
Abstract
Introduction:
Ankle sprains are among the most common injuries in dancers. Following one or more severe sprains, some individuals will experience residual mechanical and functional deficits, otherwise known as chronic ankle instability (CAI). Dancers who suffer from CAI may have weaker musculature surrounding the ankle and altered landing mechanics. The purpose of this study was to compare ankle strength and saut de chat landing mechanics between dancers with and without CAI.
Methods:
Dancers with and without CAI, defined by the Identification of Functional Ankle Instability (IdFAI), participated in the study (CAI n = 8; IdFAI = 18.75 ± 5.50 points; age = 20 ± 1.5 years; training = 15.5 ± 3.5 years) (Control n = 8; IdFAI = 7.13 ± 3.40 points; age = 19 ± 0.6 years; training = 15.9 ± 2.5 years). Strength and leap landing mechanics were measured on the affected ankle for the CAI group and on the preferred landing leg of a leap for the control group. Concentric and eccentric ankle plantar flexion, and subtalar inversion and eversion strength were determined with dynamometry set at an angular velocity of 60°•s−1. Force plates and motion capture cameras were used to calculate lower extremity kinematic and kinetic data as participants performed 3 saut de chat leaps. Independent t-tests were calculated to determine differences between groups.
Results:
Compared to dancers without CAI, dancers with CAI had lower eccentric plantar flexor strength, landed with higher vertical ground reaction forces, and absorbed greater power at the knee-joint during landing.
Conclusion:
Whether dancers who are weaker are more prone to injury or ankle-joint injury leads to muscular weakness is unknown. Dancers with CAI appear to lack control during leap landing while concomitantly shifting loads proximally away from the ankle-joint. We encourage dancers with and without CAI to engage in additional training that enhances ankle strength.
Key Points
Dancers with chronic ankle instability display weaker eccentric plantar flexors than controls.
Dancers with chronic ankle instability exhibit higher peak vertical ground reaction forces than controls during saut de chat landing.
Dancers with chronic ankle instability absorb significantly more power at the knee-joint during saut de chat landing than controls.
Introduction
The incidence of injury among professional female modern and ballet dancers ranges from 0.59 to 3.9 times per 1000 hours of training.1,2 In collegiate dancers, the incidence of injury is 3.7 times per 1000 hours of training. 3 Ankle and foot are the most common sites of injury, 4 with a prevalence of 62% in ballet dancers. 5 Most ankle injuries occur during jumping activities that result in damage to the lateral ligaments, typically through excessive ankle plantar flexion and subtalar inversion.4,6 Approximately 76% of dancers who have experienced a lateral ankle sprain suffer from chronic ankle instability (CAI). 6 CAI is characterized by residual functional and mechanical deficits following a severe subtalar inversion ankle sprain. 7 Comparison of performance characteristic discrepancies between dancers with CAI and dancers without CAI have yet to be clarified.
Compared to untrained individuals, dancers possess significantly greater concentric plantar flexor strength.8,9 Strength in dancers has shown to both enhance performance and mitigate injury.10 -12 Huang et al 11 found that dancers who engaged in additional resistance exercise outside of dance training were 61% less likely to sustain an injury. Upon sustaining an ankle injury, and for that matter a repeated injury, it may be that the surrounding musculature is or becomes weaker. 13 Although the relationship between strength and CAI is uncertain, 14 stronger dancers appear less prone to injury. 15 Specific to assessing dynamic ankle stability, concentric and eccentric subtalar inversion and eversion strength may be of interest to measure in dancers, 16 in addition to plantar flexion concentric and eccentric strength. 8 By evaluating multi-planar strength in dancers with and without CAI, we might gain insight into aspects of strength that can be improved for prevention of ankle re-injury.
In addition to muscular weakness, altered landing biomechanics would be expected in dancers with CAI. 17 While ascertaining the loads of hopping or jumping mechanics can be useful, ballet jumps and leaps provide more robust data regarding dance-specific demands due to the upright nature of performance. Dance-specific landings typically impose vertical ground reaction forces (vGRF) ranging between 1.4 and 9.6 × BW and loading rates ranging between 11.0 and 222.7 BW•s−1. 18 When examining saut de chat landings exclusively, healthy dancers typically experience vGRF of 3.2 to 4.4 × BW.19,20 It is unknown how ankle pathologies influence saut de chat landing vGRF and loading rate, however, patellofemoral pain and tendinopathy appear to result in higher vGRF during échappé and saut de chat landings.19,21 Some findings suggest that, in short, individuals with CAI land faster and harder, essentially adopting a stiffer landing style. 17 Other data indicate that a softer landing style is adopted to reduce vGRF. 17 The latter is true for dancers who’ve sustained a lateral ankle sprain landing from a sissonne fermée, 22 which might serve as a protective mechanism against re-injury. In understanding the magnitude and rate of forces during leap landing, we can speculate how CAI might influence movement patterns.
Investigating not only vGRF, but also lower extremity joint-load distribution might help to clarify the effect of CAI on landing strategy. Dancers rely considerably on the ankle-joint complex for both saut de chat take-off propulsion and landing absorption.12,23 Previous researchers have observed a propensity to shift load absorption proximally away from the ankle-joint in individuals with CAI. 24 One way this is achieved is by landing with greater dorsiflexion to employ a more “tightly packed” ankle. 25 Subsequently, individuals are less prone to frontally invert the foot with this strategy as well. However, this would in turn place higher loads on the hip- and knee-joints. As mentioned, dancers are trained to land with a “pointed” foot with angles nearing 50° of plantar flexion. 20 Modifying the angle of the foot to be less vulnerable to subtalar inversion would flaw esthetics, which are an integral component of performance. Thus, it is plausible that dancers with CAI may still absorb higher power at the ankle because of esthetics, which would explain the higher prevalence and cyclic nature of ankle re-injury in dancers.
