
Abstract
Introduction: In 2012, the Standard Measures Consensus Initiative (SMCI) of the International Association for Dance Medicine and Science (IADMS) presented 6 recommendations regarding dance injury surveillance, definitions of injury and exposure, dance-specific screening, risk reduction strategies, and collaborative data management. The aim was to standardize risk factor measurement and injury reporting by researchers in dance medicine and science. Since then, numerous reports on the recording and reporting of injury data in sport and performing arts have been published. Methods: IADMS commissioned SMCI to update the 2012 recommendations, a process that involved 3 stages: (1) current field experts were invited to join SMCI, (2) SMCI members reviewed recent and relevant sport and performing arts literature, then drafted, discussed, and revised section updates, (3) IADMS invited individuals representing diverse backgrounds in the IADMS community to critically review drafted updates. The final update serves as a bridge from the 6 recommendations in the 2012 report to the current state of evidence. Results: We continue to encourage use of dance injury surveillance systems and support that surveillance protocols be fit-for-purpose, and that failure to use clear and consistent injury definitions perpetuates a lack of rigor in dance injury research. Based on new evidence, we recommend that some aspects of injury surveillance be self-reported, that the choice of dance exposure measures be dependent on the research question, contextual factors, and type of injury/health problem(s) of interest, and that studies using dance-specific screening articulate specific objectives, validity, and reliability of each protocol. Conclusions: Future studies should focus on the development, implementation, and evaluation of strategies to minimize injury risk to improve consistency and rigor in data collection and research reporting on the health and wellness of dancer populations, thus facilitating a future dance injury consensus statement similar to recent statements published for sports and circus arts.
Key Points
In the past 10 years, the number of published dance injury studies has increased 5-fold.
The purpose of this article was to update the 6 recommendations published in 2012 to strengthen the foundation for continuing to improve the clarity, utility, and comparability of injury reporting in dance medicine and science.
Future research that builds on this foundation for evaluating, managing, and reducing dance injury risk will be particularly useful to our field.
Introduction
In recognition of the need for standardized testing and reporting methodology in dance medicine and science research, the International Association for Dance Medicine and Science (IADMS) launched a multi-year consensus-building project in 2004; the Standard Measures Consensus Initiative (SMCI). 1 The SMCI taskforce undertook a review of the literature and of current practices to develop evidence-based recommendations for the standardization of testing and reporting methods for dance-related injury research. Six recommendations were published in 2012 to provide guidance for those conducting research in the field of dance medicine and science that related to injury surveillance, how we define both injury and dance exposure, dance-specific screening, risk reduction strategies and collaborative data management. 1 The 2012 report has been cited in numerous dance injury publications that have primarily focused on pre-professional and professional ballet and contemporary dancers.2 -11
As dance injury research has continued, new knowledge has come to light that supports the need for a bridge from the original 6 recommendations in the 2012 report to the current state of evidence. For example, relatively recent systematic reviews have concluded that research striving to identify risk factors that predict musculoskeletal injury in dancers still suffers from inconsistent injury definitions,12,13 perpetuating the challenge of comparing results across studies and understanding the true burden of dance-related injury. In addition, we now know more about the perception of injury from different stakeholders, 14 and the various barriers that exist when it comes to injury reporting15,16 that is based on current research not only in dance,17 -26 but other performing arts,27 -29 and sport,30 -33 supporting the need to update the 2012 report.
While still encouraging the principle of standardization and appropriate reporting in the field, this update endorses a broader scope of methodological approaches to injury surveillance, operational definitions, screening, risk reduction, and data management in dance. A glossary of terms is included as a Supplemental file.
