
Abstract
This study examines the phenomenon of intimate partner homicide-suicide (IPHS), specifically, how it differs (or not) from intimate partner homicide without suicide (IPH), and how the ages of victims and perpetrators shape the risks, vulnerabilities and contextual features of cases. A mixed methods document analysis of 232 domestic homicide reviews (DHRs) was undertaken, using bivariate analysis to compare 37 IPHS to 195 IPH-without suicide, and a gendered, thematic analysis to gain deeper, contextualized insights into IPHS structured by victim and perpetrator age. IPHS victims and perpetrators were older, and in the case of perpetrators, more likely to be white. Risks and vulnerabilities also differed, with less substance use, criminality, and violence, but greater physical and mental health difficulties. Themes of “Separation and loss,” “Dependency,” and “Mental health and suicidality” ran through the 37 IPHS, but with IPHS involving older adults appearing as phenomenologically distinct, shaped by gendered contexts of care and a loss of autonomy due to chronic, degenerative illness. Our findings highlight the key role for physical and mental health services—particularly General (Medical) Practitioners—alongside the need for comprehensive support systems and coordinated care to manage the complex interdependencies in elderly couples.
Introduction
The rarity of Homicide-Suicide (H-S) globally is well documented, with rates across multiple countries ranging from 0.01 to 0.89 per 100,000 people per year (Prévost & Léveillée, 2025), representing between 4% and 11% of all homicides (Liem et al., 2011). Most constitute Intimate Partner H-S, hereafter referred to as “IPHS” (e.g., Dayan, 2021; Vatnar et al., 2021). A gendered pattern of these deaths is also well-established in that men kill their female ex/partner first and then kill themselves (Panczak et al., 2013; Rouchy et al., 2020; Zeppegno et al., 2019). To reflect this, Dayan (2021) advocates for the term femicide-suicide to be used and there is strong merit in doing so (see also Dawson, 2005; Solinas-Saunders, 2024). In a similar vein, Gregory (2012) posits that insufficient attention is paid to gender given that most perpetrators are men. She argues that theory relating to H-S needs to integrate concepts of hegemonic masculinity, which is closely linked to motivation (see below). Indeed, a focus on IPHS has been highlighted as vital for providing a more nuanced analysis of the phenomenon and greater conceptual disaggregation from other forms of domestic homicide such as adult family homicide (Vatnar et al., 2021).
Much of the H-S literature discusses whether homicide was the primary motivation (e.g., Harper & Voigt, 2007), if it was suicide that drove the homicide (e.g., Palermo, 1994), or indeed whether it is a separate phenomenon (e.g., Panczak et al., 2013). Where suicide is seen as a primary motivator, H-S can be conceptualized as a form of “extended suicide” (Rosenbaum, 1990) whereby the homicide victim is seen as an extension of the perpetrator’s selfhood. Gregory (2012, p. 148) argues that suicidal intent engenders “suicidal abrogation” which gives permission to the perpetrator to commit homicide before taking their own life in the knowledge that there will be no criminal consequences. Regarding older couples, Joiner (2014) suggests that H-S can be a “mercy killing” stemming from altruism. A common precipitator of H-S in older couples is a significant decline in health (Flynn et al., 2016), the caring burden (O’Neil, 2016), and loss of autonomy for both carer and cared-for. Outside of this context, one of the key precipitators of H-S is attempting to leave an intimate relationship or separation (Flynn et al., 2016; Gregory, 2012; Harper & Voigt, 2007; Liem et al., 2011). However, this precipitator is also common in domestic homicide without suicides (Daly & Wilson, 1988; Dobash & Dobash, 1979) and in domestic abuse (DA) generally. The sense of owning the victim (entitlement) and sexual jealousy based on patriarchal dominance, are frequently found both in domestic abuse and domestic homicide (Daly & Wilson, 1988; Dobash & Dobash, 1979). Harper and Voigt (2007) proposed an integrated theoretical model based on conflict intensity structures and Agnew’s (1992) work on stress-strain—the latter expressly acknowledges patriarchal structures. However, we concur with Gregory (2012) that existing theories would benefit by utilizing a more focused gendered analysis.
Many studies appear to focus on perpetrator characteristics or the type of victim-perpetrator relationship, the most common being intimate ex/partner. Studies comparing H-S to intimate or ex-partner homicide without suicide contend that there is little difference between perpetrators of each type (e.g., Vatnar et al., 2021). However, H-S perpetrators are reported to be older than homicide perpetrators or those who have taken their own lives, and more often of white ethnicity (Panczak et al., 2013; Rouchy et al., 2020; Zimmerman et al., 2023). Some studies report that approximately 25% of H-S are committed by people aged over 55 (e.g., Malphurs & Cohen, 2002). Studies analyzing younger and older perpetrators of H-S have explored differing motivations for the incident (e.g., Schwab-Reese et al., 2021; Zeppegno et al., 2019). In general terms these can be divided into H-S that are primarily motivated by the loss of an intimate relationship and more related to homicidal intent (primarily younger perpetrators) and those motivated by “mercy-killing” and suicidal intent (older perpetrators). However, this distinction between motivations of older and younger perpetrators of H-S requires further investigation. Although rates vary across studies, alcohol and substance misuse, a prior history of domestic abuse or unemployment have been found to be less prevalent in H-S compared to homicide alone (Panczak et al., 2013).
The role of mental health problems, specifically depression in perpetrators is discussed in several studies worldwide (for a review, see Rouchy et al., 2020). Flynn et al. (2016) found that depression was the most common mental health problem for H-S perpetrators, that psychosis was rare and that a quarter of their sample had previously attempted suicide. Liem and Roberts (2009) in their comparative study between intimate partner homicide and H-S also found depressive disorder and suicide threats preceding the H-S to be more prevalent in the H-S group. However, depression has been found to also be a feature of intimate ex/partner homicide (without suicide) (Chantler et al., 2020) and in domestic abuse (Oram et al., 2014).
Studies vary in terms of how H-S is defined temporally that is, the length of time between the homicide and resultant suicide (Zeppegno et al., 2019). In line with Vatnar et al. (2021), we have excluded cases involving suicide post-arrest, although extended the timeframe to include a suicide which took place 10 days post-homicide (see Methods for details).
Given the limited insight into IPHS within the UK, and the seeming importance of age in the shaping of the phenomenon, the aims of this paper are to:
Compare the characteristics of IPHS to IPH without suicide to identify points of convergence and divergence
Compare IPHS cases involving adults over and under 65 to explore how victim and perpetrator age shape the risks, vulnerabilities and contextual features of cases
Undertake a gendered analysis of the contextual features of IPHS cases to understand how gendered constructions, inequalities and expectations shaped them
Methods
Sample
Domestic Homicide Reviews (DHRs) are hosted on Community Safety Partnership (CSP) websites in England and Wales. The team downloaded DHRs (of any year) from all 322 CSP websites (where available) over a period running from 2012 until 2019, resulting in a final sample of 302 DHRs. Of these 302 DHRs, 39 (12.9%) related to cases involving H-S, where perpetrators initially killed the victim, before then taking their own lives. This figure is in line with the proportion of domestic homicides ending in “principal suspect” suicide in England and Wales over the 3-year period April 2019 to March 2022 (49/370, 13.2%) (Office for National Statistics [ONS], 2023a), suggesting good sample representativeness. Given the public availability and anonymization of DHRs, ethical approval was not required.
Cases not defined as H-S included those involving post-homicide suicide attempts (n = 6), given the difficulty in establishing whether true suicidal intent was present. Similar to previous studies (e.g., Vatnar et al., 2021), we also excluded cases where perpetrators died by suicide post-arrest (n = 4), given that it was likely no longer part of “the same action” that is, due to legal consequences rather than suicidal intent (Vatnar et al., 2021, p. 8233). Reflective of many H-S definitions (e.g., Dobash & Dobash, 2015; Vatnar et al., 2021) most perpetrators killed themselves immediately or within 24-hr of the initial homicide (n = 33).