The purpose of this study was to determine the effect of CAI on muscle strength and saut de chat leap (Figure 1) landing biomechanics in dancers. We sought to compare isokinetic plantar flexion, inversion, and eversion strength in addition to saut de chat landing mechanics in dancers who do and do not possess chronic ankle instability. We hypothesized that dancers with CAI would be weaker overall, and would exhibit higher leap landing vGRF, loading rates, and sagittal- and frontal-plane ankle powers than non-CAI dancers. Furthermore, we suspected that ankle inversion would be greater at initial contact in the CAI group than controls. Such information might help to expound the potential effects of repeated overloading, compensation strategies, or neuromuscular deficits due to CAI.

Example of a dancer performing a saut de chat leap.
Methods
Study Design
We sought to elucidate whether differences exist in ankle strength and leaping mechanics between a convenience sample of dancers with and without CAI. The Institutional Review Board of Wake Forest University approved this protocol (IRB00024462). Participants provided written informed consent.
Participants
Females between the ages of 18 and 25 years with at least 10 years of training in ballet, pointe, jazz, modern, or contemporary and currently training were recruited. Dancers were included if they were currently training at least twice a week. Dancers were excluded if they had a neuromuscular disease, sustained musculoskeletal or lower limb injury within the past 3 months, or a history of lower extremity fracture or surgery. After providing informed consent, participants filled out an Identification of Functional Ankle Instability (IdFAI) questionnaire, 26 the results of which determined group assignment, CAI or control. IdFAI consists of 3 factors: the first factor focuses on the history of ankle sprain, the second factor focuses on the initial ankle sprain, and the third factor focuses on the instability during activities of daily living. A total score of 10 or lower indicates that the participant is unlikely to have CAI, whereas a total score of 11 or higher indicates that a participant is likely to have CAI. Dancers in the CAI group had a history of at least 1 significant ankle sprain occurring at least 12 months prior to study enrollment with their most recent ankle sprain occurring at least 3 months prior to study enrollment (IdFAI > 10). Dancers in the control group scored ≤10 on the IdFAI.
Procedures
After participants completed the IdFAI, they also completed a Dance History questionnaire. Body mass and height were then measured using standard techniques. Strength and leaping mechanics were measured on the most affected ankle (ie, scored higher on the IdFAI) for the CAI group and on the preferred landing leg of a saut de chat for the control group.
Strength measures were obtained using a HUMAC NORM isokinetic dynamometer (CSMi, Massachusetts, USA). Dancers laid prone with the hips and knees fully extended and the testing foot and ankle strapped tightly in the pedal and secured with tape to ensure no heel lift occurred for plantar flexion strength testing. 8 The ankle range of motion was set to −10° of dorsiflexion to 30° of plantar flexion. Participants performed 3 warm-up concentric and eccentric plantar flexion contractions at 60°•s−1 with 50%, 75%, 90%, and 100% effort each separated by 30 seconds. After 1 minute of rest, participants performed 3 maximal effort trials of concentric and eccentric plantar flexion contractions at 60°•s−1. For inversion and eversion strength testing, dancers sat upright in the chair with the hips at 70° of flexion and the testing leg knee at 75° of flexion. Inversion-eversion range of motion was set to 10° of inversion to −20° of eversion. Participants completed 5 total concentric and eccentric inversion and eversion trials at 60°•s−1 with 100% effort: 2 familiarization trials and 3 trials for subsequent analysis. Participants were instructed to contract as fast and as hard as possible. Each trial was separated by 1 minute of rest.
Dancers warmed up and stretched prior to performing saut de chat leaps. Reflective markers were placed on L5/S1, and on the right and left iliac crest, anterior superior iliac spine, posterior superior iliac spine, greater trochanter, thigh (clusters of 3), lateral and medial femoral condyle, shank (clusters of 3), lateral and medial malleoli, the Achilles tendon in alignment with the malleoli, the posterior heel in alignment with the Achilles tendon, the calcaneus in alignment with the lateral malleoli, first and fifth metatarsophalangeal joints, on the dorsal side of the foot between the metatarsophalangeal joint markers, and on the anterior tip of the first metatarsal for static calibration. The foot model is shown in Figure 2.
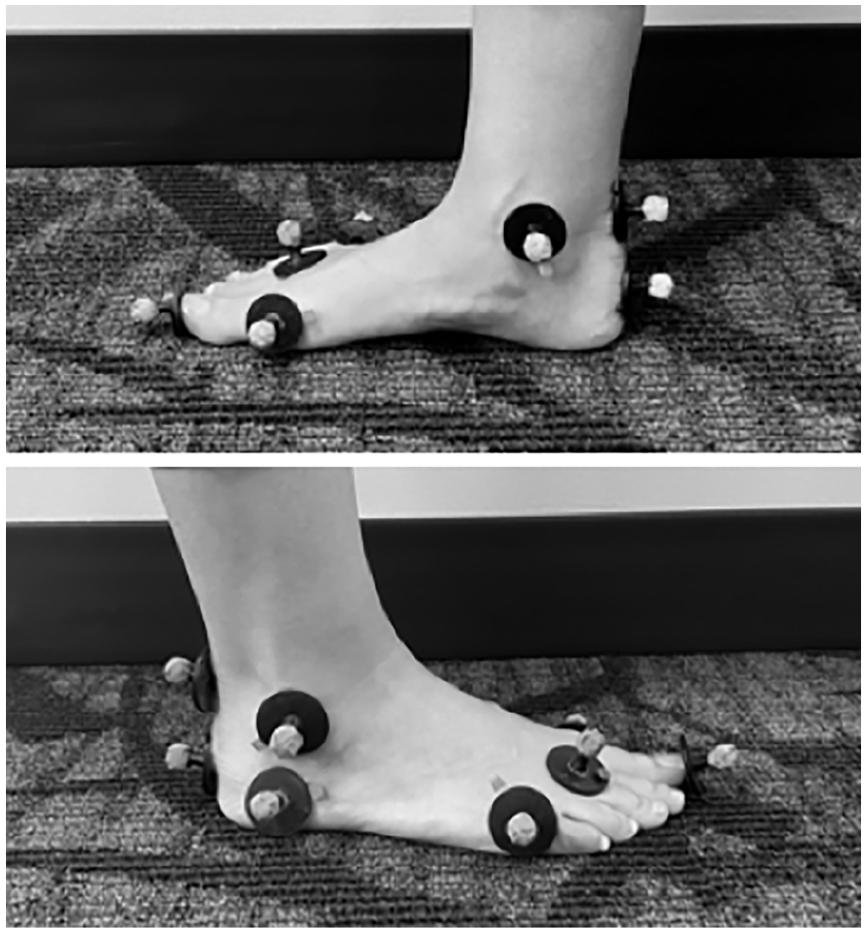
The foot model used for static calibration.
