
Abstract
Preoperative cardiac evaluation is a cornerstone of the practice of anesthesiology. This consists of a thorough history and physical attempting to elucidate signs and symptoms of heart failure, angina or anginal equivalents, and valvular heart disease. Current guidelines rarely recommend preoperative echocardiography in the setting of an adequate functional capacity. Many patients may have poor functional capacity and/or have medical history such that echocardiographic data is available for review. Much focus is often placed on evaluating major valvular abnormalities and systolic function as measured by ejection fraction, but a key impactful component is often overlooked—diastolic function. A diagnosis of diastolic heart failure is an independent predictor of mortality and is not uncommon in patients with normal systolic function. This narrative review addresses the clinical relevance and management of diastolic dysfunction in the perioperative setting.
Keywords
Introduction
Preoperative cardiac evaluation is a cornerstone of the practice of anesthesiology. This consists of a thorough history and physical attempting to elucidate signs and symptoms of heart failure, angina or anginal equivalents, and valvular heart disease. Current guidelines rarely recommend preoperative echocardiography in the setting of an adequate functional capacity (>4 METS)1,2; however, many patients may have poor functional capacity and/or have medical history such that echocardiographic data is available for review. Much focus is often placed on evaluating major valvular abnormalities and systolic function as measured by ejection fraction, but a key impactful component is often overlooked—diastolic function. A diagnosis of diastolic heart failure is an independent predictor of mortality3,4 and is not uncommon in patients with normal systolic function.3,5 This narrative review addresses the clinical relevance and management of diastolic dysfunction (DD) in the perioperative setting.
Epidemiology
We must first distinguish heart failure with preserved ejection fraction (HFpEF) (patients with clinical signs and symptoms of heart failure, but with normal systolic function) from the pathophysiology of DD (patients with abnormalities in ventricular relaxation or compliance). While HFpEF implies symptomatology, DD is the underlying pathology which leads to the degree of heart failure symptoms.6-8 Unfortunately, DD is becoming a more prevalent perioperative concern, as evidenced by epidemiologic data from the Framingham Heart Study (FHS). 9 The incidence of heart failure with reduced ejection fraction (HFrEF) is declining, while that of HFpEF is rising due to the increasing prevalence of underlying causes. 9 In fact, about half of all new cases of heart failure in the United States consist of HFpEF and this proportion has been rising over time. 9 Other analyses of the FHS and Cardiovascular Health Study (CHS) yielded similar conclusions that HFrEF is on the downturn, but HFpEF is rising, particularly in men. 10 Furthermore, when evaluating patients for DD the higher the grade, the greater the mortality impact. 3 Al-Jaroudi et al found a hazard ratio (HR) of 3.58 for mortality for patients progressing from normal diastolic function to any degree of DD and a HR of 2.13 for patients who progressed from mild to either moderate or severe disease. Any worsening of DD had a mortality HR of 1.78. 3 Overall heart failure incidence remains elevated, along with risk of heart failure-related mortality, and even reduced 5 year survival.3,10,11 These studies suggest that as anesthesiologists, we will increasingly face the challenges of managing this highly morbid disease process in the operating room.