Of the 39 H-S DHRs, 37 involved intimate partners or ex-partners (IPHS), representing 15.9% (37/232) of all intimate partner homicides (IPH) within our dataset. These 232 IPH DHRs form the total sample for our comparative analysis in Section 1 of our findings, relating to homicides that took place between 2010 and 2017, with their corresponding DHRs published between 2012 and 2019. In Section 2, the 37 IPHS DHRs form our qualitative sample for analysis. These 37 DHRs covered 23 police force areas in England and Wales, situated across all nine regions of England, with three in Wales. The 37 IPHS occurred between 2011 and 2017, with their associated DHRs published between 2012 and 2019.
Data Extraction and Analysis
Quantitative and qualitative data extraction templates were developed through our previous research on DHRs and refined using the current literature on IPHS, domestic homicide, and domestic abuse more broadly. This allowed us to extract data from the DHRs systematically and with consistency across the research team. The mixed methods study was of a convergent parallel design, in that the quantitative and qualitative components of study ran concurrently, providing distinct yet complimentary insights and evidence (Creswell & Plano Clark, 2017). However, both methods were closely aligned in an ongoing and iterative process of challenge, critical reflection and refinement.
DHRs were read in their entirety and data transformed into quantitative variables in Excel, and later SPSS (v27), capturing information on victim/perpetrator demographics, risk and vulnerability factors, relationship characteristics and history, and escalating and precipitating factors (i.e., “motives”). Frequencies, proportions and averages were used to produce descriptive accounts of the data, with bivariate correlations using Pearson’s chi-square tests used to make statistical comparisons between IPH and IPHS cases. Multivariate analysis (bivariate logistic regression) was considered as a more rigorous statistical method (see Vatnar et al., 2021); however, the small sample size would have limited the analysis to too few predictors (i.e., a minimum of ten “events-per-variable,” as per Heinze et al., 2018).
A thematic document analysis (Gross, 2018) was undertaken on qualitative data drawn from the DHRs using the qualitative template. The template enabled the team to systematically collect in-depth, nuanced, and contextualized data relating to victims, perpetrators, and the events leading to the homicide-suicide. Several a priori codes were used to structure the analysis, namely victim and perpetrator age and gender, as these were central areas of exploration. Other a priori codes were developed from the quantitative analysis/findings, including perpetrator mental health, caregiving, and length of relationship. The process was iterative and comprehensive, with two authors (VB, KB) reading and re-reading the 37 IPHS fully, before separately extracting data, coding in NVivo 14, summarizing with narrative text and raw data (quotes), and then jointly comparing, critiquing and refining based on reflection and discussion. Where possible, subthemes/codes were triangulated against their quantitative counterparts, increasing confidence in those codes. Quotes were used to anchor the themes to the raw data, selected based on their representativeness, clarity, and brevity.
Data Quality and Coding
Risk and Vulnerability Factors
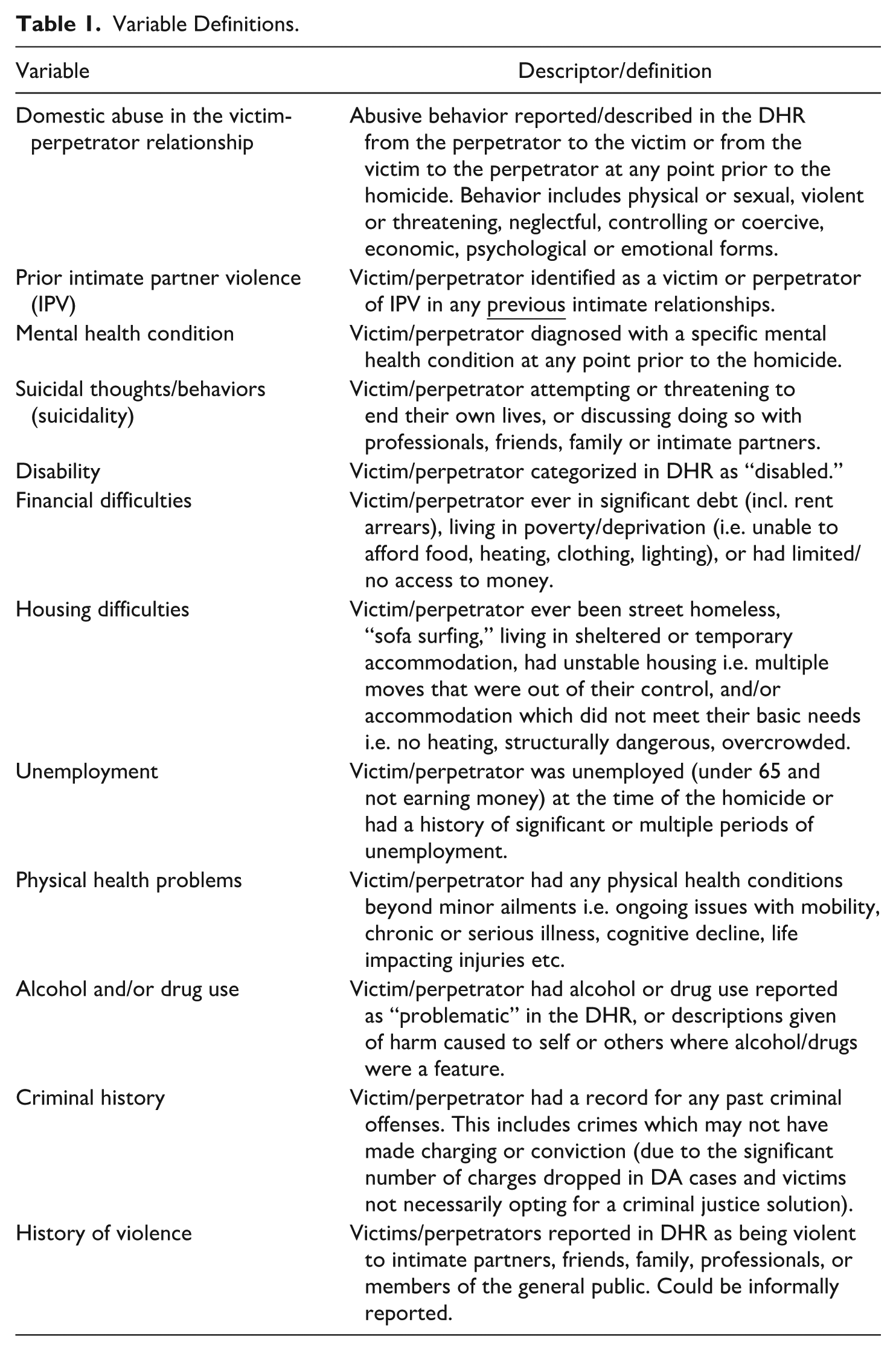
Risk and vulnerability factors were coded as present if mentioned within the DHR and represents victims/perpetrators having a history involving that specific factor (e.g., prior intimate partner violence (IPV), mental health conditions). It does not necessarily mean that the factor was present at the time the homicide took place. Variable definitions were agreed as a team and formalized in a codebook (see Table 1). Twenty-five percent of the full sample’s coding was checked for accuracy and consistency by the first author.
Variable Definitions.
To code the escalating/precipitating factors within each case, DHRs were read in their entirety and assigned an initial descriptor/code representing the single most prominent feature that appeared to precipitate, explain or contextualize the homicide. This process was iterative, involving multiple readings and category refinement/reduction. Four conceptually distinct codes were agreed upon: 1) Separation, rejection and jealousy; 2) Acute episode of mental ill health; 3) Carer despair at the future; and 4) No clear single escalating feature. Escalating/precipitating factors of all 37 IPHS were quality checked by the first author, in addition to all IPH coded to carer despair and mental health episode, 20% of IPH coded to separation/rejection/jealousy, and 20% of IPH coded to no single feature.
