
Abstract
The establishment of reciprocal friendships is a challenge for many individuals with autism spectrum disorder (ASD). Social interaction difficulties emerge early, persist throughout development, and have widespread functional impact. As such, interventions focused on social functioning are needed in early intervention programs. This two-part study evaluated the outcomes of a parent-assisted social skills training (SST) program for young children with ASD. The intervention is a downward extension of the Program for the Education and Enrichment of Relational Skills (PEERS(R)), which is one of the few evidence-based SST programs for adolescents and young adults with ASD. Modifications included developmentally appropriate social skills, greater parent involvement, and behavioral strategies embedded in play-based activities. Results reveal improvements in parent ratings of social responsiveness, social cognition, and social motivation, as well as decreased (a) restricted/repetitive behaviors and interests and (b) problem behaviors. Results are promising and encourage further evaluation of this SST curriculum.
Social impairment is a hallmark feature of many neurodevelopmental disorders and significantly affects individuals with autism spectrum disorder (ASD) across all levels of cognitive and language functioning (Carter et al., 2005). Social interaction and relationship differences emerge early in childhood and become more apparent as social contexts increase in complexity across major developmental periods. By preschool, these social difficulties may present as less involvement with peers (e.g., remaining on the periphery of activities and spending less time interacting with peers), difficulty interpreting social cues, trouble maintaining shared conversations, and difficulty developing and maintaining friendships (Barry et al., 2003; Church et al., 2000; McConnell, 2002).
The outcome of these social difficulties on overall wellbeing is substantial; manifesting in poorer peer relationships (e.g., peer rejection, isolation, bullying, fewer friendships and of reduced quality) and the development of co-occurring internalizing conditions (Barnhill, 2001, 2007; Bauminger & Kasari, 2000; Chamberlain et al., 2007; Church et al., 2000; Howlin & Goode, 1998). These social differences are recognized by children with ASD as well (Bauminger & Kasari, 2000; Church et al., 2000). Given the early onset and persistence of these social challenges, many of which are unlikely to resolve on their own (Howlin et al., 2000; Rao et al., 2008), evidence-based interventions directly addressing social functioning in young children with ASD are needed. Moreover, as the call for placement in inclusive settings grows, it is important to recognize that closer proximity to neurotypical peers alone will not improve social functioning. Rather, developmentally appropriate, structured teaching and support is needed so that children with ASD have the opportunity to experience greater and more positive social engagement in these inclusive settings (Laushey & Heflin, 2000; see McConnell, 2002, for review; Rogers, 2000).
Social skills training (SST) programs are popular in treatment planning across the lifespan (Reichow & Volkmar, 2010). Social skills training programs vary considerably in the targeted social behaviors (e.g., ranging from specific skills like sharing to broader concepts such as theory of mind), but they all aim to teach fundamental skills needed for successful everyday social situations (Paul, 2003; Rogers, 2000). Intervention studies related to the development, evaluation, and dissemination of SST programs for individuals with ASD have steadily increased since the early 2000s.
In a meta-analysis of randomized controlled trial studies for group SST programs for children with ASD, Gates et al. (2017) found that the effect size for these interventions varied by informant. Group SST programs had an overall medium effect size, but closer examination showed that parents and observers reported small effects, teachers reported none, and self-report effects were likely reflective of knowledge gain rather than change in social behaviors. Similarly, other studies asserted that gains are obtained but limited in scope. Changes were largely linked to specific social behaviors targeted in the intervention while generalization of skills to new situations was limited and improvement limited to a subset of the children (Barry et al., 2003; Kasari & Patterson, 2012; Rao et al., 2008; White et al., 2007; Yoder et al., 2013).
The knowledge base of effective SST teaching strategies continues to expand as the number of systematic reviews grows. Youth with ASD may especially benefit from SST interventions when several important factors are considered, such as simplifying complex, abstract social interactions into concrete behaviors; targeting relevant and directly meaningful goals; providing structure and predictability; teaching skills in a stepwise fashion; including cooperative work; reducing interfering behaviors and reinforcing positive behaviors; and programming for skill generalization and maintenance (Krasny et al., 2003; White et al., 2007 Preschoolers specifically may benefit from modeling and prompting, direct instruction, skills-focused storytelling, practice and rehearsal of social skills, play activities to encourage practice of skills, and behavior management strategies. Of these strategies, the most effective strategies may include modeling and prompting, learning through play activities, and behavioral practice and rehearsal (Vaughn et al., 2003).