Perioperatively, the impact of DD is just as profound. In the cardiac surgical population, severity of DD is a predictor of early mortality and recurrence of mitral regurgitation after mitral valve surgery. 12 Early operative therapy, prior to the development of DD, can prevent myocardial dysfunction in patients with mitral regurgitation. 12 Interestingly, LV diastolic function worsens immediately after coronary-artery bypass grafting (CABG) surgery but returns to baseline within 6 months.12,13 Severe DD has also been shown to predict respiratory complications and increased length of hospital stay in off-pump CABG. 14 DD has been shown to increase the rate of perioperative adverse events and heart failure exacerbations in vascular surgery and also be associated with primary graft dysfunction after lung transplantation.15,16 Overall, the profound impact of DD on perioperative mortality has been shown in a wide variety of cardiac, vascular, and transplant patients and should therefore be well understood by the perioperative consultant physician.16-21
Pathophysiology
The underlying etiologies responsible for the development of DD are complex and varied, all resulting in alterations in the rate of relaxation and intrinsic compliance of the ventricle. These changes limit ventricular filling, and therefore stroke volume and cardiac output. At a more cellular level, much of the scientific evidence points to an underlying theme of excessive inflammation. Metabolic disturbances such as obesity, diabetes, anemia, hypertension, and renal insufficiency all produce systemic inflammatory states. 22 This “Metabolic-Risk”–associated inflammation results in microvascular endothelial dysfunction due to oxidative stress and nitric oxide imbalance, which alters myocardial oxygen consumption.23-25 Over time, this pro-inflammatory imbalance increases the production of myofibroblasts responsible for collagen deposition in the myocardial extracellular matrix, resulting in reduced passive compliance of the ventricular wall.6,24 Both of these collagen alterations as well as changes in titan, an important protein responsible for cardiomyocyte stiffness, cause profound changes in ventricular cavity compliance. 26
In addition to systemic inflammation, other etiologies have been linked to changes in diastolic function. Ischemic changes, toxic necrosis, or trauma may also result in similar, though differently mediated, sterile inflammation to the ventricular myocardium. In this setting, the inflammatory state results from the pathogen recognition receptor, intracellular cytokines, and cluster of differentiation 36 receptor activation. 27 These complex cell-signaling pathways recruit neutrophils, monocytes, and lymphocytes which result in phagocytosis of damaged cells, scar formation, and cardiac remodeling, respectively.28-31 Viral myocarditis can likewise cause similar changes in myocardial substrate leading to deteriorations in both systolic and diastolic function. 32
This pathologic cascade, regardless of the precise cause, results in a sequential degradation of the two major components of diastolic function: relaxation (active) and compliance (passive). 33 Beginning in mid-systole, the contractile elements of the myocardium are deactivated. This energy-consuming process continues through the first third of the diastolic filling phase. 34 The rate at which this oxygen-dependent process occurs dictates the amount of ventricular filling that occurs during the early rapid filling phase. 33 Impairments in this process will slow the rate of relaxation and therefore limit filling during the early phase of diastole, leaving residual volume in the atrium. The atrial contraction that follows generally compensates for this limited filling until further disease progression to more advanced diastolic dysfunction occurs. 33 This abnormality in relaxation generally precedes systolic dysfunction and is commonly the earliest manifestation of DD, often due to coexisting pathologies. 33
Chamber compliance is a passive property of the left ventricle which is appreciated throughout the entirety of the diastolic phase. 35 The aforementioned changes in titan and collagen result in significant changes to this intrinsic property of the myocardium, reducing compliance and increasing stiffness. 26 Compliance can be described using pressure-volume relationships. As chamber stiffness increases, the pressure-volume curve shifts leftward and upward indicating the requirement for higher filling pressures to achieve smaller end-diastolic volumes.26,33,36,37 Over time, this curve shift results in increased end-diastolic and left atrial pressure, eventually leading to pulmonary edema if left unchecked. 26 This helps partially explains the exercise intolerance often seen in patients with heart failure due to diastolic dysfunction. The stiff ventricle is unable to fill properly despite increased filling pressures, which results in limited stroke volume and cardiac output. Increasing heart rate will only serve to limit diastolic time and therefore limit ventricular filling, further decreasing stroke volume 37 and exercise tolerance. This may go unnoticed at rest, but the inability to increase cardiac output in response to demand results in the exercise intolerance often seen in these patients. 26
No matter the inciting pathology, impairments in diastolic function largely relate to states of chronic inflammation which lead to microvascular changes, alterations in oxygen utilization and extracellular matrix composition.6,22-26 These changes first impact the rate of ventricular relaxation, an oxygen and energy-consuming process. Over time, myocardial stiffness increases leading to increased left atrial pressure and limiting ventricular filling, resulting in pulmonary edema and exercise intolerance, respectively. The progression of these processes has been well described to classify the stages of DD which follow the longitudinal course of pathophysiology described above.
Diagnosis and Grades of Diastolic Dysfunction
Grading of diastolic function is complex, particularly in a dynamic intraoperative environment. Using echocardiography, a combination of 2-dimensional (2D), Doppler blood flow and tissue Doppler measurements can be used to determine the grading and severity of most patients in the operative setting. The American Society of Echocardiography (ASE) has published comprehensive recommendations for the evaluation of left ventricular diastolic function using echocardiography. However, the guidelines expressly state that the “guidelines are not necessarily applicable in the perioperative setting.” 38 We encourage the reader of this review to do so with caution.
