
Abstract
Keywords
Introduction
New-onset POAF after cardiac surgery is arguably the most common adverse event, with up to 30 to 50% of patients developing POAF within the first postoperative week.1,2 POAF is not only associated with both longer length of Intensive Care Unit (ICU) and hospital stay3,4 but also higher morbidity and mortality.5,6 As a result, postoperative atrial fibrillation has been a focus of international and multidisciplinary guidelines.7,8
Some predictors for the occurrence of POAF exist and have been moderately useful in defining elevated risk. These include the well-known CHADS and CHA2DS2-VASC scores as well as the POAF Score, which was specifically derived for this purpose.9,10 The CHA2DS2-VASC-Score is a tool used to assess the clinical risk for a thromboembolism in patients having atrial fibrillation. 11 The POAF Score sums points (Age 60–69: 1 pt.; Age 70–79: 2 pts; Age >=80: 3 pts; Chronic Obstructive Pulmonary Disease [COPD]: 1 pt, estimated Glomerular Filtration Rate [GFR]<15 mL/min: 1 pt.; emergency: 1pt.; preop intra-aortic Balloon Pump (IABP) 1pt.; Left Ventricular Ejection Fraction [LVEF] <30: 1pt.; Valve surgery: 1 pt; >=3pts with POAF in >40%).
In addition to scores based upon a patient’s characteristics, history, and medical procedures, morphological features of the heart (e.g., atrial strain in echo and Magnetic Resonance Imaging [MRI]) 12 and the heart’s electrical activity (e.g., ECG) 13 have in part shown incremental value in predicting POAF. While some imaging modalities may not be available or require expensive and time-consuming software, the preoperative ECG is routinely available, requires no specialized hardware/software, and is both inexpensive and non-invasive. Indeed, many ECG P-wave measurements have been associated with higher rates of atrial fibrillation in non-surgical patients. 14 Recently, the abnormal PTFV1 has emerged in the non-surgical population as a predictor of atrial fibrillation in a large meta-analysis. 15 However, the utility of the PTFV1 for predicting new onset POAF in patients undergoing cardiac surgery has not been examined.
We hypothesized that an abnormal PTFV1 would be associated with a higher risk of POAF in patients undergoing on-pump cardiac surgery. In this study, we aimed to (1) examine the association of an abnormal PTFV1 with POAF in the surgical population, (2) compare other ECG-based predictors with POAF, and (3) examine a possible incremental value with other POAF predictors all in a cardiac surgery population.
Materials and Methods
Study Design and Participants
This is a secondary analysis of an observational single-center, retrospective study approved by the Ethics Committee of Northwestern and Central Switzerland (EKNZ) with an informed consent waiver (EKNZ, 2016/1550, January 10, 2017). 16 This original study included adult patients undergoing elective and non-elective on-pump cardiac surgery with median sternotomy at the University Hospital Basel, Switzerland, from December 2018 to August 2020. Aortocoronary bypasses, valve surgery, combined bypass, and valve surgery were included in the original study; patients with thoracotomies, partial sternotomies, and aortic surgery were excluded.
In this secondary analysis, patients with a history of atrial fibrillation or atrial flutter, with pacemakers and/or ICDs) and those lacking an ECG made within the 3 months prior to surgery were excluded. Additionally, ECGs deemed to be of poor quality were also excluded.
Perioperative Work-up and Anesthesia
Preoperatively, patients receive a routine medical work up including a 12-lead ECG, a transthoracic echocardiogram, and a coronary angiogram. Additionally, a number of specific examinations for cardiac surgery were performed at the surgeon’s discretion.
As customary at our institution, patients generally did not receive a premedication. Neither B-blockers nor amiodarone were administered de novo but were continued. Anesthesia was generally induced with fentanyl (1–4 μg/kg), propofol (1–2 mg/kg), and rocuronium (0.8 mg/kg) and maintained with sevoflurane titrated to achieve a Bispectral Index (BIS) value between 40 and 60. On-pump cardiac surgery is performed either with extracorporeal circulation or minimal extracorporeal circulation (for isolated Coronary artery bypass graft [CABG] surgery) using St. Thomas cardioplegia or blood cardioplegia.
At the end of the surgery, temporary epicardial pacing wires were placed on the surface of the right atrium and ventricle, and pacing leads were connected to a standard external dual-chamber pacemaker (Osypka Pace 203H). Before beginning the weaning process, the pacemaker’s sensing and pacing thresholds for the atrium and ventricle were tested, and separation commenced with a targeted heart rate of 90/min paced either A00 or—if not possible—by DVI pacing modes. Upon arrival in the ICU, patients were first weaned from catecholamines (if administered) and then the pacemaker was weaned according to hemodynamic stability.