Several factors may limit the degree to which SST programs may be impactful for young children with ASD. There are fewer empirically supported SST programs for children under the age of 6 years in comparison to older children (Hwang & Hughes, 2000; Kroeger et al., 2007; Matson et al., 2007; Reichow & Volkmar, 2010). Few studies sufficiently characterize their sample, which may be a limitation with regard to understanding which subset of children may benefit from the intervention (White et al., 2007). In addition, few social interventions include an active parent training component (DeRosier et al., 2011; Reichow & Volkmar, 2010). Parents may contribute to more successful learning opportunities, better overall treatment gains, and stronger durability of treatment gains over time (DeRosier et al., 2011; Kaat & Lecavalier, 2014; Reichow & Volkmar, 2010). Active parent training may be particularly ideal for young children given their capacity to provide direct teaching of social skills and supervise their child’s play interactions in a developmentally appropriate manner (Frankel & Myatt, 2013).
Therefore, continued efforts to better understand and formulate SST programs for young children with ASD are warranted. In this two-part study, we developed a time-limited SST program for young children with ASD without substantial intellectual disability. Several of the aforementioned treatment strategies were utilized, including parent training, play-based group format, multimodal teaching strategies, and teaching of concrete skills for positive peer interactions and friendship building. The aim of the open trial phase (Study 1) was to assess family engagement and immediate treatment outcomes. The aim of the pre-post treatment phase (Study 2) was to improve the intervention based on clinician and family feedback from Study 1, while continuing to assess family engagement and immediate treatment outcomes. Across studies, key research questions included the following:
Method: Study 1 (Open Trial)
Participants
Five young children (four male, one female) between the ages of 4 and 6 years (M = 5.28 years) and their parents (four mothers, one father) participated in the open trial phase. All children had a previous diagnosis of ASD from a licensed community provider or agency. School placement consisted of preschool (n = 1), transitional kindergarten (n = 1), and kindergarten (n = 3). The sample was ethnically diverse: 40% Asian (n = 2), 20% Caucasian (n = 1), 20% Latino/Hispanic (n = 1), and 20% “other” (n = 1).
The mean baseline Autism Diagnostic Observation Schedule–Second Edition (ADOS-2; Lord et al., 2012) comparison severity score (CSS) was in the “moderate” severity range (M = 6.20, SD = 1.30). Cognitive functioning, as measured by the Kaufman Brief Intelligence Test–Second Edition (KBIT-2; Kaufman & Kaufman, 2004), placed participants in “well below average” to “above average” ranges across composite, verbal, and nonverbal domains (Composite range = 75–116). Overall adaptive functioning, as measured by the Vineland Adaptive Behavior Scales–Second Edition (Vineland-II; Sparrow et al., 2005) Adaptive Behavior Composite (ABC), placed all participants in the lower end of the average range (M = 89.60, SD = 18.17), with scores ranging from “low” to “moderately high” (ABC range = 65–116). See Table 1 for additional demographic and baseline information.
Mean Demographic Variables for Study Participants.
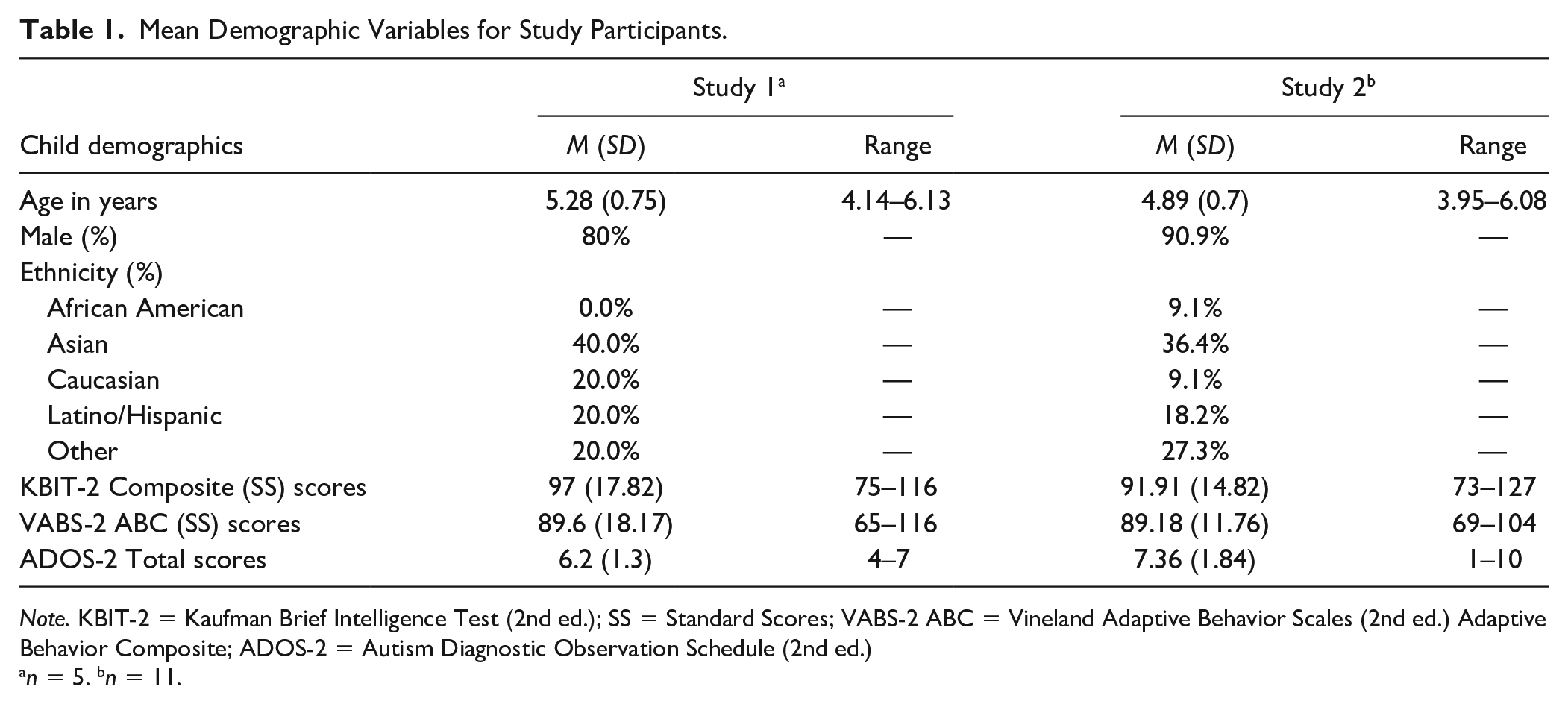
Note. KBIT-2 = Kaufman Brief Intelligence Test (2nd ed.); SS = Standard Scores; VABS-2 ABC = Vineland Adaptive Behavior Scales (2nd ed.) Adaptive Behavior Composite; ADOS-2 = Autism Diagnostic Observation Schedule (2nd ed.)
