
Abstract
The publicly funded early intervention program for preschoolers with autism spectrum disorder (ASD) in Nova Scotia, Canada, uses the pivotal response treatment (PRT) model. Parents are coached in use of PRT strategies during their children’s first week of treatment. We explored whether parents of older preschoolers with limited verbal ability learned to implement PRT strategies with fidelity after brief coaching and whether PRT strategy use was associated with gains in children’s communication skills. We coded precoaching and postcoaching parent–child play episodes of 39 children (4.4–5.5 years) with limited verbal skills for parents’ PRT fidelity and children’s correct responding to language opportunities and frequency of initiations. Parents’ use of PRT strategies significantly improved, as did children’s responsiveness to parent-provided language opportunities. This study provides evidence for the utility of brief parent coaching in PRT for older preschoolers with ASD whose verbal skills are limited.
Given that children diagnosed with autism spectrum disorder (ASD) vary considerably in their cognitive and language abilities, it is important to understand which interventions, in which contexts, provide optimal results for children with varying profiles of baseline abilities (Vivanti et al., 2018). One group that is receiving increasing attention in autism research is children with minimal verbal abilities—those who use few functional words, “significantly fewer than expected levels relative to age” (Koegel et al., 2020a). Approximately 25% to 30% of school-age children with ASD are nonverbal or minimally verbal (Tager-Flusberg & Kasari, 2013), and agreement is lacking regarding the most effective treatment for these children (for review, see Brignell et al., 2018).
Evidence-based interventions for ASD include naturalistic developmental behavioral interventions (NDBIs) in which the primary target is often communication. These interventions rely on engaging the child in naturally occurring activities in which they show interest and rewarding their communication and social behavior. The child’s everyday routines are used to incorporate increasingly complex learning experiences so that behavior generalizes to new contexts. Systematic reviews and meta-analyses have highlighted the promise of NDBIs and the rigor of studies that underscore the efficacy of these interventions (Sandbank et al., 2020; Simpson, 2005).
One NDBI widely used with children with ASD is pivotal response treatment (PRT; Koegel & Koegel, 2006). The PRT model targets pivotal aspects of learning, such as motivation and initiations, and collateral gains occur in domains such as communication. The model focuses on increasing the child’s overall motivation to develop their communication and social skills by ensuring that the adult is following the child’s choice in activities, using natural reinforcers, and reinforcing the child’s “good enough” attempts to engage in the appropriate behavior. Results of randomized controlled studies comparing PRT with general psychoeducation (Hardan et al., 2015), a delayed-treatment group (Gengoux et al., 2019), or discrete-trial behavioral therapy (Mohammadzaheri et al., 2014) favor PRT, evidencing increased functional utterances from preintervention to postintervention.
Research underscores the importance of involving parents in the delivery of ASD interventions (Prata et al., 2018). Teaching parents skills that are used in clinician-led interventions facilitates application of skills from the clinician to the parent, and in parallel, from the center to the home (Bearss et al., 2015; Bryson et al., 2007). Parents’ involvement in intervention for their children with ASD positively influences parent–child interactions and children’s understanding of language (Oono et al., 2013). Many studies have shown that parents learn to implement PRT adequately (Duifhuis et al., 2017; Gengoux, 2019; Hardan, 2015; Minjarez et al., 2011), and that their ability to implement PRT strategies has positive effects on their children’s communication gains (Minjarez et al., 2011).
In the Canadian province of Nova Scotia (NS), the publicly funded early intervention program for children with ASD under the age of 6 years provides up to 1 year of clinician-delivered PRT (Bryson et al., 2007). Critically, clinicians coach parents to implement PRT in their child’s first week of the program, learning to provide language opportunities and use natural reinforcement for verbal utterances, thereby targeting communication skills. One goal is that parents will provide developmentally appropriate language opportunities, typically one or two clear words that the child can repeat in context. A related goal is for parents to reduce the number of developmentally inappropriate questions posed to their children, for example, multiword questions to which their children cannot yet respond. Parents are coached to use PRT strategies at home, during (and beyond) the 1-year clinician-delivered program, which is most often implemented in a typical preschool or daycare setting (see Smith et al., 2015, for a description of the program).