ECG-Based Measurements
Two authors (M.G. and J.K.B.) analyzed the patients ECGs without knowing whether they later developed atriall fibrillation after the surgery evaluated 252 preoperative 12-lead ECGs (speed 25 mm/s). ECGs were recorded at most 3 months prior to surgery and stored in the patients’ electronic record. In order to most accurately quantify P-wave related measurements, ECGs were first digitally scanned in PNG format and then enlarged (1200%) to show the area of interest. In the next step, edited photos of P-waves in ECGs were examined by Plot Digitizer (Version 1.4.1, D. Medeiros, Figure 1 top), a software which allows placement and exportation of x and y coordinates on images. These coordinates were exported and analyzed by a custom-made code in R (The R Foundation for Statistical Computing, Vienna, Figure 1 bottom). Methodology for ECG-based measurements. Shown are the leads V1 and II (left and right, respectively). The top panels show a scan of the ECG region of interest and the points placed to track and export the p-wave and relevant points. The bottom panels show the measured values using customized R code.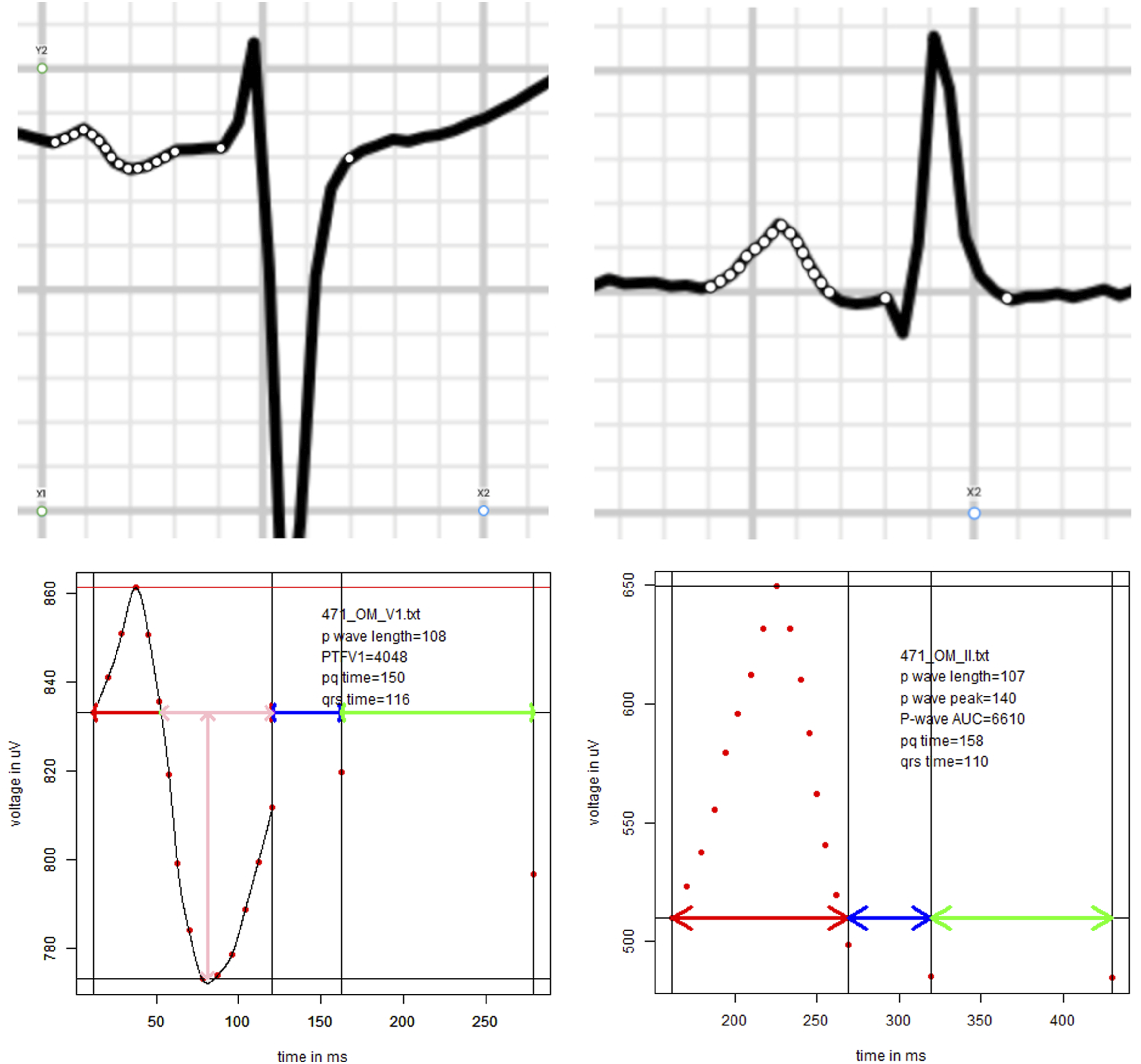
This process allowed for a detailed and uniform analysis of relevant measurements. Specifically, we examined the PTFV1 (the area under the baseline in the second portion of the biphasic P in V1, as previously described, 17 P-wave length in lead II, the area under the P-wave in lead II, PR-interval, and QRS duration in lead V1 and II.