Methods
In 2020, IADMS commissioned the SMCI taskforce to update the 2012 recommendations for best definition and measurement practices within the dance medicine and science community. This process involved three stages. First, a formal and transparent procedure was followed to select dance scientists currently researching in the field of dance injury epidemiology and healthcare professionals currently practicing in the field of dance medicine to join two members of the original 2012 SMCI taskforce, who had agreed to participate in the update. The selection process began with the IADMS Board inviting volunteers, via the IADMS quarterly e-newsletter and website, to apply to fill open seats on the taskforce. Due to the global COVID-19 pandemic, the deadline for applying to the taskforce was postponed one year. By the end of 2021, the SMCI taskforce reviewed all applicants’ background qualifications and letters of interest, and made recommendations to the IADMS Board of Directors, who then appointed eight qualified members. One member declined because they were no longer active in the field. The 2022 SMCI taskforce (i.e., authoring group of this paper) comprises 7 scientists and clinicians with in-depth knowledge regarding dancers’ health monitoring in Europe, North America, and Australia, and extensive experience working with dancers from different age groups, genders, genres, and levels. Members’ expertise represents a variety of professional backgrounds including dance medicine, dance science, dance epidemiology, human movement sciences, and biostatistical analyses. Members also represent diverse ages, career stages, genders, nationalities, and dance backgrounds.
Second, all 7 members of the 2022 SMCI taskforce reviewed and discussed the 2012 recommendations, alongside recent and relevant sport and performing arts literature. Regular meetings were conducted virtually due to the COVID-19 pandemic and geographic distance between members throughout 2022. A total of 8 online meetings were held: one as an introduction and strategizing session, followed by 6 meetings, each focused on one of the specific recommendations included in the 2012 report. A final meeting was conducted to synthesize the discussion and concluding statements. After each meeting, taskforce members volunteered to draft updates to specific recommendations based on their content expertise. The section drafts were presented and discussed during the virtual meetings and revised according to feedback from all members until there was a completed initial draft of the updated recommendations.
Third, 9 individuals representing diverse academic, professional, and geographic constituencies of the IADMS community were invited by the IADMS Board to review and provide feedback on the initial draft of the report at 2 focus group sessions moderated by a member of the IADMS Board of Directors. The 2022 SMCI taskforce incorporated revisions based upon recommendations offered by these individuals. A second draft was circulated among the authoring group and a subsequent draft was submitted to the Journal of Dance Medicine & Science (JDMS) for peer review.
Updated Recommendations
The SMCI 2012 report consisted of 6 recommendations for assessing and reporting dancer capacities, risk factors, and injuries. 1 Below, each recommendation is discussed individually in light of current literature and expert opinion.
Injury Surveillance
In 2012, the SMCI established, based on best practice behaviors and consensus recommendations at the time, that a dance injury surveillance system should, ideally, (1) be mandatory, (2) utilize licensed healthcare professionals trained in the diagnosis of injuries, and (3) employ a standardized protocol for capturing injuries per exposure for all dancers within a specified group. While these recommendations allow for a robust, valid, and reliable protocol, there has been much progression in the field of sport and dance injury research that warrants fresh consideration.
Dance organizations (e.g., companies, schools) are still strongly encouraged to have surveillance systems. If research is attached to these systems, understanding study design options that do not require mandatory participation is preferred. This is because a core principle of research ethics states that there is to be respect and opportunity for inclusion for all human participants, ensuring that participants’ autonomy be demonstrated by the provision of their voluntary informed consent. 34
Striving for full participation does not oppose this important ethical consideration. High participation rates in dance injury surveillance programs are important. Strategies to maximize participation in these surveillance programs should include the onboarding of all those involved (e.g., dancers, parents, teachers, choreographers, artistic staff, academic staff, directors, and studio owners). Onboarding can occur by providing clear rationale for why participation is important and explaining how dancers may benefit, directly or indirectly, by engaging in a process that is fully described. Involving relevant stakeholders and articulating clear advantages when introducing ethics approved studies to each group will likely encourage and support participation in dance injury surveillance programs. 7
Second, while the utilization of licensed healthcare professionals who are trained in the diagnosis of injuries increases the validity and reliability of health data captured in the surveillance system, there is now evidence to support the self-reporting of injuries by athlete and dancer populations.31,35,36 Specifically, the work of Clarsen et al.35,36 has led to the validation of two questionnaires that are able to capture a more complete picture of the injury burden experienced by athletes and dancers alike. This is particularly important among dancers who do not have easy access to healthcare and when the use of licensed healthcare professionals to diagnose or report injuries is not always feasible. The validation of self-report surveys has expanded the possibility of producing internally valid research studies focused on understanding the prevalence of dance injuries that do not result in medical attention. 19
Finally, it is understood that when protocols for collecting data are standardized, a certain level of comparability across studies is enabled, which allows for effective systematic reviews to draw important conclusions about a particular field of research. Healthcare professionals are encouraged to follow standard practice of patient documentation, but in the past decade, much debate has occurred to understand the strengths and limitations of different injury surveillance designs more fully.37 -39 As such, depending on the aims of the research, injury surveillance programs that are fit-for-purpose are strongly encouraged. For example, when it is important to understand the full extent of injury burden among a specific group of dancers, self-report may be most appropriate. If it is necessary to understand the financial cost of medical resources, an injury reporting system involving healthcare and administrative professionals may be best. Regardless of the surveillance methods chosen, what is essential for future researchers to include in the reporting of their dance injury results is a clear rationale for, and acknowledgement of, the methods utilized in their study and the relevant limitations of their choices.