n = 5. bn = 11.
Measures
Autism Diagnostic Observation Schedule–Second Edition
The ADOS-2 (Lord et al., 2012) is a standardized, semi-structured, observational assessment that evaluates behaviors associated with ASD across conversational and play activities. It was administered by site- or research-reliable pre- and post-doctoral clinical psychology trainees at baseline to support ASD diagnosis for study inclusion. For this study, participants were administered either Module 2 or Module 3 based on their expressive language level and chronological age.
Kaufman Brief Intelligence Test–Second Edition
The KBIT-2 (Kaufman & Kaufman, 2004) was administered to child participants at baseline by trained pre- and post-doctoral clinical psychology trainees to obtain an estimate of intellectual functioning and to determine eligibility. Verbal, Nonverbal, and Composite (overall) standard scores, which have a mean of 100 and standard deviation of 15, were calculated.
Vineland Adaptive Behavior Scales–Second Edition, Survey Form
Parents completed the Vineland-II (Sparrow et al., 2005) survey form at baseline to provide an estimate of their child’s adaptive functioning across four subdomains: Communication, Daily Living Skills, Socialization, and Motor. Parents rated the degree to which their child independently demonstrated the target behavior. To meet eligibility requirements, participants must have scored at least one standard deviation below the mean on the Socialization domain.
Social Responsiveness Scale, Second Edition—School Age
The SRS-2 (Constantino & Gruber, 2012) measures the presence and severity of ASD-related social impairments. The SRS-2 School Age form was completed at baseline and post-treatment by parents to assess treatment outcome. The SRS-2 uses T-scores with a mean of 50 and a standard deviation of 10, with higher scores indicating greater impairment. A Total Score of overall social impairment is calculated, along with treatment subscale scores in the areas of Social Communication, Social Cognition, Social Awareness, Social Motivation, and Restricted Interests and Repetitive Behaviors.
Social Skills Improvement System Rating Scales
The SSIS (Gresham & Elliott, 2008) assesses prosocial skills and problem behaviors in children ages 3 to 18 years and was completed at baseline and post-treatment by parents to assess treatment outcome. Prosocial skills are measured across seven domains: communication, cooperation, assertion, responsibility, empathy, engagement, and self-control. Problem behaviors are assessed across five domains: internalizing, externalizing, bullying, hyperactivity/inattention, and autism spectrum. Parents rated how often behaviors occurred. Higher scores on the Social Skills domain reflect better social functioning, whereas lower scores on the Problem Behaviors domain indicate better behavioral regulation.
Quality of Play Questionnaire
The QPQ (Frankel & Mintz, 2010) is a 26-item questionnaire that assesses the frequency of playdates and was used in this study as a measure of child social engagement (i.e., frequency of contact with peers) at baseline and post-treatment. Parents were asked to report the number of playdates their child hosted in their home and the number of playdates to which their child was invited in the previous month. According to Frankel and Mintz (2010), less than 2.5 playdates (invited or hosted) classified approximately 67% of a clinic-referred sample, whereas greater than 2.5 playdates (invited or hosted) correctly classified about 60% of a community sample (Frankel & Mintz, 2010).
