
Abstract
Congenital cardiac patients who received neonatal reconstructive aortic arch surgery are at risk of aortopulmonary space narrowing with compression of the left pulmonary artery and left main bronchus (LMB) later in life. We discuss a challenging adolescent single ventricle patient who presented for surgical treatment of a non-idiopathic thoracic scoliosis (posterior spinal fusion) with severe stenosis of the LMB and left pulmonary artery due to a narrow aortopulmonary space. Careful preoperative imaging, evaluation, and decision making resulted in successful surgical treatment and uneventful perioperative course.
Keywords
A 17-year-old male was followed during adolescent growth for a non-idiopathic (congenital heart disease and sternotomy at infantile age) thoracic scoliosis at the Wilhelmina Children’s Hospital, Utrecht, the Netherlands. The right convex primary thoracic curve (apex at spinal level T8-9) progressed from 35 to 58° with a compensatory thoracolumbar curve of 32° in the coronal plane and he was hypokyphotic in the sagittal plane. Posterior spinal fusion was advised to the patient because of high risk of curve progression with progressive reduction of his exercise capacity. At the same institution, he was treated and followed by his pediatric congenital cardiologist for tricuspid atresia with a functionally univentricular heart, transposition of the great arteries, and interrupted aortic arch. At neonatal age, he underwent cardiac surgery involving a Damus–Kaye–Stansel procedure with central shunt placement followed by a partial cavopulmonary connection (PCPC) at 4 months of age. His palliative surgical trajectory was finalized at the age of 2 (according to our institutional practice) with a total cavopulmonary connection (TCPC) procedure including placement of an 18 mm extracardiac conduit (without a fenestration). At the age of 7, he underwent a heart catheterization for unexplained fatigue during which a stent was placed in the LPA to treat LPA stenosis. Due to the relation between the LPA and left main bronchus (LMB), despite ovalization of the stent, some