
Abstract
The objective of this study is to discuss the implementation, safety, and potential benefits of on-table extubation (OTE) in surgeries involving hypothermic circulatory arrest (HCA). A retrospective analysis of all consecutive cases involving HCA from 2021 to 2024 was completed. The setting of this study is a single, tertiary academic medical center. All cardiac surgery patients undergoing HCA during the study period were evaluated for inclusion in this study. The intervention in this study was the implementation of OTE in patients undergoing HCA. Twelve out of 85 (14%) patients underwent OTE following HCA. In this cohort, there were no post-operative reintubations, major complications, or mortalities. The median intensive care unit (ICU) length of stay was 21.5 hours, and the median duration of hospitalization was 6.6 days. Patients undergoing fast track extubation (FTE) (extubation within 6 hours post-operatively), or extubation >6 hours had a median ICU length of stay of 42.1 hours (P = 0.12) and 91.8 hours (P < 0.01) and a hospital length of stay of 5.0 days (P = 0.03) and 11.5 days (P = 0.02), respectively. There were no reintubations or mortalities in the FTE group, and five reintubations and ten mortalities in the >6 hour group. OTE in patients undergoing HCA is feasible and demonstrated minimal post-operative complications in our cohort. Consideration of these cases for OTE may improve outcomes and appears to be safe in select patients. Centers experienced with OTE should consider internal evaluation of their readiness to broaden OTE to traditionally more “high-risk” populations on a case-by-case basis.
Keywords
Introduction
Early extubation, or colloquially, Fast Track Extubation (FTE), defined by the Society of Thoracic Surgery (STS) as extubation less than 6 hours after intensive care unit (ICU) arrival, has become a standard benchmark for post-operative cardiac surgery patients based on evidence that it provides similar clinical outcomes with reduced costs.1,2 A Cochrane Review by Wong et al. (2016) demonstrated that amongst a total population of 4438 participants, time-directed extubation protocols had similar risks of post-operative complications with shorter ICU length of stays. 3 The enhanced recovery after surgery (ERAS) movement has added even more momentum to this standard, with the most recent joint consensus statement from the ERAS Cardiac Society, ERAS International Society, and the STS suggesting that early post-operative extubation is safe and effective and may hasten recovery after elective procedures, with a moderate quality of evidence. 4 As is common in medicine, the question has more recently shifted to ask if early is good and faster is better. Teman et al. (2024) performed a national database analysis using the STS Database which identified a total of 36,298 patients who underwent immediate, on-table extubation (OTE) and compared them to propensity matched patients undergoing FTE at centers who routinely perform OTE. This study found that OTE was associated with significantly lower rates of post-operative mortality, reintubation, reoperation for bleeding, and prolonged length of stay (LOS). 5
Our institution was an early adopter of OTE, and with time, we have increased our OTE rate to ∼70% of all-comers for cardiac surgery with a high degree of success and surgeon buy-in. As such, we have pushed to extubate traditionally “higher-risk” patients, including those undergoing both elective and emergent procedures under hypothermic circulatory arrest (HCA). Our institution is a medium-sized academic hospital which performs approximately 600 cardiac surgery cases per year, with a 24-bed ICU. Herein, we provide a retrospective comparative case series of OTE in cases requiring HCA and describe the post-operative courses of these patients. To our knowledge, there are no previously published case series of patients undergoing HCA and OTE.
