, the relationship of such parameters and injury incidence is not clear through the existing literature. 33 Even though the results of this study support the null hypothesis, equivalence was not established and the 11+ Dance did not cause any harm. Adverse events were recorded for both groups, but these events were not directly associated with the given interventions. Based on the current evidence on neuromuscular injury prevention interventions, it is possible, that with a larger sample size the results may have been statistically significant.
Lastly, a recent systematic review and meta-analysis of randomized and nonrandomized controlled trials has suggested a best-practice meta-analytic checklist for anterior cruciate ligament (ACL) injury prevention interventions in team sports. Overall, the most effective injury prevention programs included trained personnel, were aimed at younger athletes, exposed athletes to neuromuscular training throughout the whole season, and included lower body strengthening and landing stabilization exercises. 34 Even though the focus of such interventions is on traumatic injuries (ie, ACL, ankle sprains), there is evidence to suggest these interventions can be effective in reducing overuse injuries,4,35 which characterize the adolescent vocational dance population.36,37 When assessing the 11+ Dance according to the above checklist, the intervention scores 10 out 11. When compared with current practice the 11+ Dance consists of exercises that are not included in the warm of an adolescent ballet dancer, it may therefore be useful to complement and not replace the existing practice. The 11+ Dance, however, could be considered an evolution of practice, and could be utilized as a framework for further development.
Although the current study is novel in several aspects, such as randomization, blinding of assessment, standardized intervention protocol, and statistical analyses when interpreting the results, practitioners should be aware of some identified limitations. The assessed intervention (11+ Dance) was compared against 4 different types of exercise programs, but all 4 programs were grouped as usual training for the Control group. It is thus difficult to identify which of these combinations were more or less effective against the 11+ Dance workout. Furthermore, to protect the results from the potential learning effect of the intervention, we have only analyzed data from participants who were exposed to the intervention for the first time. Even though we combined data from 2 trials, the recruitment of the necessary sample to achieve the desired power was not possible due to the trial being in an applied setting. Based on the null hypothesis testing, therefore the reported results may be giving a false negative (Type II error) outcome.
Considering the previously reported high injury prevalence in pre-professional dancers and the potential adverse effects injuries can have in their development, this trial offers a steppingstone for further research in injury prevention interventions for dancers.
Conclusion
The results of this study reveal that in the short term, the 11+ Dance elicited similar effects with the current training workouts on the selected parameters, however, equivalence was not established. Muscular power and strength improved for both groups, therefore, low intensity supplementary training may need to be part of dance training, to compliment the development of the young dancer. No negative adverse effects were observed for the 11+ Dance and adherence was high as the training was incorporated in the existing load, therefore, the 11+ Dance injury prevention intervention may be utilized to complement existing practice. Larger longitudinal studies are needed to investigate the efficacy of the 11+ Dance on injury incidence and severity.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X241300567 – Supplemental material for The Effects of 11+ Dance on Physiological Parameters in Adolescent Ballet Dancers: A Randomized Controlled Equivalence Trial
Supplemental material, sj-docx-1-dmj-10.1177_1089313X241300567 for The Effects of 11+ Dance on Physiological Parameters in Adolescent Ballet Dancers: A Randomized Controlled Equivalence Trial by Nico Kolokythas, George S. Metsios, Shaun M. Galloway, Nick Allen and Matthew A. Wyon in Journal of Dance Medicine & Science
Supplemental Material
sj-docx-2-dmj-10.1177_1089313X241300567 – Supplemental material for The Effects of 11+ Dance on Physiological Parameters in Adolescent Ballet Dancers: A Randomized Controlled Equivalence Trial
Supplemental material, sj-docx-2-dmj-10.1177_1089313X241300567 for The Effects of 11+ Dance on Physiological Parameters in Adolescent Ballet Dancers: A Randomized Controlled Equivalence Trial by Nico Kolokythas, George S. Metsios, Shaun M. Galloway, Nick Allen and Matthew A. Wyon in Journal of Dance Medicine & Science
Footnotes
Acknowledgements
The authors would like to thank the Elmhurst Ballet School students and teachers for their help and support for the completion of these trials. Also, a big thank you to Leeroy Watson for his help in the post testing. And lastly but as importantly to all the members of staff at Elmhurst Ballet School for their continuous support over the years.
CRediT Author Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: These trials were part of a PhD project that was fully funded by Elmhurst Ballet School.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.