
Abstract
Introduction:
In classic ballet, choreography often involves tiptoe standing. Tiptoe standing requires a high and stable foot arch structure, which is achieved by contraction of the plantar intrinsic foot muscles (PIFMs). Long-term repetitive loading with a specific movement can induce hypertrophic adaptation of the associated muscles. For dancers, however, limited information on the size of individual PIFMs is available from previous studies. The purpose of this study was to determine the differences in the sizes of 10 individual PIFMs between dancers and non-dancers.
Methods:
Muscle volumes (MVs) of 10 individual PIFMs were measured using magnetic resonance imaging in 15 female dancers and 15 female non-dancers. Muscles analyzed included abductor hallucis, flexor digitorum brevis, abductor digiti minimi, quadratus plantae, lumbricals, flexor hallucis brevis, adductor hallucis oblique head, adductor hallucis transverse head, flexor digiti minimi, plantar/dorsal interossei. In addition to absolute MVs, relative MVs normalized to body mass (rMVBM) and the percentage of individual MVs relative to the sum of 10 individual PIFM MVs (%MVWHOLE) were calculated.
Results:
The absolute MVs of 6 individual PIFMs, including the flexor digitorum brevis and lumbricals, were +16% to 59% larger in dancers than in non-dancers (P ≤ .048). The rMVBM of all individual PIFMs were +35% to 95% larger in dancers than in non-dancers (P ≤ .019). The %MVWHOLE of the flexor digitorum brevis and lumbricals were +10% to 36% higher (P ≤ .014) and those of the abductor digiti minimi and adductor hallucis oblique head were +8% to 11% lower (P ≤ .037) in dancers than in non-dancers.
Conclusions:
For all 3 MV measures, only the flexor digitorum brevis and lumbricals, which are functionally specialized for flexion of the second to fifth metatarsophalangeal joints, were consistently larger in dancers than in non-dancers. This may be due to long-term repetitive loading on these PIFMs during ballet training involving tiptoe standing.
Keywords
Key Points
The loading of the foot during ballet training, which is characterized by tiptoe standing, may cause hypertrophy of some individual plantar intrinsic foot muscles.
This is the first study to use magnetic resonance imaging to examine the differences in the sizes of 10 individual PIFMs between dancers and non-dancers.
The plantar intrinsic foot muscles, which cause the metatarsophalangeal joint flexion of the lesser toes, may play a specifically important role during ballet training involving tiptoe standing.
Introduction
Long-term repetitive loading with a specific movement causes hypertrophic adaptation of the muscles involved in that movement.1 -3 In classic ballet, specific movements that involve tiptoe standing (ie, “demi-pointe” or “en pointe” in ballet terminology/choreography) are often performed, in which ballet dancers (hereafter referred to as “dancers”) are required to form a high foot arch structure that is considered esthetically desirable.4 -6 The foot arch structure is primarily supported by passive, non-contractile components (bones, ligaments, plantar fascia, etc.). 7 However, under conditions of high postural demands or heavy foot loading, stabilization of the foot arch structure is achieved via the additional force produced by the contracting muscles in the foot.8,9 In addition, dancers have been reported to exhibit hypermobility in foot joints such as Chopart’s and Lisfranc’s joints. 4 In other words, dancers need to actively contract the muscles located in the foot to form a stable foot arch structure during tiptoe standing. Therefore, dancers who routinely perform tiptoe standing are likely to have hypertrophied/larger foot muscles compared to non-dancers.
The plantar intrinsic foot muscles (PIFMs) are a group of muscles that originate and insert within the foot, and have the function to stabilize or cause movements of the foot joints. 7 Electromyographic studies have revealed that among the muscles comprising the PIFMs, the abductor hallucis and flexor digitorum brevis contribute to elevating or reducing collapse of the medial longitudinal arch.10,11 Exercises targeting the PIFMs have also been shown to improve foot posture, as well as muscle and sensory functions related to postural control. 12 A recent study reported that during the push-off phase of gait (a limb position similar to demi-pointe), the abductor hallucis and flexor digitorum brevis stabilize the foot arch structure by increasing the metatarsophalangeal (MTP) joint stiffness and plantar fascia tension. 13 In addition, the abductor hallucis and flexor hallucis brevis activities increase markedly as postural demands or foot loading increase, from bipedal standing (ie, heels on the floor) to bipedal tiptoe standing, and to single-leg tiptoe standing. 8 Based on these findings, some of individual PIFMs, involved in tiptoe standing performed by dancers, may show signs of hypertrophy.