Methods
Following Institutional Review Board approval (IRB #23756; Date 2/23/2024), a retrospective analysis of all cardiac surgeries between March, 2021 and January 1, 2025 was performed. Informed consent was waived for this study. The initiation of OTE in this high-risk surgical population was a result of the success of the OTE pathway that we established at our institution. Discussions involving the intensivists, surgeons, and anesthesiologists resulted in the decision to begin considering these high-risk patients on a case-by-case basis for OTE. Both patient and surgical factors were considered when deciding which patients should be targeted for OTE, including BMI, ease of mask ventilation, neurological status on arrival, complete correction of coagulation by sonorheometry, subjective degree of hemostasis by the surgical team, and hemodynamic stability. All patients who were extubated were required to meet standard extubation criteria. For OTE, this included the ability to maintain oxygen saturations >92% on 40% fraction of inspired oxygen (FiO2) and appropriate ventilation on minimal ventilatory settings, typically defined as a pressure support less than 10cmH2O and a positive end-expiratory pressure of 5 cmH2O (see Supplemental Table 1 for full criteria). Each patient that presented to the operating room was evaluated for suitability for OTE, and a discussion between the surgeon and attending anesthesiologist occurred after chest closure to definitively decide between OTE or mechanical ventilation to the ICU. Subsequently, all procedures performed under HCA were analyzed to identify patients who underwent OTE, FTE, or extubation beyond 6 hours post-operatively. Patient demographics, comorbidities, surgical procedures, surgical times, and post-operative outcomes were then collected and analyzed using Microsoft Excel (Microsoft Corporation, Redmond, WA). Normality of continuous variables was determined with the Anderson–Darling test using Minitab (Minitab, LLC, State College, PA). Both the FTE group and extubation >6 hours group were compared to OTE using Student T-test for normal data and Mann–Whitney U Test for non-parametric data in Minitab. An extensive literature review of “on-table extubation” and “cardiac surgery” was performed.
Results
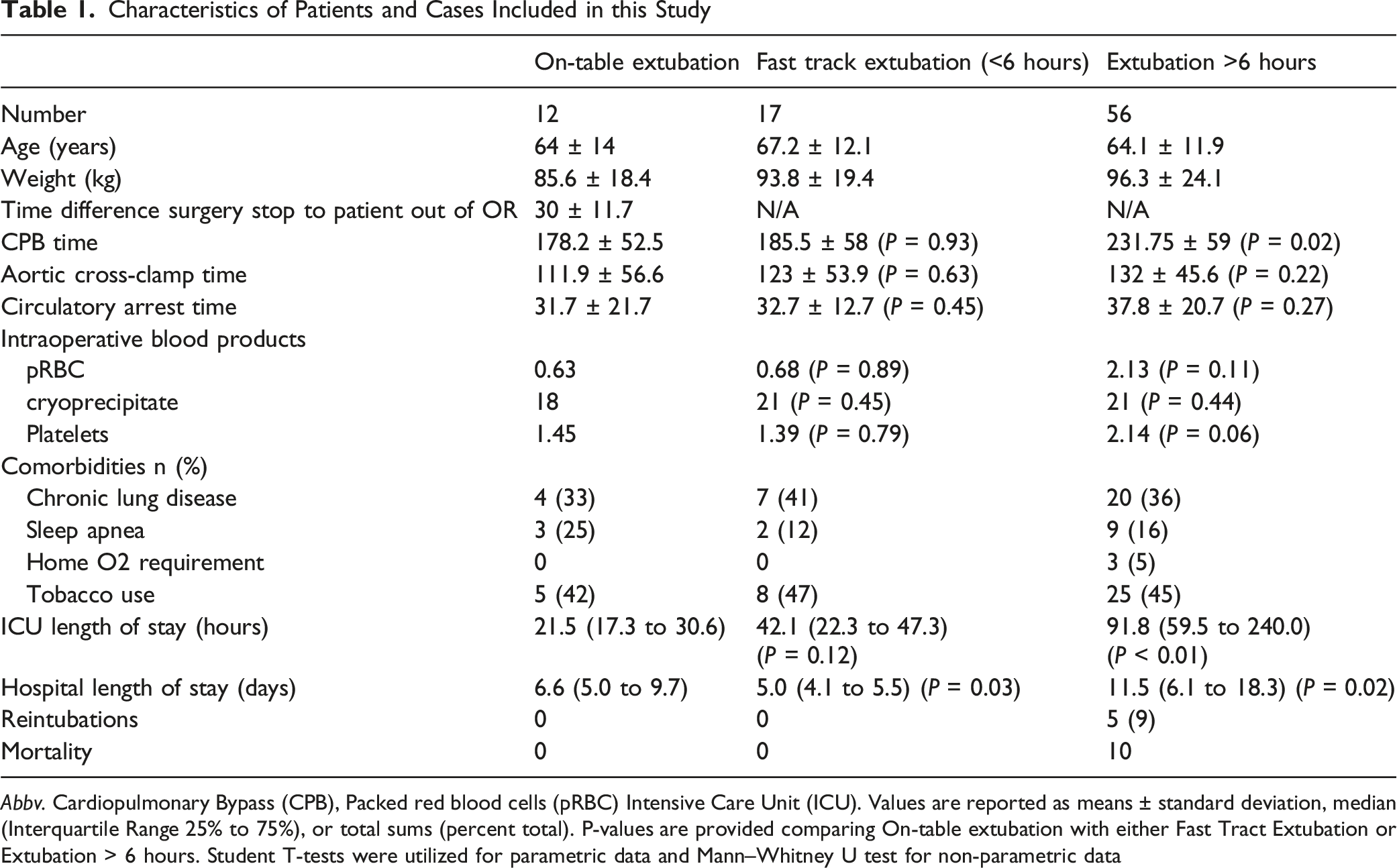
