
Abstract
This study examines family distress and quality of life among families of children with disabilities during the first wave of the COVID-19 pandemic in Israel. It considers the role of family resources, a sense of community, and the services provided by the Israeli family-centered program (IFCP). One hundred eighty-two parents of children with disabilities participated in this study through an online survey. Structural equation modeling showed that extensive family resources, better operation of the IFCP, and a sense of community were associated with a better quality of life. Lack of family resources was associated with family distress. A regression-based path analysis indicated that this association was moderated by components of the IFCP. Family-centered services were associated with a family’s quality of life and experience of distress in times of national crisis. The results highlight the importance of the partnership between parents of children with disabilities and service providers.
Families of children with disabilities have reported that COVID-19 has affected their mental health, often increasing anxiety and fear. They have reported increases in depression, distress, and stress (Asbury et al., 2021). Similarly, families living with an individual with autism spectrum disorder reported high levels of stress and disruption to their lives during the COVID-19 crisis (Manning et al., 2021). However, the degree of the COVID-19 crisis’ psychological impact on families of children with disabilities remains unclear. This study addresses that lacuna. We explore family distress and quality of life among Israeli families of children with disabilities during the first wave of the COVID-19 pandemic and how these were moderated by family resources, sense of community, and the family-centered services they received. To do so, we first briefly describe the conceptual and empirical background of families of children with disabilities in the context of the COVID-19 pandemic, as well as the association between the study’s variables—family resources, sense of community, and family-centered services—on family quality of life.
Families of Children With Disabilities in the Context of the COVID-19 Pandemic
People with disabilities and their families are particularly vulnerable to the negative consequences of the COVID-19 pandemic (World Health Organization [WHO], 2020). The unforeseen changes in everyday life resulting from the pandemic, along with regulations requiring self-isolation and social distancing, have been especially challenging for children with disabilities and have had an unprecedented impact on their families (Rose et al., 2020; Toseeb et al., 2020). The Israeli government’s response to the COVID-19 outbreak was gradual and included various measures to safeguard public health in general, as well as specific guidelines for safeguarding at-risk populations. The government adopted various control measures, ranging from social distancing and self-quarantine to total lockdown (Araten-Bergman & Shpigelman, 2020). These regulations included closing special education facilities, where children with disabilities normally receive physical, paramedical, educational, and emotional care. The closure of these educational institutions shifted the burden of care to parents and families, initially without providing formal home care assistance as a substitute. Therefore, families of children with disabilities were required to deal not only with household management and distance learning but also with providing intensive care for their children. In this context, family-centered policy and care, which is the recommended approach for planning, developing, and providing services to children with disabilities and their families (Bruder, 2010), are expected to provide the most effective help.
Associations Between the Study Variables
This study examines how a family’s quality of life and experience of distress is affected by family resources, sense of community, and involvement with the Israeli family-centered program (IFCP), which was established by the Government of Israel. A family’s quality of life encompasses the fulfillment of a family’s needs, the enjoyment of family life, and whether or not the family members have the opportunity to engage in activities that are important to them (Park et al., 2003; Vanderkerken et al., 2019).
The Association Between Family Resources and Family Quality of Life or Distress
This association is based on Hobfoll’s Conservation of Resources Theory (Hobfoll, 1989), which emphasizes the role of resources in predicting stress, distress, and well-being in times of crisis. In situations of stress and crisis, the individual’s resources are depleted, and the balance between environmental requirements and the available pool of resources is disturbed. Moreover, the greater the depletion of resources, the more vulnerable a person is to the harmful effects of stress and crisis situations (Hobfoll, 1989).
The Association Between Sense of Community and Family Quality of Life or Distress
The sense of belonging to the community corresponds to a human need for a space beyond the family of belonging, influence, and emotional and spiritual participation (Ben-Yosef, 2010). The concept of belonging is essential to community (McMillan & Chavis, 1986). In its broadest sense, the community can simply be seen as a set of people with some shared element, which can vary widely and might range from living in a particular place, to sharing some kind of interest or belief. In this sense, then, all people belong to multiple communities—our local neighborhoods are our geographic community; while our workplace, and a diverse range of ideological or interest-based groups are our interest or practice communities. In the IFCP, there are support groups based on mutual interest, as well as leadership groups in which family members work together as agents to promote their interests (Joint-Ashalim, 2018; Loeff & Rivkin, 2017). Therefore, the IFCP can be characterized as a community of practice. The people involved develop a shared repertoire of resources: experiences, stories, tools, and ways of addressing recurring problems. The development of these resources emerges through time and sustained interaction (Wenger, 1998).