Updated Recommendation #1: Injury Surveillance
Use of a dance injury surveillance system is still strongly encouraged.
The surveillance protocol should be tailored to fit the purpose for which the results are being collected.
Some aspects of injury surveillance can be self-reported by dancers (e.g., impact on dance participation, injury location, first report).
Injury Definitions
Because it was considered the most reliable injury definition available, the original report recommended that dance injury be defined as an anatomic tissue-level impairment, as diagnosed by a licensed healthcare professional, that results in full time loss of activity (i.e., dance activity) for one or more days beyond the day of onset. The 2012 guidelines recommended that events not meeting these three criteria should not be defined as “injuries” but as musculoskeletal complaints. The 2012 publication also presented several considerations that helped form this recommendation, including the acknowledgement that injuries occur along a spectrum of severity, that no single injury surveillance system can capture everything, that there are other conventional modes of defining injury (e.g., tissue pathology, time loss, functional loss, cost of care), and that there are systematic challenges in defining injury (e.g., some dancers will not experience time loss even with substantial tissue damage).
The recommended definition of injury has likely been the most discussed item of the 2012 report.9,19,37,39 While there is continued need to emphasize the use of clear injury definitions in dance medicine and science publications, 12 considerable desire to expand the recommended definition of injury has been expressed.9,19 Three key themes underlie this desire.
First, in addition to the logistical challenges described above (i.e., access to healthcare professionals who can diagnose injuries is often limited), there are now valid and reliable tools that can identify injury via other means such as self-report. 31 For example, the Oslo Sports Trauma Research Center (OSTRC) Questionnaire on Health Problems has demonstrated high reliability 35 and has been adapted for dance. 19 It is important to note however, as the period of time increases between injury event and injury report by those who are self-reporting, recall bias can compromise the accuracy of data captured. 40 Therefore, self-reported measures should only use validated tools (i.e., those that have been tested to measure what they are designed to measure) where interpretations of this data are made with caution.
Second, different operational definitions of musculoskeletal injury can impact injury estimates. For example, time-loss and medical attention injury definitions may be well suited to capture acute injuries but may be less adept for identifying the occurrence or burden of subacute, recurrent or chronic injuries that are common in dance. 19
Third, some musculoskeletal symptoms that are prevalent in dance (e.g., low back pain), can have considerable impact (including disability, care-seeking, medication use, distress, and distraction) but they may not correlate well with identifiable tissue damage and would not meet the threshold for inclusion in an injury surveillance system outlined by the 2012 guidelines.1,41 It is now more broadly appreciated that excluding injuries (or complaints) from surveillance systems because the tissue damage cannot be objectively verified may negate the individual dancer’s experience. 42
While the desire for a broader definition of injury has been heard, some caution needs to be taken when selecting a definition for individual studies. For instance, a broad definition may be more sensitive but also less specific and will therefore not suit all injury surveillance purposes. 37 It would also be remiss to discuss broadening the dance injury definition without acknowledging the potential impact of wider injury definitions. That is, a broad definition of injury may shift the boundaries between disease and health and may encourage healthcare use when it may not be needed.43,44 Examples of specific research objectives and suggested corresponding injury definitions are presented in Table 1.