Procedures
Participant recruitment
All procedures involving human participants were in accordance with the ethical standards of the institutional review board and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Participants were recruited from the UCLA Early Childhood Hospitalization Program, a university-based autism research and treatment center, and the UCLA PEERS(R) Clinic, a university-based treatment clinic providing parent-assisted, evidence-based social skills interventions for individuals with autism and other social challenges. Eligibility requirements were initially assessed via phone screen followed by an in-person appointment. To be considered for inclusion, the child was between 4 and 6 years of age; had a pre-existing diagnosis of ASD from a reliable mental health professional; had considerable peer difficulties (Vineland-II Socialization score < 85); possessed sufficient expressive language as defined by consistent, spontaneous speech comprising at least four- to five-word phrases or sentences; and had a parent who was fluent in English and willing to participate in the study. Exclusion criteria included substantial intellectual disability (KBIT-2 Composite score < 70), current physical aggression or violence, major mental illness or other interfering psychiatric conditions, and a physical or medical condition that would prevent full participation.
Children receiving psychopharmacological intervention were not excluded if medications were stable. Most children were receiving school and in-home or community-based services, which remained stable throughout the study. Families agreed to delay or temporarily withdraw from any other social skills treatment during their study participation. All participants agreed to attend at least 13 of the 16 group sessions.
Of the screened families, eight families met eligibility criteria and completed baseline assessment measures. After baseline assessments (T1) were completed, participants received the 16-week intervention. Three families discontinued during treatment due to change in availability or treatment priority (i.e., physical aggression, inability to separate from parent during the child session). Five families remained in the open trial. At the end of the intervention, participants completed post-treatment assessments (T2).
Intervention overview
The SST curriculum of the current study, Program for the Education and Enrichment of Relational Skills (PEERS(R)) for Preschoolers, includes core structural elements of the PEERS(R) treatment curriculum for adolescents and young adults, which is one of the few evidence-based social skills treatment programs for individuals with ASD (Laugeson, 2014, 2017; Laugeson & Frankel, 2010). These elements consisted of structured didactic lessons with “buzzwords” to highlight key social skills; role play demonstrations; behavioral rehearsal activities; parent education and training; and homework assignments (for a comprehensive review of the PEERS(R) treatment curriculum, see Laugeson et al., 2009, 2012). Developmentally and age-appropriate modifications were made, with a focus on teaching skills and encouraging social interactions through play (Paul, 2003). These modifications included didactic lessons led by puppets, behavioral rehearsal activities via popular group games, a predictable and consistent schedule of activities, and parent involvement. In addition, a group behavior management system was implemented to reinforce on-task behavior.
The intervention consisted of 16 sessions that occurred once weekly. The age range of 4 to 6 years allowed for participation of children beyond preschool, but “preschoolers” was included in the name to provide a general picture of the targeted social skills. Each session was 90 min, during which parents and children attended separate and joint concurrent sessions that focused on strategies for cooperative play and friendship development. A primary parent attended the group and served as the main social coach to help their child practice the newly learned skills and arrange playdates.
Parent and child group leaders consisted of licensed clinical psychologists and a post-doctoral clinical psychology fellow. The parent group leader facilitated the group independently while the child group leader conducted the group with the support of three to four behavioral coaches. Behavioral coaches were psychology graduate students or pre-doctoral psychology interns with experience working with youth with ASD. Behavioral coaches were responsible for monitoring treatment fidelity, assisting with the didactic instruction and role plays, and providing in vivo performance feedback to children and parents. During a weekly clinical case conference, the team discussed specific family goals and progress.