A sense of community promotes resilience and has frequently been shown to correlate with positive psychological outcomes in the wake of potentially traumatic events (Ben-Tzur et al., 2021). Individuals who express more connections to their communities exhibit lower levels of distress (e.g., Dekel & Tuval-Mashiach, 2012; Gelkopf et al., 2012; Levy & Friedman, 2019). A high sense of belonging to a community is also associated with a high level of well-being in general (Evans, 2007; Peterson et al., 2008).
The Association Between Family-Centered Service and Family Quality of Life or Distress
Families’ quality of life is a macro-outcome of family-centered service and indicates the quality of the service (Balcells-Balcells et al., 2019; Shippers et al., 2015). The literature shows that the support and services provided to children and their families positively affect their quality of life (Abbott et al., 2005; Davis & Gavidia-Payne, 2009; X. Hu et al., 2012; Mellon & Northouse, 2001; Schippers & Van Boheemen, 2009), and documents that the support provided can predict a family’s quality of life (Epley et al., 2011; Meral et al., 2013).
The Israeli Family-Centered Program for Families of Children With Disabilities in Israel
The State of Israel provides services to children with physical, sensory, mental health, and intellectual disabilities. The number of children with disabilities in Israel is estimated at 220,000 (about 8.5%) (Barlev-Kotler et al., 2014). The national family-centered services for families of children with disabilities provided by the Israeli Ministry of Welfare and Social Affairs are administered through the IFCP for families of children with disabilities. The service follows a family-centered and community approach, and it complements the individual services provided for the children with disabilities themselves (Loeff & Rivkin, 2017). The IFCP and the study described in this article rely on the logical model of service established by the service developers (Joint-Ashalim, 2018). The logical model is used by service developers, managers, and evaluators to evaluate the effectiveness of the services they provide. It describes the logical links between the services’ resources, activities, outputs, audiences, and outcomes related to a specific problem or situation. Once a service has been described in terms of the logical model, it can be assessed in terms of its performance (Unrau et al., 2007). According to the logical model of the IFCP, families who actively participate in the IFCP will develop a sense of belonging to a community of families who have children with disabilities. Their parental capacity will thereby be strengthened, and they will therefore promote and access more community services (Loeff & Rivkin, 2017). Therefore, we consider the contribution of the IFCP with regard to four factors: (a) the family’s satisfaction with the services provided by the IFCP, (b) participation, (c) the sense of belonging to the IFCP’s community, and (d) family leadership.
IFCP During the COVID-19 Pandemic
Hindi and Gur (2020) documented the changes in the IFCP’s services and method of providing them during the first wave of the COVID-19 pandemic. At that time, Israel was under a complete lockdown, and the special education system was closed. The study indicated that the focus of the IFCP changed in several ways. First, the IFCP helped children and their families by providing food, art kits, tablets, and specialized equipment. Second, they facilitated communities between families and local authorities. Thus, they addressed the dynamic needs of the families and also communicated information to families from government organizations. Indeed, 57% of the families reported using the IFCP’s information retrieval services. Finally, the IFCP quickly adapted to provide services online. Emotional support was provided by phone, and support groups for parents and siblings, along with lectures for parents, were provided through Zoom.
Study’s Aims
Our goal was to investigate the role of personal and community resources in helping Israeli families of children with disabilities cope with the disruption of their lives, measured in terms of their distress and the family’s quality of life, during the first wave of the COVID-19 pandemic in March–May 2020. We consider the role of the IFCP as representative of community resources. We chose this period to investigate because, on March 25, 2020, the Israeli government restricted the distance people could travel from home, and a full lockdown was imposed between April and May 2020 (Israeli Ministry of Education, 2020).
Assessment of the IFCP included investigating the services they provided, families’ satisfaction with these services, families’ sense of belonging to the IFCP’s community, and family leadership. In addition, we examined how the IFCP moderated the effects of family resources on family distress and quality of life. We expected that family resources, a sense of community, and the IFCP’s operations would have a negative effect on family distress, and a positive effect on families’ quality of life.
