
Abstract
This study provided a detailed description of the experiences of 60 treatment-seeking children and young people following parental intimate partner homicide (PIPH) in the United Kingdom, and evaluated the potential effectiveness of the traumatic grief focused cognitive behavioral therapy they received. A paired samples t-test showed that mean pre-and post-treatment posttraumatic stress scores decreased significantly, with a large effect size. Reliable change indices indicated that 75% improved and 25% remained unchanged. Despite the severe consequences for children and young people following PIPH and the great variability in their experiences, results promisingly show that they may benefit from treatment.
Introduction
Despite growing interest in the wellbeing of children and young people following parental intimate partner homicide (PIPH), research remains scarce and often relies on small samples. Losing a parent to PIPH can gravely impact children and young people’s mental health and is a risk factor for long-lasting mental health problems including posttrauamatic stress disorder (PTSD), depression, and prolonged grief disorder (PGD) (Alisic, Groot, Snetselaar, Stroeken, Hehenkamp, et al., 2017; Berg et al., 2016). It has been suggested that many of these children/young people may benefit from treatment. However, few empirical studies have evaluated such interventions. In fact, in many cases, it remains unclear what happened to these children and young people in the aftermath of the homicide (Stanley et al., 2019).
The current study sought to contribute to knowledge about the experiences and wellbeing of children and youth following PIPH. We aimed to do so by providing a brief overview of existing literature on their experiences and mental health. To extend this literature, we then aimed to provide a detailed description of the circumstances and experiences of a group of treatment seeking children and young people before, during and following PIPH (Aim 1). Furthermore, to establish an evidence-base for treatments tailored to the needs of this group, Aim 2 was to evaluate the potential effectiveness of a traumatic grief focused cognitive behavioral therapy (TGF-CBT) that this group received, using routine outcome monitoring (ROM) data that were collected before and after treatment for diagnostic and evaluation purposes.
Background
While the incidence of intimate partner violence (IPV) has declined worldwide over the past 25 years (Catalano, 2013), its occurrence is still widespread and remains a major concern. Between April 2012 and March 2018, 2998 homicides took place within England and Wales (Home Office, 2020). Of these, 575 (19.2%) were labeled as intimate partner homicide (IPH). In existing literature, some common characteristics and risk factors for IPH are described. In the large majority of cases (80.7%), the victim is a female and the perpetrator their male partner or ex-partner (Home Office, 2020). IPH accounted for almost half (42.8%) of all homicides with female victims, whereas for males, this constituted only 3.3% (Home Office, 2020). Despite men being the perpetrator in the vast majority of all homicides including IPH, in the case of IPH, females account for a relatively greater proportion of offenders compared to other types of homicides (Overstreet et al., 2021).
In most cases of IPH (67%–80%), IPV took place prior to the homicide (Campbell et al., 2007). Furthermore, evidence suggests that marginalized communities such as ethnic minorities are disproportionately affected by IPV (Breiding et al., 2014). Having access to a weapon that is readily available at the crime scene further increases the risk for IPH. Therefore, in IPH, as compared to other homicides, firearms are less likely to be used, while strangulation, suffocation and the use of knives are more common (Overstreet et al., 2021). The crime scene is most often a private location, such as in or around the victim’s residence (Corsaro et al., 2017). Further known risk factors include substance abuse and lower education level of both perpetrator and victim, a history of mental health problems and unemployment of the (male) perpetrator, and the (female) victim being separated from the perpetrator and having children from a previous relationship, especially when the children are living in the home (Spencer & Stith, 2020).
A report on domestic homicides covering the period from 2010 to 2015 stated that in just under half of cases of IPH, dependent children were present in the family structure (Home Office, 2016). This implies that with an average of 1.92 children per family (Office for National Statistics, 2015), approximately 50 children a year faced the death of a parent at the hands of the other parent in England and Wales in the period that the current study focused on, between 2012 and 2017. The current literature on IPH is largely focused on prevention, interweaved with investigating the IPV that often precedes IPH, or on characteristics of the offender. Few studies have systematically examined the wellbeing of children involved in the aftermath of IPH (Alisic et al., 2015), despite several attempts made by researchers and policy makers to make these “forgotten,” “silent,” “invisible”, or “secondary” victims of crime more visible.
In England and Wales, multi-agency reviews are written about the circumstances of death following a homicide. Since April 2011, these so-called Domestic Homicide Reports (DHRs) have been a statutory requirement for local areas in which the death of a person aged 16 or over has, or appears to have, resulted from violence, abuse or neglect by a person to whom they were related or with whom they were, or had been, in an intimate personal relationship or within the same household (Home Office, 2016). A recent study by Stanley et al. (2019) examined children’s experiences following domestic homicides in 2011 through 2016 by analyzing these reports. They concluded that their study “has revealed much about the continuing invisibility of children living with domestic violence and abuse” (p. 74) as their experiences were often overlooked in research and reports.
Experiences of Children and Young People Following PIPH
Children and young people who are faced with PIPH may lose two parents at once: one to death, and one to jail, fleeing or suicide (Steeves & Parker, 2007). In most cases, the mother is the victim and the father or the ex- or new partner of mother, the offender (Alisic, Groot, Snetselaar, Stroeken, & van de Putte, 2017; Velopulos et al., 2019). In addition to processing the death of their parent at the hands of the other, and the traumatic circumstances under which this occurred and that some of them witnessed, PIPH bereaved children and young people face many additional challenges. As the family home has often become a crime scene, they might be denied access to their home, toys, photos, clothes (Steeves & Parker, 2007). Oftentimes, the new living situation and care arrangement with the family of the deceased or the perpetrator’s side results in separation of siblings, friends and change of school. Working out the care arrangement can create stress and conflict within the family (Alisic, Groot, Snetselaar, Stroeken, Hehenkamp, & van de Putte, 2017). Living with family of the killed or the offender parent may determine whether the child or young person has contact with the offender parent, which can greatly affect their experience.
Furthermore, PIPH bereaved children and young people may experience stigmatization resulting from trial procedures and media attention. “Disenfranchised grief” can occur when “there is no social recognition that the person has a right to grieve or a claim for social sympathy or support” (Doka, 2002, p. 5), specifically when the child or young person grieves a parent who was also a perpetrator. Amidst all this, the people who would usually help them cope with the loss of a loved one are no longer there. They have to form attachment bonds with new caregivers, who may experience symptoms of PTSD, depression and/or PGD themselves, carry hatred toward the offender parent, or, in the case of being related to the offender, condone the violence (Alisic et al., 2012).