The right and left iliac crest, greater trochanter, medial femoral condyle, medial malleoli, and anterior tip of the first metatarsal were moved for leaping trials. An 8-camera 3-dimensional motion capture system (Raptor, Motion Analysis Corporation, Santa Rosa, CA, 200 Hz sampling rate) and 4-, 6-channel force plates (2 BMS464508-2K-FP2 and two OR6-7-2000, Advanced Mechanical Technology, Inc., Watertown, MA, 1000 Hz sampling rate) were used to capture motion and force during the leaps. The motion analysis system and force plates were calibrated prior to data acquisition. Participants performed 3 separate leaps to a metronome set at 106 beats per minute with arms in third position. Participants were instructed to take two steps prior to taking off and to land on the most affected leg on which strength was measured (Figure 1). 10 Participants were instructed to leap as high as possible.
The strength data was exported and analyzed in a custom-designed LabVIEW program (Version 19.0, National Instruments, Austin, TX). The outcome variables included relative concentric and eccentric plantar flexion, inversion, and eversion peak torque. Peak torque values were normalized to body mass. The 3 trials from each contraction type were then averaged per participant and used for further statistical analysis. From leaping measures, raw coordinate data were processed in Cortex to refine marker labeling and fill gaps in the marker collection. The refined coordinate data and raw force were imported into Visual 3D v5.01.10 (C-Motion, Germantown, MD) for additional processing to determine biomechanical kinetic and kinematic parameters. In Visual 3D, the coordinate and force data were filtered at 12 and 50 Hz respectively using a Butterworth low-pass digital filter. A 20 N threshold was applied to the force data. 23 Joint angles were determined from coordinate data, and inverse dynamics analysis was performed to determine internal moments, joint reaction forces, and joint powers. Outcome variables included saut de chat landing peak vertical ground reaction force (vGRF), peak loading rate, peak sagittal hip-, knee-, and ankle-joint absorption powers, peak hip adduction and abduction absorption powers, peak ankle inversion and eversion absorption powers, and initial contact joint angles. Peak vGRF and loading rate were normalized to bodyweight while all peak powers were normalized to body mass. Loading rate was calculated from initial contact to peak vGRF in increments of 3 vGRF samples. The change in vGRF was divided by the change in time, and peak loading rate was determined from the highest slope calculated. Representative relative ankle-, knee-, and hip-joint powers are demonstrated in Figure 3 from initial contact to minimum center of mass height upon landing.
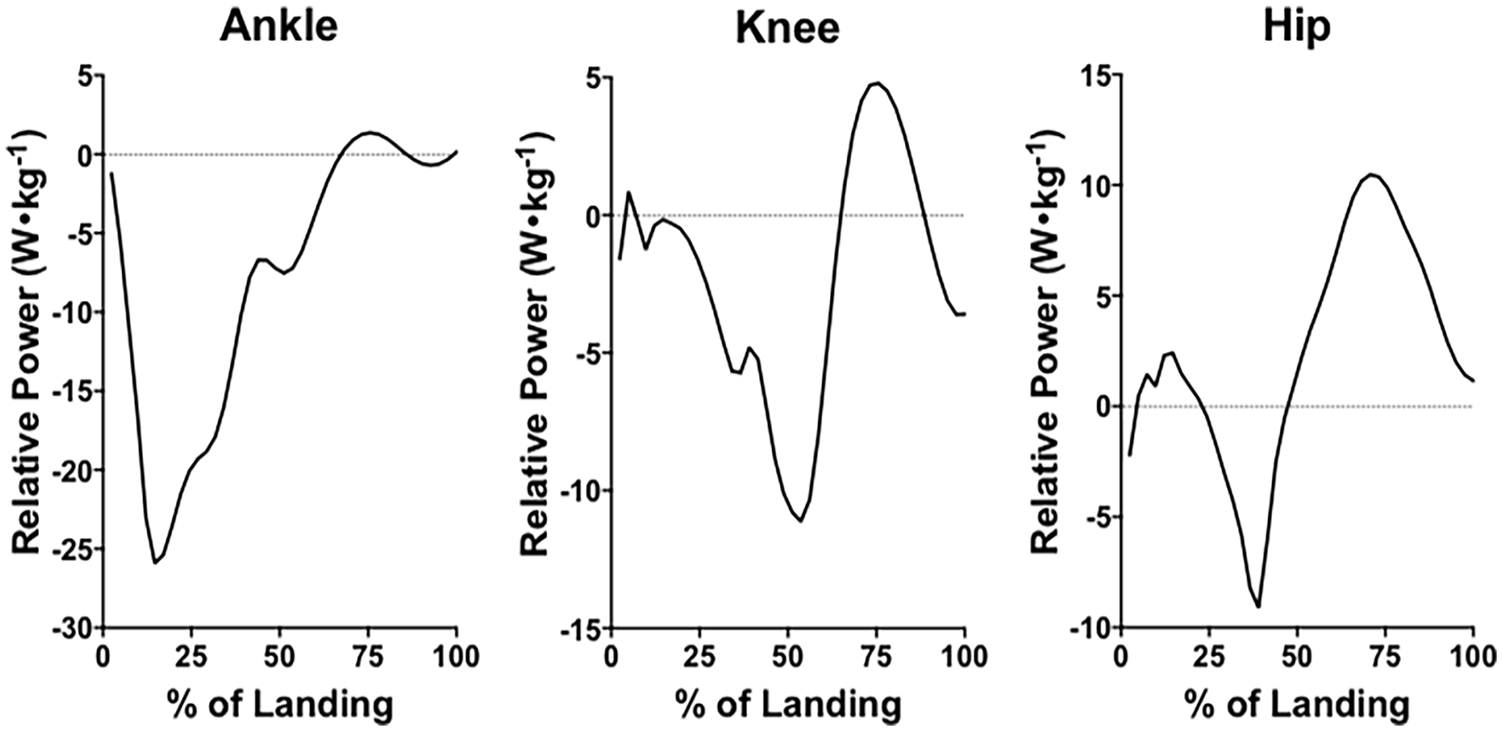
Representative data of joint powers during saut de chat leap landing.