Method
Participants
A convenience sample of 182 parents (90% of whom were mothers) of children with disabilities participated in the study. Convenience sampling is a type of nonrandom sampling in which members of the target population who meet certain practical criteria, such as availability at a given time or willingness to participate, are included (Etikan et al., 2016). The majority of participants were married (85.3%), and more than half (60.6%) had a higher education degree. More than half (61.1%) stated that their household income was lower than average, approximately a fifth (18.3%) reported having an average household income, and a fifth (20.6%) indicated that their household income was higher than average. Due to the COVID-19 pandemic, half of the participants (50.7%) had experienced a change in their employment status, as follows: one of the parents was on an unpaid leave of absence (72.6%), both of the parents were on a leave of absence (21%), or one of the parents had lost his/her job (6.5%). With regard to residence, 42.9% of the participants were from rural areas, and 57.1% were from urban areas. The age of the children with disabilities ranged from 1 to 27 years, with a mean age of 11 years (SD = 5.46). The age of the children with disabilities was not correlated with the study’s variables. More than a third of the sample were parents of children with autism spectrum disorders (35.7%), approximately a fifth (17.6%) were parents of children with intellectual disabilities, and the rest were parents of children with sensory, mental, or physical disabilities, or severe learning disabilities. Information about the children’s diagnoses was provided by parents.
Measurements
Family Distress
We used the Brief Family Distress Scale (Weiss & Lunsky, 2011) to measure the level of parental or family distress. The measure was intended to examine the experience of the COVID-19 crisis from the perspective of the family members, by placing the family’s current experiences on a continuum of distress ranging from low levels of distress to crisis. Responding to a single item, family members were asked to select 1 of 10 statements that assessed their (and their family’s) experience of crisis. Each statement corresponded with a point on a continuum, with 1 being “everything is fine; my family and I are not in crisis at all,” and 10 being “we are currently in crisis, and it could not get any worse” (Weiss et al., 2013).
Family Quality of Life
We assessed this variable with an abbreviated version of the Beach Center Family Quality of Life Scale (Beach Center on Disabilities, 2006). Its purpose is to measure families’ satisfaction with the quality of their family life in five areas: family interactions (“My family enjoys spending time together”), parenting (“Adults in my family have time to take care of the individual needs of every child”), emotional well-being (“My family members have some time to pursue our own interests”), physical and material well-being (“My family has a way to take care of our expenses”), and disability-related support (“My family member with a disability has support to accomplish goals at home”). Our participants rated the 10 items on a 5-point Likert-type scale, where 1 = very dissatisfied, 3 = neither satisfied nor dissatisfied, and 5 = very satisfied. Psychometric analysis supports the validity of the scale (Hoffman et al., 2006). We then calculated a composite quality of life score for the family by averaging the responses. High scores indicated a better quality of family life. In the current study, the scale showed adequate internal reliability for the total score (Cronbach’s α = .87).
Family Resources
Family resources were assessed using the Conservation of Resources Evaluation (Hobfoll & Lilly, 1993). The original Conservation of Resources Evaluation (Hobfoll & Lilly, 1993) consists of 74 items. Due to its length, a more common strategy has been to measure a small subset of resources that are most relevant to the study for which it is being used (Halbesleben et al., 2014). Following this strategy, we asked our participants about 14 resources, including having adequate food and clothing, suitable housing, a sense of family pride, a sense of optimism, an adequate income, and access to financial help, if needed. They rated their agreement with these statements on a 5-point Likert-type scale, with a high score indicating more resources. We created composite family resources score by averaging the responses. Cronbach’s α was .79.
A Sense of Community
The Sense of Community Index is the most widely used validated measure of the construct (Long & Perkins, 2003). It is based on McMillan and Chavis’s (1986) contention that a sense of community is a perception with an affective component. For this study, we modified two items from this index in order to assess the feeling of belonging to the local community. Participants responded to the items on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). We then calculated their overall score as the average of the responses. A previous study showed adequate reliability and validity for the complete Sense of Community Index (Obst & White, 2004). In the current study, the sense of community score had a Cronbach’s α of .77.
Family Leadership
As mentioned earlier, the IFCP aims to establish family leadership groups that work to formulate a common agenda for the benefit of all of the families of children with disabilities participating in the IFCP, as well as those living in the community. These groups were in contact online during the lockdown. Participants were asked to rate their satisfaction with the family leadership groups on a 5-point Likert-type scale, which ranged from “not satisfied at all” to “very satisfied.”