Mental Health of Children and Young People Following PIPH
Although children and young people confronted with PIPH have an increased risk for developing PTSD, depression, and PGD, a systematic review on the mental health and well-being of children aged 0 to 18 after PIPH (Alisic et al., 2015) underlined the importance of looking beyond purely psychological symptoms. Responses to parental homicide vary greatly between individuals and may impact physical, social, and academic domains of child development. During childhood and adolescence, the developing brain is more sensitive to adversity and stress (Lupien et al., 2009). The loss of a parent, with whom the attachment bond is especially strong during childhood and adolescence, can result in loss of security and stability (Alvis et al., 2022). This may lead to various emotional, social and behavioral problems which may impact mental health throughout adulthood (Melhem & Brent, 2016).
Considering the potential broad and long-lasting effects on their wellbeing, it has been suggested that all children and adolescents can benefit from bereavement counseling or psychotherapy following PIPH (Kapardis et al., 2017), and that short-term care may likely be insufficient to meet their needs (Alisic, Groot, Snetselaar, Stroeken, Hehenkamp, et al., 2017). However, only few receive such intervention (Stanley et al., 2019). Furthermore, few empirical studies have evaluated such interventions. One goal of the current study was to address this issue by using routine outcome monitoring data of children and young people following PIPH and who received treatment. A recent study found that PGD can be successfully reduced in bereaved children and adolescents using CBT (Boelen et al., 2021). The study demonstrated statistically significant reductions in symptomatology overall as well as reliable individual changes in symptoms; these findings converge with prior findings (Layne et al., 2008; Spuij et al., 2013). Furthermore, a recent systematic review indicates that overall, symptoms of PGD, PTSD, and depression decreased significantly in adults who lost a loved one to homicide following psychological interventions (Alves-Costa et al., 2021). Accordingly, we hypothesized that the children and young people described in the current study would display (a) a statistically significant and (b) clinically significant decrease in posttraumatic stress (PTS) symptom severity following the TGF-CBT they received.
Method
Study Design
The present study is a retrospective, naturalistic pre-test post-test study: treatment methods were not experimentally controlled but were measured retrospectively by therapist report. Data were collected in the context of routine outcome monitoring for diagnostic and evaluation purposes of the treatment participants received, consisting of pre-treatment and post-treatment symptom scores. Pre-treatment/post-treatment comparisons were used to indicate change in symptom severity.
Participants and Procedure
This study is part of a larger study (Soydas et al., 2020) investigating mental health outcomes and response to treatment in homicide survivors in the United Kingdom (UK), using ROM data of both children and adults seeking treatment through the National Homicide Service as provided by ASSIST Trauma Care across England and Wales. For the current study, we used a subsample of these data, specifically, of PIPH bereaved children and young people who underwent TGF-CBT.
Data for the current study were collected between January 2011 and December 2017.
A self-report questionnaire on PTS (described below) was administered at intake (T0) and at the end of treatment (T1). For the current study, data of 60 PIPH bereaved children and young people who engaged in TGF-CBT were available and included for the first aim of our study. Information about demographics, events leading up to and following the homicide, as well as the homicide itself, and judicial procedures, was documented in the client’s treatment files. Furthermore, it was indicated whether the client was related to other clients who sought treatment at the same specialized facility.
For the second aim, to compare pre- and post-treatment scores, we omitted the scores on questionnaires of 12 children aged between 0 and 7 as the questionnaires have not been validated for that age group. For three of the remaining 48 children and young people, no pre- and post-treatment scores were available. Finally, for five, no post-treatment scores were available. This left a total of 40 children and young people for whom questionnaires at both T0 and T1 were available and who were thus included in our analyses. The flowchart in Figure 1 gives an overview of the children and young people included in the final sample.
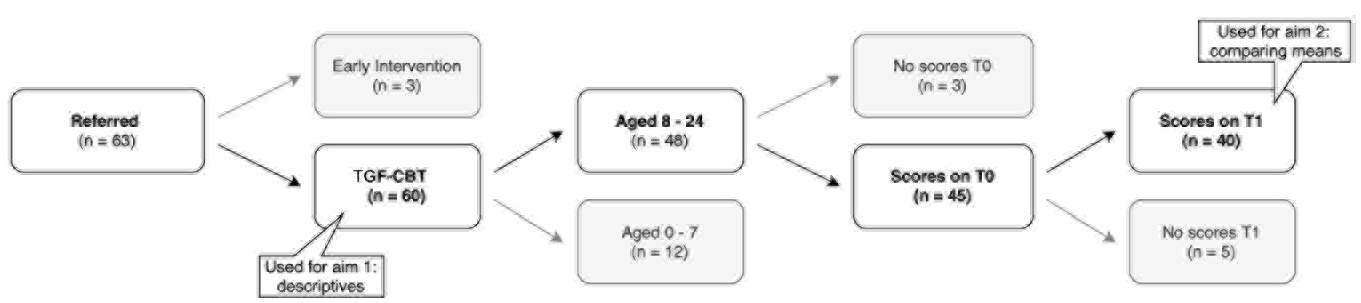
Flowchart of patients included in the study.
When available (due to their own referral to the same facility), and when given written consent to do so, ROM data of referred caregivers were also included in the current study. In total, 24 PIPH bereaved children and young people in our sample had a caregiver who was also referred. Of 22 of these caregivers, pre-treatment scores were available, and of 19 of these, also post-treatment scores.
Mean therapy duration (n = 40) was 15.31 (SD = 8.70) hr.
Ethical Standards
The Ethics Committee of the Faculty of Social and Behavioral Sciences of Utrecht University evaluated this study and deemed it exempted from formal review by the Dutch Act on Medical Research Involving Human Subjects (filed under number 20-0228). The study was conducted in accordance with ethical guidelines from the UK for service evaluation (cf. Soydas et al., 2020). Children and young people were given oral information about the course of treatment and study procedures, after which they, or their caregiver, gave written informed consent. All information from the clients’ files was anonymized and entered into a dataset that was made accessible only to the researchers and stored on a secured server.
Treatment
In accord with the clinical guidelines of the National Institute for Health and Care Excellence (NICE) for mental health care (National Collaborating Centre for Mental Health, 2005; World Health Organization, 2018), ASSIST Trauma Care offers TGF-CBT adjusted to the developmental level of the child. TGF-CBT originates from trauma focused CBT (TF-CBT), which is a form of psychological treatment encompassing psycho-education about traumatic reactions and the treatment; exposure to feared stimuli to learn that safe (but feared) stimuli need not to be avoided; and cognitive restructuring to become aware of, and change unhelpful thoughts (Zayfert & Becker, 2019). In TGF-CBT, grief-focused components are added to the trauma-focused opponents. These include both trauma and grief education in which the characteristics of the traumatic loss are discussed and basic information on cognitive processing and attachment reactions is given; grieving the loss and reducing traumatic reactions associated with the traumatic death by imaginal exposure with the use of mementos, such as objects linked to the deceased, and drawing or writing assignments to express intense emotions; and finally, cognitive restructuring by resolving ambivalent feelings about the loved one who died, preserving positive memories, and redefining the relationship with the person who died to one of memory (Boelen et al., 2021; Mannarino & Cohen, 2011; Smid et al., 2015; Smid, van der Meer, et al., 2018). TGF-CBT consists of approximately 15 sessions.