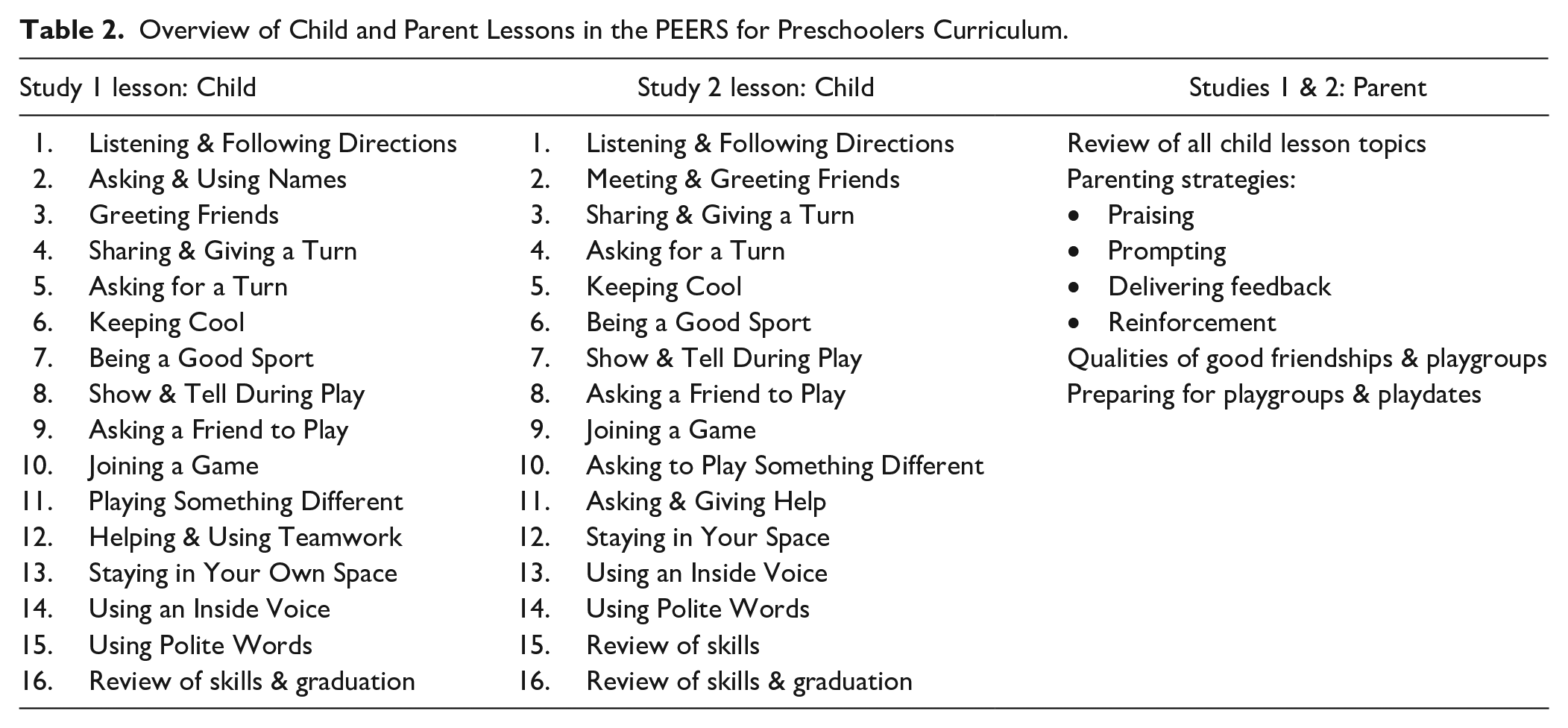
The curriculum focused on learning how to initiate play with peers and sustain reciprocal play interactions. Table 2 provides an overview of the child didactic lessons. Parent lessons included social coaching strategies, qualities of good friendships and playgroups, and strategies for having successful playdates. Topics of instruction were based on a comprehensive review of the extant literature describing characteristic social difficulties among young children with ASD, as well as common play and friendship-making skills in neurotypical young children. Skills were simplified into fundamental verbal and nonverbal behaviors, presented as concrete rules, and organized into sequential steps. The intervention progressed in a stepwise fashion, with novel skills introduced each week along with continued practice of earlier skills.
Overview of Child and Parent Lessons in the PEERS for Preschoolers Curriculum.
Child and parent groups occurred simultaneously but in separate rooms for a majority of the session (i.e., 60 min of the 90-min session). The child group began with a didactic lesson presented via a puppet show (15–20 min in length). In the context of naturalistic play situations (e.g., playing ball, building Legos, etc.), puppets modeled inappropriate social behaviors followed by prosocial friendship behaviors. To provide an additional opportunity for modeling, a behavioral coach demonstrated the target skill with puppets. The children then took turns practicing the skill with puppets, during which the behavioral coaches provided social coaching. The children then participated in two group behavioral rehearsal activities (two 15-min activities) that consisted of group games most of the children had some exposure to in other settings (e.g., Musical Chairs; What Time Is It, Mr. Fox?). The group activities provided a naturalistic context in which to practice the new skills while receiving social coaching from the clinical team. In between the group games, a bathroom break (10 min) was offered and relevant social skills were practiced (e.g., listening, maintaining appropriate body boundaries, and turn-taking).
In the parent group, parents received education and feedback regarding key social skills, behavioral strategies to address behaviors that impacted peer interactions, and strategies for creating natural social learning opportunities. Parent sessions followed a consistent routine each week and began with a review of the homework assignments from the previous week. Each family reported on their successes and challenges in completing the homework assignments, and the group leader provided individualized feedback and tailored the curriculum to meet the family’s specific needs. Then a parent didactic lesson was presented, followed by a review of the children’s lesson. Next, the group leader and parents reviewed relevant social coaching strategies to be practiced by parents during mock playdates with other group members (described in further detail below). Each week parents were provided with small coaching cards that highlighted the target social behaviors and provided specific social coaching tips. At the end of each group, homework assignments for the upcoming week were presented. Parents discussed how they planned to complete the homework assignments or possible barriers to homework completion, and the group leader helped to troubleshoot anticipated problems. The goal of homework assignments was to increase generalization and maintenance of the newly learned skills. Parents were provided with weekly handouts summarizing the targeted social skills and homework assignments.