The age of the patient should be considered, since LV relaxation slows with aging. 38 Normal filling patterns in the elderly may resemble those considered to be mild diastolic dysfunction in a younger patient. Certain other indices are far less age dependent, such as the E/e’ ratio, which is almost never >14 in a normal individual. Left atrial enlargement in the absence of chronic atrial arrhythmia is often a marker of chronically elevated left atrial pressure (LAP), and significant LV hypertrophy is usually associated with an increase in LV stiffness and diastolic dysfunction. 38
It is extremely important to note that the presence of a single measurement that falls within the normal range for a given age group does not indicate normal diastolic function. None of the measurements should be taken in isolation. Indices of diastolic function need to be interpreted in the wider context of clinical status, 2D, and Doppler parameters. These algorithms are not 100% accurate in the perioperative environment compared to the outpatient echocardiography setting and rapidly changing hemodynamic conditions may alter the results. 38 While preoperative echocardiographic data may often be available and helpful in assessing the patient’s diastolic function while awake, it may at times be helpful to evaluate these markers intraoperatively using the following data.
Echocardiographic Modalities
The ASE recommends the evaluation of four variables in the assessment of diastolic function. These are the annular e’ velocity measured with tissue Doppler, the E/e’ ratio, the maximum left atrial volume index, and the peak tricuspid regurgitation (TR) velocity. Abnormal cutoff values are a septal annular e’ velocity < 7 cm/sec, a lateral annular e’ velocity <10 cm/sec, an average E/e’ ratio >14, a maximum LA volume index >34 mL/m2, and a peak TR velocity >2.8 m/sec. The average E/e’ ratio is recommended for simplification. At times, only the lateral or the septal velocity is available, and in these circumstances a lateral E/e’ ratio >13 or a septal E/e’ >15 is considered abnormal. If more than half of the available variables do not meet abnormal criteria, then LV diastolic function is considered to be normal. LV diastolic dysfunction is abnormal if more than half of the variables meet abnormal criteria. If exactly half of the variables do not meet cutoff values, then the study is inconclusive. 38
Traditionally, assessment of LV filling has started with the assessment of the diastolic blood flow pattern through the mitral valve using pulsed wave Doppler (PWD). During ventricular relaxation, flow across the mitral valve is determined by the LA-LV pressure gradient and the lusitropic properties of the LV. As previously mentioned, the earliest manifestations of diastolic dysfunction typically present as abnormalities of the active relaxation phase of diastole. Initially, these present as decreases in E wave peak velocity and prolonged deceleration time (DT). As LV compliance worsens, distinct echo patterns of normal, impaired relaxation, pseudonormal, and restrictive LV filling patterns have been described. Deceleration time (DT) shortens as LV compliance worsens in the more advanced stages of diastolic dysfunction. 39
In the operating room, these measurements should all be made during apnea and normal sinus rhythm. Optimal parallel alignment of Doppler beams for the interrogation of diastolic function using TEE is obtained using the midesophageal (ME) 4-chamber and ME long-axis views. A focused TEE assessment of diastolic function should include a combination of PWD (trans-mitral and pulmonary venous flows) and Doppler tissue imaging (DTI). 39 A sample volume of 1 to 3 mm is placed between the mitral leaflet tips during diastole with a sweep speed set between 50-100 mm/sec. Measurements to be obtained include the peak E and A velocities, the E/A ratio, DT, and A-wave duration (Adur). It is critical the perioperative echocardiologist realizes that trans-mitral flow (TMF) provides value only when used in combination with other Doppler variables such as pulmonary venous inflow (PVF) and DTI. TMF by itself is far too load-dependent to reliably provide useful information on diastolic function by itself. 39
Measurement of high amplitude, low velocity tissue motion helps in the assessment of diastolic function. Using the DTI preset, a 5–10 mm sample volume is placed in the lateral or medial mitral annulus in a ME 4-chamber view to obtain a PWD pattern. Acquisition should be at end-expiration at a sweep speed of 50–100 mm/sec. An average of 3 beats of the lateral mitral annulus should be obtained. Typically, the DTI signal consists of 3 main waves. An early (e’) and late (a’) diastolic wave, and a systolic (s’) wave. The DTI e’ wave indicates myocardial relaxation while the DTI a’ wave indicates late LV inflow and atrial contraction. In the case of regional LV dysfunction and wall motion abnormalities, it is essential to average the septal and lateral mitral annular measurements. 39 Mitral annular calcification, regional wall motion abnormalities or the presence of a mitral ring or prosthesis will render the DTI readings uninterpretable.