To our knowledge, only 1 study has attempted to quantify the size of individual PIFMs in dancers. That study showed that the sizes of all 3 measured individual PIFMs (abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis) were significantly larger in dancers than in non-dancers. 14 However, the authors evaluated the size of only 3 individual PIFMs mentioned above, which can be imaged from the plantar surface using ultrasonography. The size of the other individual PIFMs, including the non-superficial muscles, in dancers has not been determined.
The purpose of this study was to determine the differences in the sizes of 10 individual PIFMs between dancers and non-dancers. To this end, muscle volume (MV) was assessed using magnetic resonance imaging (MRI), the gold standard for measuring muscle size.15 -17 We hypothesized that all individual PIFMs, both superficial and non-superficial ones, would be larger in dancers than in non-dancers.
Methods
Participants
The study cohort was composed of 15 female dancers and 15 female non-dancers. Participants were recruited through convenience sampling until the sample size reached 15 participants in each group. The inclusion criteria for dancers were that they had at least 15 years of ballet training experience and at least 7.5 hours of ballet training per week. The inclusion criteria for non-dancers were that they were healthy but had no ballet training experience and had not participated in a regular physical training program for at least 6 months. None of the participants in both groups had a history of ankle or foot injury in the previous 3 months or any surgery in the previous year before participation. All participants were fully informed of the purpose and risks of the experiment and provided written informed consent.
Experimental Procedure
This study first collected information on the participants’ age, ballet experience and frequency, and history of injury through questionnaires, then measured their height and body mass, and calculated their body mass index (BMI). Finally, MRI scans were taken to obtain images of the foot.
Muscle Volume
Participants were positioned on the table of a 3.0 T MR system (Magnetom Skyra, Siemens Healthcare) with the right foot and ankle immobilized in an ankle coil (Foot/Ankle coil, Siemens Healthcare). The ankle joint was held in the neutral position with Velcro straps to reduce motion artifacts. Serial images of the whole foot were acquired from the sesamoids and calcaneal tuberosities of the foot, perpendicular to the plantar aspect of the foot, using a fast spin-echo sequence (repetition time = 700 ms, echo time = 12 ms, slice thickness = 3.5 mm, gap between slices = 0 mm, field of view = 125 × 125 mm, flip angle = 120°, matrix = 1024 × 1024). 18
Using image analysis software (SliceOmatic version 5.0Rev-3b, Tomovision), 1 examiner (H.F.) manually traced (color-coded) and segmented the anatomical cross-sectional area of each of the 10 PIFMs in separate images from the most proximal to the most distal image in which the muscles were visible (Figure 1). The muscles measured were the abductor hallucis, flexor digitorum brevis, abductor digiti minimi, quadratus plantae, lumbricals, flexor hallucis brevis, adductor hallucis oblique head, adductor hallucis transverse head, flexor digiti minimi, plantar/dorsal interossei. As a measure of muscle size, the anatomical cross-sectional area of each analyzed muscle was summed and multiplied by the slice thickness to calculate the MVs of the individual 10 PIFMs and the sum of them as a whole (WHOLE). The lumbricals and plantar/dorsal interossei were not separated within these muscles because their muscle boundaries were unclear. A total of 4 muscle groups for the lumbricals and 7 muscle groups for the plantar/dorsal interossei were segmented as 1 muscle group for these muscles. The inter-rater reproducibility of MV measurement for 3 participants in this study was evaluated by intraclass correlation coefficient (ICC).18,19 The ICC (1, 3) values for individual muscles were between 0.954 and 0.994, confirming excellent reproducibility. In addition to absolute MVs, relative MVs normalized to body mass (rMVBM) and the percentage of individual MVs relative to WHOLE MV (%MVWHOLE) were calculated. The outcomes were evaluated based on these three measures (ie, absolute MV, rMVBM, and %MVWHOLE).