For the last 20 min of each session, parents and children reunified for a parent-coached play exercise that consisted of mock playdates between two children from the study. Children were assigned pairs based on several factors: practice with multiple peers, mutual interests, language abilities, and level of coaching and behavior management needed. Families brought turn-taking games from home to use during the mock playdates. Children were expected to practice the newly learned skills while parents provided social coaching to their child using behavioral strategies introduced in the parent groups. Parents were given in vivo performance feedback on their social coaching. The clinical team modeled social coaching strategies as needed in order to successfully build parents’ coaching skills and confidence. In the open trial, the first six sessions consisted of large group games in order to familiarize parents with fundamental coaching strategies (e.g., prompting, getting their child’s attention, praising, etc.) during more structured activities. Dyadic playdates were introduced at Week 7 and remained until the end of the program. Each meeting concluded with a final wrap up; the lesson and homework assignments were reviewed, and the children received rewards from a prize box.
Treatment fidelity
All child and parent sessions were recorded to assess treatment fidelity. To calculate treatment fidelity, 20% of the sessions (three of child and parent sessions) were watched by raters naive to the study. For the child sessions, mean treatment fidelity was 97% (range = 92%–100%). For the parent sessions, mean treatment fidelity was 84% (range = 78%–93%).
Results: Study 1 (Open Trial)
Family engagement was high, as measured by overall attendance of 94% across all participants. Individual participant attendance ranged from 88% to 100%.
Baseline (T1) to post-treatment (T2) comparisons were conducted using paired samples t tests for the parent-reported SRS-2, SSIS, and QPQ (see Table 3). Due to limited power resulting from a small sample size (N = 5) in the open trial, T1 to T2 comparisons were not statistically significant; however, effect sizes (per Cohen, 1988) reveal clinically meaningful findings. In particular, SRS-2 Total Scores decreased nearly a full standard deviation by an average of 9.00 T-score points (p = .158, d = .776), indicating a strong trend with a medium to large effect overall. SSIS Social Skills scores increased by an average of 5.40 Standard Score points (p = .633, d = .132) and SSIS Problem Behavior scores decreased by an average of Standard Score 2.20 points (p = .782, d = .231) with small effect sizes. On average, children were having 1.6 additional playdates per month with children unaffiliated with the program following treatment (p = .227, d = .637, medium effect) as measured by the QPQ. This included hosting 1.0 additional playdates per month (p = .189, d = .707, medium to large effect) and being invited to 0.60 more playdates per month (p = .426, d = .396).
Mean Pre- and Post-Treatment Scores for Outcome Measures.
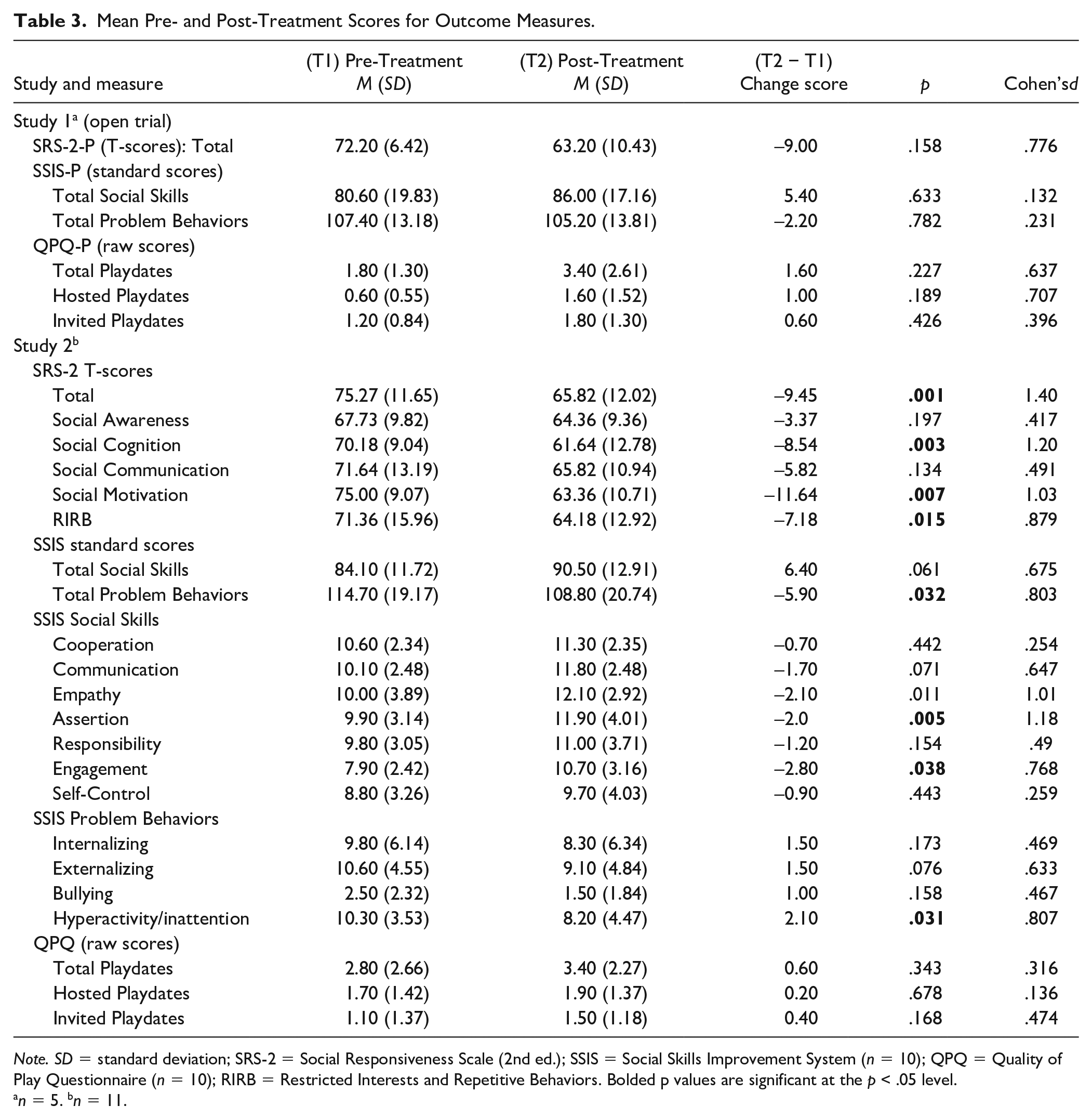
Note. SD = standard deviation; SRS-2 = Social Responsiveness Scale (2nd ed.); SSIS = Social Skills Improvement System (n = 10); QPQ = Quality of Play Questionnaire (n = 10); RIRB = Restricted Interests and Repetitive Behaviors. Bolded p values are significant at the p < .05 level.
n = 5. bn = 11.