During the study period of January 2021 through December 2024, a total of 85 cases were performed under HCA, of which 12 (14%) had OTE, 17 (20%) had FTE, and the remaining 56 (66%) were extubated beyond 6 hours. There were eight males and four females in the OTE group, with a mean (SD) age of 64 (±14) years. The average BMI of the OTE population was 29.7 (range 19–36). 5 of 12 (41.7%) cases were for emergent Acute Type A aortic dissections. Pulmonary comorbidities were similar in all three groups except for home oxygen requirement (five patients in the >6 hour group and none in the OTE or FTE groups). There were no post-operative reintubations in either the OTE or FTE groups, and there were five reintubations in the >6 hour cohort. The initial oxygen therapy required in the ICU for OTE patients consisted of nasal cannula (nine), high-flow nasal cannula (HFNC) (two), and bilevel positive airway pressure (BiPAP) (one). Additionally, there were no re-explorations for bleeding, and no incidences of post-operative pneumonia, pulmonary thromboembolisms, pleural effusions requiring drainage, or post-operative pneumothorax in the OTE group. There was no statistically significant difference between the OTE and FTE groups in terms of cardiopulmonary bypass time or aortic cross-clamp time. The >6 hours extubation group had a significantly longer cardiopulmonary bypass duration than the OTE group (231.75 ± 59.0 minutes vs 178.2 ± 52.5 minutes, P = 0.02), but there was no significant difference in the aortic cross-clamp duration (132 ± 45.6 minutes vs 111.9 ± 56.6 minutes, P = 0.22). Ten of 12 (83%) patients in the OTE group had antegrade cerebral perfusion (ACP) during circulatory arrest, with the remaining two having no cerebral perfusion technique utilized during HCA. The mean duration of HCA was 31.7 ± 21.7 minutes in the OTE group, which did not differ significantly from the FTE group (32.7 ± 12.7 minutes, P = 0.45) or the >6 hour group (37.8 ± 20.7 minutes, P = 0.27). The quantity of intraoperative packed red blood cells and cryoprecipitate did not differ significantly between the three groups; however, the >6 hour group received more platelets than the OTE group, which approached significance (2.14 vs 1.45, P = 0.06). The mean post-operative ventilator time was 3.87 ± 1.2 hours and 80.7 ± 113 hours for the FTE and >6 hour group, respectively. The median initial ICU length of stay (LOS) was 21.5 (IQR 17.3–30.6) hours, 42.1 (IQR 22.3–47.25) hours (P = 0.12), and 91.8 (IQR 59.5–240.0) hours (P < 0.01) for the OTE, FTE, and extubation >6 hours, respectively. The median duration of hospitalization was 6.6 (IQR 5.0 to 9.7) days, 5.0 (IQR 4.1–5.5) days (P = 0.03), and 11.5 (IQR 6.1–18.3) days (P = 0.02) for the OTE, FTE, and extubation >6 hours, respectively (Figure 1). There were no mortalities in the OTE or FTE cohort. There were ten mortalities in the >6 hour cohort. A summary of these data can be found in Table 1.The average vasoactive-inotropic infusion score at extubation was 3.9 (0–32) in the OTE group.