Key elements of the model of care as provided by ASSIST Trauma underlying this treatment are: timely and specialized assessment, application of time limited sessions, attention for legal and court proceedings, implementation of evidence-based traumatic grief focused CBT interventions (Boelen et al., 2006; National Collaborating Centre for Mental Health, 2005; Smid et al., 2015), provision of an outreach model of care with the possibility to engage in sessions at the homes of the clients, individual treatment with the possibility to engage other family members, deployment of qualified and experienced therapists supervised by the Oxford Cognitive Therapy Centre and close collaboration with caseworkers of Victim Support to provide practical and judicial support throughout the process. Consequently, the broad range of emotional, practical and judicial consequences that those bereaved by homicide are confronted with (Soydas et al., 2020), are addressed.
Consistency of therapy was fostered as all therapists were trained in TGF-CBT, through regular supervision and annual continuing education by the Oxford Therapy Center and through monitoring of therapy by a case manager and periodic team meetings.
Measures
Children’s Revised Impact of Event Scale (CRIES-8)
For children and young people aged 8 through 18 years, the CRIES-8 (Horowitz et al., 1979) was administered to measure self-reported symptoms of PTS as defined in the DSM-IV. Respondents indicated how frequently they experienced each of eight symptoms, such as “I had dreams about it,” during the past 7 days. The items are scored on a 4-point scale with anchors 0 (not at all), 1 (rarely experienced), 3 (sometimes experienced), and 5 (often experienced). The items are clustered in two subscales named intrusion and avoidance, each consisting of 4 items. Together, they make up a total stress score between 0 and 40, with a higher score indicating more traumatic stress. Following Perrin et al. (2005), a score of 17 or higher was used as a cut-off for clinically relevant scores.
For young people aged between 19 and 24 years, and for caregivers who were all older than 18 years, the Impact of Event Scale-15 (IES-15), validated for ages 18 and above, was administered. This questionnaire includes the same 8 items and 7 additional items (e.g., “I stayed away from reminders of it”), clustered together in the same subscales (Horowitz et al., 1979; Perrin et al., 2005).
In prior research, a strong correlation was found between the IES scores of adults, adolescents and children (e.g., Joseph et al., 1993; Sack et al., 1998). Furthermore, both the child 8-item and the child 13-item version have been applied to adult populations (John & Russell, 2007; Veronese & Pepe, 2013). We therefore chose to remove the scores on the additional 7 items for the young people and use the remaining 8-item version so that we could combine the data of the different age groups.
Mean inter-item correlation (MIIC) of the complete questionnaire consisting of eight items used for all children and young people in the current study was .13 and fell below the optimal range of .15 - .50 as recommended by Clark and Watson (1995). Deletion of single items would not improve the inter-item correlation. Since some items from the intrusion subscale correlated negatively with items from the avoidance subscale, we re-calculated the MIIC for the two subscales separately. This resulted in a MIIC of 0.25 for both the avoidance and the intrusion subscale, with positive correlations only, indicating that the sample used in the current study may present with incongruous intrusion and avoidance symptoms. Considering the heterogenous nature of the two subscales, we considered the total mean-inter item correlation acceptable for the purposes of our study and continued with the complete scale.
Sociodemographic, Homicide Related, Judicial and Therapy Related Variables
Data from the 60 children and young people included in our study were gathered from their client files and included data on age, gender, ethnicity, family composition and referral information about family members who were referred for the same treatment, prior exposure to domestic violence (DV), whether or not the child or young person was a (possible) witness to the homicide, whether the suspected offender had (a) committed suicide, (b) been hospitalized, (c) been incarcerated, or (d) been released, whether the child or young person had moved following the homicide, whether the funeral was held before or during the therapy or was not held yet by the end of therapy, whether a verdict was reached before or during the therapy or was not yet reached, and whether the child or young person had and wanted any contact with the offender.
Statistical Analyses
For our first aim, we adopted the categorization as used by Alisic, Groot, Snetselaar, Stroeken, & van de Putte (2017) to describe the experiences of the children and young people. We generated the descriptive statistics from SPSS (version 26.0; IBM). For our second aim, we checked assumptions and conducted the analyses using SPSS. To investigate hypothesis A, we used a paired samples t-test to compare the average total score on the CRIES-8 at pre-treatment and post-treatment. We then calculated the effect size (Cohen’s d) for within group effects. To interpret this result, we calculated the common language effect size for correlated samples (McGraw & Wong, 1992), and used the percentage associated with the upper tail probability of this value (Lakens, 2013).
Since most of the 40 children and young people that we included in our analyses were not nested within families (n = 28), we did not use a multilevel framework. To check whether it was necessary to control for a possible dependency of data between the 12 siblings belonging to six families within this dataset, we calculated the paired samples t-test and effect size twice: once for the 28 unrelated children and young people and six siblings who were randomly selected from their nine families (n = 34), and once for the full sample containing all children and young people including all siblings (n = 40). As the two t-tests and effect sizes were virtually similar we continued with the total sample including all siblings.
For hypothesis B, we calculated the Reliable Change Index (RCI) to evaluate individual changes in PTS from pre-treatment to post-treatment using the formula by Jacobson and Truax (1991): RCI = (X2−X1)/Sdiff, with X2 representing a participant’s score at post-treatment, X1 representing scores at pre-treatment, and Sdiff is calculated using the test-retest reliability and the standard deviation of the pre-treatment scores. Based on Jacobson and Truax’ recommendations, an RCI > |1.96| was considered as representing clinically significant change and was used to categorize participants into “improved,” “unchanged,” and “worsened.” Finally, we compared the frequencies of the descriptive statistics between these categories to describe any emerging similarities and differences.
Results
Demographic and clinical characteristics of the total sample of 60 children and young people who engaged in TGF-CBT are shown in Tables 1 to 3. On average, mean age at the time of the homicide was 11.3 years (SD = 5.8) and 12.2 years at the time of referral (SD = 5.6). Frequencies in different age groups were n = 23 for participants aged 0 to 9 years, n = 25 for participants aged 10 to 16 years, and n = 12 for participants aged 17 to 24 years. About half of the sample (53%) was female. Frequencies in ethnicity, following the classification of ethnicity in the UK as defined in the 2001 UK Census (Office For National Statistics, 2020) were “white British”: n = 46, “white Irish”: n = 1, “Other white”: n = 3, “white and Black Caribbean”: n = 1, “Other mixed”: n = 2, “Pakistani”: n = 2, “Black African”: n = 2, and “Other Black”: n = 3. The mean time since bereavement at the time of referral was 45.7 weeks, ranging from 1 week to 8.9 years (median = 14.0 weeks, IQR = 56.0 weeks). The children and young people in our sample had received between 4 and 52 hr of therapy, with a mean of 15.3 hr (SD = 8.7). Of the sample of 40 children and young people with available pre- and post-treatment scores, at the start of treatment, 36 (90%) scored above the cut-off for clinically relevant PTS-scores, whereas four (10%) did not. At the end of treatment, eight (20%) still scored above this cut-off, while 32 (80%) did not.