Examples of Research Objectives by Different Injury Definitions.

This SMCI update will stop short of recommending one specific definition of injury to be used in dance injury methodology. Instead, we recommend that those conducting dance injury research need to have clear reasoning, and articulation of, the injury definition chosen to match the purpose of their project. Having said this, injury definitions need to be valid and reliable, and the reporting of injury estimates must adhere to standards outlined in appropriate guidelines such as STrengthening the Reporting of OBservational studies in Epidemiology (STROBE).30,45 Researchers should also continue to consider definitions that allow for comparison with established studies. Finally, we emphasize that failure to use clear and consistent injury definitions will continue to perpetuate a lack of rigor in future dance injury research.
Updated Recommendation #2: Injury Definitions
Operational definitions of dance injuries should:
Be valid, reliable, clearly described, and adhere to appropriate reporting guidelines.
Align with the purpose of each research study.
Facilitate comparability with previous research.
Defining Exposure
The 2012 SMCI offered this definition of injury risk exposure: Participation in a class, rehearsal, or performance in which the dancer was exposed to the possibility of a dance injury. In agreement with a recent consensus statement published by the International Olympic Committee (IOC), 30 we acknowledge that there are several options to quantify dance exposure. The choice of the most appropriate dance exposure definition is influenced by the research question, contextual factors, and the type of health problems under consideration. 17 The 2012 recommendations outlined models used in sport that included annual contracted work hours, athlete exposure, time exposure, and element exposure, highlighting that from first to last, exposure measurement becomes more precise. For instance, if the aim of a study is to investigate the association between jumping and injury risk, assessing the element exposure, or the number of jumps or jump height, may be of most interest to answer the research question. 46 If the purpose of the study is to compare injury risk in different target groups (e.g., across different styles of dance, across different levels of dance participation, or dancers versus athletes), researchers may want to use time exposure, which aligns with epidemiological recommendations for sport and circus arts.27,30
Although assessing dance exposure is fundamental in quantifying dance injury risk, exposure is not required for all injury-related research. For example, when investigating injury prevalence, dance exposure data may not be essential. 47 However, when quantifying injury incidence, when examining the relationship between dance exposure and injury, or when exploring other contributors to injury risk where dance exposure may influence injury outcomes, collecting dance exposure data is required. 48
Updated Recommendation #3: Defining Exposure
To understand the extent of a dance injury problem, capturing and reporting dance exposure may be necessary.
The choice of dance exposure measures (e.g., contracted work hours, dancer exposure, time exposure, element exposure) should be based on the research question, the contextual factors, and the type of injury/health problems of interest.
Dance-Specific Screening
In response to the lack of standardized approaches to screening in the dance medicine and science community at the time, the SMCI recommended in 2012 that dance-specific screening utilize the Pre-participation Physical Evaluation (PPE) as a basis for dance-specific screening, given its strong consensus by major medical associations. 1 Typically, the PPE examination is conducted by a healthcare professional with clinical training to evaluate and determine medical eligibility of an athlete/dancer on a broad range of health issues. 49 What has become clearer in the last 10 years is further acknowledgement that dance educators can facilitate screenings as well, not to medically diagnose, but to provide education, resources, training, and health-informed benefits for dancers when healthcare professionals are inaccessible.50,51 Educator involvement in screening processes stems from further understanding of the multiple benefits of conducting screening with different dancer populations. These include providing education and access to resources about dancers’ health and wellness and assisting educators in identifying opportunities for improvement and most appropriate referrals. Screening results may also help with planning appropriate training, goal setting, tracking dancers’ progress across a season, and facilitating communication, collaboration, and rapport-building between dancers, parents, educators, and healthcare professionals.