Services
To assess the degree to which the families used the services provided to them by the IFCP during the emergency, we developed an index regarding seven services: emotional support by telephone, receiving information, a support group for parents via Zoom, a support group for siblings via Zoom, lectures on Zoom, creative kits for children, and activities for families. Participants were asked to indicate what services they had used, and to what extent each of these services had helped them during the COVID-19 pandemic, on a 5-point Likert-type scale (ranging from 1 = not helpful at all to 5 = very helpful). We then calculated the overall score as the average of the responses. The services contribution scale exhibited good internal reliability (Cronbach’s α = .93).
Participation
We assessed participation in IFCPs by using the 4-item Sense of Sharing Index (Friedman, 2006), which we adapted to reflect participation in the IFCP for families of children with disabilities. Participants were asked to indicate their agreement with statements such as, “I have an impact on things that happen in the IFCP to which I belong,” and “I have an important role when discussing issues relating to the IFCP’s operation.” Responses were rated on a 5-point Likert-type scale, where 1 = strongly disagree, 3 = moderately agree, and 5 = strongly agree. We calculated overall participation as the mean score. A previous study reported an excellent internal consistency of α = .91 (Friedman, 2006). The Sense of Sharing Index exhibited good internal reliability (Cronbach’s α = .88).
Sense of Belonging
We measured the participants’ sense of belonging to the IFCP community by using two items from the Sense of Community Index (Long & Perkins, 2003). Participants were asked to rate their agreement with these items on a 5-point Likert-type scale. We then calculated their overall score to generate the mean score. A high score reflected a stronger sense of belonging to the IFCP community. A previous study showed adequate psychometric properties for the original index (Obst & White, 2004). In the current study, the scale showed adequate internal reliability with a Cronbach’s α of .87.
Procedure
All measures were completed through an online survey using Qualtrics software. The study was approved by the institutional review board of the School of Social Work at Bar-Ilan University. In addition, the study was also approved by the Research Division of the Ministry of Welfare and Social Affairs, State of Israel, the governmental entity responsible for the IFCP. Participants were recruited by the managers of six IFCPs that were chosen by the steering committee of the study to participate. Three of the IFCPs were in urban areas, and three were in rural areas. In both cases, we selected one center each from the north, the center, and the south of Israel. We provided the managers of the IFCPs with a link to the online questionnaire, which they then forwarded to all of the users of the IFCPs. The data were collected during May 2020. Information on the response rate is not available.
Statistical Analysis
We utilized Pearson’s correlations to assess the associations between the research variables. A two-step structural equation modeling procedure was employed using analysis of moment structures software to estimate the parameters: a measurement model and a structural model. Data normality was scrutinized using skewness and kurtosis in SPSS. All of the factors displayed validated values for skewness and kurtosis (<+2), which confirmed the absence of abnormality in the data. The fit indices chosen were the Tucker–Lewis index (TLI), incremental fit index (IFI), comparative fit index (CFI), and the root mean square error of approximation (RMSEA). To directly test the proposed moderation model, we conducted a regression-based path analysis using Process software (Hayes, 2012).
Results
Results of the Structural Equation Modeling
In the structural equation modeling analysis, we applied a composite or full structural model, combining factor analysis (the measurement model) and path analysis (the structural model). Based on the Bivariate correlations between research variables (see Table 1), and omitting the nonsignificant associations, the research model yielded a nonsignificant chi-square statistic, χ2(df=16) = 20.83, p = .185. The null hypothesis is that the predicted model and observed data are equal. Therefore, a nonsignificant chi-square result indicates a good model fit. In addition, fit indices indicated that the model fit the data very well: TLI = 0.962; IFI = 0.984; CFI = 0.983; RMSEA = .041. Regarding the TLI, IFI, and CFI, a value of 1 represents a perfect fit. A value ≥ 0.9 indicates a reasonable fit (L. T. Hu & Bentler, 1998). A value of ≥0.95 is considered an excellent fit (Kline, 2005). In relation to RMSEA, values ≤0.05 are considered excellent (MacCallum et al., 1996). Figure 1 presents the research model.Structural equation modeling showed that the family’s quality of life during the first wave of COVID-19 in Israel was best explained by family resources (β = 0.48***). More family resources predicted a better quality of life for the family. In addition, the IFCP’s operations had a positive effect on the family’s quality of life (β = 0.23**) with better operation of the IFCP predicting a better quality of life for the family. A modest but significant contribution was found for the sense of community (β = 0.19*) in predicting a better quality of life for the family. These variables explained 38% of the variance in the total family’s quality of life score. Family distress was explained only by family resources (β = −0.31***), and not by the IFCP’s operations or sense of community.