6
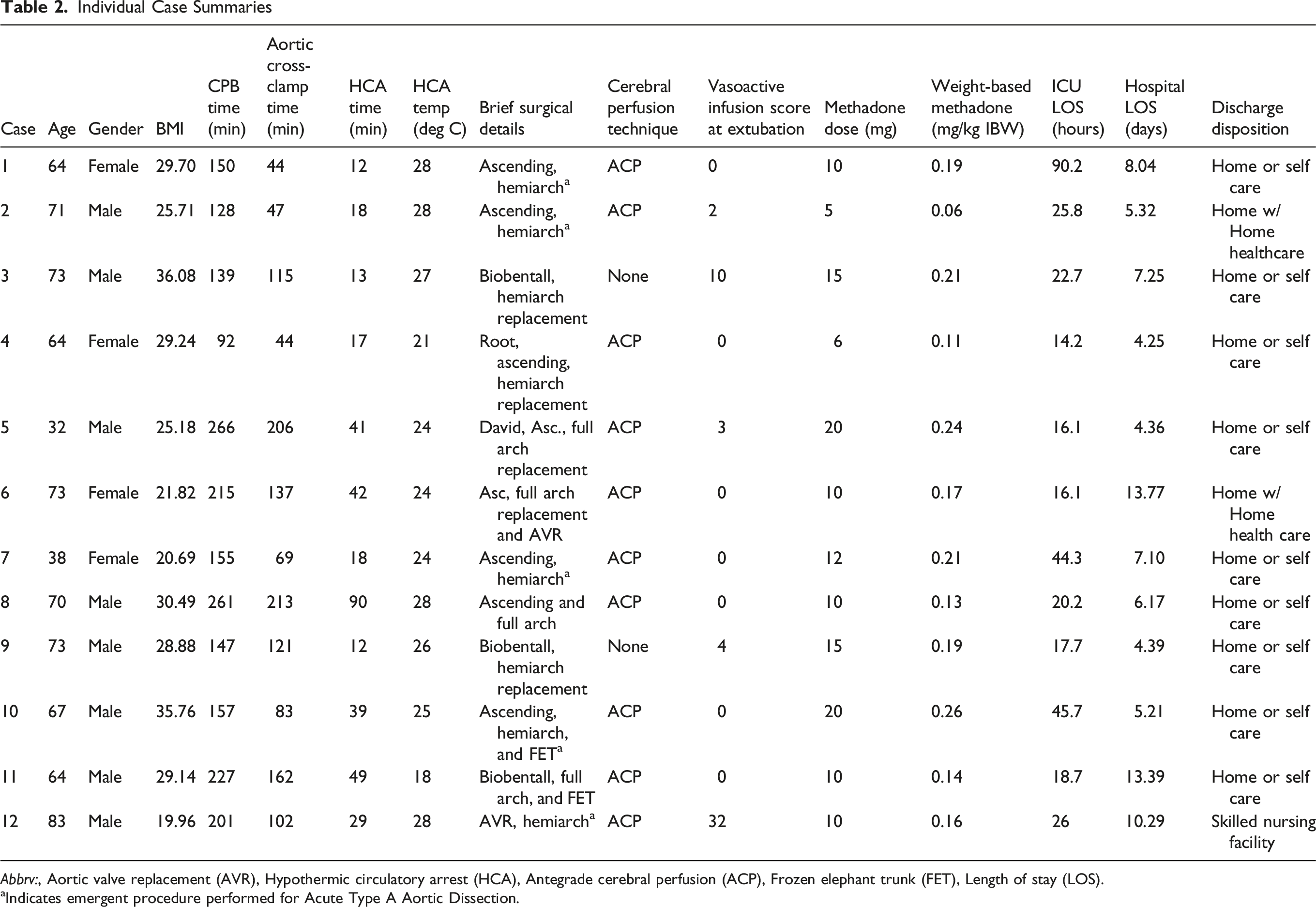
Intraoperative methadone was utilized for analgesia in all 12 (100%) of OTE patients with an average dose of 11.9 mg (±4.6) or 0.2 mg/kg (±0.1). All OTE patients additionally received superficial parasternal blocks (previously pectointercostal fascial plane blocks) prior to emergence from anesthesia. Additional demographics, including patient conditions and operative details, are available in Table 2. Comparison of perioperative times between OTE, FTE, and >6 hour extubation groups Characteristics of Patients and Cases Included in this Study Abbv. Cardiopulmonary Bypass (CPB), Packed red blood cells (pRBC) Intensive Care Unit (ICU). Values are reported as means ± standard deviation, median (Interquartile Range 25% to 75%), or total sums (percent total). P-values are provided comparing On-table extubation with either Fast Tract Extubation or Extubation > 6 hours. Student T-tests were utilized for parametric data and Mann–Whitney U test for non-parametric data Individual Case Summaries Abbrv:, Aortic valve replacement (AVR), Hypothermic circulatory arrest (HCA), Antegrade cerebral perfusion (ACP), Frozen elephant trunk (FET), Length of stay (LOS). aIndicates emergent procedure performed for Acute Type A Aortic Dissection.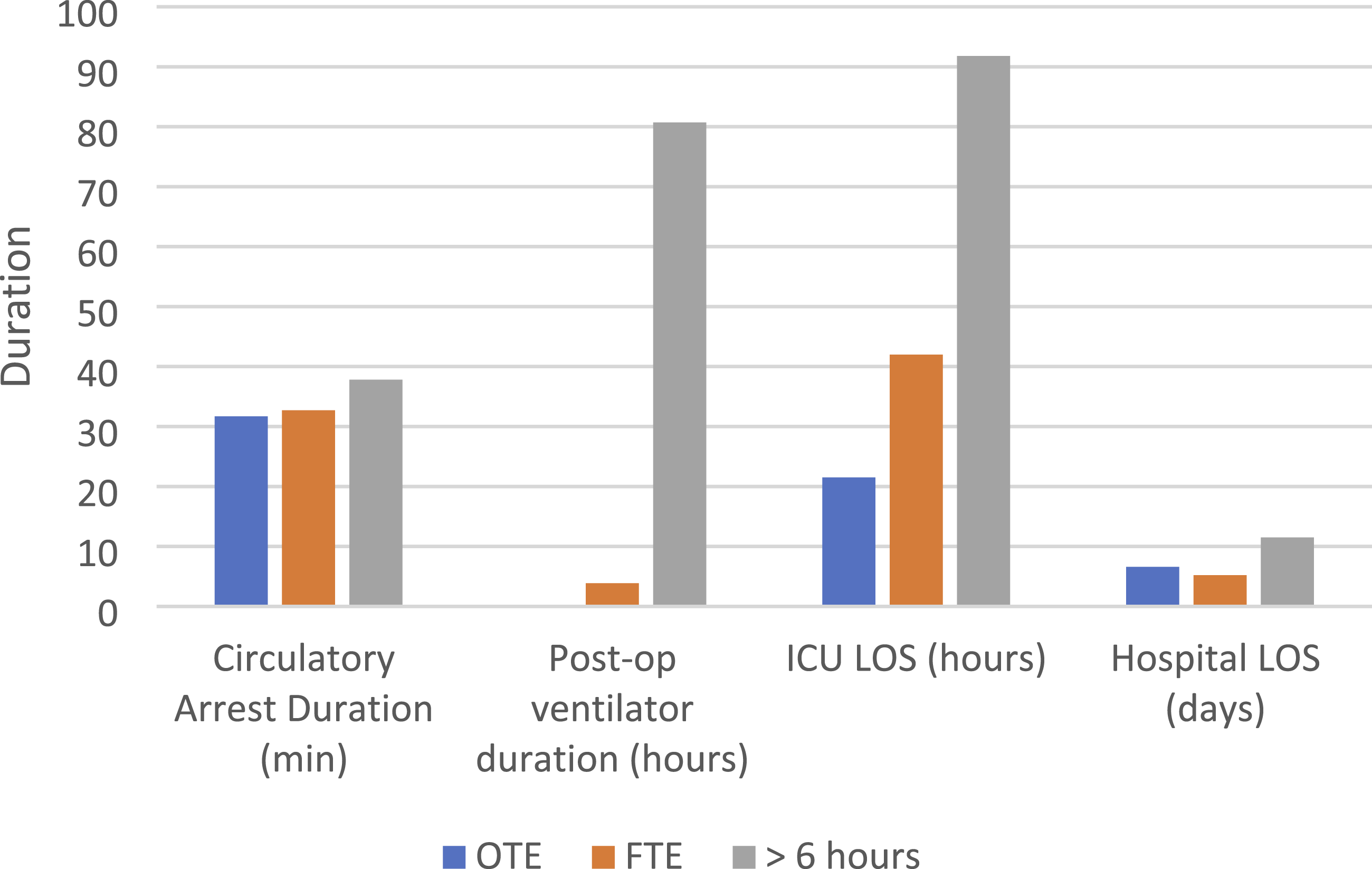
Discussion
There is increasing evidence supporting the practice of OTE in select, low-risk cardiac surgery patients undergoing elective surgeries. We would challenge, however, that such techniques need not be limited to a small selection of patients once a degree of comfort has been established at an institution. Although randomized controlled trials are lacking, observational data suggest that OTE conveys significant reductions in ICU and hospital LOS and reduces hospital costs.7,8 Furthermore, prolonged ICU admissions are associated with worsened outcomes even when adjusted for illness severity scores, with one study