In most studies exploring the impact of parent coaching in PRT, parents are coached over weeks, ranging from 8 to 25 hours of direct parent coaching in an individual or group format (Verschuur et al., 2014). Coolican et al. (2010) used a single-case experimental design to explore the impact of brief coaching for parents of children who were waiting to start the NS PRT-based program. Children were between 2 and 5 years of age and their baseline language levels varied from one-word approximations to short phrases. With just 6 hours of coaching, all eight parents improved from precoaching to postcoaching in their ability to implement PRT strategies accurately, with five parents reaching a criterion level of fidelity (i.e., 75% accuracy). Furthermore, all children’s use of functional verbal utterances increased significantly. Coolican and colleagues’ study provides empirical evidence for the effectiveness of brief parent coaching in PRT. Similar findings have been reported regarding the positive impact on parents’ learning of naturalistic strategies following brief parent coaching (Lane et al., 2016). Our goal was to extend these findings using a larger sample of older preschoolers with limited verbal abilities, for whom the benefits of verbal interventions are inadequately understood (Koegel et al., 2020b).
Characterization of children’s verbal ability is inconsistent in the literature. Descriptions of children’s communication skills vary, ranging from ability to imitate syllables to phrase speech. In addition, diverse language assessment measures have been used. These variables complicate comparability between studies and the identification of appropriate treatment options (Koegel et al., 2020a). The term “limited verbal ability” has been a helpful addition to the literature. Children who have limited verbal abilities have significant delays compared to their peers of the same age; this category may include older preschoolers using single words or short-word combinations (see Koegel et al. (2020a) for differentiation between minimally verbal and limited verbal categorizations).
Most intervention studies for minimally verbal children with ASD have explored the impact of augmentative and alternative communication interventions, which include aided systems such as picture books, symbols, or speech-generating devices (Brignell et al., 2018; Koegel et al., 2020a). To our knowledge, only one study has investigated the impact of a PRT program specifically for minimally verbal children. Schreibman and Stahmer (2014) conducted a randomized controlled trial comparing intensive parent- and clinician-delivered PRT with a commonly used augmentative and alternative approach, the picture exchange communication system (Bondy & Frost, 1994), in which children are taught to use pictures to communicate. In their study, minimally verbal 2- to 4-year-olds (defined as those with nine or fewer intelligible words) made similar gains in expressive and receptive language after 23 weeks of intensive intervention using either PRT or the Picture Exchange Communication System. This study provides evidence that intensive parent- and clinician-delivered PRT may be effective for minimally verbal children with ASD; however, the authors did not explore the specific impact of the parent coaching intervention component.
In a systematic review, Koegel et al. (2020b) found that few studies that have explored verbal communication interventions for minimally verbal children with ASD have looked at the impact of parent education or coaching components. Moreover, details have been lacking regarding fidelity of parents’ implementation of these interventions. To our knowledge, no study has investigated the impact of brief parent coaching in PRT on the communication gains of preschoolers with ASD whose verbal abilities are very limited. Shire et al. (2018) examined the ability of parents of older (school-age) minimally verbal children with ASD to implement an adapted NDBI and the associated gains in their children’s communication. Children of parents whose postintervention implementation fidelity was at least 70% (achieved by 11 of 22 parents) showed significant increases in spontaneous commenting (either spoken or using an augmentative device) during intervention, whereas no significant gains were found for children whose parents did not meet the fidelity criterion. Parents in that study were coached in an intervention combining two NDBIs: Joint Attention Symbolic Play Engagement and Regulation (Kasari et al., 2010) and enhanced milieu teaching (Hemmeter & Kaiser, 1994), with half of the parents additionally trained in the use of a speech-generating device. The combined intervention shares some features with PRT, such as modeling and prompting to promote communication, but differences include the Kasari et al. (2010) study’s explicit focus on increasing joint attention behavior and imitating children’s language and functional play actions. Furthermore, parents’ receipt of 8 hours of active parent coaching took place over 3 months in conjunction with weekly workshops and passive coaching (clinician delivers intervention while verbally highlighting information to the parent), and this coaching component was not examined in isolation (Shire et al., 2015). Despite this distributed coaching and enhanced opportunities for practice, only half of these parents of older children reached 70% fidelity in intervention implementation. Further research is necessary to better understand the effectiveness of parent coaching with parents of preschoolers whose verbal abilities are limited.
