
Abstract
Failure to provide one-lung ventilation can prohibit minimally invasive thoracic surgeries. Strategies for one-lung ventilation include double-lumen endotracheal tubes or endobronchial blockers, but rarely both. Inability to provide lung isolation after double-lumen endotracheal tube placement requires troubleshooting and sometimes the use of extra equipment. This case describes using a unique Y-shaped endobronchial blocker placed through a left-sided double-lumen endotracheal tube after failure to achieve lung isolation with a double-lumen endotracheal tube alone.
Keywords
Introduction
One-lung ventilation (OLV) is necessary during many thoracic surgical procedures to aid in surgical visualization, and failure to provide OLV can be especially prohibitive in minimally invasive thoracic surgeries. Multiple strategies exist for establishing OLV, including double-lumen endotracheal tubes (DLT) or the use of an endobronchial blocker (EBB)1-3 through a single-lumen endotracheal tube (SLT). Selection between a DLT or EBB is multifactorial, with ease of intubation,4,5 variant anatomy, 6 site of surgical procedure, and provider experience being some of the considerations. Overall, DLTs are often considered the gold standard for lung isolation. Regardless of the method of establishing OLV, being able to manage inadequate lung isolation once the patient is in lateral decubitus position is a clinically challenging scenario. Here, the authors describe a unique approach to establishing OLV by placing a Rüsch EZ-Blocker (EZB) (Telflex Inc., Wayne, PA) through a left-sided DLT after failing to achieve optimal and consistent OLV with a DLT. Verbal and written informed consent for publication was obtained from the patient.
Case Report
A 67-year-old, 195 cm, 156 kg man presented for right video-assisted thoracoscopic pleural biopsy secondary to pleural thickening and shortness of breath. The patient’s medical history was significant for chronic obstructive pulmonary disease requiring supplemental oxygen, gastroesophageal reflux disease, obesity (body mass index of 41 kg/m2), cerebrovascular accident, and combined liver plus kidney transplantation.
After induction of general anesthesia with propofol and rocuronium, the patient was intubated uneventfully with an 8.0 mm SLT via video laryngoscopy for presurgical surveillance bronchoscopy. The bronchoscopic exam was unremarkable for any airway pathology. The SLT was exchanged for a 41 Fr left-sided DLT. Proper placement of the DLT was confirmed via fiberoptic bronchoscopy (FOB), showing the bronchial lumen and cuff in the left mainstem bronchus. After the patient was placed in the left lateral decubitus position, appropriate DLT position was confirmed again. Initiation of OLV was attempted with inflation of the bronchial cuff with 2 mL of air and clamping of the tracheal limb. After surgical entry into the chest, poor lung isolation was noted with partial lung ventilation on the operative side. Despite multiple attempts at repositioning the bronchial lumen and the addition of air to the bronchial cuff, satisfactory lung isolation could not be established. It was noted on bronchoscopy that the bronchial cuff was persistently herniating into the trachea following further bronchial balloon inflation. This issue was suspected to be secondary to bronchomalacia, which had not been evident during initial bronchoscopy in the supine position. Due to concern for tracheobronchial injury with further manipulation of the DLT, an alternative method of establishing OLV was pursued. Given suboptimal airway features secondary to body habitus and lateral positioning with the surgical procedure underway, it was deemed too risky to attempt to exchange the 41Fr DLT to either a different 41Fr DLT or an SLT plus EBB combination. Therefore, the authors elected to place an EZB through the DLT.