The SMCI recommended in 2012 that additional tests and measures with specific relevance to dancers be added to the fundamental PPE as they are developed and validated. 1 The emphasis on dance-specificity has become more important in recent years, especially with publications concluding that dance injury risk profiles may be unique to the dance genre. 52 Further, screening for mental health, 53 risky behavior which may increase likelihood of long-term disability or premature death, 54 and removing the inappropriate use of body composition measurements, 55 may also be important, all of which reinforces the 2012 conclusion that screening is most effective when undertaken in the context of a broader, longitudinal healthcare program approach that addresses the biopsychosocial aspects of the dancer’s life. 1
While utilizing standardized, evidence-based assessments (e.g., injury history, functional physical tasks) allows for comparisons to be made across studies, it has become increasingly clear that screening is limited in its ability to predict injury. 56 With multiple reasons to employ dancer screening, specific goals and objectives should be considered when designing studies and developing protocols. Key considerations include using valid and reliable assessments to ensure a high quality of research, explaining the specific use of all data gathered to ensure efficiency, and including enough detail in manuscripts for comprehensive systematic reviews to be conducted. What remains a central, enduring strength of the 2012 publication, is that “the communication of results and a follow-up plan with the dancer should be an essential part of the screening process.” 1
Updated Recommendation #4: Dance-Specific Screening
Study designs that use dance-specific screening need to articulate the specific objectives of the screening program and the validity and reliability of each protocol.
Communication of results and a follow-up plan with the dancer should continue to be included in the screening process.
Risk Reduction Strategies
The biopsychosocial model of functioning from the World Health Organization (WHO) recognizes that risk of injury is due to the interaction of causative factors over time.1,57 The WHO model can serve as a useful framework, and several other models also emphasize the complex interplay between different injury risk factors that are dynamic in nature. For example, the Dynamic, Recursive Model of Etiology in Sport Injury has been widely used in sport injury research. 58 Like the WHO, this model emphasizes the importance of examining both intrinsic and extrinsic factors, possible interactions between these factors, and how these factors change with repeated participation (repeated exposure), irrespective of injury outcome. Bittencourt et al. 59 similarly have proposed that sport/dance injuries arise from the complex interaction among a web of determinants, rather than from a linear interaction between isolated and predictive factors. 59 Though based on anterior cruciate ligament (ACL) injuries that have low prevalence and incidence in professional ballet when compared to team ball sports, this starting point can provide a basis to generate the development of injury risk reduction strategies by encouraging researchers to identify an individual dancer’s and dancer groups’ risk profiles, and to move toward recognizing injury risk patterns rather than simply identifying specific independent risk factors.
The second part of the SMCI 2012 risk reduction recommendation states that successful predictive models can only be built once there is broad acceptance of standards for reporting, such as embracing the WHO’s biopsychosocial model of functioning. A successful predictive model requires biostatistical analyses that account for predictive power between risk factor(s) and injury outcome. A possible limitation with the current dance injury research is the use of correlation and regression analyses to identify risk factors that may lead to a reductionist view in which causality is assumed to be linear and unidirectional. That is, they do not acknowledge the complex interplay between injury determinants described above. Therefore, it may be important to use more sophisticated biostatistical techniques to account for constellations of risk factors that interact in ways that make dancers vulnerable to an injury event.18,60
What has not changed since 2012 is that reducing dancers’ injury risk remains one of the greatest challenges in dance medicine and science. Since the 2012 report, few evidence-based reduction strategies for dance injuries have been published.23,24 This might be explained by the complex process needed to develop, implement, and evaluate these strategies. As an example, the randomized controlled trial (RCT), which is considered the gold standard of experimental research designs, 61 may not be feasible in some dance settings such as recreational, vocational, or professional environments.
The Translating Research into Injury Prevention Practice (TRIPP) framework, 62 which builds upon van Mechelen’s 1987 sequence of prevention model, proposes 6 steps needed to develop good understanding and strong evidence for how to minimize the risk of injury:
Step 1. Identify the magnitude of the injury outcome(s) of interest.
Step 2. Identify risk factors and causes of the injury outcome(s) of interest.
Step 3. Develop and introduce risk reduction strategies based on the injury outcome(s) of interest.
Step 4. Evaluate the effectiveness of the risk reduction strategies.
Step 5. Integrate the risk reduction strategies into real-world settings.
Step 6. Evaluate the real-world implementation of the risk reduction strategies.