Our aim in this study was to investigate the effects of brief parent coaching in PRT on the communication skills of older preschoolers with ASD with limited verbal abilities—those with significant expressive delays for their chronological age. Our research questions were as follows:
Method
Participants
This study was carried out within the context of a larger project designed to examine children’s preintervention behavioral characteristics and their association with outcomes in the Nova Scotia program, approved by the IWK Health Research Ethics Board (#1020646). The project was developed collaboratively with intervention program leaders, notably author D.C., and families were provided information about the contributions of the research team to the on-going development of the early intervention program. To be eligible for the government-funded service, children must be younger than 6 years of age and have a confirmed or provisional diagnosis of ASD from a specialist psychologist or developmental pediatrician (see Smith et al., 2019).
As part of the intervention program, clinicians routinely gather videos of parent–child play episodes before and after initial parent coaching. Videos from families that had provided written research consent (n = 284) were screened by author T.H. for study eligibility. Videos fulfilled these inclusion criteria: (a) video-recorded episodes available precoaching and postcoaching, (b) parent–child play episodes no less than 10 minutes at each time point, (c) same caregiver in parent–child play episodes at each time point, and (d) child’s maximum utterance in pre-parent-coaching video no more than a two-word combination (with routinized units such as “I want” and “thank you” considered one-word utterances; see Biller & Johnson, 2019). Given our study’s focus on older preschoolers with limited language, we excluded children with phrase speech or greater verbal abilities. (Our sample included some children who would meet minimally verbal criteria; see Koegel et al., 2020a for differentiation between minimally verbal and limited verbal categorizations). Videos were also excluded if nonverbal communication methods (i.e., picture exchange communication system or gestural communication) were used in the precoaching recording. Furthermore, we excluded recordings for which poor video or audio quality precluded accurate behavioral coding such that parents’ use of PRT strategies or child communication within the parent–child interaction could not be adequately assessed. The target sample size was 40, based on an alpha level of .05, power of .80, and a medium effect size (d = 0.46 for child initiations; cf. Hardan et al., 2015).
Of 284 videos screened, 142 were of children with stronger verbal abilities, 66 were missing one time point, 24 were less than 10 minutes, one did not include the same caregiver precoaching and postcoaching, and one included a staff member. Three videos were excluded because of poor audio quality, seven for use of nonverbal communication methods, and one for parent coaching not completed. Videos of 39 children (sex assigned at birth: 34 male, 5 female) and their caregivers (hereafter, “parents”; 27 mothers, 10 fathers, one grandfather, and one aunt) met eligibility criteria. Children were between 4.4 and 5.5 years of age (M = 4.8, SD = 0.19) and were nonverbal (38%), used single words (21%) or used no more than two-word combinations (41%).
Parents who consented to full participation in research (consent A, which included direct contact with the research team and completion of research measures not discussed here) were provided with a demographics form that gathered information regarding race/ethnicity and socioeconomic status. Parents who consented to partial research participation (consent B, limited to anonymous sharing of information gathered by the clinical service) shared videos of parent–child play episodes but did not complete other research measures. Only three families from our study’s sample provided full research consent (consent A); therefore, demographic information is not reported here. However, during the study period 89% of families who were offered the early intervention program participated and 94% of those enrolled consented to research participation, so we expect our subsample is similar as that described by Smith et al. (2019).
Intervention
The program’s primary target areas included communication and social/play skills. Treatment goals for some children included self-care skills (e.g., toileting) and reducing challenging behavior. Owing to a waitlist structure that required offering treatment to the oldest preschoolers first, all children in this cohort began intervention at age 4 or 5. The program was designed to be 12 months, but 10 children in our sample transitioned to school earlier (minimum participation was 6 months). At the beginning of the program, clinicians coached parents in PRT for 2 hours per day for 4 consecutive days. On Day 1, clinicians recorded precoaching videos while parents were asked to play/interact with their child as they typically would while trying to elicit communication. Clinicians then provided parents with didactic information, including a handout, on the pivotal area of motivation and strategies involved in PRT. Importantly, clinicians tailored strategies to each child’s developmental level (e.g., model prompts were encouraged for children with little speech). In vivo feedback regarding parents’ PRT use started on Day 1 and continued throughout parent coaching. The early intervention program has developed a structured training model for parent coaching. Before coaching independently, all coaches must have been coaching with fidelity (>80% for all criteria) across two families (see Appendix).