Trans-mitral PWD assessment of diastolic function can be further refined by measurement of pulmonary venous PWD tracings. In an ME view, a 2–3 mm sample volume is placed at 1 cm depth usually in the left upper pulmonary vein. Wall filters are set low to allow for the acquisition of the atrial reversal (Ar) wave. The peak S and D waves, the S/D ratio, and the Ar peak velocity and duration should all be measured. Atrial arrhythmias can be a limiting factor in obtaining the PVF tracing. Reversal of forward flow in the pulmonary veins occurs during atrial contraction causing the Ar wave. Comparing the duration of this wave to the mitral inflow A wave (Ar > A greater than 30 msec) has been associated with increased left atrial pressure. 38 Likewise, a comparison of the flow during systole to the flow during diastole can also be useful in evaluating for high LAP. High left atrial pressure for any reason (DD, mitral regurgitation, mitral stenosis, etc.) inhibits inflow during systole, causing an S wave which is less prominent than the D wave. 38 This information, in concert with the aforementioned measures can be very useful in assessing the patient’s LAP and severity of DD.
Grading Diastolic Dysfunction
All measurements should be performed during periods of apnea and relatively stable hemodynamics to minimize the effects of hemodynamic changes on diastolic parameters. Measurements should be made multiple times to eliminate significant outliers.
39
A workflow process should start with TMF and then continue in a stepwise fashion to incorporate information from the DTI of the mitral annulus and PVF (Figure 1). Left ventricular filling pressure (LVFP) may be estimated using ratios of various peak velocities to help further develop the assessment of diastolic function; however, the accuracy of these measurements has come into question and the systolic function of the LV needs to be considered when estimating LVFP.39,40 A step-wise approach to perioperative assessment of diastolic function 326 x 85 mm (72 x 72 DPI).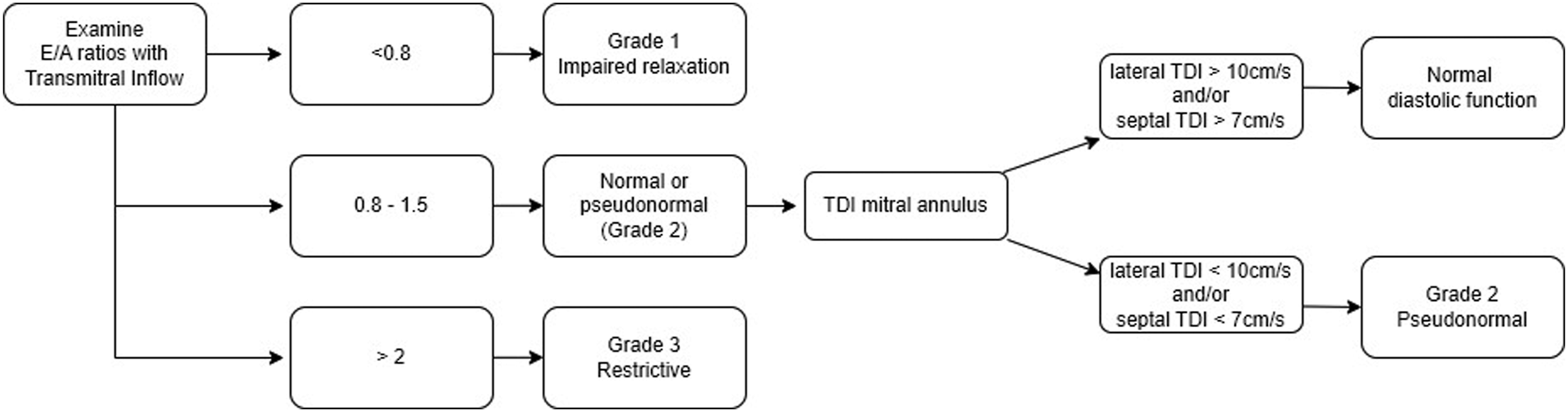
Patients with normal diastolic function typically show E wave predominance (E/A ≥.8) of TMF, indicating the majority (∼80%) of LV filling occurs during early diastole. There is systolic predominance of PVF (S/D >1), and normal DTI values >7 cm/s and >10 cm/s for the septal and lateral annuli respectively. 38 Normal diastolic function can therefore quickly be identified in patients with normal systolic function and normal DTI values. 41
For patients with depressed EF (<50%), the assessment should also start with PWD of the TMF. A peak E velocity <50 cm/s or E/A ratio <1 suggest normal LAP while E/A >2 or a DT <160 ms is diagnostic of increased LAP. Should the TMF E/A ratio lie between 1 and 2, then further workup using DTI (e’) and PVF (S/D ratio, Adur, and Ar duration) needs to be employed. E/e’ (>15) can be used for prediction of increased filling pressures. Likewise, Ar duration longer than A (>30 ms) suggests elevated filling pressure. 39
The approach for determination of LVFP in patients with normal systolic function is somewhat different. It starts by examination of the E/e’ ratio. A ratio >13 indicates elevated LVFP, whereas a ratio <8 suggest normal LVFP. Ratios between 9 and 13 require use of other Doppler variables. Ar-Adur > 30 ms is also suggestive of elevated LVFP. 39 It is interesting to note that assessment of diastolic function is more reliable in the setting of systolic dysfunction. However, regardless of the EF, E/e’ <8 and E/e’ >13 to 15 separate normal from increased LVFP.