Although our analysis of DHRs carries with it a relatively low risk of generating false positives (i.e., identifying risks or vulnerabilities where there were none), it carries a relatively high risk of generating false negatives (i.e., not identifying risks or vulnerabilities which were in fact present). This is particularly relevant given the varied and sometimes limited timeframe of the reviews, in addition to the fact that risks and vulnerabilities—particularly involving experiences of victimization or inequality—can often remain unidentified or undisclosed and therefore invisible to the review process (Rowlands & Bracewell, 2022). For this reason, the absence of a risk or vulnerability factor should only be viewed as its absence from the DHR itself. Prevalence rates should always be viewed as conservative estimates.
Missing Data
High proportions of missing data were present across victim and perpetrator ethnicity (32% and 35% respectively) and age (27% for both) variables. As age was a grouping variable for some parts of our analysis, supplemental media searches were made using the Google search engine and specific websites (e.g., www.femicidecensus.org). This enabled the identification of victim and perpetrator ages for all 37 IPHS cases and all but two of the 195 IPH without suicide cases. These two cases were removed from analyses involving age as a grouping variable. Although utilizing media reports to establish demographic variables carries some limitations (i.e., the potential for inaccurate media reporting; the mixing of data sources for only a proportion of the sample) this was the best route available given the data limitations.
Findings
Section 1 presents our statistical analysis comparing the 37 IPHS DHRs to the 195 IPH DHRs without suicide (referred to as “IPH”), exploring victim and perpetrator characteristics and key contextual features. Section 2 presents an in-depth, qualitative exploration of the 37 IPHS DHRs, drawing out key themes across two distinct groups comprising adults older and younger than 65 years of age. Themes are anchored to the data using quotes from the DHRs, with detailed accounts allowing for contextualization and in-depth explication of the themes.
Section 1: Comparing IPHS to IPH
Victim Demographics
Victims across both groups were predominately female (IPHS 97.3%, IPH 85.6%) and of a White British background (IPHS 78.1%, IPH 73.3%). However, IPHS victims were on average 12 years older than IPH victims (IPHS 51 years, IPH 39 years), with no IPHS victims under the age of 26 and nearly a third (29.7%) aged 66+. Indeed, the higher proportion of “older adults” represents a key difference between IPHS and IPH victims, with only 4.7% of the latter aged 66 and above. See Table 2 for full statistics.
Comparing Victim Characteristics Across IPHS and IPH.
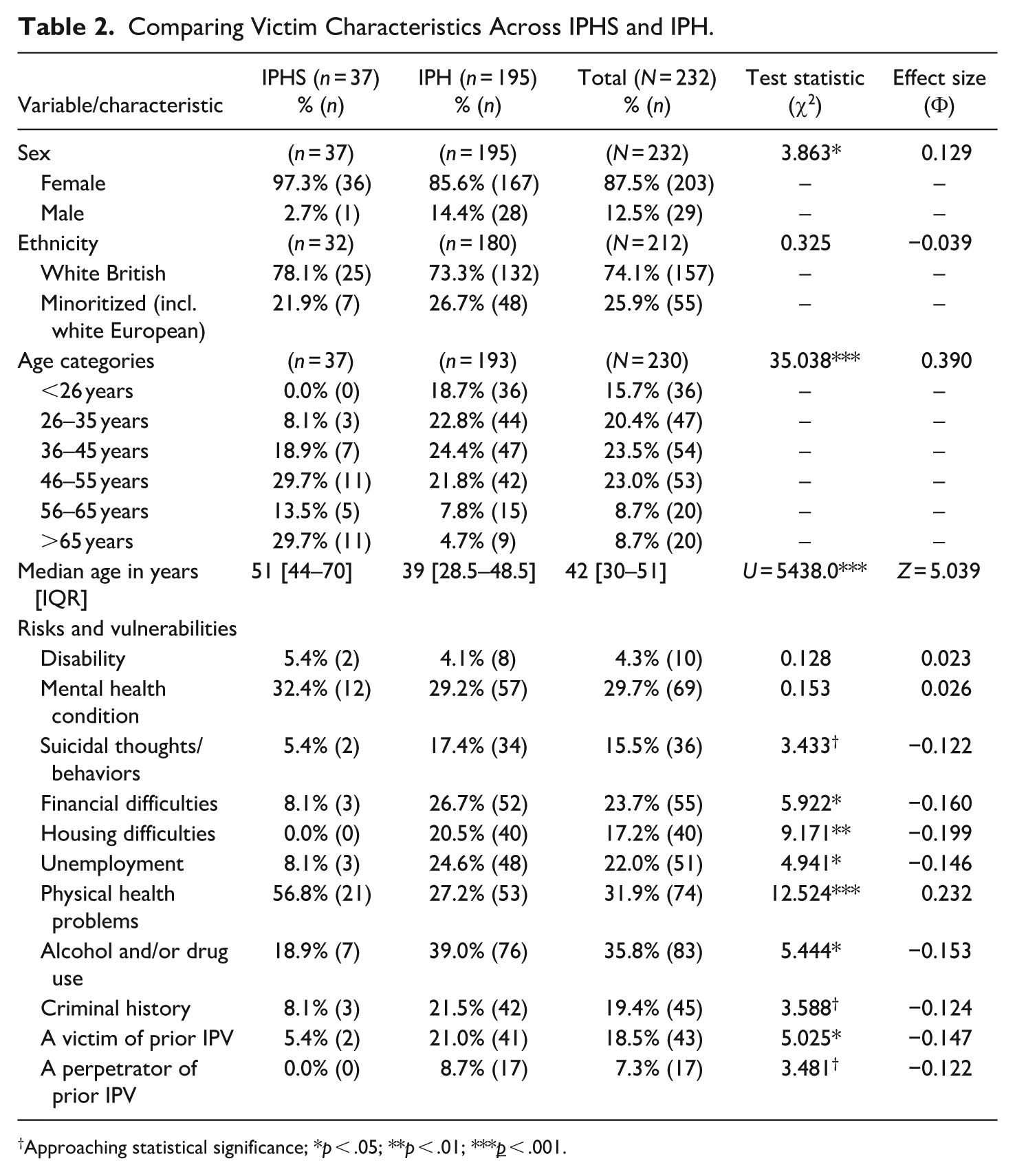
Approaching statistical significance; *p < .05; **p < .01; ***p < .001.
Victim Risks and Vulnerabilities
Although IPHS victims shared some similarities to IPH victims, they differed in several respects. Namely, they were less likely to have experienced victimization from a prior intimate partner (IPHS 5.4%, IPH 21.0%) and less likely to have had problematic drug and/or alcohol use (IPHS 18.9%, IPH 39.0%). They were, however, more likely to have physical health problems (IPHS 56.8%, IPH 27.2%)—particularly chronic, age-related conditions impacting mobility and cognition. From a socioeconomic perspective, they were less likely to have had difficulties relating to finances (IPHS 8.1%, IPH 26.7%), housing (IPHS 0.0%, IPH 20.5%) or unemployment (IPHS 8.1%, IPH 24.6%), although the latter is likely related to their greater likelihood of having reached retirement age. See Table 2 for full statistics.
Perpetrator Demographics
Perpetrators across both groups were predominately male (IPHS 97.3%, IPH 87.2%) and of a White British background (IPHS 84.8%, IPH 62.2%). However, the proportion of White British perpetrators was significantly higher within the IPHS group. Similar to victim age, IPHS perpetrators were older than IPH perpetrators (IPHS 53 years, IPH 42 years), with no IPHS perpetrators under the age of 25 and nearly a third (29.7%) aged 66+. Again, the higher proportion of “older adults” represents a key difference between IPHS and IPH perpetrators, with only 5.7% of the latter aged 66 and above. See Table 3 for full statistics.
Comparing Perpetrator Characteristics Across IPHS and IPH.