stenosis of the LPA remained and external compression by the aorta and LPA led to narrowing of the LMB. Recent spirometry showed a peak expiratory flow (PEF) 38%, a 1-second forced expiratory volume (FEV1) 43%, a total lung capacity (TLC) of 81% predicted with signs of severe air trapping. A high-resolution in- and expiratory computed tomography (HRCT) and angiography of the thorax demonstrated severe compression of the LMB at the level of the LPA stent (Figure 1) with air trapping of the complete left lung, signs of reduced blood flow through the left lung, as well as some air trapping in the right inferior lobe due to the relative intrusion of the spine into the right hemi-thorax. This is also illustrated in online video content (Online Movie 1). Computed tomography angiography with transverse and sagittal view of the chest showing severe malacia of the left main bronchus and its anatomical relation with the ascending (*) and descending (†) aorta, the left pulmonary artery stent (‡), and the spine. Narrowing of the aortopulmonary space in a Fontan patient presenting with a thoracic scoliosis.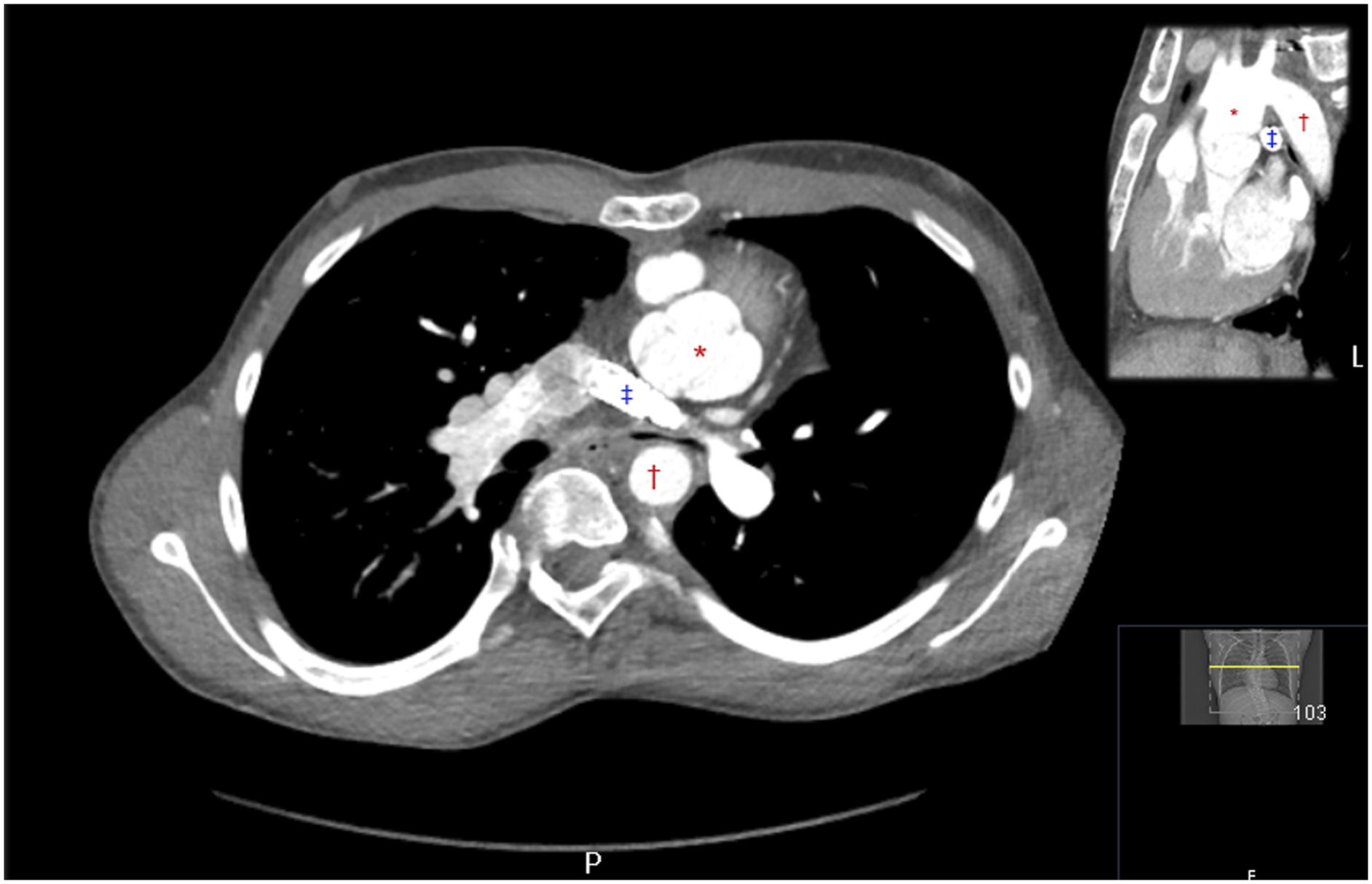
Clinical Challenge
Severe LMB compression with air trapping in a single ventricle patient who is completely dependent on passive lung flow was considered a major risk during spine surgery.1-4 Prone position and positive pressure ventilation will reduce venous return to the heart in a healthy non-cardiac patient, 5 and will profoundly decrease gradient-driven pulmonary blood flow in Fontan physiology.6-8 In this patient, that could be exacerbated by atelectasis, air entrapment, and tension pneumothorax on the left side due to LMB compression. Air entrapment has detrimental effects on pulmonary blood flow and may quickly become lethal due to inadequate ventricular filling and poor systemic circulation. Furthermore, high venous pressures in Fontan physiology increases the risk of bleeding even further.1,3,4 If major blood loss in single ventricle patients is not adequately managed, pulmonary blood flow, ventricular filling, and cardiac output will deteriorate.