Data Analyses
Outcome variables were analyzed in SPSS (version 28.0.0.0, SPSS Inc., Chicago, IL, USA) with the alpha level set at P ≤ .05. Independent t-tests between groups analyzed all relative peak torque strength values, vGRF, loading rates, and joint kinematic and kinetics during leaping. Levene’s Test for Equality of Variances was used to identify whether equal variance existed. Equal variance was met for all relative strength measures except eccentric inversion peak torque (P = .03). Unequal variance was also observed in peak vGRF and peak loading rate (P < .001 and P = .001, respectively) as well as knee flexion angle at initial contact (P = .009). Equal variance was met for all other saut de chat variables. A Bonferroni post-hoc test was calculated and applied to the following variable groupings: strength (P ≤ .008), center of mass forces (P ≤ .03), initial contact angles (P ≤ .01), frontal joint peak powers (P ≤ .01), and sagittal joint peak powers (P ≤ .02). Results were reported as means ± standard deviation (SD) in addition to mean differences (μd) and 95% confidence intervals. Effect sizes were calculated with Hedges’ g correction and interpreted as trivial (<0.25), small (0.25-0.50), moderate (0.5-1.0), and large (>1.0). 27
Results
Aside from IdFAI scores, descriptive characteristics and anthropometry did not significantly differ between the CAI group and the control group (Table 1).
Descriptive Characteristics of Dancers With and Without Chronic Ankle Instability (CAI).
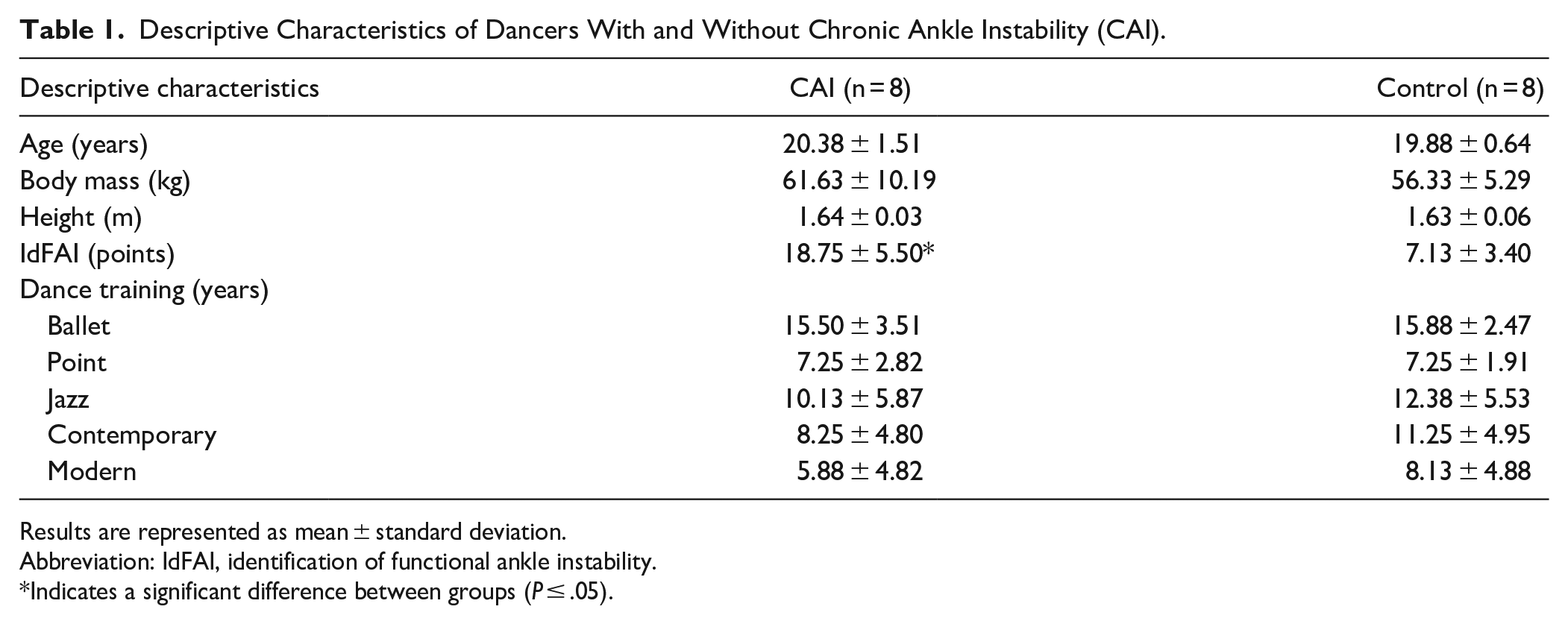
Results are represented as mean ± standard deviation.
Abbreviation: IdFAI, identification of functional ankle instability.
Indicates a significant difference between groups (P ≤ .05).
Relative eccentric plantar flexion peak torque was significantly lower (P = .008, μd = 0.62 ± 0.20 Nm•kg−1, 95% CI 0.19 to 1.05, g = 1.46) in the CAI group than the control group while no significant differences (P = .14, μd = 0.19 ± 0.12 Nm•kg−1, 95% CI −0.73 to 0.45, g = 0.73) existed between groups for relative concentric plantar flexion peak torque (Figure 4). There were no significant differences between groups in relative eccentric inversion peak torque (P = .57, μd = 0.04 ± 0.06 Nm•kg−1, 95% CI, −0.10 to 0.17, g = 0.28), relative concentric inversion peak torque (P = .43, μd = 0.03 ± 0.04 Nm•kg−1, 95% CI, −0.05 to 0.11, g = 0.39), relative eccentric eversion peak torque (P = .44, μd = 0.04 ± 0.05 Nm•kg−1, 95% CI, −0.06 to 0.13, g = 0.38), nor relative concentric eversion peak torque (P = .89, μd = 0.004 ± 0.03 Nm•kg−1, 95% CI, −0.05 to 0.06, g = 0.07) (Figure 4).