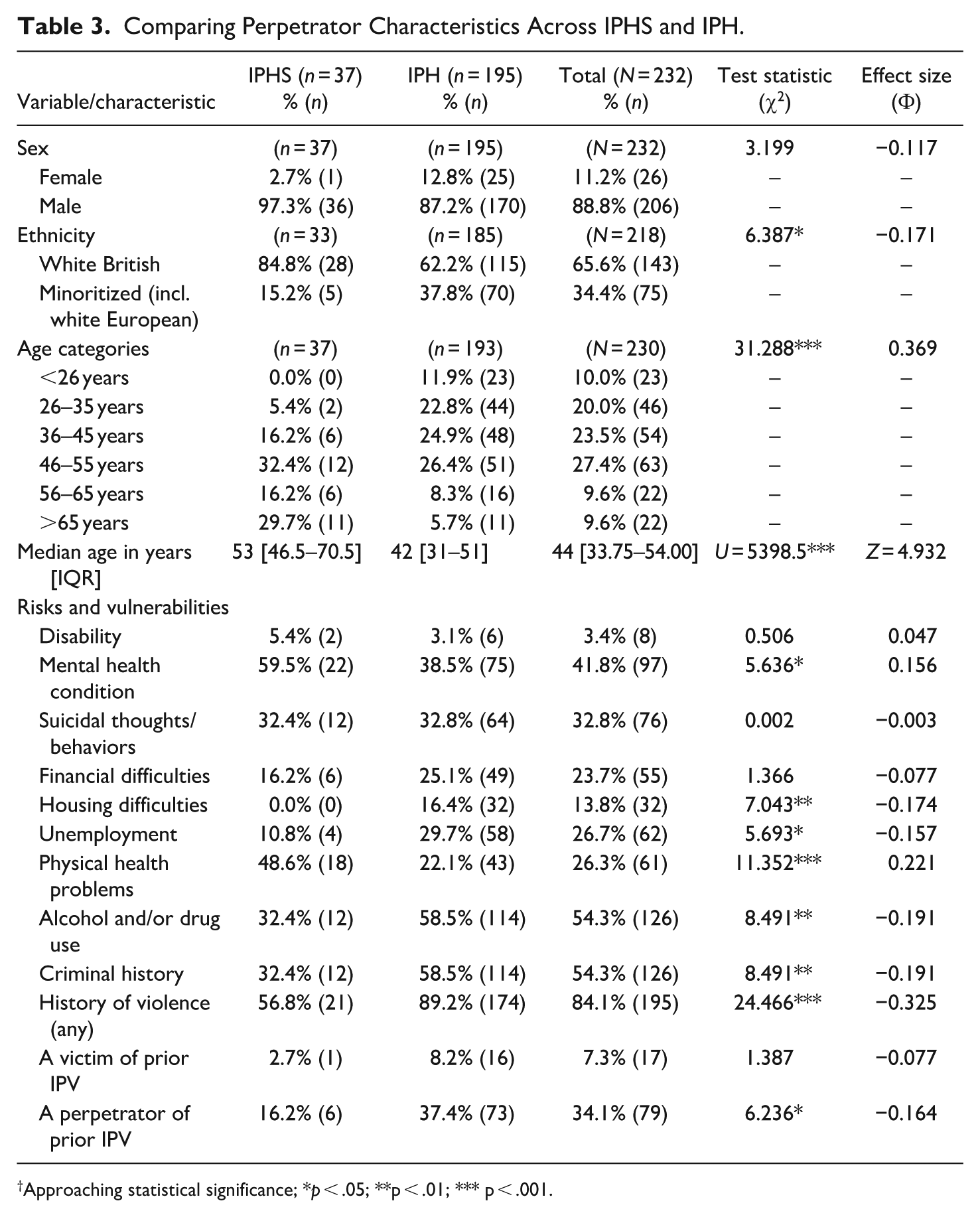
Approaching statistical significance; *p < .05; **p < .01; *** p < .001.
Perpetrator Risks and Vulnerabilities
Key differences were identified between the risks and vulnerabilities of IPHS and IPH perpetrators, many of which are reflected in the aforementioned literature. With regards to health, IPHS perpetrators were more likely to have physical (IPHS 48.6%, IPH 22.1%) and (diagnosed) mental health conditions (IPHS 59.5%, IPH 38.5%), although surprisingly, suicidality was similar across the two groups (IPHS 32.4%, IPH 32.8%). With respects to socioeconomic factors, IPHS perpetrators were less likely to have experienced housing difficulties (IPHS 0.0%, IPH 16.4%) or unemployment (IPHS 10.8%, IPH 29.7%), although just as likely to have had financial difficulties (IPHS 16.2%, IPH 25.1%). Other differences included their lower levels of problematic alcohol/drug use (IPHS 32.4%, IPH 58.5%), criminality (IPHS 32.4%, IPH 58.5%) and violence (IPHS 56.8%, IPH 89.2%)—including violence toward previous partners (IPHS 16.2%, IPH 37.4%). See Table 3 for full statistics.
Relationship Characteristics
Although similar proportions of victim-perpetrator relationships were “intact” at the time of the homicide (IPHS 64.9%, IPH 64.1%), there were several differences in relationship characteristics between the two groups. The relationships of IPHS “dyads” were longer-lasting, with 84.4% having lasted for over 10 years (compared to 38.9% of IPH dyads). IPHS victims and perpetrators were also more likely to have been living together at the time of the homicide (IPHS 75.7%, IPH 55.9%) and were more likely to have been in a caregiving/care-receiving relationship (IPHS 32.4%, IPH 11.3%)—most commonly perpetrators “caring” for victims (IPHS 24.3%, IPH 6.2%). Lastly, IPHS DHRs were less likely to have identified domestic abuse within the victim-perpetrator relationship (IPHS 59.5%, IPH 84.1%), with no IPHS victims or perpetrators being discussed at a Multi-Agency Risk Assessment Conference (MARAC) (IPH 16.9%). See Table 4 for full statistics.
Comparing Relationship and Case Characteristics Across IPHS and IPH.
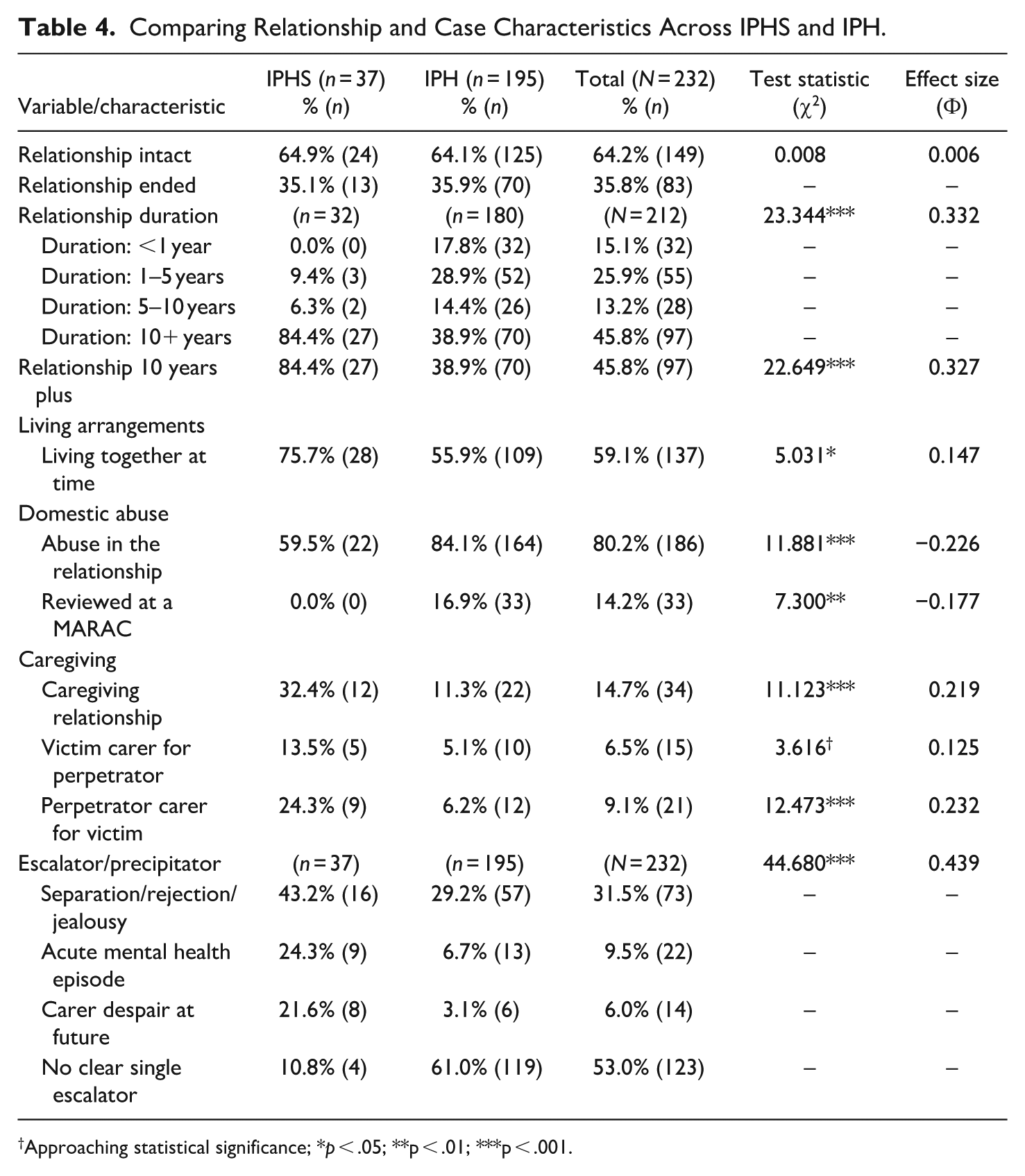
Approaching statistical significance; *p < .05; **p < .01; ***p < .001.