Grade I (impaired relaxation) is considered the initial stage of diastolic dysfunction. Typically, there is a decrease in the E wave velocity and prolongation of the DT >220 ms due to a delay in early relaxation. The A wave increases in a compensatory manner due to residual atrial blood volume, and the result is an E/A ratio <1. The typical PVF pattern shows an S/D ratio >1, e’/a’ will be < 1. 39 Most patients with lateral e’ velocity <8.5 cm/s also have impaired relaxation. It should be noted that the left atrial pressure remains normal at this stage.
As the process of myocardial dysfunction and relaxation abnormalities worsen, the LV remodels resulting in a worsening of LV compliance. This noncompliant ventricle requires increased filling pressures, resulting in an increased LVEDP and an increase in LAP. Increased LAP overcomes the impairment in LV relaxation which enhances early diastolic filling, thereby increasing the E wave velocity as pressures equalize between the LA and the LV, returning the TMF E/A ratio to normal. Here, though, the LAP provides the driving force for early LV filling, rather than ventricular relaxation. Compliance may still be normal at this stage. Due to the normal appearance of TMF, this phase is referred to as a “pseudonormal pattern,” with E/A ratio (E/A >1) using TMF and a shortened DT. 39 The next phase, Grade III (reversible restrictive) diastolic dysfunction, is characterized by an increased E velocity and shortened DT on TMF. PVF is marked by an S/D ratio <1, and DTI is marked by an e’/a’ <1 consistent with high LAP. 39 Further disease progression to Grade IV (fixed restrictive) occurs over time with further worsening of LV compliance and extremely high LAP. It is characterized largely the same echocardiographic parameters with the E:e’ ratio of >15, rather than >13 for Grade III, but without the ability to decrease the LAP with maneuvers that reduce preload.
One of the challenges in assessment of diastolic dysfunction using TEE becomes differentiation of normal from “pseudonormal” filling. Various methods including preload reduction with nitroglycerin and Valsalva maneuvers have been described to alter the LAP and look at changes in the TMF. Unfortunately, the utility of these changes is questionable. 39 However, the increases in LAP should result in abnormal PVF and DTI which would lead the echocardiologist to the correct diagnosis despite a normal-appearing TMF. 41
Several caveats to the assessment of diastolic function are noteworthy. Interpretation of E/A and S/D require sinus rhythm. Additional LV filling, such as from aortic insufficiency or mitral regurgitation, affects LVEDP and therefore both the E/A and the S/D ratios. Increased preload will revert impaired relaxation to a pseudonormal pattern and vice versa. A brief Valsalva maneuver may unmask this preload compensation. 39 Furthermore, the ASE guidelines recommend evaluating TR velocity in the assessment of diastolic dysfunction. While this may be useful, other causes of elevated RVSP in the perioperative, anesthetized state may impact its interpretation. 38
Swaminathan et al report on the use of a simplified algorithm for grading diastolic dysfunction in patients after CABG. 42 Their algorithm, based on retrospective data from 905 patients, demonstrated a higher percentage of patients being assigned a grade of diastolic dysfunction (99% using the simplified algorithm vs 62% using the control algorithm). In their study, worsening grades of DD were clearly associated with major adverse cardiovascular events as demonstrated by worse event-free survival through 60 months of follow-up. In their simplified algorithm which is yet to be externally validated despite being widely adopted in practice in the cardiac anesthesia community, diastolic dysfunction was graded based exclusively on the e’ velocity (less than or equal to 10 cm/s) and the transmitral E/e’ ratio. 43 This approach, while simplified, highlights the incredible clinical importance of assessing diastolic function as it pertains to perioperative morbidity and mortality.