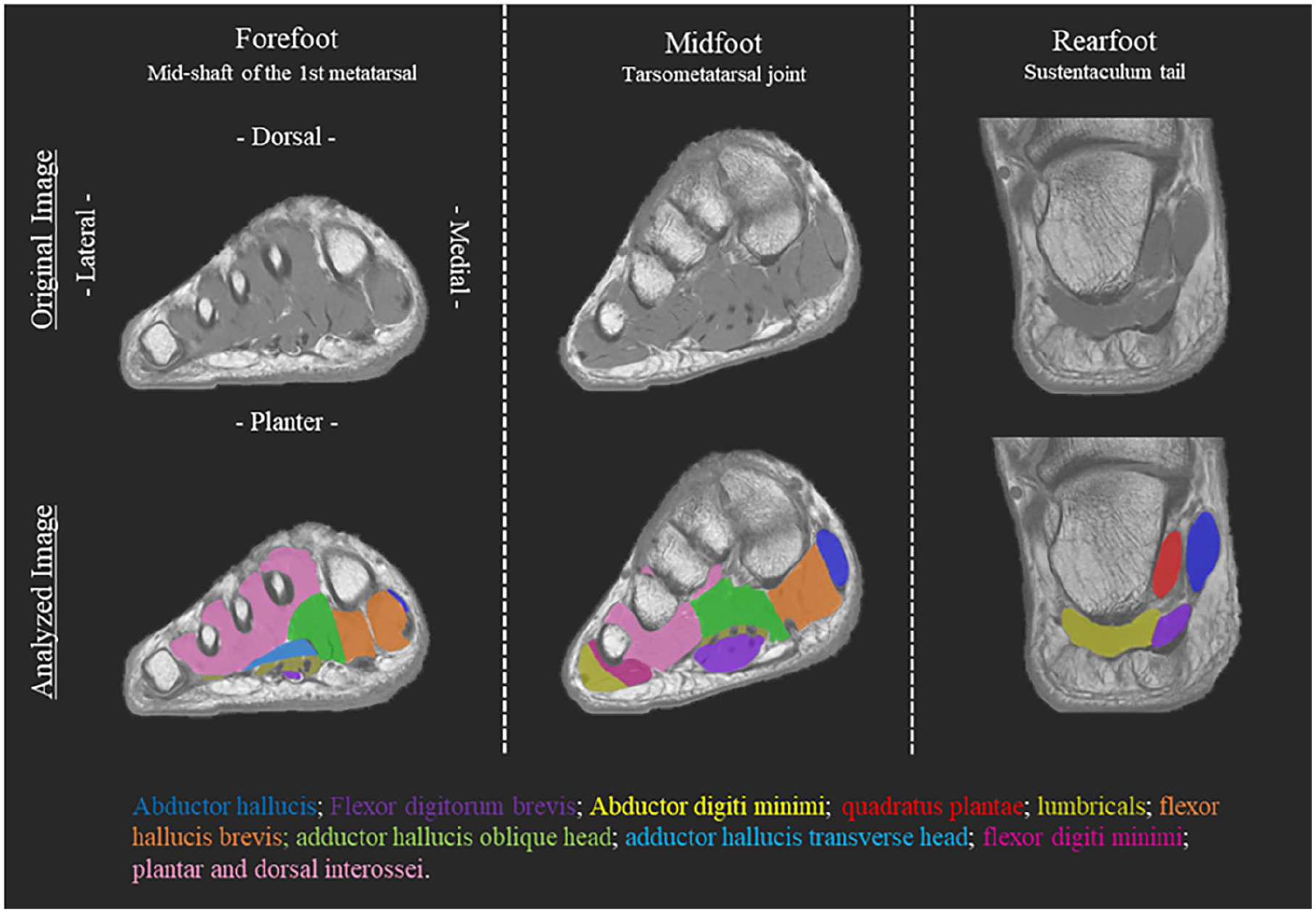
MRI image of the right leg. The top is the original and the bottom is the analyzed image. The images obtained at the level of the mid-shaft of the first metatarsal for the forefoot, the tarsometatarsal (Lisfranc’s) joint for the midfoot, and Sustentaculum tail for the rearfoot.