describing a mortality odds ratio of 3.21 for an ICU LOS >5 days. 9 Healthcare-associated infections, ICU-acquired weakness, post-intensive care syndrome (PICS), delirium, and malnutrition are all positively associated with longer ICU stays, as well.10-13 In our study, patients undergoing OTE were noted to have a near 50% shorter ICU LOS compared to patients in the FTE group; however, this did not reach significance [21.5 (IQR 17.3–30.6) hours vs 42.1 (IQR 22.3–47.3) hours, P = 0.12]. Current data suggest a low complication rate associated with OTE, with reintubation rates ranging from 0.6% to 3.3%, and no statistically significant difference in post-operative morbidity.5,8,14 Although these data come primarily from low-risk surgeries, in our cohort of patients undergoing higher-risk surgery with HCA, we noted a similarly low risk of post-operative complications, including no reintubations and no mortalities in the OTE group.
A critique can be made that OTE in our cohort was performed in highly selected individuals; while this is certainly true, it is important to emphasize that the decision to extubate is made on a case-by-case basis and not pre-determined by patient comorbidity or the type of surgery they undergo. Additionally, our cohort of OTE patients did not differ significantly as compared to the FTE cohort in terms of age, weight, HCA duration, intraoperative product transfusion, or preoperative pulmonary comorbidities, and experienced similar post-operative outcomes. Although this paper was not powered to assess for infrequent post-operative complications, the similarities between the OTE and FTE group may suggest that many of the patients who are candidates for FTE at outside institutions could safely undergo OTE. Pertinently, the patients in our OTE cohort had many of the same preoperative pulmonary comorbidities as the general cardiac surgery population, including four with chronic pulmonary disease (31%), three with obstructive sleep apnea (23%), and five with chronic tobacco use (38%) (Table 1). BMI in this cohort ranged from 20–36 with an age range of 32–83 years (mean 64 years). Five patients (42%) were on vasoactive infusions at the time of extubation. The patient’s airway exam and probability of needing non-invasive positive pressure ventilation (NIPPV) should be taken into consideration when determining the feasibility of OTE and is a major factor when we consider patients for OTE at our institution once hemodynamics and hemostasis are deemed adequate. In this cohort, only one patient required NIPPV (BiPAP) for post-operative respiratory acidosis. The two patients who arrived in the ICU on HFNC were weaned to nasal cannula within one hour of arrival.
In addition to the aforementioned benefits associated with OTE, the ability to obtain a complete, rapid neurological exam after surgeries involving HCA provides potentially management-altering information. The incidence of stroke in cardiac surgery procedures involving CPB is quoted at 1–3%, 15 and for surgeries involving HCA, the risk increases to 3.1–13.1%. 16 In octogenarians undergoing surgeries requiring HCA, that risk is elevated nearly two-fold, with a 20% incidence of ischemic stroke. 17 Early identification of neurological deficits in cardiac surgery allows for imaging and interventions which may reduce the long-term sequelae associated with such an infarct, especially in the setting of a large vessel occlusion. 18 Reestablishing adequate cerebral perfusion through modifications of blood-pressure goals or interventions on large vessel occlusions with endovascular options have been shown to improve neurological outcomes after cerebral infarctions; however, timeliness is essential.19,20 In our experience, our surgical colleagues appreciate the early neurological assessment and, in fact, specifically encourage OTE when safe and clinically appropriate.