For the perioperative echocardiologist, it is important to note that the above-mentioned criteria are based on transthoracic echocardiography (TTE) performed in the outpatient setting, and may not be entirely applicable to the use of TEE in the operating room. 39 Positive pressure ventilation and use of general anesthesia radically change cardiac loading conditions compared to the awake ambulatory patient. The intraoperative hemodynamic state is constantly changing and any isolated Doppler measurement represents only one snapshot in time. Left atrial size and volume is not well assessed using TEE as the entire left atrium frequently cannot be fit in the image’s sector. Hence, its use in the assessment of diastolic function using TEE is not feasible. 44 Rigid application of the ASE guidelines to intraoperative TEE has demonstrated limitations in the classification of diastolic dysfunction; 43 however, important insights into the patient’s LAP and preload status may be gleaned from this information.
Perioperative Management
In the perioperative setting, patients can be thought of as having either severe or non-severe disease (Figure 2). Patients with mild disease include those with Grade I and II DD while those with severe disease include those with Grade III and IV. Among those with non-severe disease, patients with grade I diastolic dysfunction (DD) have clearly defined goals of care. Most importantly, these patients need the active atrial contribution to their ventricular filling during diastole due to the delayed relaxation and E/A <1. In other words, maintaining normal sinus rhythm (NSR) is incredibly important. Aggressive fluid resuscitation is needed to help overcome the impaired relaxation of the left ventricle.
43
Patients with Grade II DD (pseudonormal pattern) are more challenging to manage. While these patients will be less sensitive to the loss of atrial kick, they are more sensitive to fluid status and can have dynamic physiology. If these patients receive too little fluid, they will behave like patients with Grade I dysfunction. If they are volume overloaded, they may progress to physiology consistent with Grade III dysfunction. Underlying causes of diastolic dysfunction and its perioperative management. 356 x 275 mm (300 x 300 DPI).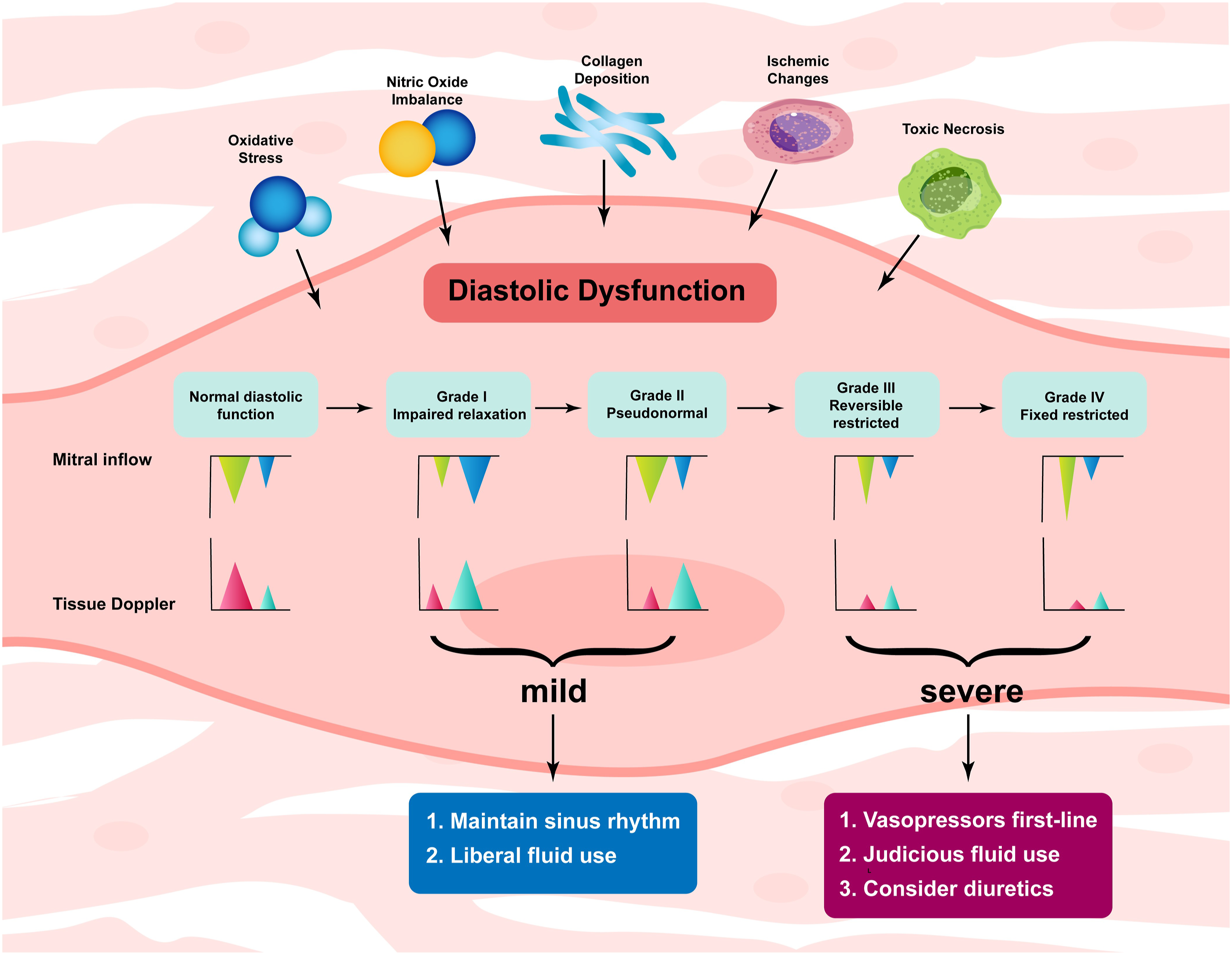