Data Collection, End Points, and Bias
Variables were extracted in the original study from the electronic patient record as was the occurrence of diagnosed new-onset POAF. To accurately describe the patient population, the following pre- and perioperative variables were predefined: age, gender, heart failure, hypertension, diabetes mellitus, stroke, TIA (transient ischemic attack), thrombosis, vascular disease, CHA2DS2VASC-Score, body mass index (BMI), COPD, obstructive sleep apnea syndrome (OSAS), creatinine clearance, renal failure (defined as glomerular filtration rate [GFR] less than 50 mL/min), mitral valve disease, valve surgery, potassium levels upon ICU, LAVI (left atrial volume index in cm2/kg), and left atrial (LA) dilation.
Due to the high correlation between the CHA2DS2VASC-Score and other significant variables (such as age), the score was not included in the adjusted model to avoid multicollinearity.
Statistical Analyses
Patient characteristics are presented as mean (standard deviation), median (Q1-Q3), and count (%), for normally distributed continuous data, for non-normally distributed data, and for categorical data, respectively. The distribution was visually assessed by histogram. Potential differences in the distribution of these variables in patients with and without POAF were assessed by t test, Wilcoxon tests, and Chi-square test.
An initial unadjusted logistic regression analysis was conducted with the variables shown in Table 2 (e.g., age, CHA2DS2VASC-Score, and PTFV1). For variables with statistically significant odds ratios, a second round of analysis using adjusted logistic regression models was performed to control for potential confounding variables. In cases of strong collinearity, the variable with the strongest association was selected.
The sample size was determined by the following estimation: Applying a rule of thumb that 20 events are required per variable in multivariable models, a total of 60 events would allow for a robust univariable analysis of the PTFV1 as well as for its incremental value in addition to the CHA2DS2VASC-Score and one other variable. The rule of thumb, as a simplified principle in statistics, refers in this case to determining the number of events needed to ensure adequate power in our analysis. Assuming a POAF incidence of 25% in our population, a total of 240 patients would have to be included in our analysis to arrive at 60 events. Allotting for 5% missing patient characteristics, 4 patients (or 1 POAF) were added per estimator, yielding 252 patients.