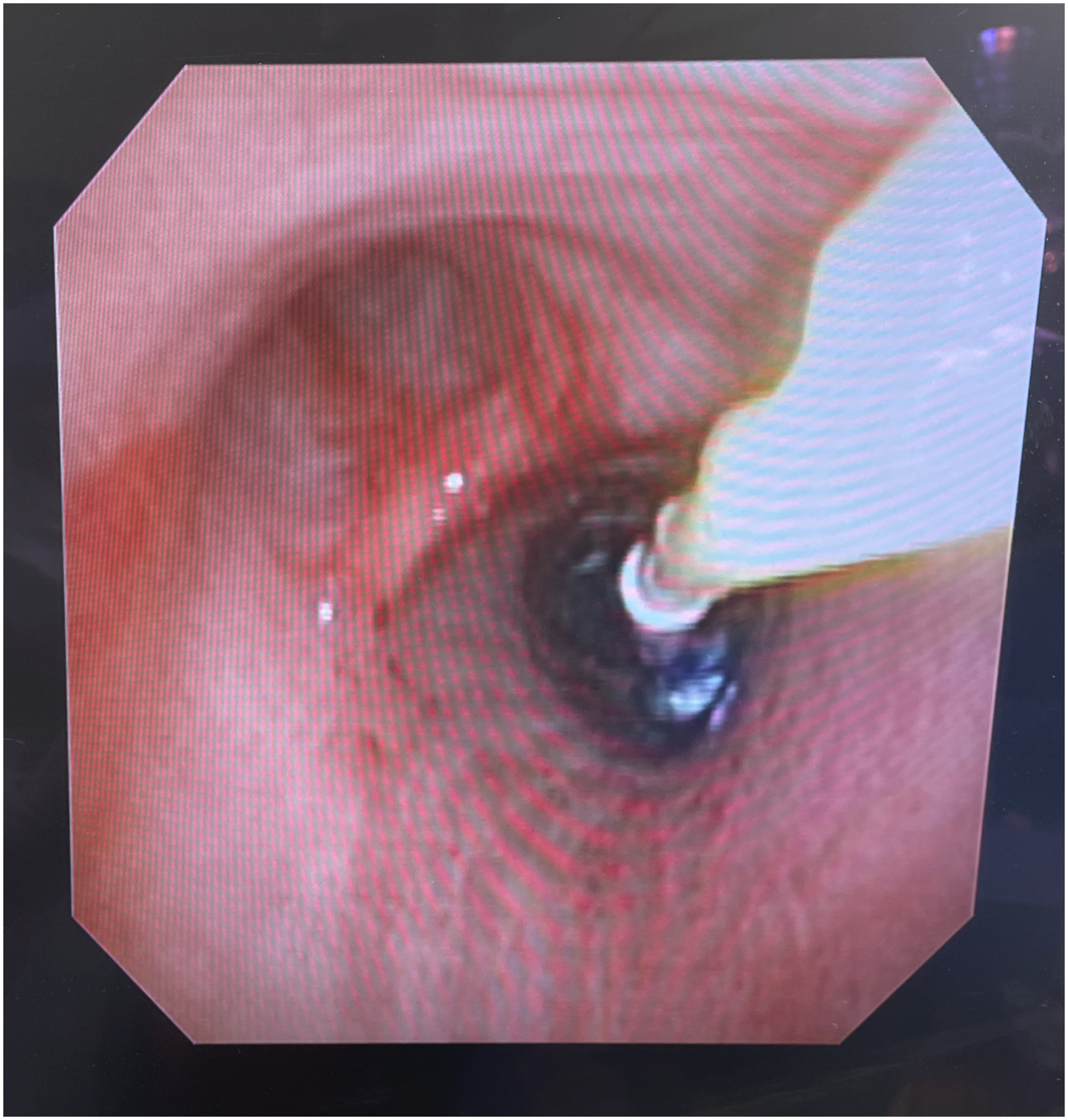
The DLT was withdrawn until the bronchial lumen was positioned above the carina, and an EZB was then inserted into the bronchial lumen. There was initial difficulty in deploying the EZB correctly with the bifurcation at the carina and the balloons located in each mainstem bronchus. We then elected to rotate the DLT so the bronchial lumen was directed toward the right mainstem bronchus and positioned the EZB with 1 limb in the bronchus intermedius and the other limb in the right upper lobe bronchus (Figures 1 and 2). Both balloons were subsequently inflated to entirely isolate the right lung. At this point, satisfactory lung isolation was obtained, and the surgical procedure was completed without further complications. At the conclusion of the case, both balloons of the EZB were deflated to reinitiate two-lung ventilation, and the patient was extubated uneventfully. Fiberoptic view of the Rüsch EZ-Blocker in the bronchial lumen of a 41 Fr left-sided double-lumen endotracheal tube. Fiberoptic view of the Rüsch EZ-Blocker placed in the bronchial lumen of a 41Fr left-sided double-lumen endotracheal tube. The bronchial lumen is oriented toward the right mainstem bronchus with 1 balloon of the EZ-Blocker in the bronchus intermedius and the other in the right upper lobe bronchus.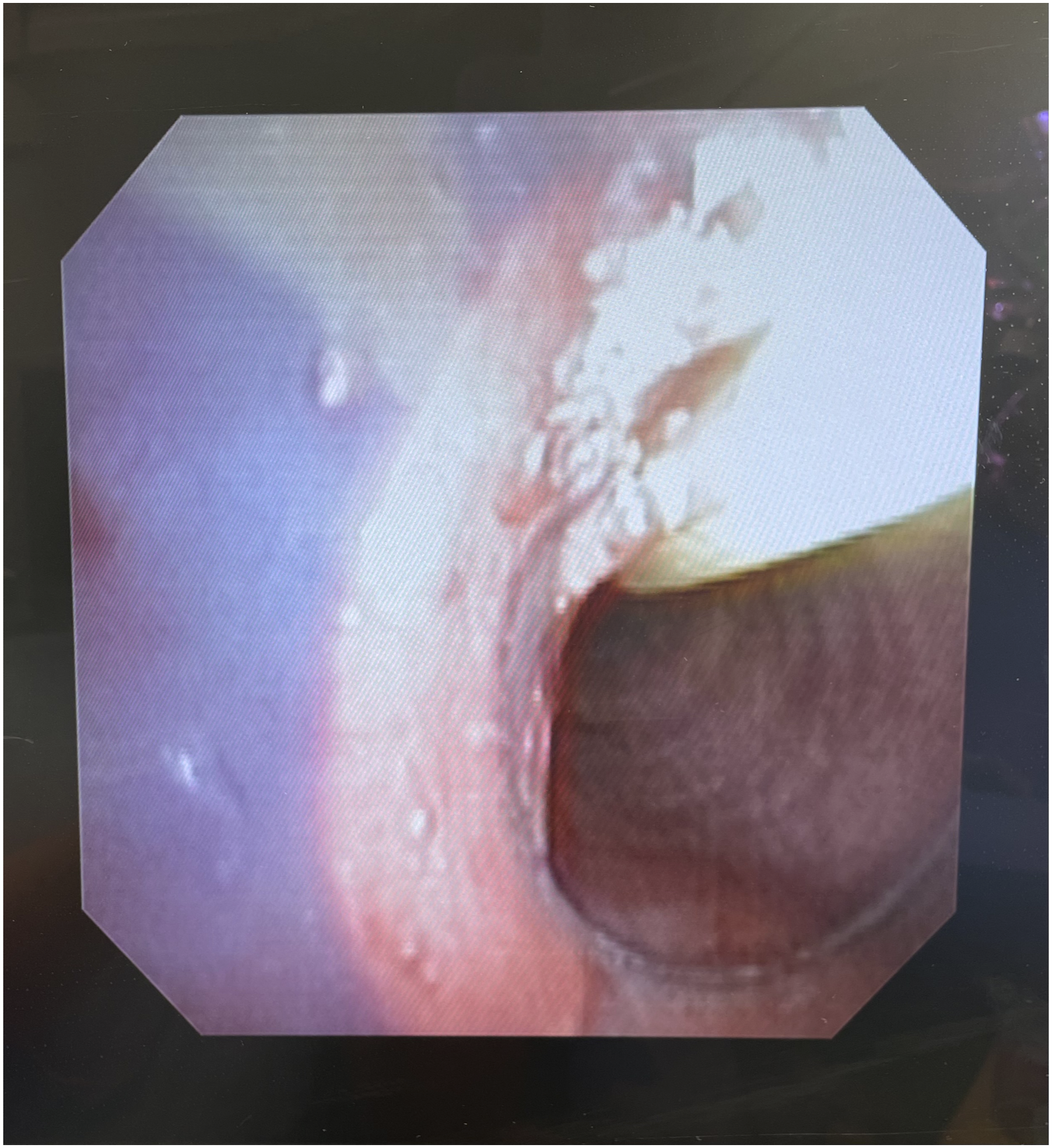
Discussion
Allowing for adequate surgical exposure during video-assisted or robotically assisted thoracoscopic surgery is considered one of the absolute indications for establishing OLV. DLTs are often considered the gold standard for lung isolation, but as this case highlights, there are certain conditions under which a DLT may not be effective. Inappropriately small DLTs are one potential cause of this failure, but the use of a 41 Fr DLT in this case makes this explanation unlikely. Instead, it is more likely that bronchomalacia led to recurrent displacement of the bronchial lumen into the trachea upon cuff inflation. Since the risk for airway injury increases with multiple attempts of DLT repositioning, higher cuff volume/pressure, and excessive angulation of the bronchial lumen impinging on the tracheal wall with the advancement of the DLT, the decision was made to place an EZB through the DLT as an alternative means for obtaining OLV.7-9 Alternatively, there was consideration for exchanging the DLT for an SLT plus EBB combination. However, in our scenario, the patient was already in lateral decubitus position with the procedure underway, and exchanging the DLT under such circumstances posed additional risks, including tracheobronchial rupture (due to further manipulation of the airway) or loss of the airway entirely.