Method: Study 2
Participants
Nineteen participants initially enrolled, but five families dropped from the study due to relocation, childcare issues, and medical issues. Three families completed the intervention phase but did not return for post-treatment assessments. Following attrition, a total of 11 children (10 males, 1 female) completed Study 2. All 11 children were enrolled in school; nine children were in preschool, one child was in transitional kindergarten, and one child was in kindergarten. Mean age of the participants was 4.89 years (range = 3.95–6.08 years), with one child within 1 month of turning 4 years old and all other children ranging from ages 4 to 6 years. Parent-reported child ethnicity was as follows: 9.1% African American (n = 1), 36.4% Asian (n = 4), 9.1% Caucasian (n = 1), 18.2% Latino/Hispanic (n = 2), and 27.3% “other” (n = 3). Consistent with their pre-existing diagnosis of ASD, mean baseline ADOS-2 CSS was in the “moderate” severity range (M = 7.00, SD = 2.61). Mean KBIT-2 Composite scores ranged from 73 to 127 (SS = 89–96), reflecting a range of functioning from “well below average” to “well above average.” The Vineland-II ABC Standard Scores ranged from 69 to 104, spanning “low” to “adequate” ranges with the mean score in the average range (M = 89.18, SD = 11.76). See Table 1 for additional demographic and baseline information for Study 2 participants.
Measures
The measures used in Study 2 were identical to those used in the open trial (Study 1).
Procedures
Participant recruitment and eligibility screening was consistent across Studies 1 and 2. After the conclusion of the open trial, minor modifications to the intervention were made based on an assessment conducted with parents following treatment (e.g., parents requested more time spent in the dyadic playdates), along with consensus from the treatment team. Substantial changes to the intervention included combining lessons on meeting/greeting friends and asking/giving help; introducing an additional week of lesson review; introducing dyadic playdates in Week 1; and revising group behavioral rehearsal activities (see Table 2).
Treatment fidelity was calculated for 20% of all sessions (seven child and parent sessions) using the same procedures from Study 1. For the child sessions, mean treatment fidelity was 99% (range = 96%–100%). For the parent sessions, mean treatment fidelity was 85% (range = 60%–100%).
Results: Study 2
Family engagement was moderately high, with overall attendance at 87%. Individual participant attendance ranged from 69% to 94%.
Pre- to post-treatment comparisons were conducted using paired samples t tests for the SRS-2 and SSIS, and QPQ (see Table 3). Consistent with Study 1 findings, SRS-2 Total Scores decreased nearly a full standard deviation by an average of 9.45 T-score points (p = .001, d = 1.40), indicating a clinically and statistically significant improvement with a large effect size. Change was statistically significant in the following domains: Social Cognition (p = .003, d = 1.20), Social Motivation (p = .007, d = 1.03), and Restricted Interests and Repetitive Behaviors (p = .015, d = .879). From pre- to post-treatment, T-scores decreased by 8.54, 11.64, and 7.18 T-score points, respectively, and effect sizes were large. Changes were not statistically significant in the Social Awareness or Social Communication domains, and effect sizes were small to medium.