Statistical Analysis
Normality of the variables was assessed by the Shapiro-Wilk test. All variables except for the rMVBM of the adductor hallucis transverse head in dancers, the absolute MVs of the plantar/dorsal interossei and WHOLE and %MVWHOLE of the flexor hallucis brevis in non-dancers exhibited a normal distribution. Comparisons between groups for variables with skewed distribution were done using the Mann-Whitney U test, and for the normally distributed variables an independent samples t-test was used. All data were analyzed using SPSS software (SPSS statistics 28, IBM, USA). The significance level was set at P < .05. Effect sizes of between-group differences were calculated as Cohen’s d values and were interpreted as trivial <0.2; small 0.2 to 0.49; moderate 0.5 to 0.79; and large ≥0.8. 20
Results
Dancers had 21.4 ± 2.6 years of ballet experience and trained 19.9 ± 4.5 hours per week. There were no significant differences in age and height between dancers and non-dancers (Table 1). Body mass and BMI were significantly lower in dancers than non-dancers (P < .001, d = 1.71–2.25 [large], Table 1).
Participants’ Physical Characteristics.
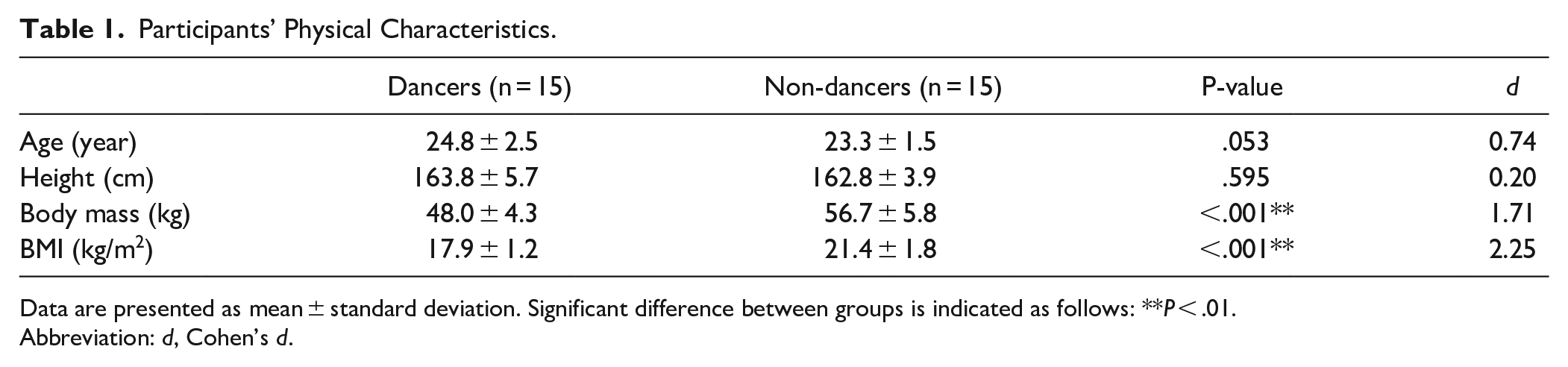
Data are presented as mean ± standard deviation. Significant difference between groups is indicated as follows: **P < .01.
Abbreviation: d, Cohen’s d.