The unique Y-shaped distal end of an EZB typically separates after exiting the ETT approximately 3–4 cm, and the goal is to place 1 cuff in the right mainstem bronchus and the other cuff in the left mainstem bronchus concurrently. When one of the balloons is inflated, this orientation allows for ipsilateral lung isolation. In our case of EZB insertion through a 41Fr left-sided DLT, the DLT was withdrawn until the tip of the bronchial lumen was approximately 3–4 cm proximal to the carina. However, in our case, there was difficulty placing the EZB in the correct orientation with 1 limb sitting in each of the left and right mainstem bronchi. Therefore, to effectively isolate the right lung, we were able to utilize the EZB in a manner similar to that used for lung isolation in the context of a tracheal bronchus, with 1 limb of the EZB sitting in the bronchus intermedius and the other limb in the right upper lobe bronchus. 6 To facilitate both limbs of the EZB entering the right mainstem, the DLT was rotated 180°, so the angulation of the distal bronchial limb of the DLT was directed towards the right mainstem bronchus. The EZB was placed down the bronchial limb (Figure 1) and advanced into the right mainstem bronchus. Once both balloons were advanced past the carina into the right mainstem bronchus, the EZB was rotated, so 1 limb of the EZB was positioned in the right upper lobe bronchus and the other placed in the bronchus intermedius. Both balloons of the EZB were inflated under FOB surveillance (Figure 2). As the distal airways are narrower than the more proximal airways, it is particularly important to inflate the balloons in this position under visualization, as less air is required than usual to obtain an adequate seal (5–7 mL vs 9–10 mL), 6 and excessive inflation may increase the risk of cuff herniation or bronchial injury. Although not attempted at the time, it may have been possible to achieve a similar EZB configuration by instead placing the EZB through the tracheal lumen of the DLT without having to withdraw the bronchial lumen from the left mainstem bronchus.
Fortunately, both the tracheal and bronchial limbs of a DLT use a standard 15 mm ETT connector, which fits to an EBB multiport to facilitate the passage of an EBB. Although the internal diameter of a 41 Fr DLT lumen is less than the EZB manufacturer’s recommendation of using a 7.0 mm ETT or larger, we found this to be a non-issue.10,11 Ex vivo mock-up showed that both a smaller 3.8 mm FOB and EZB can fit through the bronchial lumen of a 35 Fr DLT. Typically, in the case of a smaller SLT, this would lead to issues with increased ventilator pressure requirements to maintain adequate