Clinicians taught parents the Antecedent-Behavior-Consequence (ABC) model of behavior and encouraged parents to use this framework to create language opportunities for their children. Pivotal response treatment motivational strategies were emphasized within this model: clinicians taught parents the antecedent strategies to follow the child’s lead, obtain shared control of a reinforcer, obtain the child’s attention then provide a clear language opportunity; and consequence strategies to provide immediate, natural reinforcement of the target behavior. Clinicians gave parents the rationales for strategies and specific positive feedback regarding their use of these strategies. Corrective feedback/prompting focused on one strategy until the skill was demonstrated starting with following child lead and moving through to the last skill of immediate reinforcement. A strength-based, least-to-most prompting approach was used to enhance parental self-efficacy and encourage new learning and independent problem-solving. At the end of Day 4, a postcoaching video was recorded. After this coaching period, children continued in the 1-year intervention program, which included therapist-provided PRT and positive behavior support (Carr et al., 2002). Some children with sustained low responsivity to PRT were supported to transition to the Picture Exchange Communication System (Bondy & Frost, 1994). Parents received follow-up coaching throughout the program and were encouraged to use learned strategies across daily routines (see Bryson et al. (2007) and Smith et al. (2015) for other program details).
Outcome Measures
Fidelity of PRT Implementation
We coded video-recordings of pre–post parent–child play episodes for PRT strategies based on a protocol adapted from Koegel and Koegel (2006; available upon request). We used 2-minute interval coding (i.e., five 2-minute intervals per 10-minute video). First, we coded parents’ ability to provide at least two developmentally appropriate language opportunities per interval. Language opportunities that met criteria as developmentally appropriate included brief model prompts (e.g., holding up a block and saying “block,” cueing the child to repeat), choice questions (e.g., “red or blue block?”), time delays (e.g., holding the block in anticipation of the child saying “block”), or leading prompts (e.g., “ready, set, . . .”). Critically, the parent had to have shared control of the object and/or activity for the language opportunity to be scored as acceptable. Shared control requires that the parent pause the activity, either by holding back/impeding the child’s access to an object (e.g., holding a block out of reach), or pausing a physical activity (e.g., waiting to provide tickles). Second, we assessed whether parents attained the child’s attention prior to providing language opportunities (child needed to be attending to the object and/or activity when most language opportunities in the interval were presented). Third, we observed whether parents provided reinforcement contingent on the child’s appropriate verbal response following most language opportunities in an interval. To meet criteria, parents had to either provide natural reinforcers following the child’s correct/good attempts or withhold natural reinforcers for inadequate responses. Last, we coded parents’ ability to follow the child’s lead (i.e., allowing the child to choose toys/activities in which they were interested and using these as the basis for language opportunities). Parents who provided at least two developmentally appropriate language opportunities with shared control, appropriate attention, contingency, and who followed their children’s lead in four of the five 2-minute intervals (i.e., 80%) met fidelity criteria for PRT implementation. These criteria are used in training clinical teams in this program and have been previously used in measuring parents’ implementation fidelity in PRT (Gengoux et al., 2019; Hardan et al., 2015) and other NDBIs (Abouzeid et al., 2020). Precoaching and postcoaching overall fidelity composite scores were created by averaging scores for PRT strategies: attention, lead, contingency, and two language opportunities per interval.
Frequency of Language Opportunities
We counted the number of developmentally appropriate language opportunities provided by parents throughout each 10-minute video.
Questions Posed
We recorded counts of developmentally inappropriate questions parents posed to their children within precoaching and postcoaching parent–child play episodes. For children at this early language level, only simple choice questions (e.g., “ball or cup?”) were counted as appropriate; all others were considered too complex (e.g., what would you like to play?).
Initiations
We counted children’s spontaneous utterances (including word attempts and vocal exclamations of excitement or protest). Initiations needed to be socially directed (to the parent), which may have included shifts in gaze toward the parent, direct eye contact, or coordinated vocalizations (see Maljaars et al., 2011, for a similar conceptualization).
Correct Responding
We calculated percentages of children’s correct responding to parent-provided language opportunities.