Escalating/Precipitating Factors
Through assessing the most prominent (single) escalating or precipitating factor described within each DHR, we identified that separation/rejection/jealousy was the most common across both groups (IPHS 43.2%, IPH 29.2), although IPHS cases were more likely to involve an acute episode of mental ill-health (IPHS 24.3%, IPH 6.7%) or carer despair at the future (IPHS 21.6%, IPH 3.1%). However, in a large proportion of IPH cases (61%), no clear single escalating feature could be identified, with multiple and intersecting factors of entrenched and escalating domestic abuse (toward the victim), perpetrator criminality and serial IPV perpetration, victim and perpetrator poverty, homelessness, mental ill health and substance use appearing to shape the homicide context. See Table 4 for full statistics.
Section 2: A Qualitative Exploration of IPHS by Age
Through our quantitative IPHS/IPH comparisons and subsequent thematic analysis of qualitative IPHS data, it became evident that IPHS could broadly be divided into cases involving: 1) “younger” adults (both) aged 65 and under, with contexts involving perpetrator abuse of victims and relationship separation (n = 24); and 2) “older” adults (either) aged over 65 experiencing physical and cognitive decline, with male carers (IPHS perpetrators) despairing at a future characterized by infirmity and reduced autonomy/independence (n = 13). Exploring the contextual features of the homicide-suicides within these two groups, three themes emerged as particularly salient to both, but with presentations shaped by age: “Separation and loss,” “Dependency,” and “Mental health and suicidality.”
Theme 1: Separation and Loss
For both younger and older IPHS dyads, separation and loss were key themes which appeared to shape the homicide context in age-specific ways.
Separation and Loss in Younger Adults
For younger dyads, separation meant the ending of the intimate relationship. Although, in some cases, this was feared/anticipated rather than actual.
[Perpetrator] also articulated the idea to colleagues that he would kill [Victim], himself and his youngest son should she ever leave him (DHR166, p. 22, younger)
In others, separation led to victims beginning new relationships. Here, perpetrator jealousy and a desire for retribution appeared to be key emotional-relational drivers for the homicide: “If I can’t have you, no one can” (DHR152, p. 13, younger). This is not necessarily surprising given that 19 of the 24 victims had experienced abuse from the perpetrator prior to separation. However, distinctive of IPHS was the enduring nature of the victim-perpetrator relationship, with the majority having lasted for over 10 years, and in several cases, beginning in adolescence/early adulthood. This, alongside other (interrelated) contextual features such as fear of financial loss and economic hardship, suggest that the suicide component in these cases may stem from despair at a future perceived as lost or hopeless, and indeed, a future perpetrators felt entitled to. As stated by one perpetrator in his suicide note:
“[Victim] is sacrificing my life so that she can change hers. I end up as a sad old man in a cheap flat somewhere and she enjoys the high life, I’ve worked too hard for too long to allow this”. (DHR308, p. 32, younger)
Separation and Loss in Older Adults
For older dyads—in all but one case still together at the time of the homicide—separation and loss meant the loss of health, independence, and a future together. Here, IPHS perpetrators were often the primary carers for victims and were struggling, not only with their caring responsibilities, but with the realities of their lost independence, “younger” lifestyles, and health. For example, in DHR107 the victim (aged 73) and perpetrator (aged 61) had been married for over 20 years, having “lived a good care free luxury lifestyle that involved extensive travel” (p. 48). Six months prior to the homicide, the victim suffered a stroke, which “brought this lifestyle to an abrupt end” (p. 48). Insights from family and friends indicated that the perpetrator “could not accept that his much envied lifestyle was effectively over” (p. 49), something reflected in his “joint” suicide note which stated “Sorry to everyone, no way forward for us. . .” (p. 10). Subsequent investigation established that only the perpetrator, not the victim, had been involved in writing the note. Similarly, in DHR093 the victim (aged 78) and perpetrator (aged 82) had been married for nearly 60 years, living “a somewhat independent and isolated lifestyle” (p. 7) in a remote part of the countryside. The perpetrator had bowel cancer and the onset of dementia, and the victim had recently been diagnosed with terminal lung cancer. In the days before the H-S the victim had arranged for them to move into a care home together, seemingly in good spirits. However, during his call to the police to report their deaths, the perpetrator stated: “. . .in love, enjoyed life but can now only see death and horrible things in front of them” (p. 7). Here, as with DHR107, only the perpetrator voice is heard, speaking both for himself and for the victim, the latter of whom had recently expressed a more positive outlook incongruent with an intention for joint suicide.
A fear of separation due to increasing care needs featured in a number of older adult IPHS, with victims making it clear they “did not want to go into a care or nursing home” (DHR195, p. 13) and couples declining support such as respite care because they preferred to “do things together” (DHR064, p. 23). In DHR192, the perpetrator “wanted more support but didn’t want to be separated [from the victim]” (p. 22), and in DHR102 the perpetrator carried out the H-S the day after telling a visiting occupational therapist that “he felt the time had come to consider [Victim] going into residential care” (p. 35). In these cases, older couples were often described as particularly “close-knit” (DHR315), “inseparable” (DHR107, p. 25), and “unable to do without each other” (DHR093, p. 8), something which at times resulted in the removal/ending of much-needed services and supports. Further, such descriptions often appeared alongside other service constructions of older couples as “loving,” “devoted,” and “caring.” In some cases, such constructions appeared to mask potential indicators of abuse and prevented active enquiry or consideration of domestic abuse by practitioners.
Loss of Control
Although IPHS in younger and older adults appeared to have distinct presentations, a feature common to both was perpetrators’ fear of losing control—both over their own lives and over the lives of their victims. In younger perpetrators, this presented as behaviors which were clearly coercive, highly controlling, and abusive: “[Perpetrator] was wanting sex everyday as proof that she loved him” (DHR166, p. 22, younger). Whereas in older perpetrators, behaviors included taking control over household finances: “He would control the money and made records of all transactions even the cost of a newspaper” (DHR107, p. 12, older); and control over victims’ care schedules and medication: “The Victim was only [in respite care] 2 days before the Perpetrator removed her, not being satisfied with the care and took her home” (DHR192, p. 8, older). Although not necessarily part of an abusive dynamic in these cases, threaded throughout all the DHRs were accounts of highly inflexible men with the need to have high levels of control over their environment.