All analyses were conducted in R 3.5.2 (The R Foundation for Statistical Computing, Vienna).
Results
Figure 2 shows a flow chart of patient inclusion. We screened 353 patients underlying on-pump cardiac surgeries, of which 101 were excluded (32 missing ECGs, 17 ECGs with insufficient quality, 11 pacemakers or ICDs, and 41 patients with a history of atrial fibrillation). This left 252 patients for analyses of whom a total of 62 patients (24.6%) developed new-onset POAF during their hospital stay. Flow chart of included and excluded patients.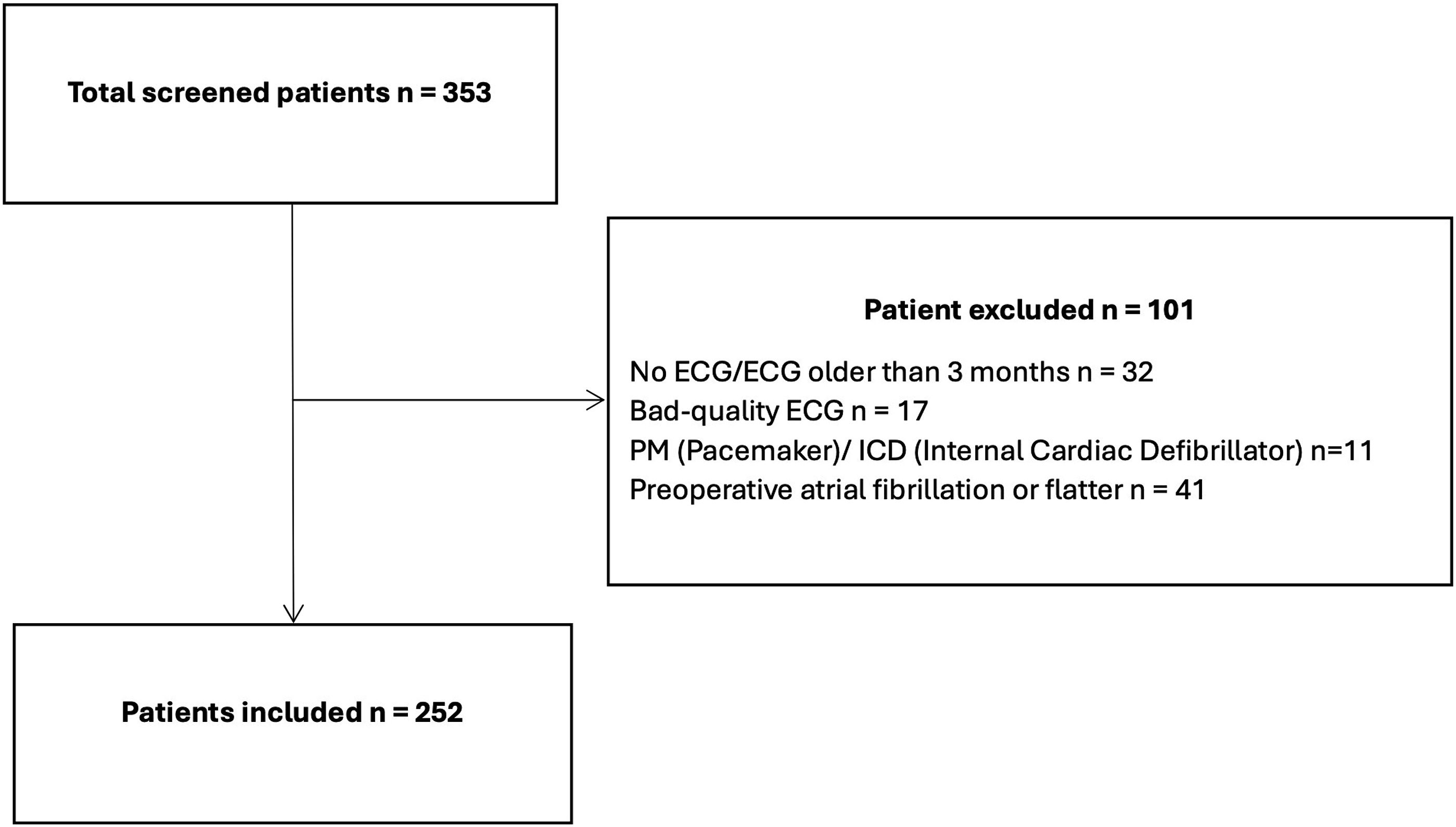
Comparison of Patient Characteristics by POAF Status. Patient Characteristics are Presented as Standard Deviation, Median (Q1–Q3), and Count (%). Unless Otherwise Stated Data was Available for all 241 Patients.
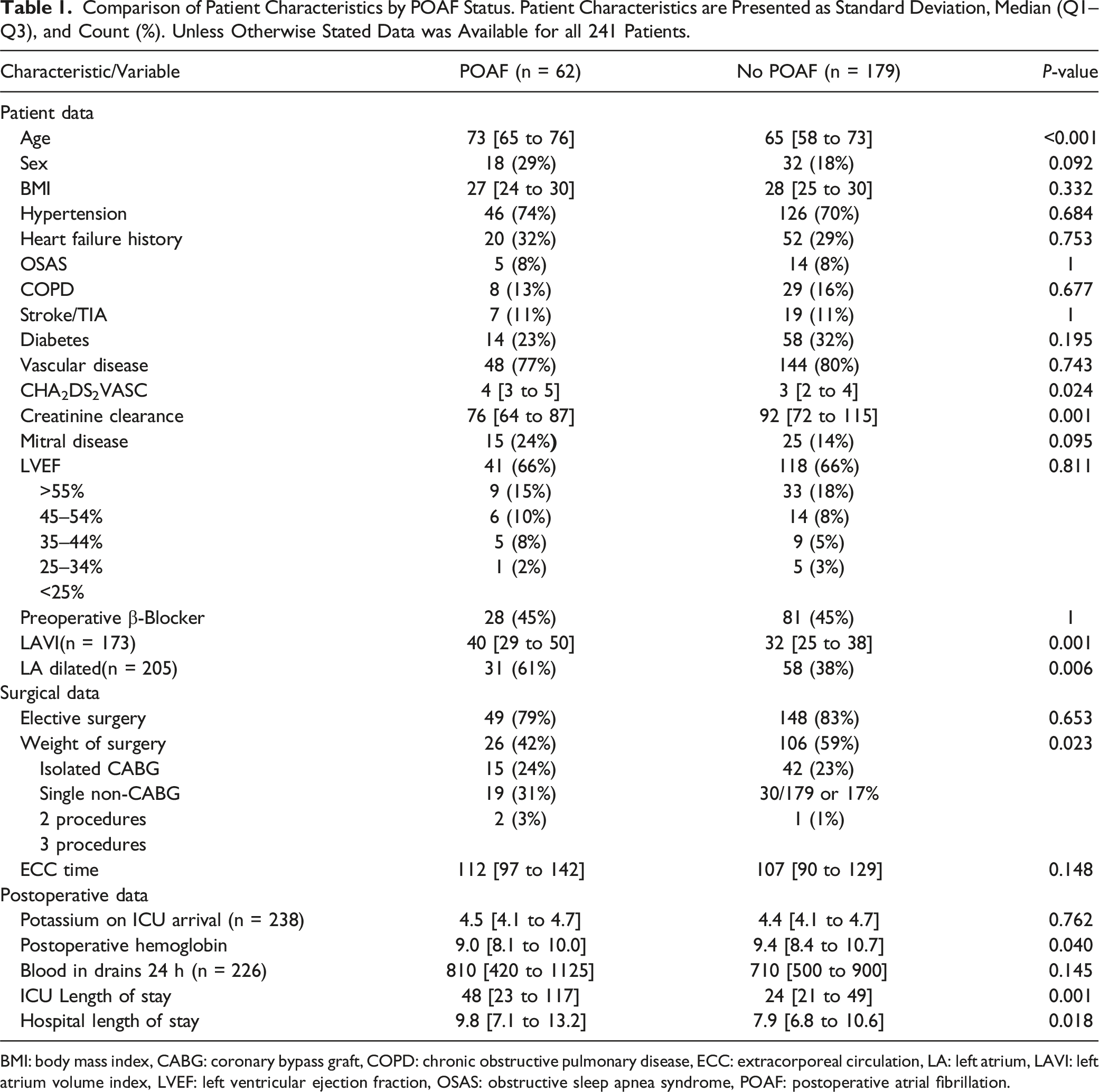
BMI: body mass index, CABG: coronary bypass graft, COPD: chronic obstructive pulmonary disease, ECC: extracorporeal circulation, LA: left atrium, LAVI: left atrium volume index, LVEF: left ventricular ejection fraction, OSAS: obstructive sleep apnea syndrome, POAF: postoperative atrial fibrillation.
Unadjusted and Adjusted Odds Ratios (ORs) for Postoperative Atrial Fibrillation (POAF).