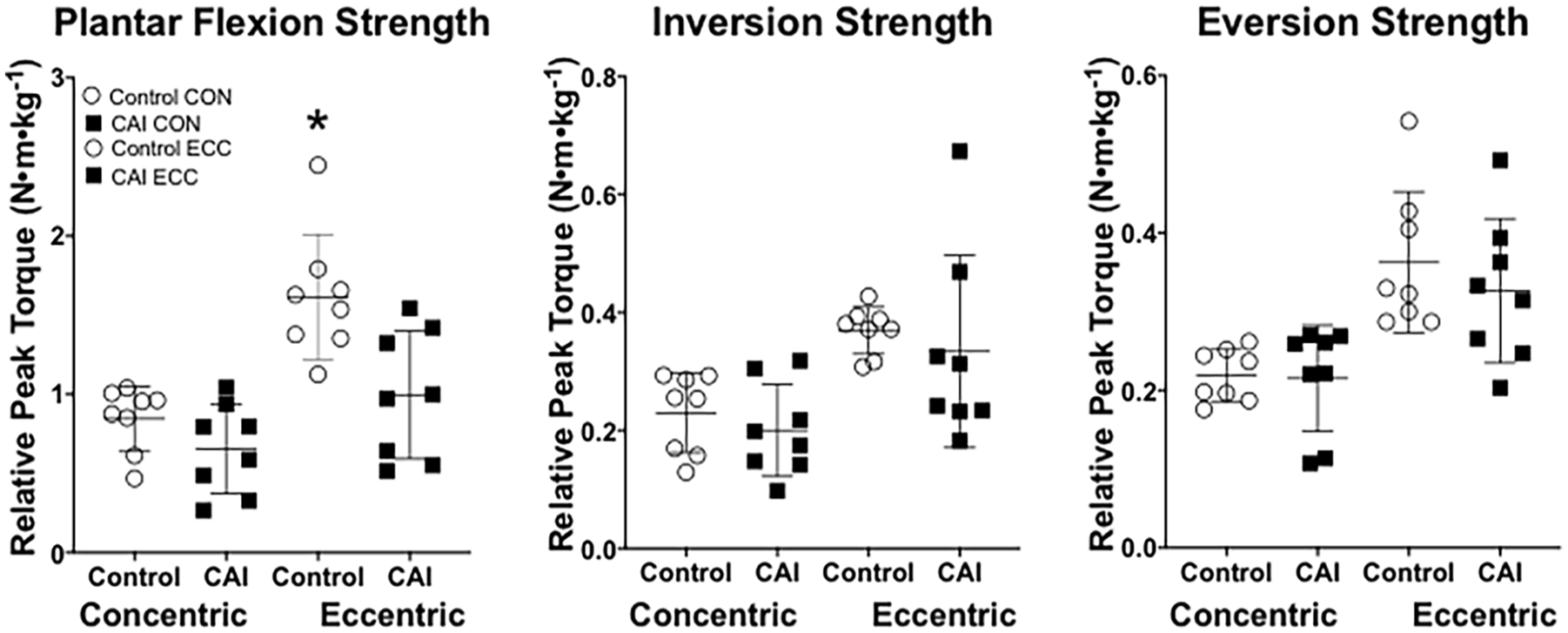
Concentric (CON) and eccentric (ECC) plantar flexion, inversion, and eversion isokinetic strength at 60°•s−1 in dancers with and without chronic ankle instability (CAI). *Indicates a significant difference between groups (P = .008).
The CAI group exhibited significantly higher peak vGRF than the control group (P = .02, μd = −0.88 ± 0.31 N•BW, 95% CI, −1.58 to 0.17, g = −1.37) (Figure 5). No significant differences existed between groups for peak loading rate (P = .06, μd = −122.25 ± 54.73 BW•s−1, 95% CI, −249.04 to 4.54, g = −1.06) (Figure 5).