Clinical Considerations
His case was presented and discussed in the pediatric congenital heart team to seek advice on a potential therapeutic strategy. During the first cardiac intervention, the main pulmonary trunk was connected with the aortic arch, followed by patch plasty for extreme coarctation of the aorta. These reconstructive surgeries are known for the potential to narrow the aortopulmonary space with compression of the LPA and LMB.9,10 Figure 2 shows a schematic representation of the anatomical relations between LMB, LPA stent, ascending, and descending aorta. Surgical options to reduce the bronchus compression would consist of a complex reoperation involving circulatory arrest to take down the current aortic reconstruction, reduce and extend the neo-aortic arch, cleave the stented LPA, and perform a plasty of the LMB. Such a procedure was never described in a Fontan patient before. Alternatively, a pneumectomy was considered, but this has negative consequences for pulmonary blood flow and prognosis. A second opinion was requested at 2 eminent cardiac congenital clinics with airway expertise. Neither recommend cardiac surgery or stenting as spinal surgery hereafter could further alter the mediastinal configuration. They recommended addressing of the spinal surgery first, accepting the risk of an acute LMB compression and the need for a dorsal aortopexy to improve LMB patency. Schematic representation of the close anatomical relations between the ascending (NeoAo). and descending (AoDesc) aorta, left main bronchus (LMB) and left pulmonary artery (LP) -stent. Right ventricle (RV), left ventricle (LV), superior vena cava (SVC), common atrium (CA) and inferior vena cava (IVC).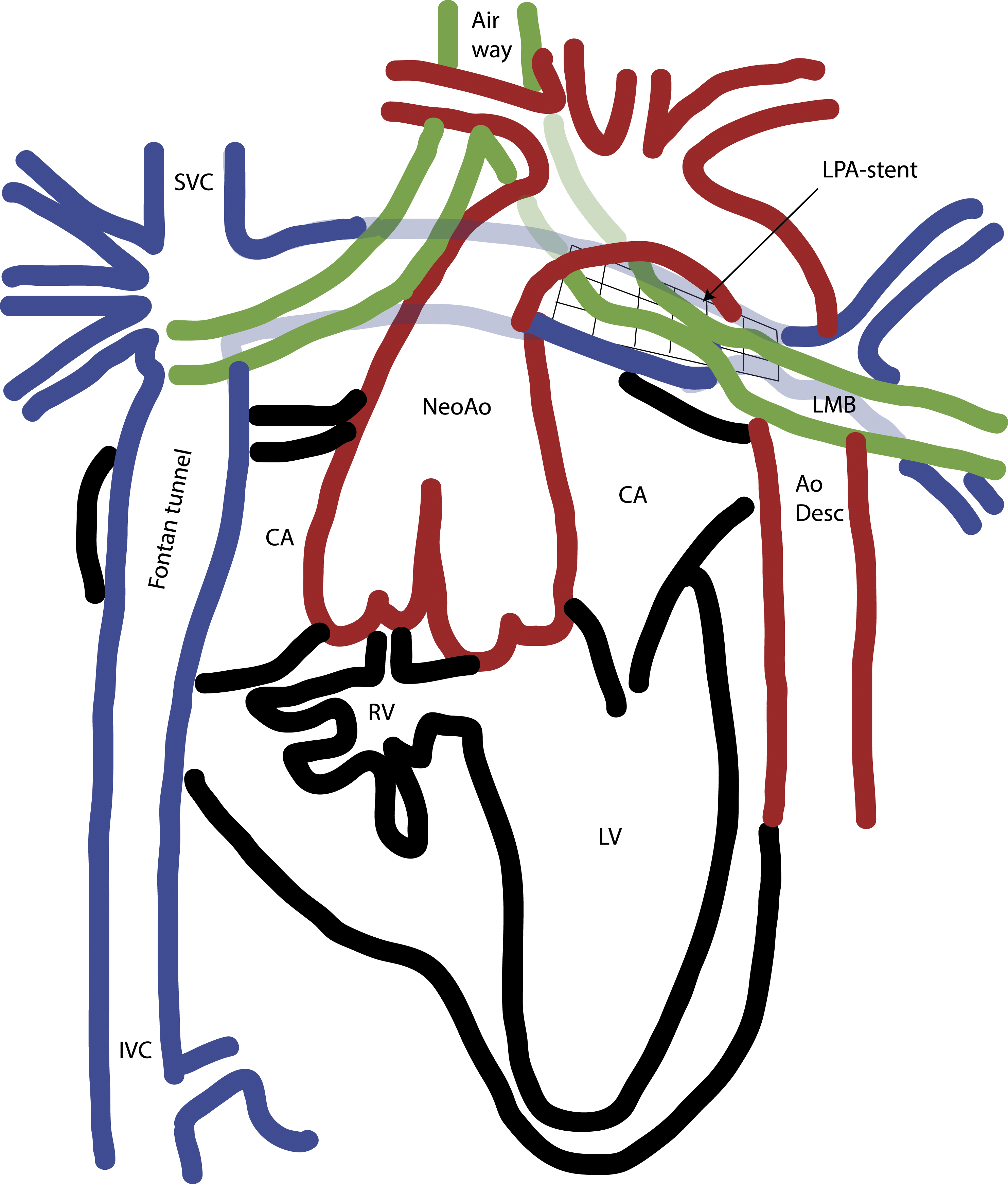
Dynamic Evaluation of Bronchus and LPA
We performed a diagnostic catheterization combined with a dynamic evaluation of the LMB patency to measure whether an airway device could be placed to stent the airway during spine surgery without compromising the LPA. This diagnostic procedure, under general anesthesia during which spontaneous breathing was retained, confirmed that further optimization of the LPA stent was not possible. Total cavopulmonary connection pressures measured were 20 mmHg (previous: 14 mmHg) with a transpulmonary gradient of 10 mmHg (previous: 4 mmHg). During spontaneous breathing, flexible bronchoscopy showed that the LMB was completely collapsed, however, easily to pass. A 10 mm balloon (Powerflex 10 × 30) was inserted through the LMB and slowly filled with air while monitoring for potential LPA stent compression. The 10 mm balloon could be inflated 100% while opening the LMB without detrimental effects on the vascular structures around it. The LMB compression was located near the carina and caused bronchial malacia and not stenosis. A crucial finding for the airway management plan: Placement of a left-double lumen (DLT) or bronchial tube was expected to successfully clear LMB obstruction during surgery. Placement of a biodegradable airway stent was only considered as a potential rescue intervention after surgery when the aortopulmonary narrowing would have deteriorated further and the patient could not be extubated successfully. A biodegradable airway stent might have advantages in this case, but degradation is also associated with the risk of in-stent obstructive material. 11
Surgical Plan and Course
Posterior spinal fusion under neuromonitoring is the treatment of choice for scoliosis patients at the end of their adolescent growth spurt. With this technique, the spinal and chest deformity can be corrected, and in the long-term, this correction can be maintained with low risk for revision procedures and excellent health-related quality of life outcomes. 12 In this patient, based on the severity of the spine and chest deformity, only limited loss of compliance and limited loss of restrictive and obstructive lung function was expected. The effects of operative scoliosis correction on the mediastinal anatomy have not been studied so far. Based on the compromise of the left-sided mediastinal structures and the right-sided rotation of the apex of the thoracic curvature, less vertebral derotation, and maximal kyphosis restoration (to pull the spine out of the chest and restore physiological sagittal spinal alignment) was planned. If perioperative negative effects on the cardiopulmonary system were detected, in situ fusion of the thoracic spine would be considered. In this situation, the spine deformity is not corrected but stabilized to prevent progression of the scoliosis. Surgical decision were aimed at reducing operative time and minimize blood loss. A posterior spinal fusion from T3 to L3 was undertaken, and correction of the scoliosis, minimal derotation, and restoration kyphosis was performed as planned. Total duration of the surgical procedure was 130 minutes with a total blood loss of 4500 mL.