ventilation. However, when employing an EBB through a DLT, the additional lumen remains unobstructed, and the ventilator can be attached to the unobstructed lumen to provide ventilation. If a larger FOB/smaller DLT combination is used, the EZB can be placed in the bronchial lumen when it is positioned above the carina, and the FOB can be placed through the tracheal lumen. It is important to note that with the ventilator circuit attached to the tracheal limb of the DLT, the side port of the EZB adapter remains open, creating a potential circuit leak. Here, a DLT adapter can be connected and clamped to close the circuit, as was performed in our case (Figure 3). Intraoperative configuration of the Rüsch EZ-Blocker and 41Fr left-sided double-lumen endotracheal tube. The ventilator circuit is attached to the tracheal lumen. The bronchial blocker multiport adapter is connected to the bronchial lumen, with the clamped double-lumen tube adapter attached to the side-arm to occlude it.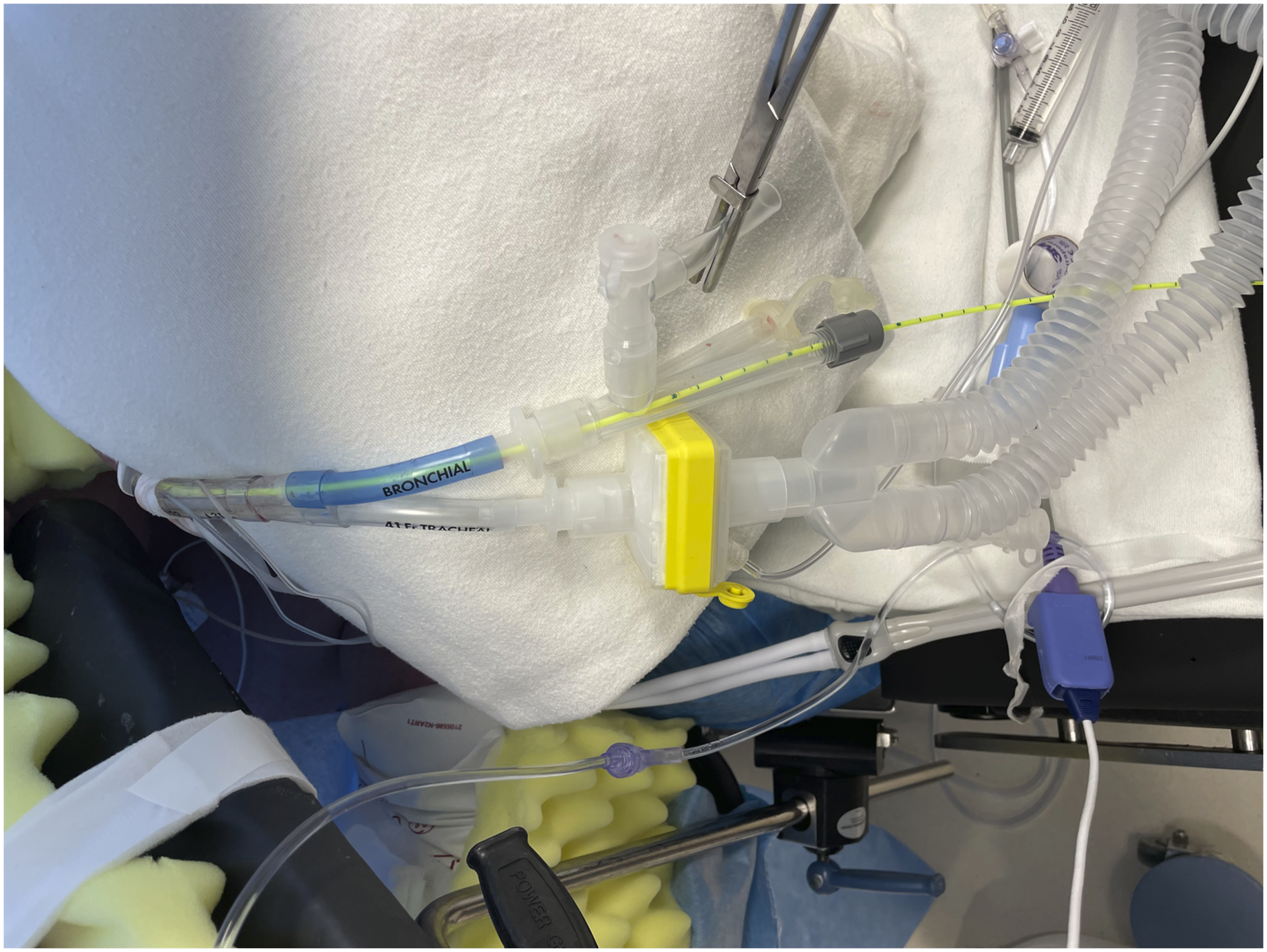
It should be noted that at the authors’ institution, the EZB is the primary EBB of choice when selecting an EBB for lung isolation. The authors suspect that it is also possible that adequate lung isolation could have been obtained using a single-balloon EBB, such as the Arndt or Cohen EBB (Cook Medical, Bloomington, IN), through the DLT.
Utilizing a DLT as a SLT for the purpose of EBB placement allows for an additional method of establishing OLV in situations where a DLT was initially placed, but OLV is, or becomes, inadequate during the surgical procedure, and in which exchange of the DLT is deemed too risky to attempt. Our case highlights one such example, but another potential situation where this may arise is if the bronchial cuff ruptures and can no longer maintain adequate seal for lung isolation.
Conclusions
Maintaining airway control is critical during surgery, but especially during OLV. Although the DLT may be considered the gold standard for establishing OLV by some anesthesiologists, there are certain conditions in which the use of a DLT fails or is unavailable. Therefore, the authors contend that anesthesiologists who perform thoracic anesthesia regularly should be familiar with multiple methods of obtaining OLV.
Footnotes
Acknowledgements
The authors acknowledge that AI bots, such as ChatGPT, or other AI-generated material WAS NOT utilized during the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael K Essandoh is a consultant for Boston Scientific and S4 Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors have obtained verbal and written informed consent from the patient for the publication of this case report.