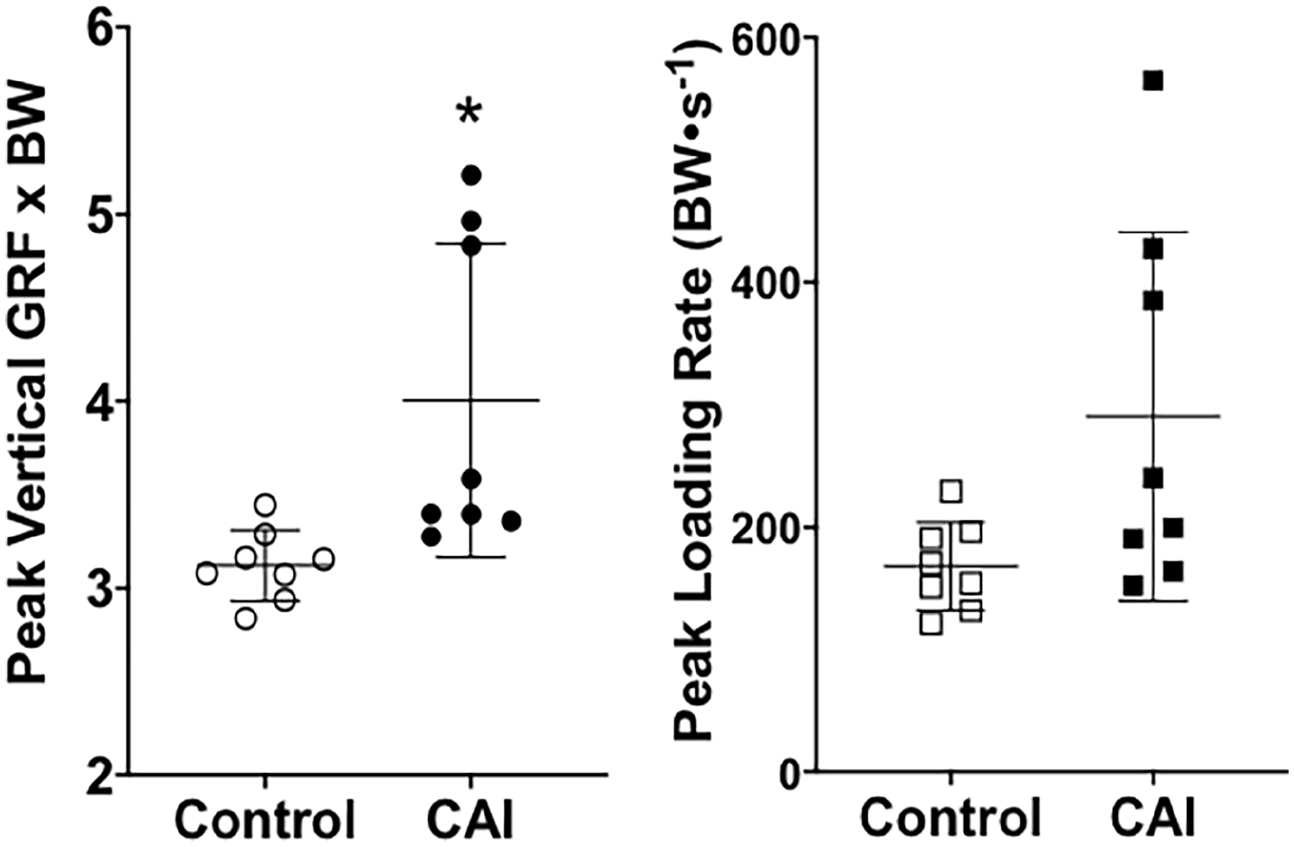
Peak vertical ground reaction forces (GRF) × bodyweight (BW) and peak loading rate during leap landing dancers with and without chronic ankle instability (CAI). Results are represented as mean ± standard deviation with individual data points. *Indicates a significant difference between groups (P = .02).
Relative sagittal knee peak power was significantly higher in the CAI group than controls (P = .02, μd = 8.55 ± 3.35 W•kg−1, 95% CI = 1.36 to 15.74, g = 1.21) (Figure 6). Neither relative sagittal ankle peak power nor relative sagittal hip peak power significantly differed between groups (P = .11, μd = −3.69 ± 2.18 W•kg−1, 95% CI = −8.36 to 0.98, g = −0.80; P = .09, μd = −10.35 ± 5.58 W•kg−1, 95% CI = −2.18 to 22.87, g = 0.88) (Figure 6). No significant differences existed between groups for relative frontal joint peak powers for the hip- and ankle-joint and sagittal and frontal joint angles upon initial contact of landing (Table 2).
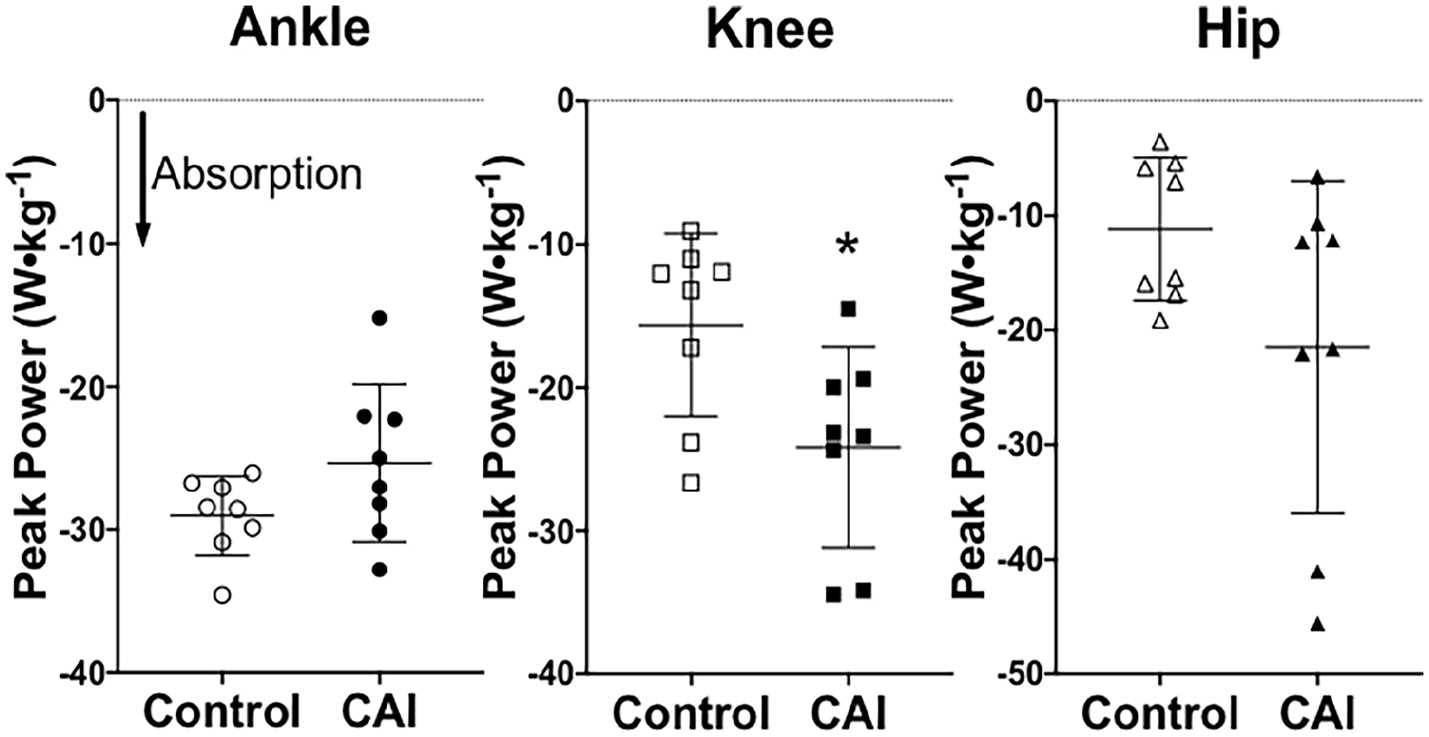
Peak absorption power during leap landing for the ankle-, knee-, and hip-joints in dancers with and without chronic ankle instability (CAI). Results are represented as mean ± standard deviation with individual data points. *Indicates a significant difference between groups (P = .02).