Anesthetic Plan and Course
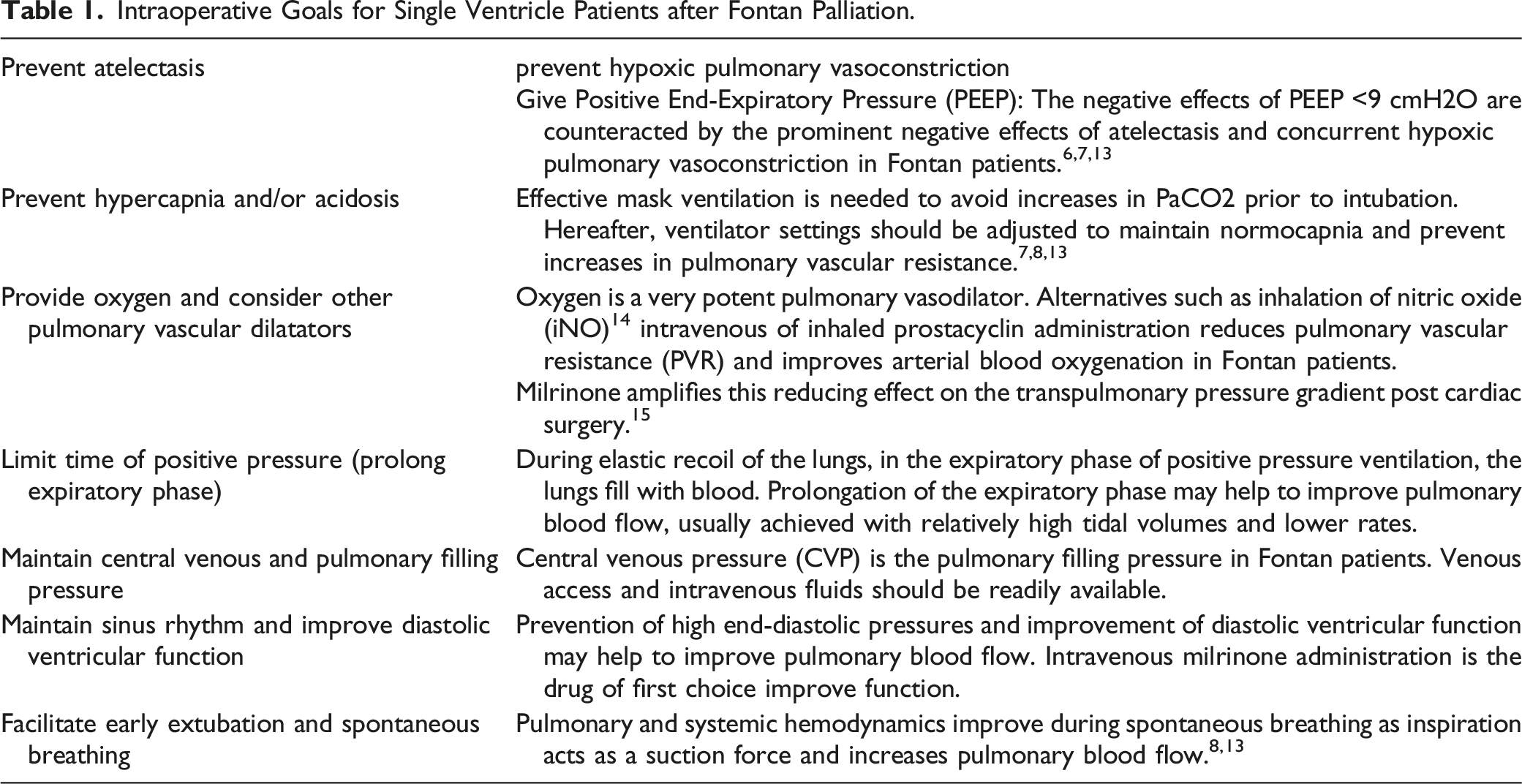
Intraoperative Goals for Single Ventricle Patients after Fontan Palliation.