In dance injury research, studies have largely focused on step one of this model. While there has been recent work investigating risk factors for and causes of dance injuries,18,21,22 the need for high-quality and high-level studies to inform practice remains. The two final steps of the TRIPP framework guide researchers to understand the real-world, context-specific settings (e.g., exploring dancer beliefs related to injury, 14 as well as barriers and facilitators to the uptake of risk reduction strategies), 63 prior to integrating and evaluating them.
Updated Recommendation #5: Risk Reduction Strategies
Risk reduction strategies should continue to be evidence-informed and recognize that dance injury risk is due to the dynamic interaction of causative factors and repeated dance exposure over time.
Future study designs and data analyses need to account for the changing nature of risk within dancer populations.
Effective implementation of risk reduction strategies must acknowledge the feasibility and reality of the dance settings of interest.
Collaborative Data Management
Collaborative data management, the sharing of privacy-protected participant data across independent research groups, was encouraged in the 2012 recommendations, as it offers an approach that can allow greater comparison of injury patterns across groups and provide greater statistical power to identify risk factors. While collaborative data management is not free from challenges, embarking on such a task was described in 2012 as realistic, especially with a parent organization taking responsibility for quality control, ethics, and legal obligations.
These updated recommendations continue to encourage collaborative data management and collaborative surveillance projects. In agreement with the original paper, we note a single cohort on its own is unlikely to provide adequate power to detect exposure–injury relationships, and that collaboration has untapped potential to advance knowledge in dance science. We also agree that successful collaboration will continue to require consistent study design, definitions, and data collection of injury and other surveillance variables, which would ideally be negotiated between collaborators in advance. While ideal, collaboration may not need a single parent organization to oversee data collection, storage, and sharing. Other models may include sharing data gathered in independent studies with other researchers or stakeholders in a responsible manner. Katakura et al. 64 provide an example of collaborative research between two comparable professional ballet companies whereby dance injury data collected by respective onsite physical therapists was pooled to enable a large sample size reflective of the target population. It is important to note however, that individual studies and institutions, as well as differences in language and across geographic regions, may be bound by different rules regarding data sharing that may affect how collaboration can be conducted. Collaboration need not be international; starting collaboration within cities, regions, and states may be a more pragmatic approach to answering some research questions.