Figure 2 summarizes the data for 3 measures of absolute MV, rMVBM, and %MVWHOLE (see Supplemental Table 1 for details). The absolute MVs of 6 individual PIFMs and WHOLE were significantly larger in dancers than in non-dancers (P ≤ .048, d = 0.76–2.38 [moderate-large], Figure 2A). The rMVBM of all 10 individual PIFMs and WHOLE were significantly larger in dancers than in non-dancers (P ≤ .019, d = 1.01–3.16 [large], Figure 2B). The %MVWHOLE of the flexor digitorum brevis and lumbricals were significantly higher and those of the abductor digiti minimi and adductor hallucis oblique head were significantly lower in dancers than in non-dancers (P ≤ .037, d = 0.82–1.68 [large], Figure 2C).
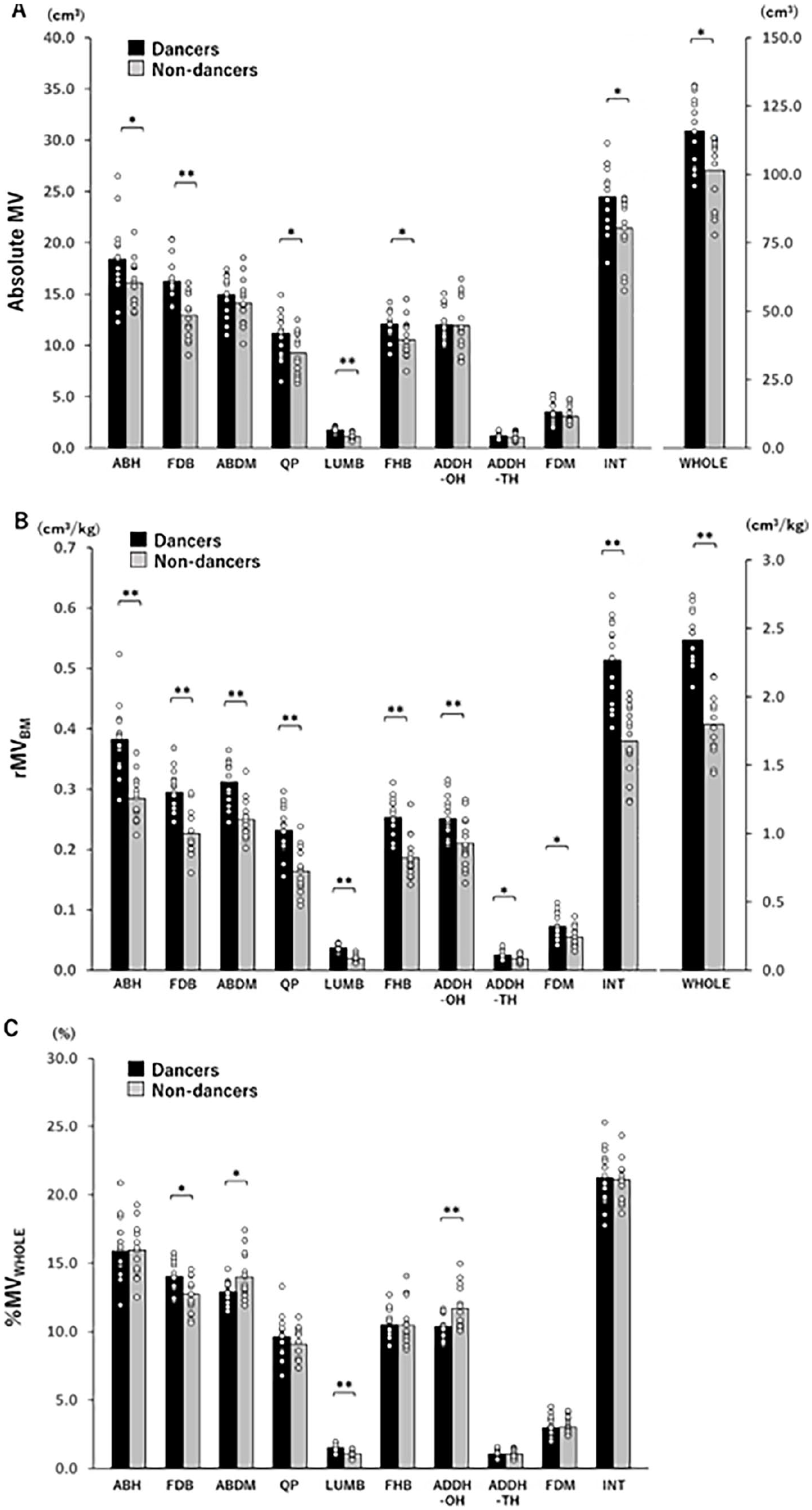
(A) Absolute MV. (B) Relative MVs normalized to body mass (rMVBM). (C) Percentages of individual MVs relative to WHOLE MV (%MVWHOLE) in dancers and non-dancers. Significant differences between groups are indicated as follows: *P < .05, **P < .01.