Correlation Matrix for the Variables in the COVID-19 Study.
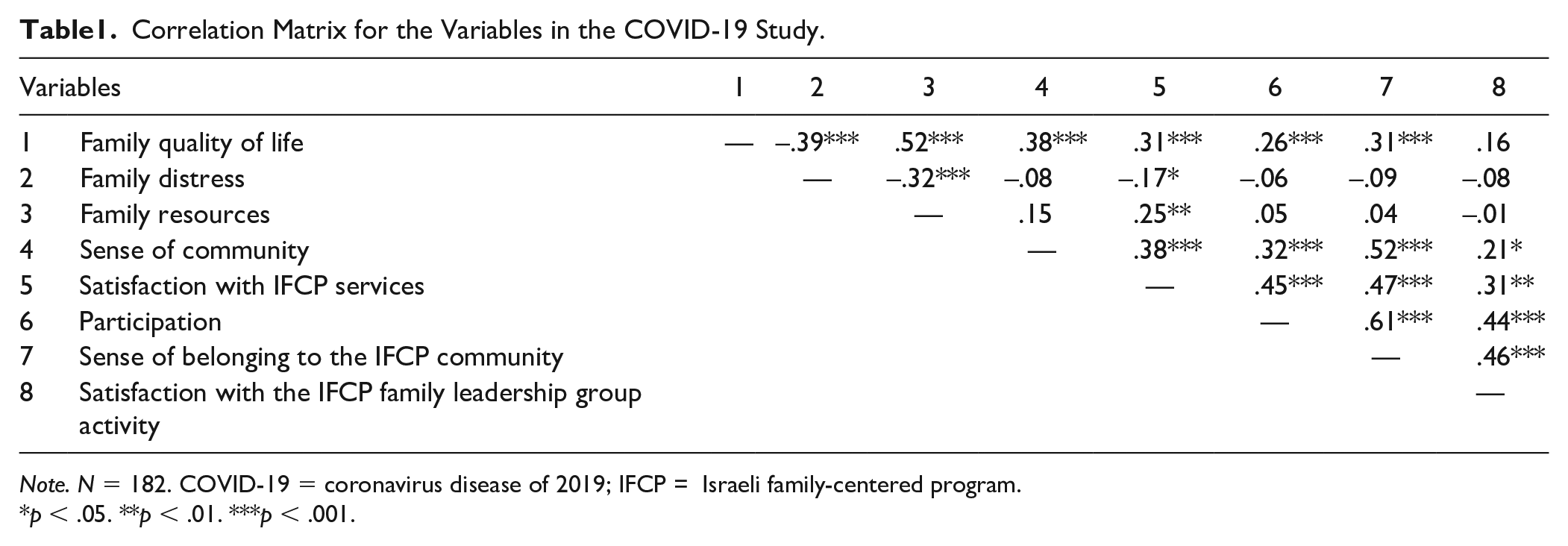
Note. N = 182. COVID-19 = coronavirus disease of 2019; IFCP = Israeli family-centered program.
p < .05. **p < .01. ***p < .001.