Updated Recommendation #6: Collaborative Data Management
Collaboration and data sharing continues to offer opportunities to address a wide range of research questions in dance.
Collaboration may be performed with a parent organization responsible for data collection, or via researchers sharing data from standalone research studies that have similar study designs.
Starting collaboration at a local level may be more feasible than at an international level.
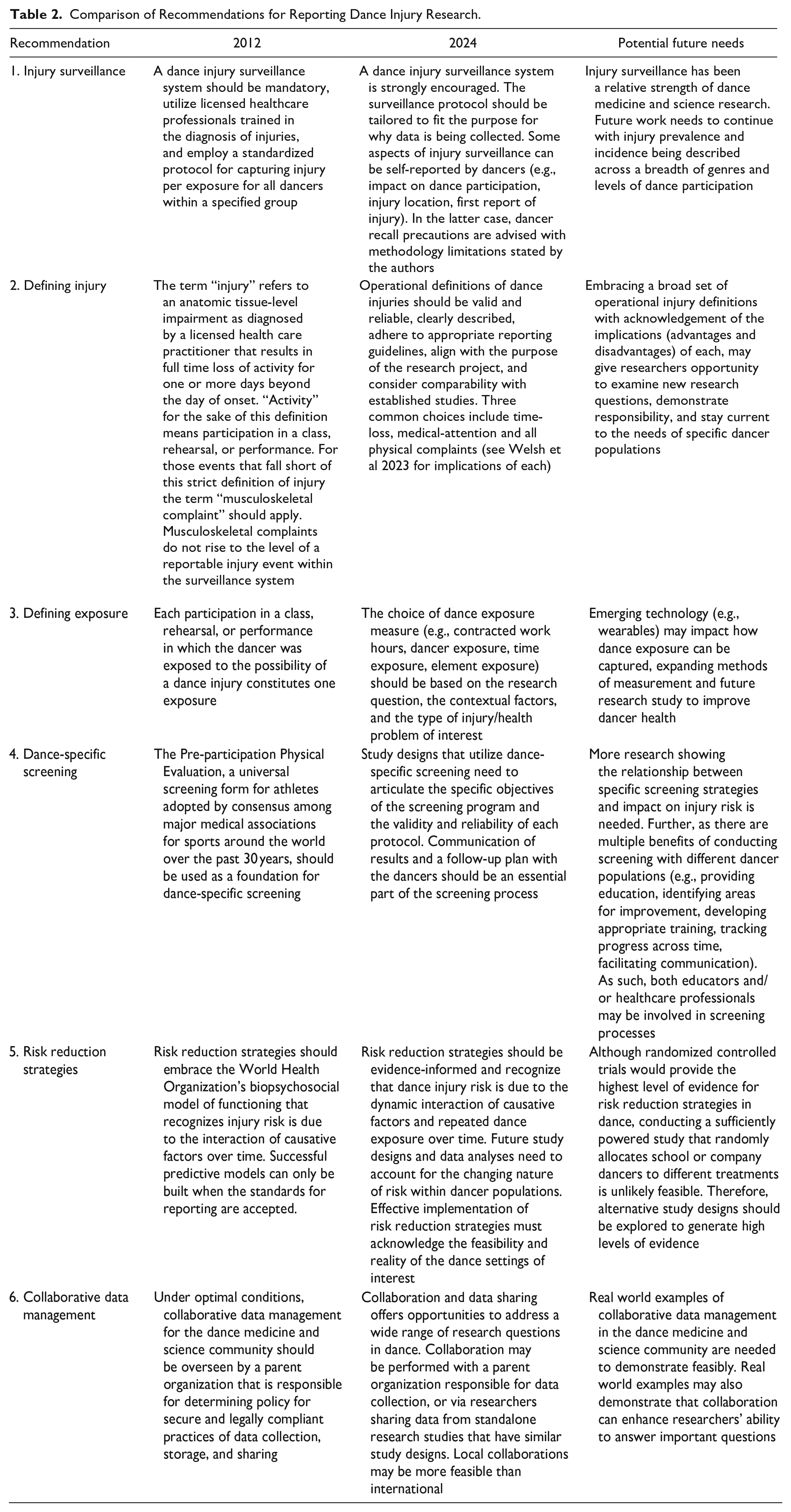
Comparisons of the 6 recommendations published in 2012, the current state of evidence, and suggestions for possible future study in these specific areas are presented in Table 2.
Comparison of Recommendations for Reporting Dance Injury Research.
Concluding Remarks
The recommendations published by the SMCI in 2012 were offered in hopes of improving the quality of scientific information to reduce the risk of dance-related injuries and that is exactly what is transpiring. During the past 12 years, the number of published studies related to one or more of the elements reviewed in this report has increased 5-fold with more papers being accepted into high quality peer-reviewed journals. Most of this research, however, has focused on the prevalence and incidence of dance-related injuries, with some research exploring injury risk factors.
This update serves as a bridge to current evidence, reporting on progress made in these 6 areas since 2012. Giving more attention to the development, implementation, and evaluation of injury risk reduction strategies will be an important next step. Conducting additional comprehensive systematic reviews to synthesize the evidence for specific dance injury research questions is advisable. As the evolving domain of dance injury research reaches a critical mass, broader reviews and meta-analyses will become feasible. All will provide useful input for a future standard measures consensus report, should IADMS choose to commission one.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X241288998 – Supplemental material for An Update on the Six Recommendations from the 2012 IADMS Standard Measures Initiative: Assessing and Reporting Dancer Capacities, Risk Factors, and Injuries
Supplemental material, sj-docx-1-dmj-10.1177_1089313X241288998 for An Update on the Six Recommendations from the 2012 IADMS Standard Measures Initiative: Assessing and Reporting Dancer Capacities, Risk Factors, and Injuries by Sarah J Kenny, Janine H Stubbe, Chris T V Swain, Joshua Honrado, Claire E Hiller, Tom M Welsh and Marijeanne J Liederbach in Journal of Dance Medicine & Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.