The Mental Health team described [Perpetrator] as methodical and that he liked things to be in order. [Victim’s] diagnosis made this difficult and he told staff that he felt the situation was getting out of control. . . They described [Perpetrator] as a practical, intelligent, black and white thinker who would not have been able to cope with the disarray. (DHR315, p. 4, older).
Theme 2: Dependency
Dependency was a theme which ran through the majority of the DHRs, often intersecting with issues relating to physical and mental health, financial difficulties, and substance use. As with the previous theme on separation and loss, dependency was often shaped by age.
Dependency in Younger Adults
For younger adults, dependency often meant perpetrators being financially reliant upon victims, living in their homes—whether separated or not—and in most cases, using substances. For example, in DHR023, the victim (aged 46) and perpetrator (aged 48) lived in a housing association home. The perpetrator had problematic alcohol use, with attempts at treatment unsuccessful. The couple were separated but lived in different parts of the house. They had frequent arguments about alcohol use and financial problems, with the perpetrator threatening to harm himself if the victim did not give him money. In the months prior to the homicide, the perpetrator’s business failed, his mother died, and the victim began divorce proceedings. Despite the victim’s requests, the perpetrator would not leave the home. Shortly after this, he killed the victim with an axe and knife and proceeded to take his own life. Here we see the intersection of the ending of long-term relationships, financial dependency, forced cohabitation, and substance use shaping the homicide context.
The issue of forced/coerced cohabitation was present in several other DHRs and often intersected with financial difficulties and substance use:
In the immediate period before [Victim’s] death, [Perpetrator’s] drug-related behaviour was deteriorating, bringing with it irrational and violent behaviour. . . Following the ending by her of their relationship, [Victim] allowed [Perpetrator] to remain in her flat, because at that time he had nowhere else to go. (DHR072, p. 8, younger)
In these cases, perpetrators were frequently dependent on their victim for financial, physical, and emotional support, with DHRs reporting victims as feeling “very sorry” for perpetrators and “worried” about the effect that leaving might have on them (DHR248, p. 14/15, younger). This was particularly difficult in situations where the perpetrator had care needs. In DHR248, the perpetrator was reported as “desperate” for the victim to stay with him because he was dependent on her not just financially but also for his care: “she would fetch his tablets, his drinks, food, anything” (DHR248, p. 14/15, younger). In the lead up to the homicide, the perpetrator’s awareness of his complete reliance on the victim is illustrated in the texts between the couple, showing “an increasing desperation on [his] part at the thought of [Victim] leaving the marriage.” (DHR248, p. 35, younger). In this case (as with others), a paradoxical intersection between dependency and “ownership” could be seen, with perpetrator jealousy and stalking behaviors appearing alongside significant dependencies.
In cases where substance use, precarity and housing difficulties were less well-evidenced, emotional dependency upon the victim was equally apparent, with family/friends of perpetrators reporting “he said he would kill himself if he and [victim] split up” (DHR310, p. 8, younger) and “he could not survive without her” (DHR257, p. 25, younger). Importantly, entwined with such emotional dependency were significant controlling and coercive behaviors, including victims coerced into maintaining “significant electronic contact via texts and calls, because [perpetrator] found this reassuring” (DHR166, p. 22, younger), and the everyday monitoring and restricting of victim agency: “He controlled the family’s access to the Internet by setting additional firewalls limiting the sites that could be accessed” (DHR238, p. 18, younger). Victims in these cases also reported significant financial control: “[Perpetrator] kept a tight rein on finances and expected [Victim] to account for any money she spent” (DHR238, p. 18, younger), with DHR243 highlighting acutely the intersection of dependency and control:
The perpetrator would give little or no money to [Victim] but would rely on her to put the family’s needs first providing food and clothing for the children from her wages. He restricted her finances to the extent that he managed all of her income, syphoning money that he considered was necessary for such expenditure as on-line gambling. . . (DHR243, p. 19, younger)
Dependency in Older Adults
For older adults, dependency was dynamic and complex, often involving victim, rather than perpetrator dependency, and in some cases, a switching of the dependent/carer role. Prior to deteriorations in their own health, victims had often been carers for perpetrators and had greater responsibility for daily tasks such as cooking, cleaning, and personal care. Where victims’ health declined this meant that perpetrators had to take on such tasks as well as immediate, substantial, and ongoing caring responsibilities (i.e., administering medications, bathing, feeding, dressing, and attending multiple medical appointments). However, given perpetrators’ own poor health, wellbeing, and mobility, they were often not best placed to provide such care. To illustrate, in DHR265, the couple had held very successful careers and had an active lifestyle. As they aged, the perpetrator (aged 77) struggled with severe hearing impairment, which led to feelings of isolation. His diary revealed his deteriorating mental health and self-esteem, exacerbated by his wife’s (aged 79) declining health, possible dementia, and his inability to cope: “Our beautiful world has died with dementia and deafness and my inabilities” (p. 11/12). Less than 2 weeks prior to the homicide, the perpetrator wrote in his diary: “Sorry everybody. . .I can’t cope anymore. . .The last 3 months have been the worst of my whole life” (DHR265, p. 12) and “[Victim] wants to carry on, I don’t think I can” (DHR265, p. 11). Importantly, in this case, the lack of a dementia diagnosis acted as a significant barrier to accessing support options and carer assessment processes.
However, a common feature in older adult IPHS cases was a resistance to external intervention, with services reporting that victims and perpetrators “often declined the offers of help” (DHR192, p. 16, older). At points, such resistance was linked by DHRs to older victims and perpetrators who were “too proud to accept outside help” (DHR195, p. 33, older) with masculine archetypes of older perpetrators as “proud” men: “All those who knew him regarded [Perpetrator] as a proud man who wanted to deal with his own problems” (DHR195, p. 10) and “who wanted to care for his wife to the best of his ability” (DHR192, p. 13).
Nevertheless, although caregivers often declined external support, preferring to manage the care themselves, there were missed opportunities by healthcare professionals to assess the combined care needs of older couples and provide integrated support: “An individual conversation with [Perpetrator by GP] would have allowed him the opportunity to flag up his concerns about [Victim’s] more intimate problems such as incontinence and his increasing inability to cope” (DHR265, p. 21, older).
Theme 3: Mental Health and Suicidality
Although suicidality (thoughts, threats, and attempts) appeared in similar proportions across IPHS and IPH cases, IPHS perpetrators were more likely to have been diagnosed with a mental health condition—most commonly a mood disorder—and acute deteriorations in their mental health were more likely to have precipitated the homicide. Contexts of acute mental health deterioration often related to those themes already discussed, such as separation, loss, and contexts of dependency and caregiving, but also related to intersecting issues of financial insecurity—often feared rather than actual: “[Victim’s] husband became increasingly concerned about financial investments he had made. . .His concerns were unfounded, but nevertheless, they prayed heavily on his mind and eventually, he sought medical attention for it” (DHR143, p. 6, older).
In some cases, such deterioration led to admissions into inpatient mental health facilities, typically when perpetrators presented as suicidal.
The husband initially presented [at hospital] with mental health problems triggered by his difficulties in coping with his wife having left him and the subsequent divorce proceedings. The emotional and financial consequences were causing him distress and he had been abusing and self-medicating with alcohol in an attempt to cope. (DHR089, p. 10, older) [Perpetrator] was pre-occupied, tearful, and referred to a plan of suicide “jumping off a multi storey car park”, he was concerned about an upcoming court appearance to look at the custody of his children as he was concerned that his wife had taped their conversations, he was expressing hopelessness. (DHR307, p. 28, younger)
Unfortunately, in both instances, perpetrator inpatient care ceased too soon—in DHR307 because the perpetrator was “concerned that being an inpatient would affect his bid for custody of his children” and so “expressed his wish to leave the unit” (p. 28), and in DHR089, because the victim agreed to return to the perpetrator to care for him, despite his abusive behavior. In this case, it seemed that a lack of alternative arrangements for supporting the perpetrator led the victim to return to the relationship, a coercive context which limited her “space for action” (Kelly, 2003) and perceived options to leave permanently.