Patient/Family, Deceased Parent, Perpetrator, and Homicide Characteristics for the Total Sample and the RCI Categories “Improved” and “Unchanged.”.
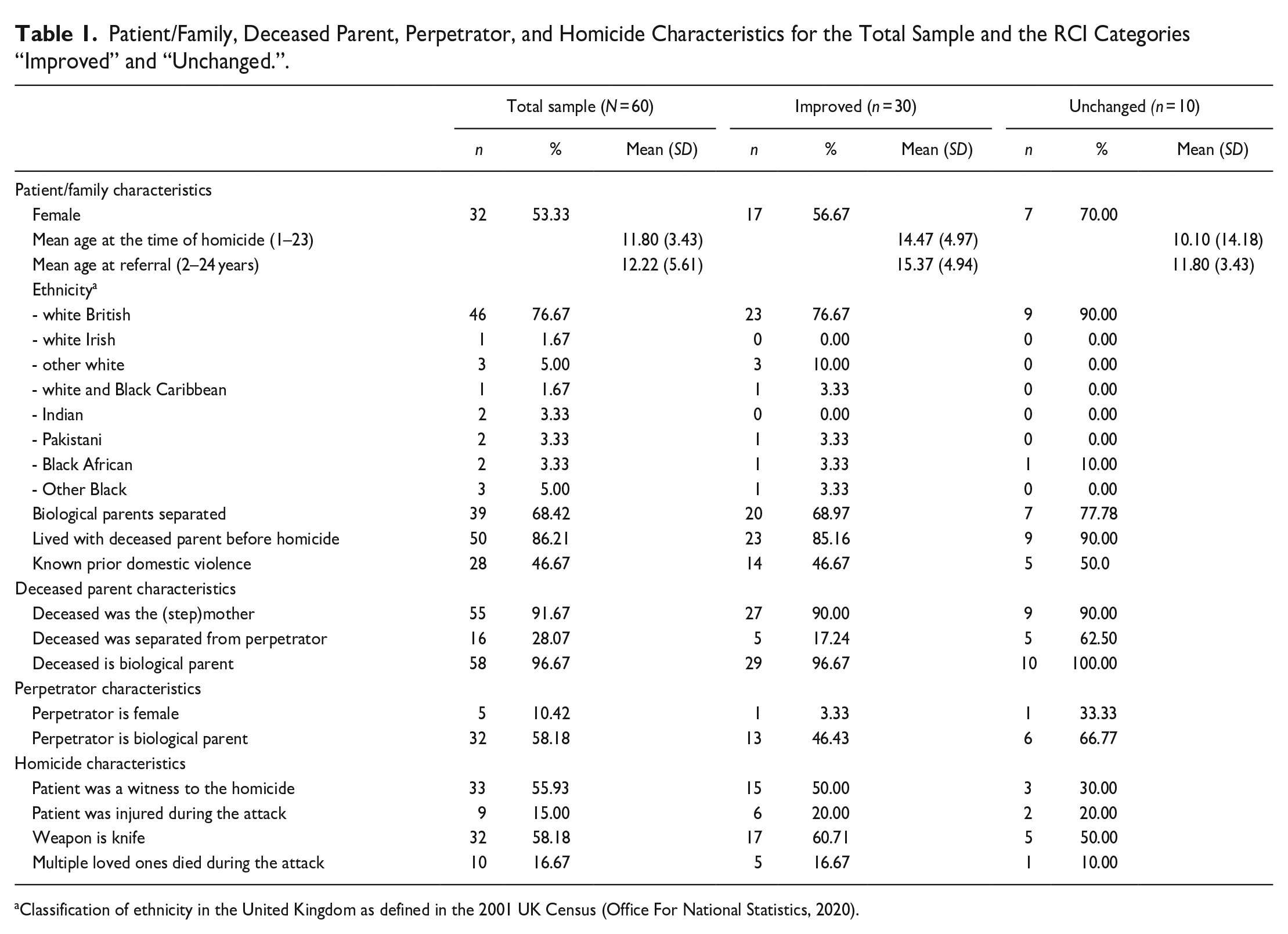
Classification of ethnicity in the United Kingdom as defined in the 2001 UK Census (Office For National Statistics, 2020).
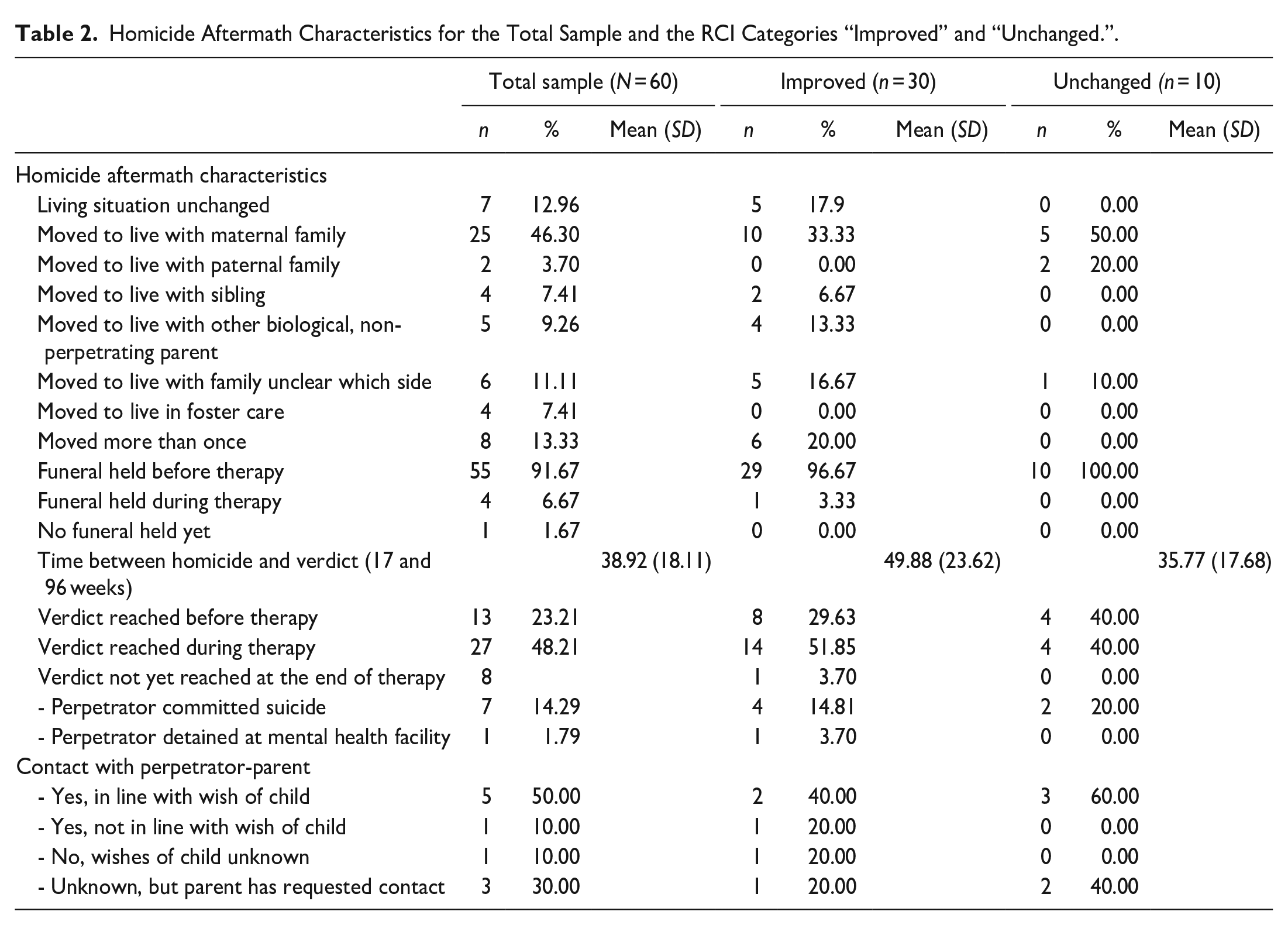
Homicide Aftermath Characteristics for the Total Sample and the RCI Categories “Improved” and “Unchanged.”.