Statistical Analyses
We conducted statistical analyses using R software (R Core Team, 2013). We examined change in aspects of parents’ fidelity of PRT implementation from precoaching to postcoaching using paired-samples t-tests. To examine the effects of parents’ use of PRT strategies on their children’s communication gains during training, we first conducted paired-samples t-tests to examine whether children’s frequencies of initiations and percentages of correct responding increased from precoaching to postcoaching. Then, Pearson correlations were conducted to examine whether these proximal child outcomes were associated with parents’ PRT implementation quality (change in fidelity scores during coaching) and frequency (increased frequency of parent-provided language opportunities).
Interobserver Reliability
We calculated interobserver reliability for all play-episode-based coding. Author T.H. coded all pre- and post-parent-coaching videos. Two other coders, one of whom was blind to whether videos were precoaching or postcoaching, together coded 20% of the videos (n = 16). The videos for double coding were stratified by child language level (no words, single words, two-word phrases) then selected by using an online random number generator (Randomizer.org). We used the AC1-statistic (Gwet, 2002) to calculate reliability for interval coding (i.e., attention, contingency, following lead, and two language opportunities per interval), given its relative stability irrespective of prevalence of ratings, compared to Cohen’s kappa (Wongpakaran et al., 2013). Intraclass correlation coefficients using two-way random-effects models (Koo & Li, 2016) were used to examine reliability of other constructs (frequency of developmentally appropriate language opportunities and questions posed, child initiations, and correct responding). Interobserver reliability was calculated for each reliability coder separately.
Intraclass correlations between the primary coder and coders 1 and 2, respectively, were: .85 and .98 for initiations; .97 and .98 for question count; .92 and .99 for language opportunity count; and .83 and 1.00 for percentage correct responding, indicating good to excellent reliability (Koo & Li, 2016). Overall, interval coding reliability ranged from moderate to excellent. AC1-statistics for the primary coder and coders 1 and 2 were .62 and .85 for attention; .73 and 1.00 for contingency, and .78 and .91 for language opportunities, respectively. The AC1-statistic could not be computed for “lead” for either reliability coder as codes were the same in every interval (i.e., no variability in coding). However, percentage agreements for each coder with the primary coder (author T.H.) were high (93% and 100%).
Results
On average, four and a half days elapsed between the precoaching and postcoaching videos (SD = 2.38, Mdn = 3) with a range of 2 to 13 days due to family circumstances affecting service delivery. The number of days between precoaching and postcoaching was not significantly associated with parents’ PRT fidelity after training (r = −.12, p = .41).
Details regarding parents’ fidelity of PRT implementation are in Table 1. Parents’ mean overall fidelity scores significantly increased from 33% to 73% during training. Parents showed significant increases with large effect sizes in their ability to provide a minimum of two language opportunities per interval with appropriate attention and contingency, from precoaching to postcoaching. Parents were successfully following their children’s lead in activities before coaching and continued using this skill at postcoaching. Before training began, parents were providing their children, on average, with four language opportunities in a 10-minute span. This significantly increased after coaching, such that parents gave an average of 16 language opportunities. Furthermore, parents significantly reduced the number of inappropriate questions they posed their children during training, from a mean of 38 to a mean of 16. When each PRT strategy was explored in isolation, 44% (n = 17) parents met fidelity for attention, 46% (n = 18) for contingency, 67% (n = 26) for two language opportunities, and 90% (n = 35) for following lead. Overall, 31% (n = 12) of parents met the PRT implementation fidelity criterion for all four PRT strategies after coaching (minimum of 80% for attention, lead, contingency, and language opportunities).
Descriptive Statistics and Paired-Samples t Test Results for Fidelity of Parent Implementation of PRT Strategies (% of Intervals), Overall Composite Scores, and Questions Posed Precoaching and Postcoaching.