In IPHS involving older adults, the declining mental health of perpetrators was often due to their own deteriorating physical health and/or because of the burden of caring responsibilities. For example, in DHR102, an older perpetrator—who had “historic issues with anxiety and insomnia” (p. 18/19)—made 28 recorded consultations with his GP practice in a 4-month period as he was so impacted by the challenges of his caregiving role. In DHR195, the perpetrator was “severely clinically depressed” (p. 13) due to struggling to care for his wife with dementia whilst himself dying from terminal cancer. At the scene of the homicide, “A note was found on the stairs by the officers indicating [Perpetrator] had killed his wife due to her mental illness and his difficulty in caring for her.” (p. 3).
Concerningly, in several cases where perpetrator mental ill health was significant and enduring, DHRs reported that victims remained “virtually ‘invisible’” and “peripheral to the work being undertaken” with perpetrators (DHR104, p. 9, older). This was despite numerous domestic abuse indicators being present, including perpetrators’ expressed thoughts of killing the victim, relationship difficulties, suicide attempts, and paranoid accusations. Although in part hypothesized as a symptom of mental health practitioners being “less aware of such indicators” (DHR104, p. 10), in cases involving older adults, it was noted that ageist assumptions could be at play, with practitioners “less likely to consider older people as potential perpetrators or victims of domestic violence” (DHR104, p. 10).
Discussion
The aim of this paper was to identify what (if anything) distinguishes IPHS from IPH without suicide, and how the ages of victims and perpetrators shape the risks, vulnerabilities, and contextual features of cases. Our study both reinforces pre-existing knowledge and identifies novel insights to further research, policy and practice in this area.
Several findings from our comparative analysis of IPH and IPHS correspond to and reinforce existing knowledge in the H-S literature. Firstly, that IPHS is highly gendered, with almost all victims being female and perpetrators male (Johnson, 2024; Prévost & Léveillée, 2025; Rouchy et al., 2020; Zeppegno et al., 2019), secondly that IPHS victims and perpetrators tend to be older than those involved in IPH without suicide (Johnson, 2024; Prévost & Léveillée, 2025; Solinas-Saunders, 2024). Thirdly, IPHS victims and perpetrators had increased vulnerabilities related to their physical and mental health (Johnson, 2024; Liem & Roberts, 2009; Solinas-Saunders, 2024). Our analysis indicates that homicides precipitated by acute deterioration in perpetrator mental health were more common to IPHS than IPH. This indicates the differing needs and risks associated with IPHS and the central role of physical and mental health services in the identification and response to domestic abuse (Chantler et al., 2023; Dheensa et al., 2025).
Relational and contextual features also distinguished IPHS from IPH. Our study corroborates previous studies, namely, the longer length of the victim-perpetrator relationship (Flynn et al., 2016), the higher proportion of caregiving relationships (Johnson, 2024), and the lower likelihood of domestic abuse in the relationship prior to the homicide (Solinas-Saunders, 2024). As discussed by others (e.g., Marzuk et al., 1992; Panczak et al., 2013), such differences point to H-S as being “typologically distinct” and therefore a separate phenomenon to IPH. However, our in-depth qualitative exploration by victim/perpetrator age challenges the notion that IPHS is entirely typologically/phenomenologically distinct from IPH, with IPHS involving “younger” adults more closely resembling IPH than differing from it. These younger IPHS perpetrators often had histories of violence, substance use, and in many cases were abusive to the victim prior to the homicide. Further, as with IPH, younger IPHS was often primarily motivated by a desire for retribution after relationship separation (Flynn et al., 2016; Gregory, 2012; Harper & Voigt, 2007; Liem et al., 2011; Solinas-Saunders, 2024). What appears to set IPHS apart, was evidence of perpetrators’ poor mental health, a sense of hopelessness, and fear of financial precarity—characteristics more aligned to victims of suicide (Prévost & Léveillée, 2025). As suggested by Liem and Roberts (2009, p. 327), it is possible that those perpetrators perceiving they have “nothing more to lose” after killing their intimate partner, may have a lowered threshold for suicide post-homicide.
Although difficult to establish whether younger IPHS perpetrators were driven primarily by homicide or by suicide, what featured strongly was their emotional (and sometimes physical/financial) dependency upon the victim, likely intensified by the longer length of their intimate relationship. Such insights parallel the findings of Liem and Roberts (2009) particularly in the context of “symbiotic” relationships. Utilizing a feminist understanding of intimate partner abuse, such dependency was often counterpointed by perpetrators’ dominance and sexism. This was evidenced through their sense of ownership and entitlement, alongside their high need for relational and situational control, ultimately expressed through their killing of the victim (Daly & Wilson, 1988; Salari & Sillito, 2016).
Unlike IPHS involving younger adults, IPHS involving adults over 65 appears to present as typologically distinct, characterized by contexts of poor physical health and caregiver burden (Flynn et al., 2016; O’Neil, 2016; Schwab-Reese et al., 2021), but with limited presence of complex risks related to histories of domestic abuse or perpetrator criminality. This suggests that many of the aforementioned differences could in part be a function of this older cohort, rather than indicating universal differences between the phenomena of IPHS and IPH per se.
In line with previous studies exploring older adult IPHS (e.g., Schwab-Reese et al., 2021; Zeppegno et al., 2019), contexts involved age-related physical and cognitive decline and associated carer burnout. Perpetrators experienced loss of autonomy and despair at a future characterized by infirmity and the pressures of caregiving. Although Joiner (2014) suggests that in this context, H-S can be a “mercy killing” stemming from altruism, we caution against the use of such a term given the extensive evidence that women are more likely to be caregivers to intimate partners (ONS, 2023b), but rarely do they perpetrate a “mercy killing” (Canetto & Hollenshead, 2000; The other Half, 2024). Far from indicating that women are less altruistic than men in caregiving contexts, we argue that notions of hegemonic masculinity instead give shape to, and indeed, encourage, IPHS in this older cohort. Similar to Salari and Sillito (2016) we find that rather than “altruistic,” perpetrators more often had “self-absorbed intentions” (p. 33) and that there is nothing “merciful” about killing a partner. A feminist framing of older adult IPHS fits well with Rosenbaum’s (1990) conceptualization of H-S as a form of “extended suicide,” with the female victim seen as an extension of the male perpetrator’s selfhood—an identity all but lost to age, infirmity and caregiving.
Given the caregiver context, older victims and perpetrators were more likely to have contact with health and social care professionals. However, professionals in these service settings do not necessarily recognize the risks of domestic abuse, ask appropriate/any questions, undertake risk assessments, or they assume that other agencies are responsible for DA support (Chantler et al., 2025; Bows et al., 2024). In their analysis of DHR recommendations for adult social care, Chantler et al., (2025) argued that the intersections of disability, caring, and domestic abuse are key sites of vulnerability. Alongside victims, several older adult IPHS perpetrators in our sample had significant and enduring physical and mental health difficulties of their own, hence there is a need for comprehensive support systems and coordinated care to manage the complex interdependencies in elderly couples.