Therapy Characteristics for the Total Sample and the RCI Categories “Improved” and “Unchanged.”.
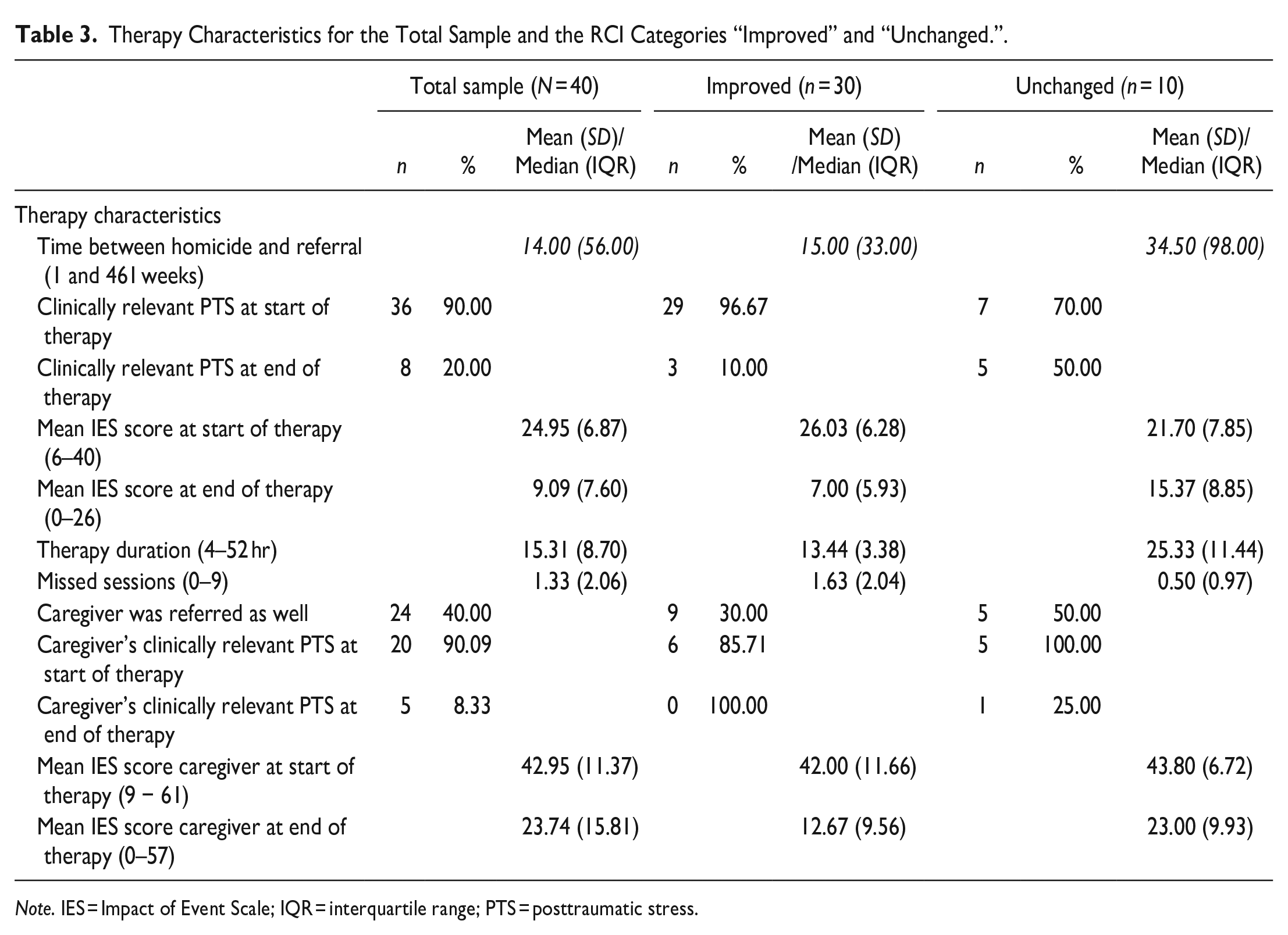
Note. IES = Impact of Event Scale; IQR = interquartile range; PTS = posttraumatic stress.
Objective 1: Description of the Total Sample (N = 60)
An overview of patient/family, deceased parent, perpetrator, and homicide characteristics is given in Table 1. An overview of the characteristics of the homicide aftermath and the therapy are given in Tables 2 and 3, respectively. Characteristics with insufficient data for meaningful interpretation were not included in the tables.