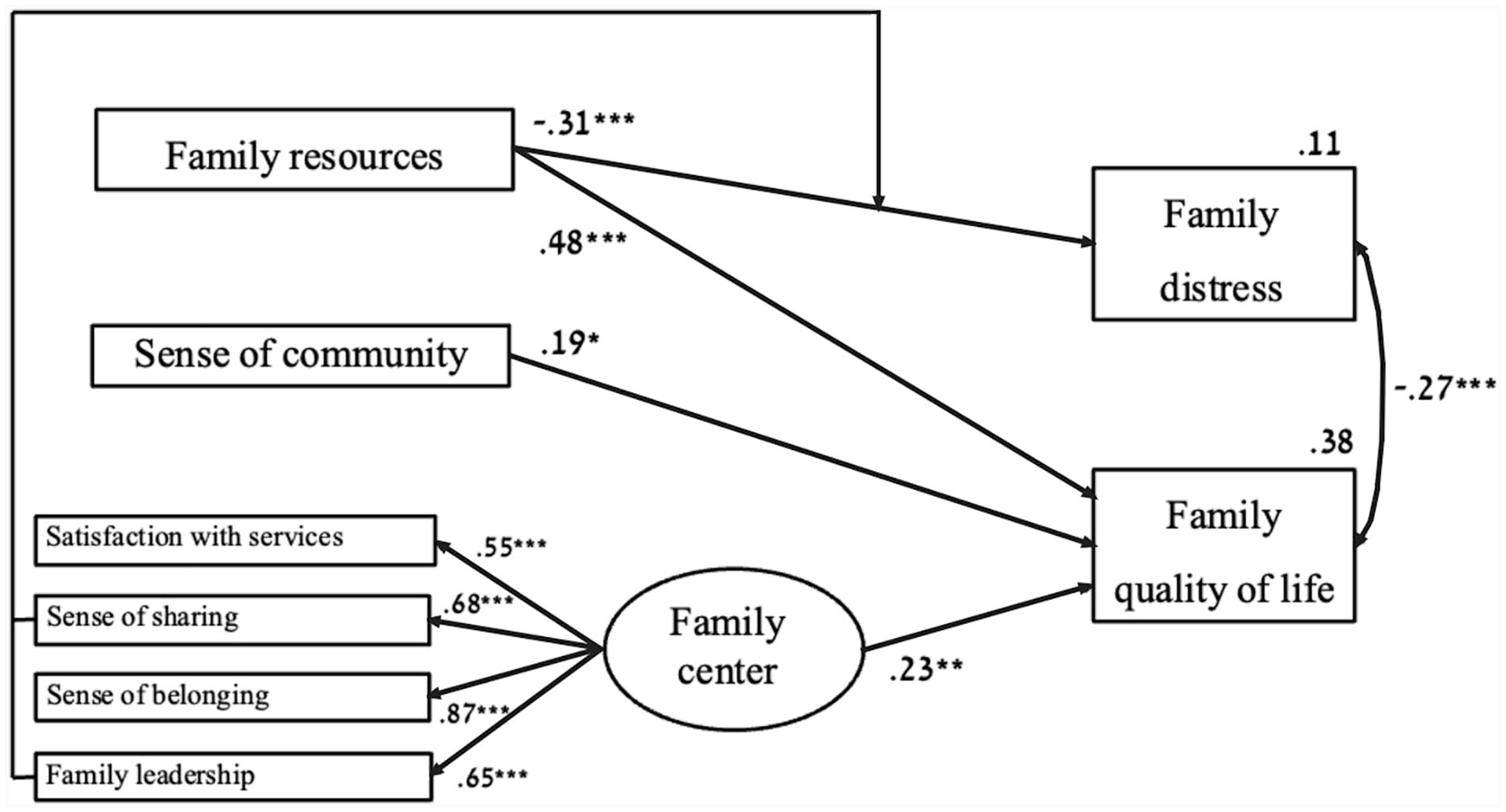
Structural Equation Modeling to Explain Family Distress and Family Quality of Life (N = 182).
Moderating Effects of the IFCP’s Operation
The proposed research model suggests that the IFCP’s operations, which include satisfaction with the IFCP’s services, participation, a sense of belonging to the IFCP’s community, and satisfaction with the IFCP’s family leadership group activity, all moderate the association of family resources with family distress and quality of life. These factors also moderate the association of a sense of community with family distress and quality of life. Among the moderation models examined, only the two following moderating effects were significant.
Participation Moderates the Association Between Family Resources and Family Distress
Results showed that participation significantly moderated the association between family resources and family distress (B = 0.42, SE = 0.21, LLCI = 0.006, ULCI = 0.828, p < .05). Among families with a high level of resources, family distress was low. Furthermore, the differences between families who experienced little, moderate, or strong participation were insubstantial. In contrast, among families with a low level of resources, participation was associated with significant differences in family distress. In these families, those who experienced lower participation reported more family distress than did those who experienced moderate or strong participation.
Family Leadership Moderates the Association Between Family Resources and Family Distress
Results showed that satisfaction with the IFCP’s family leadership group activity significantly moderated the association between family resources and family distress (B = 0.49, SE = 0.21, LLCI = 0.0799, ULCI = 0.9071, p < .05). Among families with a high level of resources, family distress was low. Furthermore, the differences between families that reported little, moderate, or strong satisfaction with family leadership activities were not substantial. In contrast, among families with a low level of resources, family leadership was associated with a significant difference in family distress. In these families, those who reported little satisfaction with family leadership activities reported more family distress than those who experienced moderate or strong satisfaction with family leadership activities.