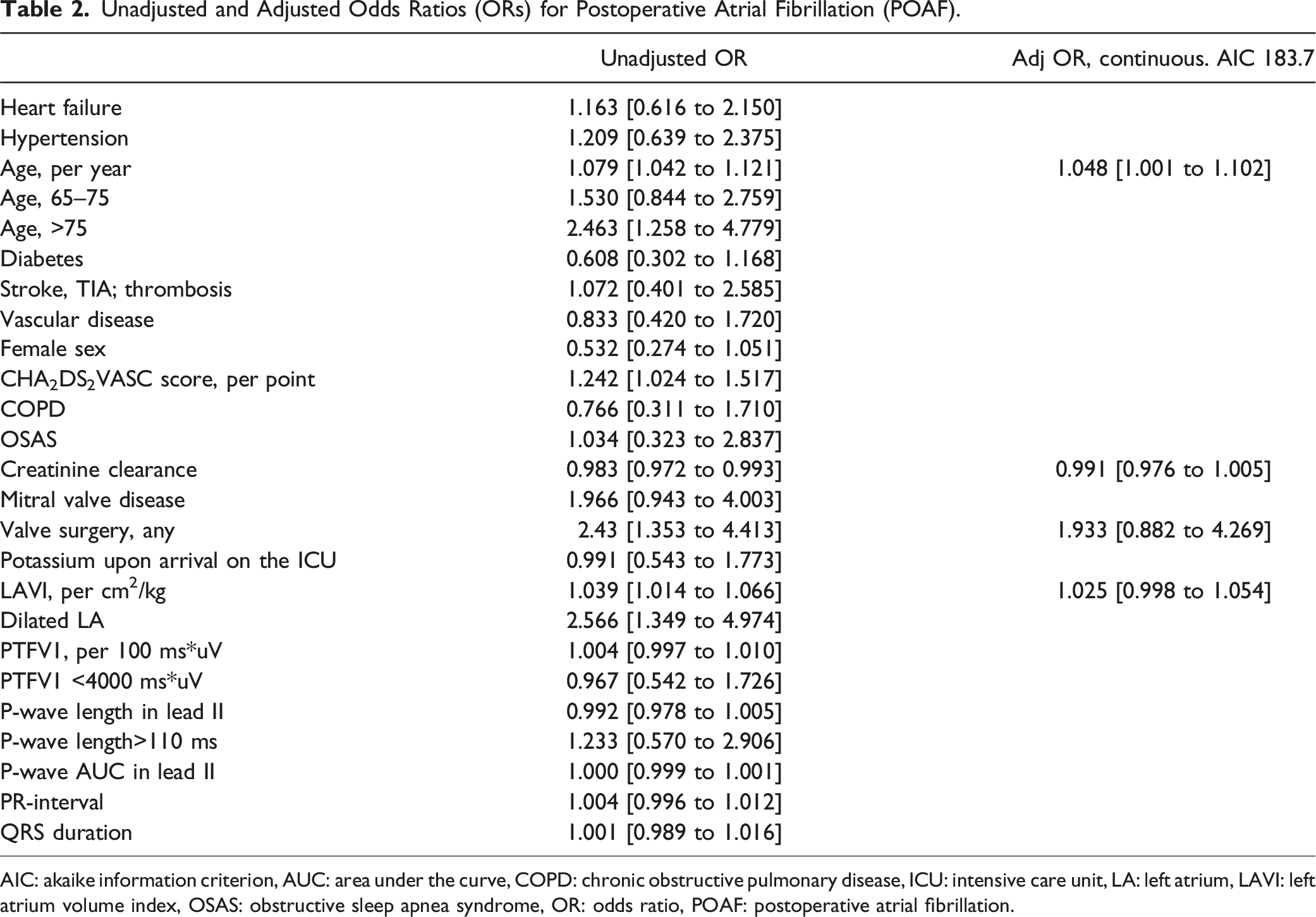
AIC: akaike information criterion, AUC: area under the curve, COPD: chronic obstructive pulmonary disease, ICU: intensive care unit, LA: left atrium, LAVI: left atrium volume index, OSAS: obstructive sleep apnea syndrome, OR: odds ratio, POAF: postoperative atrial fibrillation.
Discussion
In this observational retrospective analysis, we found no association between PTFV1 or other ECG-based variables and new onset POAF in patients undergoing cardiac surgery with cardiopulmonary bypass. However, age, creatinine clearance, valve surgery, and LAVI were associated with a higher incidence of POAF with age seeming to be the most robust.
Comparison to Previous Studies Examining PTFV1
To the best of our knowledge, this is the first study to investigate PTFV1 in the postoperative cardiac surgery population. The PTFV1 was first described by Morris et al. 16 dividing the P-wave in lead V1 into initial and terminal portions. They were able to show that normal subjects could be distinguished from patients with left-sided valvular lesions.
An Overview of Studies That Explore AF in Relation to PTFV1.
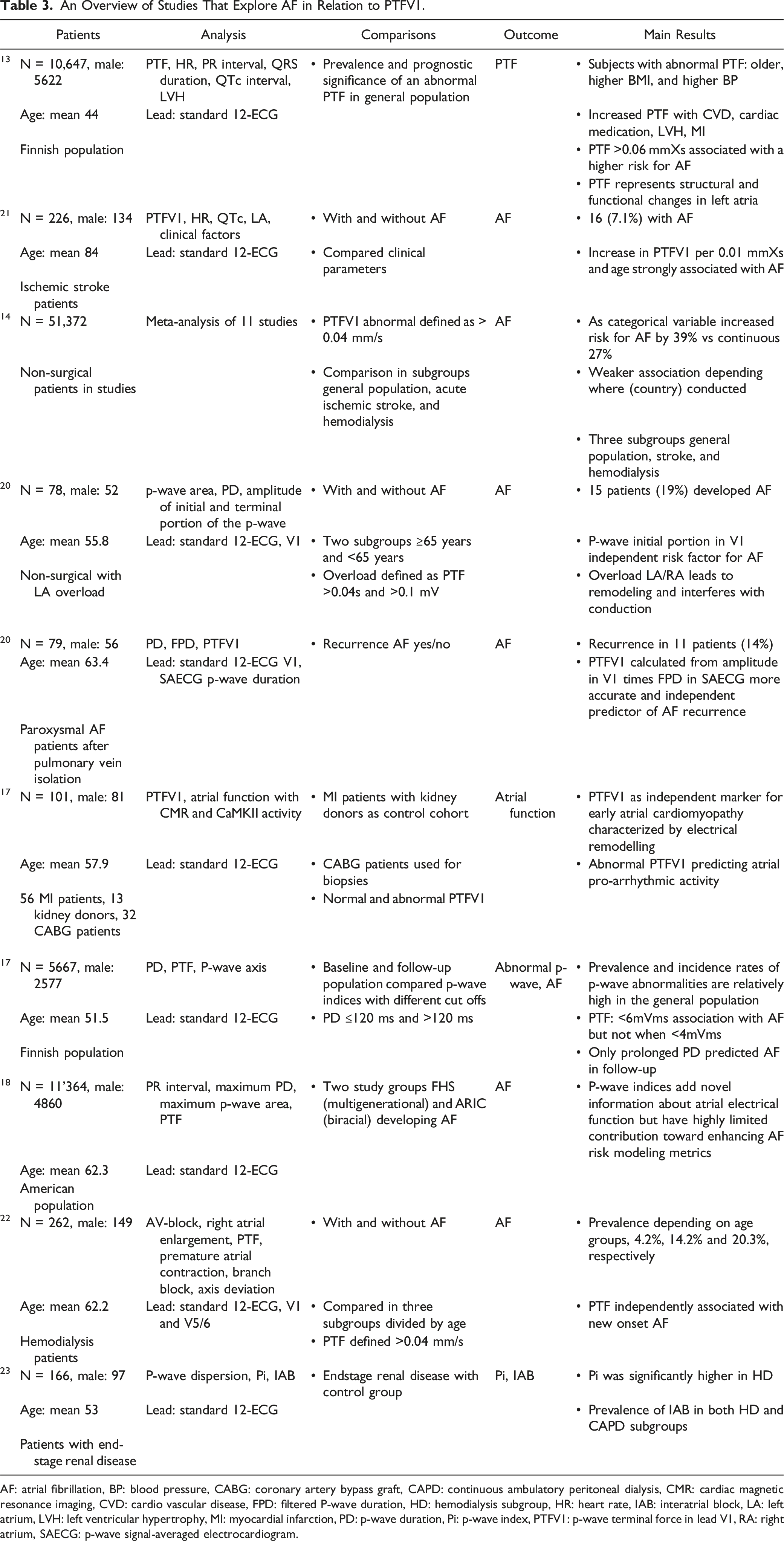