General Description of the Complete Sample
Although the characteristics varied greatly, generally speaking, the following applies to our sample: about half of the children and young people were female, most were classified as “white British,” most had lost their biological mother and lived with the deceased at the time of the homicide; the deceased was separated from the perpetrator who in the majority of cases was their biological parent; it was unknown whether there had been any prior exposure to violence; in just over half of the cases, they were a witness to the homicide which happened most often by stabbing, a small but significant proportion got severely injured themselves during the attack; the median time since bereavement was 14.0 weeks; the funeral was held before the start of therapy; a verdict was most often reached during the course of therapy and all cases reached a guilty verdict; the living situation of most children and young changed and most came to live with their maternal grandparents; and there was very little information about whether or not they remained in contact with their offender parent. In about half of the cases for whom this was known, the child wanted and had contact with the offending parent. Finally, the large majority scored above the cut-off for a clinically relevant PTS-score at the start of treatment, but did no longer meet that criterium at the end of treatment.
Domestic Situation Prior to the Homicide
In 55 cases, the deceased was the (step)mother and the perpetrator her male (ex-) partner (vs. five cases where the (step)father was killed by his female (ex)-partner). In 58 cases, the deceased was the biological parent. In 39 cases, the biological parents were separated at the time of the homicide. In 41 cases, the deceased was in a relationship with the offender at the time of the homicide. Fifty children and young people lived with the deceased parent at the time of the homicide. In the other cases, they had either moved out to live on their own (four cases), lived with the other (biological, non-perpetrating) parent (one case), lived with other relatives (one case), or lived in foster care (one case).
Domestic Violence and Involvement of Other Organizations
In 28 cases, domestic violence prior to the homicide was reported, while for the other 32, this was not documented. In five cases, it was documented that the reported violence was also directed against the children/young people, and in two cases this also involved sexual abuse of the children/young people. There was no documentation about whether or not the family was known to Social Services prior to the homicide. In one case, it was documented that reports of DV had been made to the police prior to the homicide. Information on the mental health of the parents or partners of the parents was largely unknown. There were two documented instances of substance abuse by the victim or the perpetrator prior to the homicide, which were reported during therapy.
In eight cases, it was documented that Social Services were involved in the aftermath of the homicide. In seven cases, Child and Adolescent Mental Health Services (CAMHS) were involved before, during or following the current treatment, and in two cases, a referral to a local therapist/grief support group was made following the current treatment.
Exposure to the Homicide (Witness)
Therapists documented that 33 children and young people had directly witnessed the homicide; 26 did not witness the homicide and for one case, it was unknown. Although it was not known for all of those who were a witness, at least nine were injured themselves during the homicide (e.g., stabbing, suffocation, sexual abuse, or burning by the perpetrator, or fractures as a result of fleeing the house). The description of the experiences of children and young people who witnessed the homicide varied greatly. Some were simply described as being a witness to the attack. In three cases, it was initially assumed that despite them being present, they had not witnessed the homicide (e.g., because they were thought to be asleep or in a different room), and it only became apparent during therapy that they had witnessed the events. In four cases, the children and young people were the ones to discover the body. In other cases, the children and young people were found at the crime scene covered in blood (three cases), had wrestled with the offender parent trying to save the other parent’s life (two cases), or had been able to flee the scene (five cases). This variability did not only exist between cases, but also between siblings within the same family.
Type of Homicide
In 32 cases, the children and young people lost their parent due to stabbing. Other known causes of death were strangulation (seven cases), burning (four cases), beating (four cases) and the use of a gun (two cases). In 10 cases, the child or young person additionally lost one other family member during the homicide, such as a sibling, grandparent or (ex) partner of the deceased parent.
Funeral
In 55 cases, the funeral took place before the start of therapy. For four, the funeral took place during therapy. In one case, the funeral had not yet taken place at the completion of therapy.
Course of Justice of the Offender
The time between the date of the homicide and the date of the (initial) verdict ranged between 17 and 96 weeks, with a mean of 38.9 weeks (SD = 8.1). Before the onset of therapy, for 13 cases, a verdict was spoken. During the course of therapy, another 27 cases reached a verdict. Eight cases were still ongoing during the last therapy session, and for six cases information about the course of justice of the offender was not available. In eight cases, a trial was not possible, due to suicide (seven cases) by or hospitalization at a mental facility (one case) of the offender. Of the 41 cases that we were able to identify that reached a verdict, all offenders were found guilty. Some children and young people reported to be very happy with the outcome of a long sentence whereas others firmly believed in the innocence of their parent and wanted to appeal.
Housing Situation Following the Homicide
Of the 50 children and young people whose living situation changed following the homicide, 25 came to live with their maternal grandparents or other family of their mother’s side. Five went to live with their previously separated biological parent who was not the offender, four with a sibling, and four in foster care. Three children and/or young people went to live with their paternal family, one of whom went to live with their maternal family during the therapy. Four were taken into custody by their family but it was unclear whether that was their maternal of paternal family. For six, the housing situation following the homicide was unknown. Although in most cases, siblings remained to live together, two siblings went to live separately following the homicide. For eight children and/or young people, it was known that they were forced to move more than once after the homicide: some started with family but ended up in foster care, moved from paternal to maternal family members, or moved from grandparents to extended family or the other way around. Two moved to live with another family member due to conflicting views regarding talking about the homicide or wanting contact with the offender parent.
Contact With the Offender (Step)Parent
There was very little information about the children and young people having or wanting contact with their offender (step)parent: in 37 cases, there was nothing reported in the client’s treatment file about this. In five cases, it was reported that the children had contact with the perpetrator parent, in accordance with the children’s wishes. Despite having been told the truth of what had happened, three of these were struggling to believe that their parent was guilty or firmly believed in their innocence. Two believed their parent was guilty and either supported the parent or wanted contact to make sense of what had happened. One child or young person is reported not to have contact with their parent as their new caregiver disapproves, although the wish of the child is unknown. In four cases, the perpetrating parent requested or initiated contact with the child. For three of these cases, it is unknown whether the child or young person wanted contact and whether contact was established. In one case, contact was initiated against the wishes of the child or young person. Furthermore, it was undisclosed to three children and/or young persons that it was their parent who was the perpetrator, but it is undocumented whether they wanted or had contact with the perpetrator parent.
Mental Health of Family Members
Thirty-seven children and young people had a family member who had also been referred to ASSIST Trauma Care. In 24 cases, this was their new caregiver. For 22 caregivers, pre-treatment PTS-symptom scores as measured by the IES-15 were available, with 20 scoring above the cut-off for a clinically relevant score. In total, 19 caregivers engaged in a full course of therapy themselves and had their scores taken at the end of their treatment, with five still scoring above cut-off, and 14 scoring below cut-off. Two caregivers received the early intervention only and no end scores were obtained. No further information regarding the mental health or course of treatment of the new caregivers was available for this study.
Objective 2: PTS-Symptom Change Following Treatment
For the second objective of this study, we tested for differences on pre-treatment PTS-symptom severity, age, and gender between children and young people (aged 8 years and older) for whom both pre- and post-treatment scores were available and for those for whom only pre-treatment PTS-scores were available. Children and young people for whom both pre- and post-treatment scores were available (n = 40) did not differ from those for who no end scores were available (n = 5).