Patients with grade III and IV DD should be classified as having severe disease, albeit the rarest presentation of the disease. 45 These patients are at high perioperative risk due to the persistently elevated left atrial pressures. Fluid overload and hemodynamic instability make these patients susceptible to pulmonary edema, post-capillary pulmonary hypertension, and right ventricular systolic dysfunction. 43 In high risk surgical procedures with potentially large fluid shifts either intraoperatively or postoperatively, these patients should be carefully monitored with invasive monitoring and/or echocardiography. Instead of volume as first line treatment of hypotension in these patients, vasopressor and/or inotropic therapy may be indicated; as these patients may, but not always, present with combined systolic and diastolic dysfunction. 45 Likewise, many inotropes also bring a positive lusitropic effect as well, which may enhance ventricular relaxation and decrease left atrial pressures.46,47 Vasoconstriction may help reduce vascular capacitance and thereby shift volume into the circulation without adding exogenous fluid that is likely to be unnecessary for these patients undergoing most procedures. In fact, diuretic therapy may have a beneficial effect by shifting the pressure-volume relationship toward normal. 48 Similarly, preload-reducing maneuvers such as Valsalva, Reverse Trendelenberg position, or nitroglycerin administration may be effective in reducing left atrial pressures and revert echocardiographic measures back to a “pseudonormal pattern.” 38
Perioperative Monitoring
Arterial Blood Pressure
Traditional indications for invasive arterial blood pressure (BP) monitoring include anticipated hypotension or acute changes in BP, frequent repeated blood gases, and end-organ disease requiring close monitoring. 49 As such, while it may not be readily apparent, an arterial line for monitoring BP may be indicated in severe diastolic dysfunction to assess end-organ perfusion and indirectly volume status for more complex cases that involve large fluid shifts.