Getting to this point at our institution took time and was born from an endeavor to improve post-operative pain control and adhere more closely to the tenants of modern ERAS protocols. While we believe there are benefits to OTE that should not be limited to low-risk patients having elective procedures, we would emphasize that there must be a systematic, multi-disciplinary strategy in place prior to initiating an OTE program. Optimal analgesia is imperative to allow for appropriate respiratory mechanics immediately upon extubation; in our experience, we accomplish this with a single intraoperative dose of methadone in addition to supplemental fentanyl and a routine use of an appropriate regional anesthetic technique at the end of surgery prior to extubation. In this study, every patient received intraoperative methadone prior to surgical incision, with a mean dose of 11.9 mg (±4.6) as well as pre-emergence superficial parasternal blocks. The dose range we consider appropriate for methadone is between 0.15 mg/kg and 0.3 mg/kg based on prior dose finding studies, and the average weight-based dose in this study was 0.2 mg/kg (±0.1) of ideal body weight.21-24 Meticulous surgical hemostasis, sonorheic or viscoelastic-guided correction of coagulopathy, and maintenance of normothermia are also vital to the success of OTE in these cases. It should be noted that the preferred HCA strategy at our institution is moderate hypothermia with ACP, which may decrease the degree of coagulopathy and risk of bleeding in our patient population and reduce relative CPB times due to the decreased time needed for cooling and rewarming. Seven of the 12 patients underwent moderate HCA (core temperature ≥25 deg Celsius), with additional three patients being cooled to 24 deg Celsius with a target temperature of 25 deg Celsius. Additionally, buy-in from surgeons, cardiac anesthesiologists, intensivists, respiratory therapists, and nursing staff is critical to success and should be obtained prior to the initiation of any OTE program.
Limitations of this study include the relatively small sample size of the OTE group which makes identification of rare post-operative outcomes challenging and limits the amount of statistical significance which can be drawn between groups. Additionally, as previously mentioned, all OTE patients are specifically selected which inherently introduces bias in this population. While true, we would argue that this stringent selection should be the approach taken with OTE and is not a limitation of the technique but rather encourages the intraoperative team to critically evaluate their patients on a case-by-case basis. It is also worth noting that this manuscript describes a patient cohort from the infancy of OTE in HCA cases through four years of experience. Additional follow-up and larger prospective trials are warranted to evaluate the utility of this technique in the HCA surgical population.
Conclusion
OTE represents the next iteration of FTE, and while in its infancy, has early evidence supporting its safety and effectiveness in reducing ICU LOS, hospital costs, and potentially mortality. However, current studies are limited to low-risk populations undergoing low-risk, elective surgeries. This current case series describes 12 cases of OTE in patients with multiple high-risk comorbidities undergoing both elective and emergent high-risk cardiac surgeries with exceptionally low post-operative complication rates. While additional comparative studies are needed to assess either the non-inferiority or superiority of OTE in this patient population, we wish to emphasize that the consideration of a patient for OTE should not be dictated solely by the urgency of their surgery or their medical history but should be completed on a case-by-case basis. Routine consideration of these cases for OTE may result in decreased ICU LOS, hospital LOS, and improved outcomes, and future large trials are needed to assess this. Centers experienced with OTE should consider internal evaluation of their readiness to broaden it to traditionally more “high-risk” populations within their own institutions.
Supplemental Material
Supplemental Material - Implementation and Results of on-Table Extubation Following Hypothermic Circulatory Arrest: Early Experience and Outcomes
Supplemental Material for Implementation and Results of on-Table Extubation Following Hypothermic Circulatory Arrest: Early Experience and Outcomes by Justin W. Walker, Nicholas D’Alonzo, Cooper Grove, Abdulrham S. Elnaggar and S. Michael Roberts in Seminars in Cardiothoracic and Vascular Anesthesia.
Footnotes
Acknowledgments
The authors would like to acknowledge Jennifer Hahn and Michael Hess for their role in obtaining the STS data, and Meredith Fausey-Kreider for her role in compiling data from anesthesia records.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
IRB approval was obtained for the present study. This study was conducted under the appropriate ethical standards.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.