Discussion
During the COVID-19 pandemic, people with disabilities and their families are more likely than others to experience negative outcomes (Sabatello et al., 2020; WHO, 2020). More specifically, the closure of special education facilities, along with regulations requiring self-isolation and social distancing, increases the burden of care on families of children with disabilities. Therefore, families of children with disabilities may experience more family distress and a decreased quality of life.
The IFCPs for families of children with disabilities employ community and family-centered approaches to support families in routine times and in emergencies (Loeff & Rivkin, 2017). This study focused on the contribution of family-centered social services to helping families cope with very stressful circumstances, such as the COVID-19 crisis. Our research model explains family distress and quality of life among Israeli families of children with disabilities during the first wave of the COVID-19 pandemic based on their family resources, sense of community, and the IFCPs’ operations.
We expected that a family’s resources and sense of community would have a positive association with family outcomes during the COVID-19 crisis. In addition, we posited that obtaining resources might protect the family and its members from the negative consequences of the resources lost during a crisis. Hence, we expected that the IFCPs’ operation during the crisis would moderate the association of family resources and a sense of community with family outcomes. Our findings supported these contentions to some degree. Family resources made the strongest contribution to explaining the family’s quality of life, while a sense of community made a modest contribution. A moderate positive effect was attributable to the IFCP’s operations, including satisfaction with the IFCP’s services, participation, a sense of belonging to the IFCP’s community, and satisfaction with the IFCP’s family leadership group activity. The findings of this study concur with those of other studies conducted during crises, which have found that quality of life is related to personal resources, a sense of belonging to the community, and a sense of participation (Asbury et al., 2021; Dekel & Tuval-Mashiach, 2012; Gelkopf et al., 2012; Levy & Friedman, 2019). A family’s resources were the only explanation found for its level of distress. However, this association was moderated by participation in, and satisfaction with, the IFCP’s family leadership group activity. Among families with a low level of resources, participation and satisfaction with the family leadership group activity were associated with significant differences in family distress. In these families, those who experienced strong participation and strong satisfaction with the family leadership group activity reported less family distress than those who had low participation and experienced little satisfaction with family leadership activity.
The results expand our understanding about the role of IFCPs in times of national crisis. These services create an environment in which families are empowered, identify, and address the individual needs of each family member, and give family members the tools to become active agents in their own care. The underlying premise of this approach is that parents, knowing their own capabilities and the needs of their children, are best equipped to make decisions about the kinds of services and support they require. Therefore, these services encourage family involvement, allowing the family to seek the care and resources they need to better care for their children with disabilities and improve their collective quality of life (Bruder, 2010; Dempsey & Keen, 2008; Keen, 2007; Law et al., 2003; Sheridan & Burt, 2009). In the field of disability, family-centered services should promote greater agency and self-determination among parents, streamline collaboration between families and available services, and heighten self-efficacy among parents (Tomasello et al., 2010).
The positive effects of IFCPs are likely not limited to emergencies, and they are expected to reduce stress and improve the quality of life for families at all times. Hence, this study supports family-centered practice for families of children with disabilities at all times. Two factors moderated the association between lack of family resources and increased family distress: participation and satisfaction with family leadership activity. These two factors highlight the importance of the partnership between parents of children with disabilities and their service providers. This sense of partnership can provide families with more control over their own lives (Beckman, 2002; Resch et al., 2010; Sheridan & Burt, 2009).
Family leadership programs are designed to empower families by transforming them from passive participants into active agents in their own care. For families of children with disabilities, this means soliciting parental input to coproduce unique services for each family, assessing and nurturing parents’ strengths, encouraging parent-to-parent support, and giving families the opportunity to advocate for themselves both locally and nationally as part of the larger socio-political conversation (Morrison & Espiner, 2018). Indeed, participants in these leadership development programs describe them as central to their personal development and even as life-changing (Freedman & Boyer, 2000; Shepherd & Kervick, 2016).
Limitations
The study’s results should be interpreted with caution. The first limitation is the nonrandomized sampling method. Nonrandomized samples are those in which the probability that a subject is selected is unknown, and therefore, some members of the population may be more likely to be included than others. As a result, participants may disproportionately possess certain traits that could affect the study outcome. Although nonrandomized samples are used in convenience sampling, a sampling bias risk exists. The second limitation is associated with the cross-sectional approach. Given the fact that we assessed all of the variables simultaneously, there is no evidence of a temporal relationship between the independent variables and the outcomes. Hence, it is impossible to establish a cause-and-effect relationship. Furthermore, interpretation of the findings needs to consider the lack of data on the participants’ family resources, sense of community, and the IFCPs’ operation before the COVID-19 pandemic. Additional limitations were that the majority of the participants were mothers, that the data were self-reported, and that we did not confirm the children’s diagnoses.