AF: atrial fibrillation, BP: blood pressure, CABG: coronary artery bypass graft, CAPD: continuous ambulatory peritoneal dialysis, CMR: cardiac magnetic resonance imaging, CVD: cardio vascular disease, FPD: filtered P-wave duration, HD: hemodialysis subgroup, HR: heart rate, IAB: interatrial block, LA: left atrium, LVH: left ventricular hypertrophy, MI: myocardial infarction, PD: p-wave duration, Pi: p-wave index, PTFV1: p-wave terminal force in lead V1, RA: right atrium, SAECG: p-wave signal-averaged electrocardiogram.
Comparison to Previous Studies Examining ECG Based Markers and POAF in Cardiac Surgery
An Overview of Studies That Explore AF in Relation to PTFV1 With Focus on POAF.
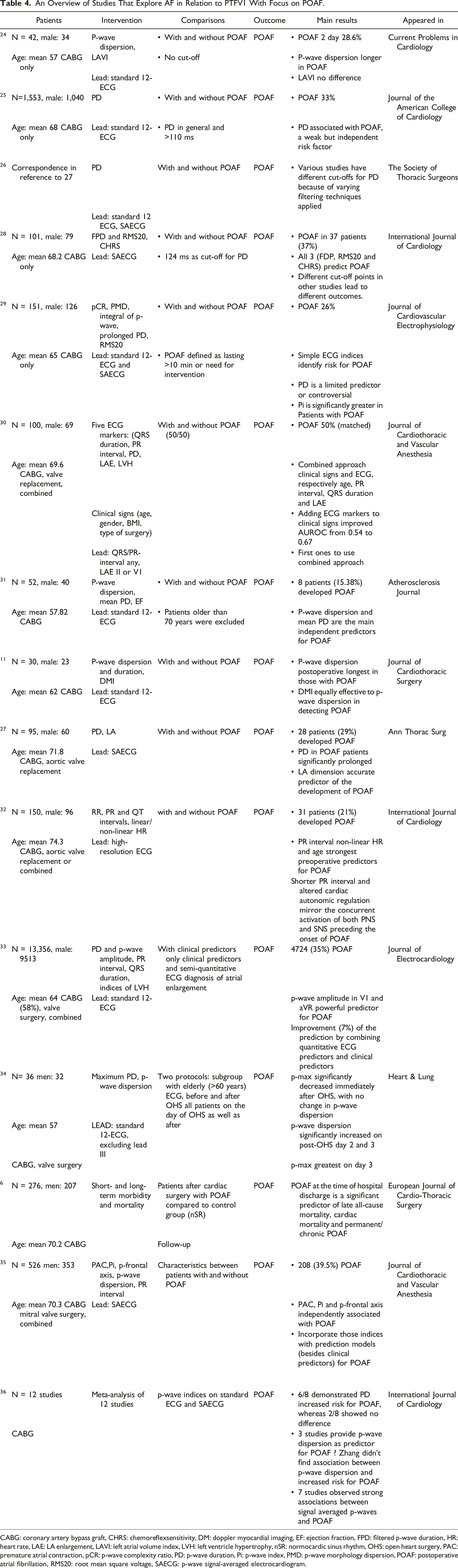
CABG: coronary artery bypass graft, CHRS: chemoreflexsensitivity, DM: doppler myocardial imaging, EF: ejection fraction, FPD: filtered p-wave duration, HR: heart rate, LAE: LA enlargement, LAVI: left atrial volume index, LVH: left ventricle hypertrophy, nSR: normocardic sinus rhythm, OHS: open heart surgery, PAC: premature atrial contraction, pCR: p-wave complexity ratio, PD: p-wave duration, Pi: p-wave index, PMD: p-wave morphology dispersion, POAF: postoperative atrial fibrillation, RMS20: root mean square voltage, SAECG: p-wave signal-averaged electrocardiogram.