Objective 2A: Mean Changes in PTS-Symptom Severity (n = 40)
Since the summed PTS-scores at T0 and T1 were skewed, we carried out a related samples Wilcoxon signed ranks test and calculated the effect size r, and compared these to the paired samples t-test and its effect size Cohen’s d. The Wilcoxon test and the t-test and its corresponding effect sizes yielded similar results.
Mean PTS-scores decreased significantly from pre-treatment (M = 25.0, SD = 6.9) to post-treatment (M = 9.1, SD = 7.6, t(39) = 11.96, p < .001). Cohen’s d effect size was 2.18 and exceeded Cohen’s (1988) convention for a large effect (d = 0.80). The common language effect size indicates that after controlling for individual differences, the likelihood that a child scored lower at post-treatment than before treatment was 97%.
Objective 2B: Individual Changes in PTS-Symptom Severity
RCIs showed that, of all 40 children and young people with pre- and post-treatment scores available, 30 (75%) improved, 10 (25%) remained unchanged, and zero worsened. Tables 1 to 3 provide an overview of the frequencies of the descriptive statistics per category.
Several differences were observed when comparing the “improved” and “unchanged” category. The improved category included less girls/young women (57% vs. 70%) with a higher mean age (15.4 vs. 11.8 years), whose biological parents were less often separated (69% vs. 78%), whose deceased parent was less likely to be separated from the perpetrator parent (17% vs. 63%), whose perpetrator parent was less likely to be their biological parent (rather than stepparent) (46% vs. 67%), and who were more likely to be a witness to the homicide (50% vs. 30%). A knife was more likely to be the murder weapon (61% vs. 50%) and a verdict was less likely to be reached before the start of therapy (30% vs. 40%) and more likely to be reached during therapy (52% vs. 40%). The mean time between the homicide and the verdict being reached and the median time between the homicide and the date of referral was shorter (39 vs. 50 weeks and 15vs. 35 weeks, respectively). Furthermore, “improved” participants were more likely to score above the cut-off for a clinically relevant PTS-score (97% vs. 70%) at the start of treatment, had a shorter therapy duration (13vs. 25 hr), were less likely to live with a caregiver following the homicide who was also referred for treatment (30% vs. 50%), and were more likely to have their caregiver score above the cut-off for a clinically relevant PTS-score (86% vs. 100%) before their start of therapy.
Discussion
The current study used routine outcome monitoring data of 60 children and young people (aged 8–24 years) following PIPH, who received TGF-CBT from a specialized mental health care organization in the UK. Following Alisic et al.’s (2015) recommendation to focus on more than exclusively psychological symptoms, we sought to provide a detailed description of their experiences covering multiple domains of their lives. To do this, we used the data of the total sample. Furthermore, we evaluated the potential effectiveness of TGF-CBT using data from a subgroup of 40 children and young people with available pre- and post-treatment PTS-scores.
Generally speaking, the majority was classified as “white British,” had lost their mother, and was a witness to the homicide. A stabbing weapon was most often used and a small but significant minority got severely injured themselves during the attack. For almost half of the cases, a verdict was spoken during the course of therapy. Documentation on several characteristics, such as the changed living situation and contact with the offender parent, was incomplete. Mean PTS-scores decreased significantly from pre- to post-treatment with a large effect size (d = 2.18); 75% of the children and young people improved to a clinically significant degree, 25% remained unchanged, and none worsened. The effect size of this study compares favorably to effect sizes in earlier studies (Morina et al., 2016) and is in line with the effect size of Cohen’s d = 1.94 found in prior work on adults who received TGF-CBT following the loss of a loved one to homicide (Soydas et al., 2020). Our results promisingly demonstrate that children and young people are likely to benefit considerably from CBT including both trauma- and grief components following PIPH.
With some caution, we can conclude that for all children and young people included in this study, the homicide had a major impact on multiple aspects of their lives and their development, impacting their basic needs of security and predictability (Alvis et al., 2022). Over 85% of all the children and young people in our sample passed the threshold for clinically relevant PTS at the start of treatment. In almost half of the cases in our sample, it was documented that domestic violence had taken place prior to the homicide. In those cases where details were available, the violence (sometimes including sexual abuse) was also directed toward the children/young people. Existing literature suggests that IPV and child maltreatment co-occur at a rate of roughly 80% (e.g., Coulter & Mercado-Crespo, 2015). The suspected high occurrence of violence toward the children and young people in our sample prior to the homicide may account in part for the high baseline PTS-symptom severity. This may implicate that some children and young people were traumatized prior to the homicide, making them more vulnerable for developing problems even before the homicide. Subsequently, they may have been less able to cope with the consequences of the homicide, putting them at risk for developing problems in various domains of their lives (Alisic, Groot, Snetselaar, Stroeken, & van de Putte, 2017). Due to the traumatic nature of the loss and situation prior to the homicide, trauma and grief symptoms are presumably inextricably linked (Mannarino & Cohen, 2011). The loss of both parents at once, in addition to the potential subsequent loss of social surroundings, existing social support system and for some, loss of siblings, likely had a major effect on their grief process. This may have fueled symptoms such as longing for the deceased, intense emotional pain such as sadness and anger, feelings like one has lost a part of one’s self, and difficulty in engaging with social or other activities (Alvis et al., 2022). This further supports that including both trauma and grief focused components in psychological interventions following PIPH may be beneficial.
Notably, despite the current dataset being slightly more ethnic diverse compared to the general population in England and Wales (Office For National Statistics, 2020), our sample still mainly comprised people from the group that was classified as “white British.” However, people from marginalized communities such as ethnic minorities are known to be overrepresented among homicide survivor populations (Sharpe, 2015). For example, the likelihood that Black youth in the United States will lose a relative or someone other close to them to homicide is 7.8 times that of White youth (Finkelhor et al., 2005). Furthermore, individuals belonging to ethnic minority groups may receive less material, social, and emotional support than members of ethnic majority groups following trauma and loss (Smid, Drogendijk et al., 2018) and are therefore at greater risk for compromised mental health (Sharpe, 2015), such as persistently high PGD and/or PTSD symptom severity (Glickman, 2021; Smid, Groen et al., 2018). However, this overrepresentation was not reflected in our dataset.
Despite some of the aforementioned similarities, the experiences of the children and young people following PIPH in our sample varied widely. The situation prior to the homicide, such as separation from the biological parents and siblings, domestic violence or sexual abuse, and a history of mental health problems of the victim or perpetrator may gravely affect the child or young person’s coping following the homicide, as well as their response to treatment. Likewise, circumstances of the homicide, such as having witnessed the homicide, being injured themselves or losing multiple loved ones during the attack, may exert an influence. Finally, factors in the aftermath of the homicide, such as the loss of one’s familiar environment and attachment figures due to forced relocation, ongoing police investigations or trial procedures, but also support obtained from new caregivers, potentially strengthened developmental assets and increased emotional and physical safety, might influence the emotional consequences and response to treatment. Such risk and protective factors are important to include in future research and interventions offered.