Discussion
This is the first study to use MRI to examine the differences in the sizes of 10 individual PIFMs between dancers and non-dancers. The main finding here was that only the flexor digitorum brevis and lumbricals were consistently larger, along with large effect sizes (Cohen’s d = 0.95–3.16), in dancers than in non-dancers on all 3 MV measures (ie, absolute MV, rMVBM, and %MVWHOLE). These findings did not support our hypothesis that all 10 individual PIFMs, including superficial and non-superficial ones, are larger in dancers than in non-dancers. The results instead suggest that among individual PIFMs, the flexor digitorum brevis and lumbricals play a specifically important role during ballet training involving tiptoe standing.
A common functional movement for the flexor digitorum brevis and lumbricals is the flexion of the second to fifth toes (hereafter referred to as “the lesser toes”) at the MTP joints. 21 In tiptoe standing, the second metatarsal functions as the long axis of the foot and the fifth and/or fourth metatarsal heads do not touch the floor as the ankle plantarflexion angle increases. 22 This suggests that in this limb position with a narrower ground contact surface than the normal standing position with the heels on the floor, the long axis joints (ie, the second ray) must be more reliably aligned to support the load and stabilize the posture. In such a case, theoretically, a greater load would be applied to the second ray, 6 which could be why the flexor digitorum brevis and lumbricals were larger in dancers than in non-dancers. However, it should be remarked that there are differences between the flexor digitorum brevis and lumbricals in terms of the layers located within the foot, the origin and insertion and other factors, as well as a considerable difference in muscle size, 21 as observed in the present study (Figure 2).
The flexor digitorum brevis, located in the first layer (ie, the most superficial layer), originates from the medial process of the calcaneal tuberosity and the plantar fascia, and inserts into the middle phalanx of the lesser toes. 21 An electromyographic study has shown that in movements such as tiptoe standing, the flexor digitorum brevis stabilizes the lesser toes against the floor and maintains the foot arch structure by regulating the plantar fascia tension. 13 In addition, the size of the flexor digitorum brevis is positively associated with the height of the transverse arch. 23 Recent evidence suggests that the transverse arch is responsible for over 40% of the longitudinal stiffness of the foot. 24 Dancers, especially those who perform with special shoes called pointe shoes (also known as toe shoes), often suffer fatigue fractures at the base of the second metatarsal bone (ie, the keystone of the transverse arch).6,25 This is because pointe shoes with rigid arch supports and toe covers allow for tiptoe standing with the MTP joint in a neutral or slightly flexed limb position, while placing excessive stress on that region. 6 These points would explain why the flexor digitorum brevis is larger in dancers than in non-dancers, suggesting that this muscle plays a major role in the load placed on the foot during ballet training involving tiptoe standing.
The lumbricals, located in the second layer, originate from the flexor digitorum longus tendon, and insert into the extensor apparatus of the lesser toes. 21 The lumbricals do not generate a large torque due to their small size. 18 However, the lumbricals have a specific function in extending the interphalangeal joints of the lesser toes and, in addition, coordinate the activities of the flexor and extensor muscles because of their mobility at both their origin and insertion.21,26 Previous research suggests that the atrophy of the lumbricals is associated with deformity of the lesser toes (ie, buckling of the proximal and/or distal IP joints of the second to fifth toes).26,27 When tiptoe standing with pointe shoes, dancers arch the entire plantar foot, along with the toes, in line with the sole of the shoe (ie, ideally, without buckling of the interphalangeal joint); in fact, dancers repeatedly perform these fine movements of the toes just like the specific function of the lumbricals.28,29 Considering these aspects, the current result that the lumbricals were larger in dancers than in non-dancers may be attributable to the fact that this muscle group functions especially during ballet training involving tiptoe standing with pointe shoes.