Implications for Practice
The research makes clear that IFCP services benefit families of children with disabilities in times of crisis. Moreover, the partnership between families and service providers moderates the association between low levels of resources and family distress, even in extremely stressful circumstances, such as the first wave of the COVID-19 crisis. The results of this study highlight the importance of the partnership and coproduction of services between parents of children with disabilities and their service providers. Coproduction refers to the joint involvement of professionals and laypeople in designing, planning, creating, implementing, and evaluating social policy and in delivering public services (Nabatchi et al., 2017; Osborne et al., 2016; Pestoff et al., 2013). As such, coproduction is increasingly recognized in public services internationally (Holland-Hart et al., 2019) and is viewed as a cornerstone of social innovation in the public sector (Voorberg et al., 2015). By considering citizens as valuable partners in public service delivery and by basing policy on information exchanges, shared decision-making, and crowdsourcing, this approach is effective in responding to complex and unique service user needs and providing better quality services (Beeri, 2021; Realpe & Wallace, 2010; Vamstad, 2012).
There is a need to continue investing in parents’ and families’ self-determination and leadership at the local and national levels, in order to ensure that families have clear and meaningful options to design the services they need (Cohen & Mosek, 2019; Cooper & Ward, 2011). Despite the importance of parental leadership in service planning and the impact of this on social policy around disabilities, research on building leadership and development skills among parents of children with disabilities is limited (Shepherd & Kervick, 2016). There are also few studies on how these factors affect social policy (Parish et al., 2003). Family policy in the disability field ought to develop a formal and robust communication infrastructure, such as public round tables. It should also provide training, such as agenda-setting courses for both family members of children with disabilities and service providers, to promote better partnerships and coproduction processes between them.
Implications for Family-Centered Services in Times of Emergency
In times of crisis, family-centered service should focus first on mapping the dynamic needs of families of children with disabilities and then adapt their services accordingly. As Hindi and Gur (2020) described, in an emergency, IFCPs become a channel for information and communication between government officials and families of children with disabilities. Hence, it is essential to strengthen their online capabilities by purchasing appropriate equipment and by training service providers to work both online and offline. It is also necessary to routinely engage in hybrid service delivery in order to preserve these capabilities and ensure that service providers can use them effectively in times of emergency. Service providers should develop additional channels and tools for providing vital information to families in real-time, particularly to populations with limited access to the internet and technology. However, beyond its primary role as a communication channel, the IFCP also addressed other family needs, including providing emotional support and leisure activities (Hindi & Gur, 2020). In times of emergency, family-centered services must flexibly and creatively adapt their services to their clients’ current needs. Furthermore, we recommend that the IFCPs’ employees cooperate with local emergency teams, as the former’s expertise and intimate knowledge of the families, will enable them to advise those in the local authority about how to effectively support families of children with disabilities in times of emergency.
Implications for Future Study
While parents of children with disabilities may benefit from involvement in coproduction processes, they tend to experience unique barriers to doing so (Cohen & Mosek, 2019). Government policy has a critical role in generating the conditions under which families of children with disabilities participate in coproduction processes. Therefore, existing government policies can facilitate or hinder participation and involvement in public service coproduction (Bovaird & Löffler, 2013; Holland-Hart et al., 2019). There is scarce research overall on coproduction processes involving families of children with disabilities (Jenhaug & Askheim, 2018). Therefore, future research should explore the barriers and facilitators in coproduction processes. More specifically, there is a need to explore the relationship between family leadership groups in the disability field and the government bodies with whom they engage, to understand the diverse mechanisms and pathways through which family leadership groups influence policy design; and to identify barriers and facilitators for coproduction from the perspectives of family leadership group members and government officials.
Footnotes
Declaration of Conflicting Interests
The authors report no declarations of interest. The first and second authors report no conflicts of interest. The third author is employed by Ashalim JDC-Israel.
Funding
This research project was funded by Ashalim JDC-Israel and the Israeli Ministry of Welfare and Social Affairs.