Potential Mechanisms of New-Onset Postoperative Atrial Fibrillation after (Cardiac) Surgery
Although an abnormal PTFV1 may be promising in predicting atrial fibrillation in a non-surgical population, 15 it may be less relevant in cardiac surgery. This lack of association may be due to the different mechanisms of new-onset postoperative atrial fibrillation in cardiac surgery patients. 38
The type of surgical procedure and the surgical steps themselves may play a distinctive role. Patients undergoing valve surgery have a higher incidence of early postoperative AF than patients after CABG. 39 Moreover, off-pump CABG is associated with a lower incidence of AF than traditional on-pump CABG. 40 A recently conducted large randomized trial examined the effect of a left posterior pericardiotomy. 41 A total of 420 patients undergoing elective cardiac surgery (excluding patients scheduled for mitral or tricuspidal valve surgery) were included in the study. POAF occurred in 37 (17%) of 212 patients having left posterior pericardiotomy compared to 66 (32%) of patients with no intervention. The large effect size of this surgical step not only highlights the relevance of surgery and surgical steps in POAF, it also describes a potential pathomechanism in which blood and clots accumulating in the pericardial cavity trigger POAF. However, whether pleural effusion induces the pathomechanism of an inflammatory response or the exertion of compression and stretching of the atrial wall is not well understood. 21
If, as suggested, the negative terminal part of the P-wave serves as an indicator of heightened atrial fibrosis, electrical remodeling, and structural changes in the atrium, the effect in surgical patients may simply be relatively smaller due to the impact of the surgical procedure.
Clinical Implications
Current guidelines on POAF recommend perioperative oral B Blocker and perioperative amiodarone for the prevention of postoperative AF (Class I, A/B, Class IIa A/B). 8 Additionally, pre, intra, and postoperative prophylactic amiodarone are reasonable in elevated-risk patients. However, identification of elevated-risk patients remains difficult with no specific recommendation made (risk factors: age, history of atrial fibrillation, renal failure, mitral valve surgery/disease, heart failure, COPD; no cut-off for elevated risk made). It seems ECG-based measures may be of limited value. Of the available scores, the CHA2DS2VASC and POAF Score have been recommended to stratify risk. While our study showed the CHA2DS2VASC-Score to be associated with POAF, it was largely driven by age and without model improvement for the CHA2DS2VASC-Score (age AIC = 257.1, CHA2DS2VASC AIC = 271.1). The POAF score incorporates a number of variables not applicable to our patients (preoperative IABP, emergency surgery) and was hence not calculated. However, it is largely based on age and in addition to the above, it includes COPD, GFR, heart failure, and valve surgery, all of which were included in our sample.
Study Strengths and Limitations
This study had a number of strengths. First, it is one of the larger studies examining P-wave signs for POAF after cardiac surgery and the only one to date examining PTFV1 in a cardiac surgery population. Second, we included CABG and non-CABG patients, which may have increased heterogeneity in the sample but led to larger external validity. Third, several different P-wave signs were analyzed in a detailed fashion.
However, our study also has some limitations. First, it was a single center, retrospective secondary analysis, and—as such—deserves all the inherent caveats. Second and relatedly, as a secondary analysis examining native P-waves in patients with no history of atrial fibrillation, some patients were excluded (e.g., paroxysmal atrial fibrillation and pacemakers). These patients still require management and may exhibit the highest risk. Third, preoperative 12-lead ECGs were examined and hence no conclusions can be drawn about intraoperative or postoperative ECGs.
Conclusion
Our study found no association between PTFV1 and the incidence of POAF after cardiac surgery. Clinical characteristics (e.g., age and renal function) and surgical considerations (type of surgery) seem to be more important in the risk assessment for new-onset POAF after cardiac surgery. For non-cardiac surgery, PTFV1 remains uncertain as there is no interaction on the heart itself.
There remains an urgent need for standard care protocols for cardiac surgery patients, given the consistent or even rising incidence of POAF and the potential adverse effects of atrial fibrillation and antiarrhythmic drugs used for thromboembolism prophylaxis in atrial fibrillation patients. 42
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. Intramural only.