Interestingly, %MVWHOLE of the abductor digiti minimi and adductor hallucis oblique head were lower in dancers than in non-dancers. This finding could be explained by the following possibilities. Firstly, the abductor digiti minimi and adductor hallucis oblique head primarily cause the adduction/abduction of the toes, and secondly, these muscles function on rays other than the second (abductor digiti minimi: the MTP joint abduction of the fifth toe, adductor hallucis oblique head: the MTP joint adduction of the great toe). 21 Thus, it is possible that the abductor digiti minimi and adductor hallucis oblique head are not loaded much during ballet movements, and do not primarily generate torque to counteract the vertical load in the second ray, which is most loaded during tiptoe standing. It should be noted, however, that the current results on %MVWHOLE of the abductor digiti minimi and adductor hallucis oblique head do not imply that the 2 muscles are atrophied in dancers. This is because for both muscles, absolute MV was similar between groups (Figure 2A), and rMVBM was significantly larger in dancers than in non-dancers (Figure 2B).
The rMVBM values of all 10 PIFMs were larger in dancers than in non-dancers. Given the significant differences in body mass between dancers and non-dancers, these results may be unsurprising (Table 1). Also, the absolute MVs showed that 3 individual PIFMs (abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis) examined in a previous study that used ultrasonography to examine the absolute anatomical cross-sectional area of these muscles, 14 plus 3 individual PIFMs (quadratus plantae, lumbricals, plantar/dorsal interossei), were larger in dancers than in non-dancers. Given dancers’ experience and frequency of ballet training and the characteristics of the shoes they wear, these results make sense. Dancers wear ballet shoes with little or no arch support as well as pointe shoes during ballet training to allow for functional foot movements such as tiptoe standing. Running training in minimalist shoes with minimal arch support has been shown to cause hypertrophic adaptation of the PIFMs. 30 On the other hand, the absolute MVs of 4 individual PIFMs (abductor digiti minimi, adductor hallucis oblique head, adductor hallucis transverse head, and flexor digiti minimi) were not significantly different between dancers and non-dancers. However, similar to the %MVWHOLE results discussed above, these muscles either primarily cause the adduction/abduction of the toes and/or function on rays other than the second. Thus, these findings in this study may suggest that the PIFMs do not necessarily function as a single unit, but rather that individual muscles function according to their own requirements in dancers.
Limitations
This study has some limitations. This was a cross-sectional study, and we did not strictly adjust for frequency, duration, or load of dancers’ training. Also, variables such as performance level might influence the muscle size in specific muscles. Furthermore, foot deformities such as flat feet and hallux valgus might affect the variables analyzed in this study. Further work is needed to examine the relationship between the above variables and the functional roles of individual muscles, including measurements during weight bearing or functional limb positions (eg, single-leg standing and tiptoe standing).31,32
Conclusions
The current study suggests that among 10 individual PIFMs, the flexor digitorum brevis and lumbricals, which primarily cause the MTP joint flexion of the second to fifth toes, were consistently larger in dancers than in non-dancers. These findings could be attributable to long-term repetitive loading on the corresponding individual PIFMs during ballet training involving tiptoe standing.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X241273887 – Supplemental material for Differences in the Size of Individual Plantar Intrinsic Foot Muscles Between Ballet Dancers and Non-Dancers
Supplemental material, sj-docx-1-dmj-10.1177_1089313X241273887 for Differences in the Size of Individual Plantar Intrinsic Foot Muscles Between Ballet Dancers and Non-Dancers by Hiroshi Fukuyama, Sumiaki Maeo, Yuki Kusagawa, Takashi Sugiyama, Hiroaki Kanehisa and Tadao Isaka in Journal of Dance Medicine & Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.