Initial contact joint angles and relative hip- and ankle-joint frontal plane peak powers upon leap landing in dancers with and without chronic ankle instability (CAI).
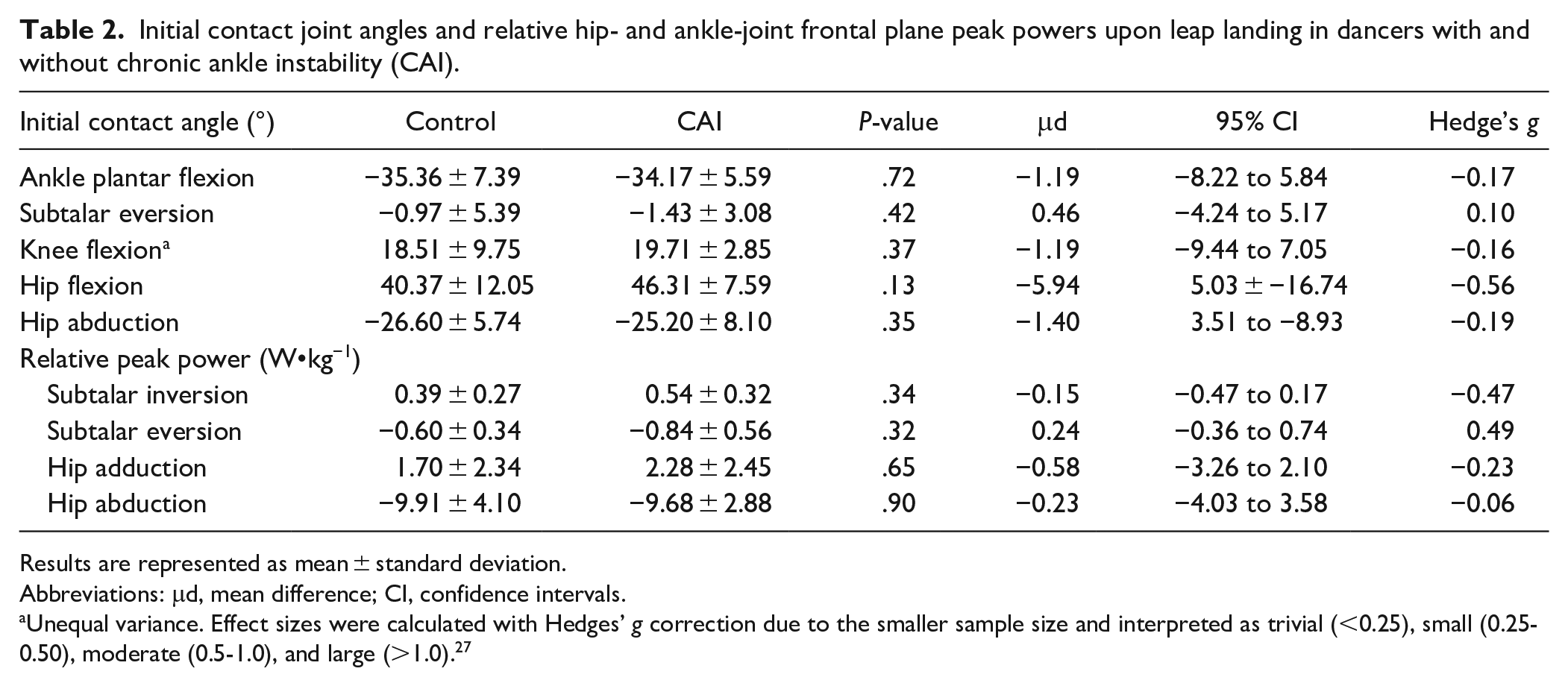
Results are represented as mean ± standard deviation.
Abbreviations: μd, mean difference; CI, confidence intervals.
Unequal variance. Effect sizes were calculated with Hedges’ g correction due to the smaller sample size and interpreted as trivial (<0.25), small (0.25-0.50), moderate (0.5-1.0), and large (>1.0). 27
Discussion
The main findings of the present work suggest that dancers with CAI display weaker ankle plantar flexors in eccentric actions, exhibit higher landing forces, and absorb more power at the knee joint during landing. Ankle strength is an integral part of dancers’ injury prevention and performance capabilities. Of particular importance for dancers is eccentric plantar flexion strength as they attempt a controlled landing from a jump or leap. High volumes of jump or leap landings can lead to injury, 1 which can be exacerbated by increased vGRF. With less controlled or improper mechanics and joint-loading distributions, the risk of injury will increase. 28 It is plausible that a potential connection exists between lower ankle strength and a power absorption shift to the knee in efforts to avoid ankle loading during leap landings in dancers with CAI. Thus, our results indicate how ankle injury history and strength profiles might translate into altered saut de chat leap landing strategies. While our findings provide insight into the ankle strength and saut de chat landing mechanics of dancers with CAI, next steps would be to design a strength intervention that addresses altered landing strategies after ankle injury.