There was less concrete evidence of prior DA in cases involving older couples and few instances of help-seeking records for DA. However, is it possible that as reviews do not look back over several decades, this, combined with the presence of dependency/care needs, and living in affluent or rural geographical locations may have contributed to making DA less visible in these cases. Such features also connect to limited professional curiosity around DA due to a primary focus on healthcare needs and possible ageist assumptions regarding DA which work to invisibilize it, with fewer opportunities for professional identification and intervention. Arguably, the prevalence of physical and mental health problems means that practitioners across health and social care must be alert to the connection between caregiver burnout and domestic abuse/homicide—particularly in cases involving male carers with physical and/or mental health problems of their own. This will likely be challenging given services’ framing of couples in our sample as “devoted” and “loving.” Such constructions can serve to mask the potential for domestic abuse/homicide in these relationships, with ageist assumptions of older men as less threatening potentially preventing a more questioning stance to behaviors and relational dynamics (Bows et al., 2024).
Our analysis concurs with Marzuk et al. (1992), and Zeppegno et al. (2019), that there are two main types of intimate partner homicide-suicide: those involving younger adults in the context of relationship separation, possessiveness or jealousy, and those involving elderly couples within a caregiving context. However, our gendered analysis extends this conclusion by framing it within the context of patriarchal gender norms and hegemonic masculinities that encourages sexism toward women—by younger and older IPHS perpetrators respectively—both of which have been used as explanatory frameworks for DA (Levell & Hester, 2023), particularly for younger perpetrators.
Regarding the older cohort, hegemonic masculinities is a helpful framing, specifically related to the feminization of care. For older male carers, there is a “role reversal” where they are now expected to undertake caring and run the household, contrary to ideas of hegemonic masculinity. The feminization of care therefore places male carers in positions that are at odds with hegemonic masculinity (Connell, 1987) which discusses a collective “pattern of practice,” reflecting social structures that “allow[ed] men’s dominance over women to continue” (Connell & Messerschmidt, 2005, p. 832). Our analysis evidences hegemonic masculinity operationalized where older men have strong notions of what it means to be a man and the social relations it speaks to: breadwinner, in charge of and responsible for the family, capable, and strong. These ideas of masculinity can work in two ways. Firstly, this presentation can influence professionals’ assessments, as strength is not equated with having needs. The notion that both strength and vulnerability can be present is overlooked in the performance of hegemonic masculinities. Secondly, the burden of hegemonic masculinities works to make men reluctant to accept help when offered. This two-way interaction of hegemonic masculinities is clearly unhelpful. The loss of independence and autonomy which comes with care responsibilities, should not be underplayed and professionals have a key role to ensure that carers have a carer’s assessment to help support them. Where help is refused, more in-depth work is required to understand reasons for refusal. We acknowledge that Adult Social Care services in England and Wales are under immense pressure due to sustained cutbacks in welfare provision and so may close a case once carers have refused help. Further, depending on the financial situation of the couple, couples may have to finance care themselves which may contribute to refusing help. Whilst we recognize these contextual features, we argue that this does not legitimize the idea of “mercy killing” and that the gendered nature of these killings should be fully acknowledged.
Given the differing presentation of IPHS in older and younger adults, professional responses in this area need to be attuned to the specific situational contexts involved (Vatnar et al., 2021), with specific risks relating to separation and caregiving contexts understood by health and social care practitioners.
Conclusion
Our paper analyzed what (if anything) distinguishes IPHS from IPH without suicide, and how the ages of victims and perpetrators shape the risks, vulnerabilities, and contextual features of cases. Our analysis illustrates many points of convergence with existing literature, namely the many similarities between IPHS and IPH, particularly for those IPHS involving people aged 65 and under. For both groups (under and over 65) three themes were identified from close reading of DHRs: i) separation and loss, ii) dependency and iii) mental health and suicidality. However, these three themes had vastly different meanings structured by age, with different implications for policy and practice. The first two themes are argued to be underpinned by hegemonic masculinity whereby gender roles are tightly defined with men needing to be in control over their environment (including their partners/spouses). This works to obscure their vulnerabilities, thus missing important opportunities for intervention. In a hard-pressed health and social care environment, refusing help will often result in closing the case rather than an in-depth exploration of why such help is being turned down. In relation to our third theme, although suicidality appeared in similar proportions across IPHS and IPH cases, IPHS perpetrators were more likely to have been diagnosed with a mental health condition—most commonly a mood disorder—and acute deteriorations in their mental health were more likely to have precipitated the homicide. General (Medical) Practitioners (GPs) have a key role in relation to perpetrators’ declining mental health and victims’ physical and mental health. Common mental health problems are widely diagnosed so focusing on those patients that are potential candidates for H-S or indeed IPH is challenging.
The specific contextual issues for older cohorts may help with narrowing down the potential pool of relevant patients, namely “role reversal” where the man is now the primary carer and home manager and despair at a future with diminishing autonomy and control due to the victims’ and their own ill-health. These are challenging and difficult circumstances, yet we strongly refute the term “mercy-killing” which is often used to describe such homicides. Instead, strengthening responses to domestic abuse in both the statutory sector and DA specialist sector is key and understanding the different manifestations of distress and control structured by age is central. Additionally, understanding the dynamics of gender and the care context, conducting carers’ assessments, displaying appropriate professional curiosity around refusal for help and remaining victim-survivor-centric is key to preventing these deaths. These findings are likely to have relevancy at a wider level, as globally we are an aging population with an increasing care burden (World Health Organisation [WHO], 2025). The World Health Organisation is also concerned that older people are invisible within the Sustainable Development Goals (SDGs) (WHO, 2024). This paper helps to highlight a specific issue particularly relevant to SDG 5 (Gender Equality).
In relation to younger couples, our research confirms previous studies where a key motivator for homicide is potential or actual separation from the victim. Ideas of hegemonic masculinities are important here too, as perpetrators’ sense of entitlement and control are paramount. Suicidal ideation and behavior may be displayed as part of a coercive and controlling relationship and works to deter the victim from leaving the relationship. Alternatively, such behaviors may also be indicative of deteriorating mental health. As domestic abuse was more commonly recorded in DHRs pertaining to younger couples, this highlights the importance of mental health practitioners, substance use workers, and adult social care understanding this context, inquiring about domestic abuse, utilizing a gendered framework, and responding in a manner which works to protect victims—a much needed and overdue response. The following recommendations for policy and practice lead from this study’s key findings.
1) Where older adults are turning down health and social care support, practitioners should explore the reasons for this, including how normative gender roles may influence such refusals. Contact should be maintained, with regular reviews to assess ongoing support needs, and with suitable adaptations to encourage engagement.
2) Health and social care practitioners (particularly GPs) should be cognisant of the risks posed by the caregiver context in older adulthood, particularly where men are caring for female partners. Older male carers discussing fears and concerns around the loss of independence and autonomy, stresses around coping with caring, and managing their own care needs alongside those of their partner should be viewed as possible indicators of escalating need. Such indicators should be responded to with early intervention including sensitive enquiry and the implementation of care plans addressing the needs of both the cared for and the carer, underpinned by comprehensive carers assessments.
3) Training and professional development for health and social care, substance use, and DA specialist sector practitioners should include exploration of how age, gender and hegemonic masculinities shape the contexts, indicators, and appropriate professional responses to domestic abuse/homicide. For example, that dependencies of all forms represent potential sites of risk and perpetrator control—with age-related contexts of (typically) declining physical and cognitive health in older adults and complex co-morbidities involving substance use in younger adults.
4) Mental health practitioners and GPs should ensure that assessments of relational risk are prioritized where individuals are displaying suicidal thoughts/behaviors and/or there is a significant decline in their mental health.
Footnotes
Acknowledgements
The support of the Economic and Social Research Council (ESRC) is gratefully acknowledged. Grant Reference: ES/S005471/2.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council [grant number ES/S005471/2].
Ethical Considerations
Ethics approval was not required due to the source material being pre-anonymized, publicly-available documents.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
All domestic homicide reviews (DHRs) analyzed within this study are hosted within the HALT repository https://domestichomicide-halt.co.uk/ and on the UK Home Office DHR repository ![]() . The quantitative data utilized within the HALT study is hosted by the UK Data Service. Study number 855879.
. The quantitative data utilized within the HALT study is hosted by the UK Data Service. Study number 855879.