Observations From the RCI Categories
When considering the categories resulting from the RCIs, some differences were observed between the “changed” and “unchanged” group. The largest differences were observed for age (younger ages in the “unimproved” group), gender (more girls in the “unimproved” group), whether the perpetrator and deceased were separated (this was more likely in the “unimproved” group), whether the child or young person was a witness to the homicide (this was less likely for the “unimproved” group), baseline symptom severity (this was lower for the “unimproved” group) and response to treatment of the caregiver (this was lower for the “unimproved” group). However, we did not test whether these differences were statistically meaningful as we did not have sufficient information on all these variables and a large enough sample to do so. Although it would be interesting for future research to systematically collect information on these variables and to test whether they influence treatment outcome, one important observation was that the improved group was rather heterogenous in terms of gender (slightly more females), age (ranging from 8.0 to 24.0 years with a mean of 15.4 years), type of homicide (a knife was used in 61% of cases), being a witness (50%), the perpetrator being the biological parent (in 46% of cases) and timing of the verdict (52% of verdicts were spoken during therapy). This suggests that these individual characteristics and experiences may not have large impacts on therapy outcome.
Finally, it is important to note that six children and/or young people scored below cut-off score for clinically relevant PTS at the start of treatment. Recent latent class analyses in violently and homicidally bereaved adults showed that a class with no disturbance often emerges (Lenferink et al., 2019; Murphy et al., 2016). Although these six children and/or young people did display some PTS-symptoms (four scored in the “subclinical” range), and it is unclear whether they would also score low on measures assessing, for example, symptoms of PGD or depression, it would be of interest to include a broader range of symptom measures in future research to explore whether groups similar to those emerging in LCAs can be identified.
Limitations and Strengths
Several limitations should be taken into account. First, the absence of a control group prevents us from drawing any conclusions on the effects of the intervention in comparison to the passing of time, regression to the mean or other factors, on PTS-symptoms. Second, the sample comprised a treatment-seeking population and the degree to which the descriptive findings generalize to non-assessed groups not seeking treatment is unclear. As a result of the limited ethnic diversity in our dataset, we cannot infer whether our findings are generalizable across different cultures. Further, the inter-item correlation of the CRIES-8 fell below the optimal range whereas in other studies, internal consistency was acceptable to good (e.g., Verlinden et al., 2014). This may indicate that the internal consistency of the CRIES-8 in the current study was low. Alternatively, our finding that the inter-item correlation fell in the optimal range for both of the subscales may indicate that PIPH bereaved children and young people may present with incongruous intrusion and avoidance symptoms, possibly because the judicial proceedings and interest in the media prevent them from avoidance. Additionally, due to many missing values, we could not include predictors in our statistical analyses. Therefore, the impact of the experiences and characteristics of the sample on the reduction of PTS-symptoms remains unclear. It is conceivable that some of these factors affected symptoms reduction. For example, prior domestic violence likely exerted great influence on the high PTS-symptom severity found in this study; and the changes in living environment following the homicide may be associated with the decrease in symptom severity. Moreover, the reliance on self-report measures precludes any statements about the presence of a disorder. Finally, we did not measure grief symptoms and cannot make any statement about the presence of symptoms purely related to grief.
Strengths of the current study lie in its relatively large sample size, an almost equal gender distribution, and the use of quantitative data to measure symptomatology, next to the descriptive data. Since most prior studies have relied on smaller sample sizes or single cases, the combined descriptive and quantitative information of the current study contributes to the existing knowledge of this hard to reach and often overlooked target group.
Recommendations for Practice and Research
The consequences for children and young people following PIPH are severe, both in terms of mental health and wellbeing and disruptions in their caregiving, housing, and social environment. It is important for policy makers and those offering interventions to be aware of this, and to keep in mind the many different and complex factors that may contribute to this disruption. Information on the experiences and broader wellbeing of these children regarding physical, social, and academic domains of their development (Alisic et al., 2015) should be systematically collected and monitored over time, so that the impact of such factors both prior to and following the homicide can be better understood and targeted in interventions. Since none of the children and young people in our study worsened following treatment, clinicians should not be hesitant regarding the use of preventive or curative interventions.
PTS-symptoms and grief symptoms are likely to be intertwined in children and young people following PIPH. Prior research has shown that in patients confronted with traumatic loss, separation distress (yearning for the deceased, preoccupation with the death) may even overshadow traumatic distress (including intrusive symptoms and alterations in arousal and reactivity) (Boelen et al., 2020). Our study demonstrated that psychological interventions can effectively reduce PTS-symptoms in children and young people following PIPH. However, since the treatment that the children and young people in our study received included both trauma and grief focused components, it would be of great interest to also investigate their grief response, by measuring grief related symptoms such as PGD. Additionally, it would be valuable to evaluate the effect of TGF-CBT on such grief related symptoms following PIPH. Notably, recent evidence shows that PGD can be successfully reduced in bereaved children and adolescents, using cognitive behavioral therapy (Boelen et al., 2021). In the case of TGF-CBT, it would be of interest to unravel which specific components of the therapy are associated with, for example, change in PTS- and grief related symptoms. Furthermore, in addition to PGD, we would recommend including measures tapping into several additional disorders such as depression and generalized anxiety (Soydas et al., 2021).
It is important for all actors involved in the aftermath of a homicide, to be aware that ethnicity and culture influence the ways children and young people confronted with PIPH define their experiences and, especially in the case of marginalized groups, how they consequently seek out social or mental health services (Agoff et al., 2007; Bauer et al., 2000). Marginalized groups often experience high barriers in finding their way to (mental) health services. Future studies focusing specifically on marginalized groups are a major priority, and it would be interesting to examine whether the findings of the current study will be replicated in a more ethnically diverse sample.
Moreover, future studies could use systematically collected data to quantify the preliminary findings of the current study, investigate whether subgroups of children and young people can be distinguished who follow a similar course of complaints, and to broaden such research to children and young people bereaved by PIPH who did not undergo treatment. Studies including a non-treatment control condition are needed to enhance knowledge about which interventions yield the strongest symptom reductions. It would be useful for this research to consider the impact of potential risk and protective factors, including the ones mentioned above, on the impact of such interventions. Finally, qualitative studies such as those using participatory methods are needed, to include the perspectives of the children and young people and other actors involved.
Despite the aforementioned limitations, the current study suggests that children and young people faced with PIPH may benefit from treatment, and the working mechanisms of such interventions merit more research attention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.