Previous research has shown that multi-planar eccentric and concentric isokinetic strength varies widely in individual’s with CAI. 14 In this cohort of dancers, those that suffered from CAI possessed significantly lower isokinetic eccentric plantar flexion peak torque than healthy controls. There are 2 potential pathways that might explain the lower ankle strength in the CAI dancers: structural tissue damage from subtalar inversion sprains has encumbered force output capabilities or habitual loading away from the ankle has resulted in the adaptation of lower eccentric strength. We posit that proximal loading away from the ankle during landing may be responsible for weaker eccentric plantar flexors in dancers with CAI. Dynamic muscular strength adaptations occur from the load imposed on tissues. 29 Therefore, the higher power absorption at the knee might suggest that the ankle experiences less of a stimulus for maintained or increased eccentric plantar flexion strength in dancers with CAI. What is unknown is whether weaker dancers are more prone to ankle sprains or if ankle strength decreases ensuing an ankle sprain. Future longitudinal research might help to clarify this complex of whether weaker dancers are more likely to be injured or if weakness is a byproduct of injury. Although insignificant, dancers with CAI tended to be overall weaker than controls as hypothesized. It is plausible that the lower ankle strength was further observable in landing forces.
With significantly higher vertical ground reaction forces than controls, the requisite center of mass deceleration during saut de chat landing appears to be compromised in dancers with CAI. The average time from touchdown to minimum center of mass displacement during landing was approximately 160 ms. Such a temporal scale would theoretically allow for feedback loops to modify muscle forces and ultimately, reduce landing forces. We believe that these findings could be indicative of proprioceptive (cutaneous, joint, muscular) diminution due to previous injury. 30 In the classic work of Freeman et al, 31 they describe that subtalar ankle sprains might damage proprioceptors located in the ankle capsule and ligaments. Eventually, the lack of “activatable” mechanoreceptors will lead to further destabilization of the ankle complex if insufficient or inappropriate threshold motor units are recruited during an unexpected perturbation. Such notion is supported by data suggesting that dancers who possess the sensorimotor capacity to respond to dynamic environments might have a protective advantage against injury.32,33 Taken together, our findings might demonstrate the impaired sensorimotor control in dancers with CAI that is necessary for controlled leap landing. 32 Although the peak loading rate was not significantly higher in the dancers with CAI, a trend toward significance was observed (P = .06). We acknowledge that our results are likely confounded by the unequal variance and small sample size. With higher loading rates and significantly higher vGRF, dancers with CAI are more likely to sustain additional injury. 34 It is imperative that dancers engage in some type of re-injury preventative program.
Contrary to our hypothesis, ankle power was not significantly higher in the dancers with CAI than the controls. The observed compensatory power absorption at the knee-joint is likely a protective mechanism in dancers who’ve previously sprained their ankles. Since there were no significant differences between the groups for lower extremity initial contact angles, we cannot infer how this strategy was achieved kinematically. However, dancers’ intention not to “sickle,” or supinate the foot, could explain the lack of differences between groups in initial contact kinematics of the ankle. 35 For the hip- and knee-joint, we speculate whether leap height is compromised, which is a significant determinant of saut de chat performance. 10 It is critical to note that increased magnitude and rate of GRF’s in combination with higher knee-joint loading could subject dancers to injury or chronic pathologies at the knee as well. The dancers in this study trained ~8 hours per week, suggesting that this protocol would not induce fatigue. After a dance-specific fatigue protocol, peak knee extensor moments significantly increase during sauté jumping. 36 To further understand how individuals with CAI alter movement strategy, it may be beneficial for practitioners to understand how fatigue might exacerbate saut de chat landing forces and knee power absorption.
Limitations
The present study contained numerous limitations. Due to the limited number of dancers from which we recruited, the sample size posed as the greatest limitation. Because of this, 3 dancers with CAI appeared to differ from the rest of the CAI group (ie, vGRF of 5.00 ± 0.11 × BW vs 3.40 ± 0.19 × BW, respectively). With a larger sample size, we believe that some of the discrepancies would either further distinguish dancers with CAI that continue to operate mechanically similar to dancers without CAI from dancers with CAI who significantly alter landing mechanics or provide a more even distribution of data. Additionally, we hypothesized that inversion and eversion strength would be significantly lower in dancers with CAI than dancers without CAI, given the nature of lateral ankle sprains. However, we did not observe significant differences between groups for dynamic frontal plane ankle strength. One limitation of this movement is that anecdotally, dancers verbalized that maximal subtalar inversion and eversion strength assessments are not familiar assessments. It may be that a familiarization visit would help participants to become more comfortable with this type of strength testing. Overall, our study warrants further investigation into the strength and leap landing mechanics of dancers with and without CAI.
Practical and Clinical Applications and Implications
We encourage dance scientists and practitioners to implement training that would serve as preventative medicine to ankle re-injuries. 29 Upon ankle injury and development of chronic ankle instability, our findings suggest that dancers should consider focusing on eccentrically strengthening plantar flexors concurrently with proper landing mechanics during leaping. The importance of preventing repeated injury is evident based on a study by Smith et al 37 where they surveyed persisting conditions in retired professional ballet dancers. The most prominent finding was that 80% of the retired professional ballet dancers suffered from osteoarthritis. 37 Early signs of osteoarthritis are observable at the cervical and lumbar spine, hip, knee, ankle, and foot in professional dancers as young as 19 years old. 38 In the case of dancers, osteoarthritis likely arises from repetitive microtrauma that leads to formation of osteophytes, osteochondral lesions, cartilage alterations, and/or loss of joint space. 39 Ideally, developing additional training that is preventative would reduce CAI prevalence altogether. By prioritizing strength and power development and proper jumping and landing mechanics, dancers might evade not only career ending injuries, but also life-altering conditions.
Conclusion
The purpose of our study was to compare multi-planar eccentric and concentric strength along with saut de chat landing mechanics in dancers with and without CAI. The dancers with CAI possessed weaker eccentric plantar flexors, higher vertical ground reactions forces, and greater power absorption at the knee during saut de chat leap landing. Within the limitations of this study, it appears that CAI affects or is affected by ankle muscular strength and leaping mechanics. How chronic ankle instability manifests after a lateral ankle sprain in dancers remains unknown. Our findings warrant further investigation into the ways that mechanical and functional ankle instability manifest in eccentric strength and landing mechanics of dancers. Future work should examine the effect of strength training on saut de chat mechanics, and proprioception of the foot and ankle in dancers with and without CAI.
Footnotes
Acknowledgements
We would like to thank Gabriel Pate and Allie Williams for their help with data collection. We would also like to sincerely thank the dancers who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.