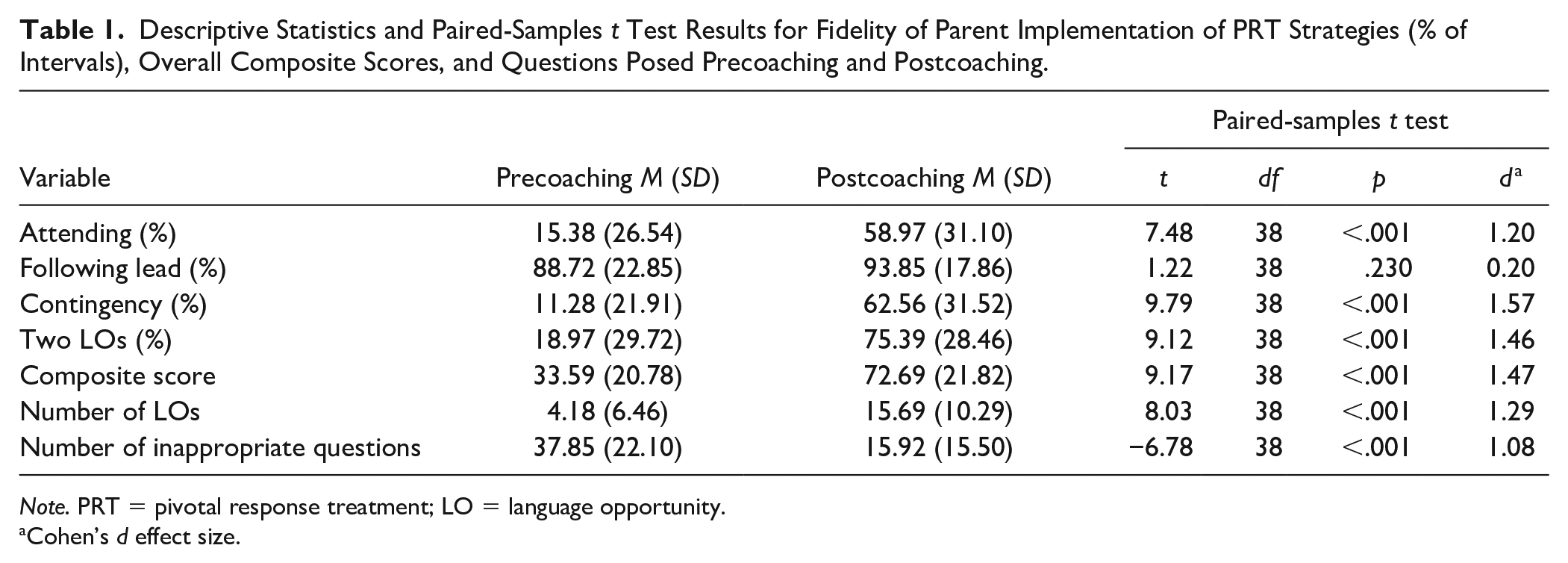
Note. PRT = pivotal response treatment; LO = language opportunity.
Cohen’s d effect size.
Children correctly responded to language opportunities that their parents provided at a higher rate at end of training (see Table 2), and this was significantly associated with parents’ fidelity score increases (see Table 3). No significant improvements were observed for children’s frequency of initiations (see Table 2); however, increased frequency of parents’ language opportunities from precoaching to postcoaching as well as fidelity score increases were significantly associated with increases in children’s initiations during coaching (see Table 3).
Means, Standard Deviations, and Paired-Samples t Test Results for Child Outcomes.
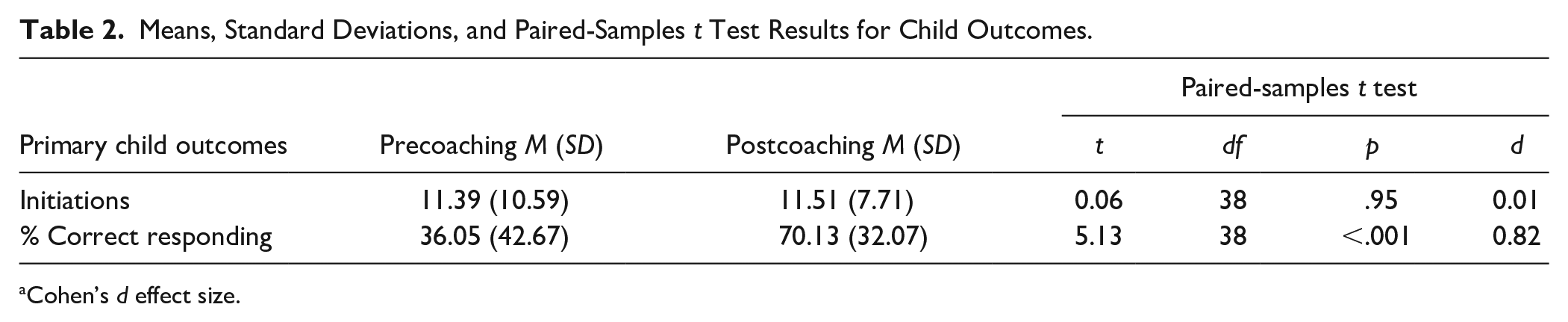
Cohen’s d effect size.