Central Venous Catheter
Central venous access is classically indicated for the administration of caustic medications that cannot be administered peripherally, such as vasopressors and inotropes, monitoring, and vascular access. 50 It is a poor monitor, both as an absolute value and as a trend, to predict fluid responsiveness,50,51 which is a key aspect in the management of patients with diastolic dysfunction. It may be necessary, depending on the surgical procedure, to administer longer-term, higher dose vasopressors or inotropes or for vascular access; however, for shorter duration and under close observation, peripheral administration of vasopressors may be appropriate without additional complication. 52 In short, the authors see little value is placing a central line, which is itself not without risk, to guide the perioperative management of patients with DD.
Pulmonary Artery Catheter
The use of a pulmonary artery catheter (PAC) as a monitoring device continues to be extensively debated in the literature.53-56 As it relates to the discussion regarding its use for the perioperative management of the patient with DD, despite our extensive literature search, we could not find any publications regarding this topic. Much of the criticism of the use of a PAC is that is does not alter outcomes; however, often times it is used as a salvage or rescue therapy which may largely skew not only the data but individual clinician perception. We feel that in the proper circumstances, a PAC may be indicated perioperatively, particularly in patients with severe DD. A PAC can help assess volume responsiveness 57 by allowing serial measurements of cardiac output after an intervention and provides the managing physician with data to guide inotrope and pressor selection. Another fault of the use of PAC in the literature has been the misinterpretation of the data 58 ; that said, if you are not comfortable with placing, using and interpreting a PAC, we would discourage its use.
Echocardiography
Echocardiography is necessary to grade and diagnose DD as we have reviewed. As a monitoring tool, it is likely the single best tool to help the perioperative physician manage DD. As a monitor of volume responsiveness, it is superior to measurements obtained from a PAC in critically ill patients, 57 allowing tailored patient care. Mitral inflow patterns as well as 2-dimensional measurements of left ventricular end diastolic area predict cardiac output changes. 59 A preoperative evaluation may be done using transthoracic echocardiography (TTE). Transesophageal echocardiography utility intraoperatively may be limited depending on the operation; procedures causing large volume shifts typically will involve the chest or abdominal cavity, making TTE difficult. Transesophageal echocardiography may be the preferred modality. Not only can this help guide volume administration and help the clinician answer the questions often asked “Do I need more volume? Have I given enough?” but it allows for an ongoing, real-time assessment of diastolic function based on dynamic changes in pre-load, after-load, and lusitropy. We would recommend the use of TEE in patients with severe disease undergoing complex cases that are expected to causes large volume shifts.
Choice of Anesthetic Technique
Many clinicians may wonder whether avoiding general anesthesia and employing neuraxial and/or regional anesthetic techniques can help improve outcomes in patients with DD. The short answer is we simply don’t know; there is no literature to support any guidance on this topic. However, we can make some reasonable assumptions and conclusions based on what we do know. Patients with poor functional capacity are at higher risk under general anesthesia. 60 We would surmise that patients with severe DD should be considered for alternative techniques, if possible, to avoid the impact of induction, positive pressure ventilation, the myocardial depressant effect of anesthetics used for maintenance of anesthesia and the potential for arrhythmogenic neuromuscular blockade reversal agents.
Patients with DD may have comorbidities, such as coronary artery disease or atrial fibrillation, that require systemic anticoagulation and we would encourage the clinician to be diligent in the review of medications and if they should be stopped to facilitate the perioperative plan.
Conclusion
Diastolic dysfunction is not just an esoteric concept found within the cardiology literature. It is a complex and expanding healthcare problem that can create substantial clinical challenges for the anesthesiologist in the perioperative setting. The confusing juxtaposition of volume responsiveness in low-grade disease and volume restriction in severe disease often poses a dilemma. A detailed understanding of the pathophysiology, diagnostic criteria, and perioperative management strategies is critical to providing optimal patient care while future research into outcomes associated with diastolic dysfunction in more surgical patient populations is needed.
Footnotes
Acknowledgments
We would like to thank Tatyana Starikova Harris, Illustrator and Designer, of www.Tatyana-Starikova.com for her assistance in creating ![]() .
.
Declaration of Conflicting Interests
The authors have no conflicts of interest with the information presented in this manuscript.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This research has been supported by a grant from the Department of Anesthesiology and Perioperative Medicine, Penn State Hershey Medical Center.