Postoperative Course
His postoperative course was uneventful. On the fifth postoperative day, he was discharged home. Three months after the procedure, a computed tomography angiography was repeated to image anatomical relations of LMB, LPA, aortic root, and descending aorta. Results showed no change of the available space for the LPA and the LMB between the aortic root and the descending aorta after correction of the scoliosis (Figure 3). Transverse view of the aortopulmonary space pre- and post-scoliosis correction in a Fontan. Patient with severe compression of the left main bronchus. Unchanged anatomical relations and compression of the left main bronchus.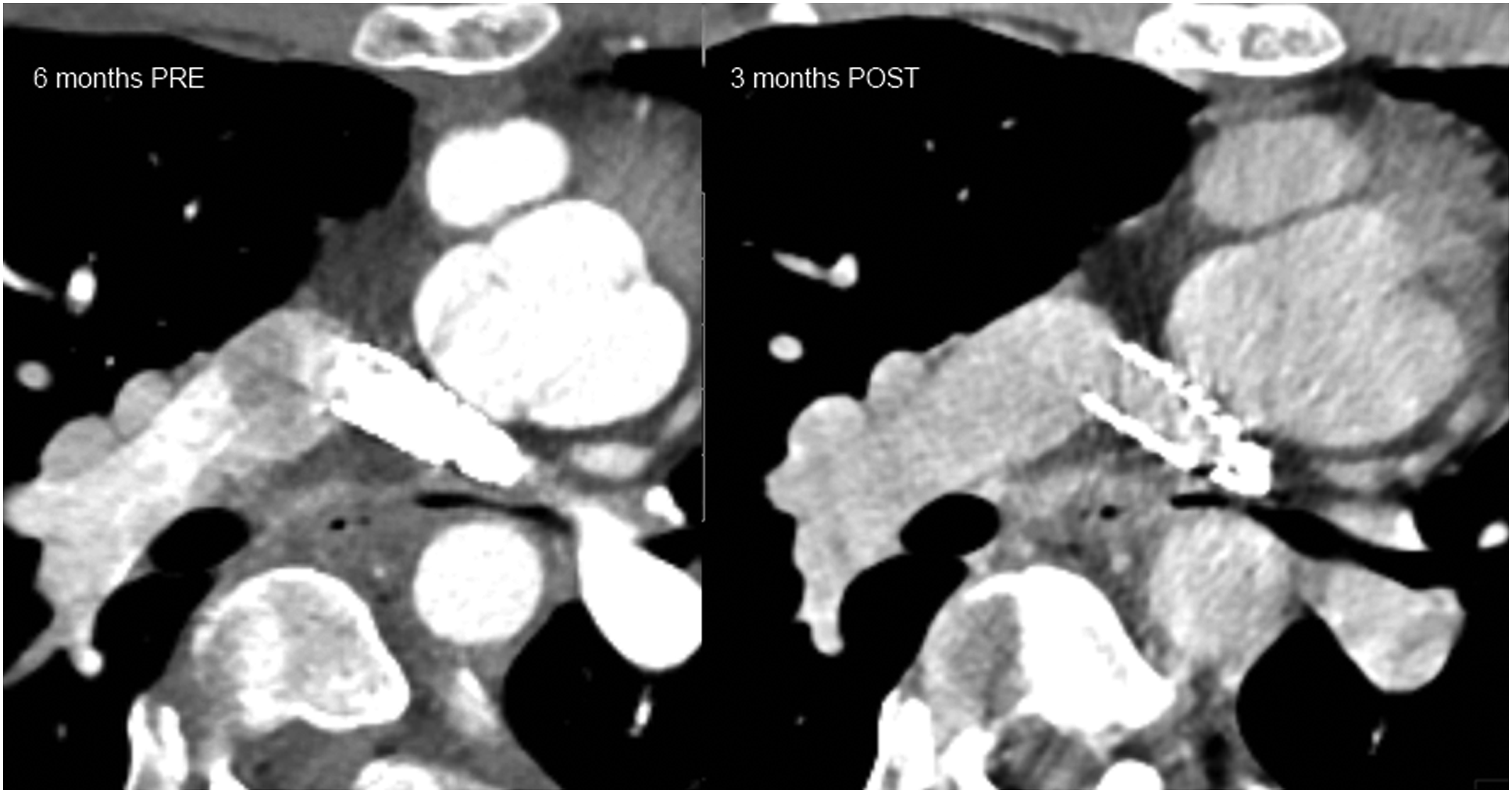
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.