Pearson Correlations Between Parent Variables and Changes in Children’s Communication Outcomes.
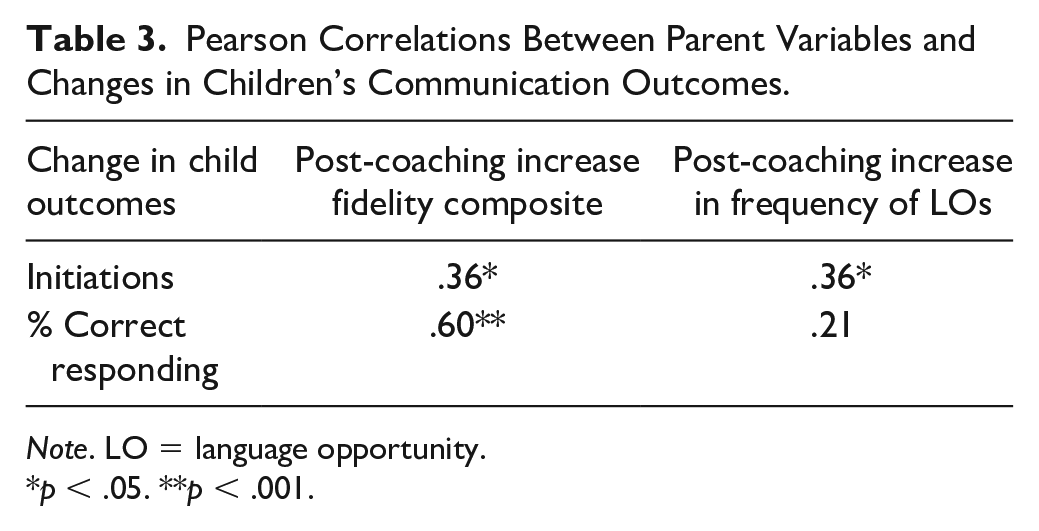
Note. LO = language opportunity.
p < .05. **p < .001.
Discussion
In this study, we aimed to evaluate the impact of brief parent coaching in PRT for children with limited verbal abilities. Fifty-nine percent of our sample of 4- to 5½-year olds used no or only single words and others used no more than two-word combinations prior to intervention.
Our results corroborate previous findings of parents’ ability to learn and use PRT strategies with fidelity (Gengoux et al., 2019; Hardan et al., 2015; Minjarez et al., 2011) and provides further evidence that even brief parent coaching in PRT leads to meaningful gains (Coolican et al., 2010). With 8 hours of coaching, parents improved their ability to provide their children with language opportunities with appropriate attention and contingency. Parents in this sample were appropriately following their children’s leads before the training week. This is likely because parents of children with ASD in Nova Scotia are routinely taught this skill by speech-language pathologists prior to entering the PRT program. A key finding was that parents significantly increased the number of developmentally appropriate language opportunities they provided to enhance their children’s communication (from 4 to 16 per episode, on average). We saw a parallel decrease in developmentally inappropriate questions (i.e., questions to which these children could not be expected to respond; from 38 to 16 per episode, on average).
Approximately one-third of parents (n = 12) met PRT implementation fidelity after training. After only four coaching sessions, these parents attained a similar level of skill to that required of beginner early interventionists. A smaller proportion of parents met full criteria for fidelity than in the study by Coolican et al. (2010) [five of eight]. However, we used a higher fidelity criterion (80% vs 75%) and included only older children with limited verbal abilities, who may be more challenging to teach. For example, it may be more challenging to be contingent on vocalizations/verbalizations in children who vocalize less frequently, and the children therefore have fewer occasions from which to learn. Our findings are comparable to those of Shire et al. (2018), who found that less than half (10 out of 22) of the parents of minimally verbal school-age children who received 8 hours of active coaching in another NDBI intervention over 3 months met their 75% fidelity criterion. Thus, our findings add to a small body of research that suggests that many parents of children with limited verbal skills can be coached to fidelity in a short period, while others may make meaningful gains without meeting full fidelity criteria.
In our study, children demonstrated significant increases with a large effect size in correctly responding to language opportunities provided by their parents during training. This increase was associated with parents’ improved implementation of PRT strategies. These gains are particularly promising as these children’s spoken language skills were considerably delayed relative to typical developmental expectations. This suggests that parents’ provision of developmentally appropriate language opportunities, followed by natural reinforcement, helped these children to show important short-term gains. If sustained, such changes have the potential to change children’s communication development trajectories.
We did not find significant increases in spontaneous initiations by children during training. This is not surprising considering both these children’s verbal abilities and the short study period. However, the significant association between increases in parents’ language opportunities and fidelity scores with increases in children’s initiations is encouraging. Studies with longer follow-up periods have documented gains in spontaneous communication in children characterized as minimally verbal (e.g., Schreibman & Stahmer, 2014; Shire et al., 2018). Differences between our methods and (Shire, Shih and Kasari, 2018) treatment approach, duration of treatment, or the operationalization of “minimally verbal” for their participants (i.e., fewer than 20 spontaneous words in the 5- to 8-year age range) may have contributed to different findings. The Schreibman and Stahmer (2014) sample consisted of 2- to 4-year olds with delayed speech (no more than nine words) and as such, communication gains may have been more likely for those younger children than our 4- to 5-year olds with substantial expressive language delays.
This study’s limitations include that, given the necessity to screen more than 250 precoaching video-recordings for participants’ eligibility, author T.H. was not blind to pre–post video categorization, which may have influenced coding of parents’ implementation fidelity. In addition, we lack family demographic information including ethnicity, household income, and parent education, which we were able to gather only for a few families who completed other components of the larger study. Parent coaching is a prerequisite to start clinician-delivered intervention for this public program; the high uptake of early intervention participation by families suggests that our subsample represents families enrolled. In addition, parent participation was supported in many ways, primarily by the naturalistic context in which PRT was delivered, but also by providing letters when requested that describe parents’ involvement in coaching for use with their employers. Last, although quantitative data regarding parents’ satisfaction with the program was sought as part of the larger study, none of the parents in our sample completed this questionnaire. Earlier studies of this program support its social validity (D’Entremont et al., 2021).
Our results underscore the importance of parents’ involvement in treatment for all children, including for children with limited verbal abilities. This group often requires high levels of support, and studies are needed to understand the impacts of coaching these parents (Koegel et al., 2020b). Parent coaching programs are empowering and provide the necessary psychoeducation and skills training so that parents can better understand their child’s diagnosis, manage developmental expectations (Karst & Van Hecke, 2012) and importantly, incorporate therapy into their children’s natural environments and routines. Generalization of skills can occur by providing many and varied opportunities for the child to learn (Karst & Van Hecke, 2012; Prata et al., 2018). This study demonstrates that even brief parent coaching programs can have important positive effects.
This study adds to a body of research supporting the importance and effectiveness of parent coaching in NDBI strategies. The Nova Scotia early intervention model for preschoolers with ASD consistently incorporates individualized parent coaching as a first step in a comprehensive intervention program. Our team’s research has highlighted links between the use of this model and higher parent satisfaction (D’Entremont et al., 2021). This study demonstrated impacts of this training component on children’s outcomes, even in older preschoolers whose limited verbal skills create challenges for treatment.
Footnotes
Appendix
Child Name: ___________ Trainee: ______________
Trainer: _______________ Date: ____________
Acknowledgements
The authors thank Dr. Loriann Williams and Brittany Fitzgerald for their help in adapting the coding scheme and in coding videos.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.C. is the Clinical Leader of the NS early intervention program for preschoolers with ASD. Other authors have no potential conflicts of interest to disclose.
Funding
This work was supported by a CIHR Operating Grant (MOP 142293), as well as the CIHR Canadian Graduate Scholarship, Nova Scotia Graduate Scholarship, and the Research Nova Scotia Scholars Award to the first author, and the Joan & Jack Craig Chair in Autism Research to the last author.