Pre- and post-treatment parent-reported SSIS scores were available for 10 of the 11 participants. From pre- to post-treatment, there was a statistically significant decrease in parent-reported SSIS Problem Behavior scores, which decreased by an average of 5.90 SS points (p = .032, d = .803, large effect), and a strong trend toward a significant improvement in parent-reported SSIS Social Skills, with children improving on average 6.40 SS points (p = .061, d = .675, medium to large effect). To better understand the source of these changes, post hoc analyses were conducted for SSIS subdomains. Results indicated a statistically significant decrease in Problem Behaviors in the subdomain of Hyperactivity/Inattention (p = .031, d = .807, large effect), along with a strong trend toward a decrease in Externalizing behaviors (p = .076, d = .633, medium to large effect). Results further indicated statistically significant improvements in SSIS Social Skills in the following subdomains: Assertion (p = .005, d = 1.18, large effect), Empathy (p = .011, d = 1.01, large effect), and Engagement (p = .038, d = .768, large effect), with a strong trend toward improvement in Communication (p = .071, d = .647, medium to large effect).
Pre- and post-treatment QPQ scores were available for 10 of the 11 participants. Although changes in scores were not statistically significant (possibly due to lack of power), children were having on average 1.6 more playdates per month (p = .227, d =.637, medium effect) at the end of treatment. Following treatment, on average children were being invited to 0.40 more playdates per month (p = .168, d = .474, small to medium effect), and hosting .20 more playdates per month (p = .678, d = .136, small effect).
General Discussion
The steady rise in the popularity of SST programs calls for continued study of existing treatments, as well as the development of more effective and efficient treatments. The aim of this study was to develop and assess family engagement and immediate treatment outcomes of a group-based, parent-assisted SST program for young children with ASD with IQs above 70 and moderate verbal fluency. Findings from this study are promising, call for further testing and expansion of this intervention, and contribute to the growing body of evidence that supports the role of SST programs in comprehensive treatment planning for young children with ASD. Across both phases, families showed good engagement as reflected in their consistent and high attendance throughout the 16-week intervention (averages of 94% and 87%).
While results from Study 1 were not statistically significant (potentially due to small sample size and being underpowered), the outcomes are arguably clinically meaningful in that overall social impairment associated with ASD symptomatology shifted from “moderate severity” to “mild severity” on the SRS Total Score, demonstrating a large effect size. Moreover, frequency of social engagement through organized playdates revealed a moderate effect size at the end of treatment, although not statistically significant (again possibly due to lack of power and small sample size). Thus, Study 1 findings are limited due to lack of statistical significance. Study 2 findings, which included a larger sample, corroborated the pattern of findings from Study 1, but to a larger degree and with statistical significance in several areas, including reduction in overall social impairment associated with ASD symptomatology and problem behaviors.
Positive changes in social behavior in Study 2 may also be associated with high level of parent involvement and use of empirically supported teaching strategies. Parents assumed a powerful role in treatment as they served as the mechanism through which their children had more regularly occurring social interactions with peers via playdates and playgroups; this allowed children to practice their skills during naturalistic peer interactions with parent feedback. This is a key feature of this study as many SST programs for young children are delivered without parent involvement (Reichow & Volkmar, 2010). Treatment gains may also be attributable to the structure and teaching strategies used across parent and child sessions. The intervention uses evidence-based methods of instruction, including consistent structure at each session, simplified language, behavioral modeling, behavioral rehearsal of newly learned skills in the context of play with other group members, in vivo performance feedback, and homework assignments to generalize skills to natural social settings (Krasny et al., 2003; Vaughn et al., 2003; White et al., 2007).
Several other aspects of this study are noteworthy. High attendance rates, coupled with parent-reported behavioral improvements, may reflect positive parent perceptions of the program; however, further study of parent perceptions and acceptability is needed. Second, manualized curricula were developed and refined based on parent and clinician feedback. Treatment manuals play an important role as they allow for replication of clinical trials and dissemination into community clinical practice settings. Since SST manuals are not yet customary (Rao et al., 2008; White et al., 2007), the development of the study’s manual is a strength and will allow for future research and dissemination efforts. Third, characterization of the samples eases replication studies (White et al., 2007) and provides information about who may be most likely to benefit from the program (Rao et al., 2008).
While the preliminary findings are encouraging and merit further testing, a limitations are noted. We cannot determine causality in these studies due to the lack of a control group. Future studies would benefit from larger samples using randomized controlled trial designs with active treatment control groups. Other possible improvements include the use of behavioral observation assessments as a more objective measure to assess the meaningful generalization of skills (e.g., assessing social behaviors during a playdate with a peer) rather than relying on parent observation measures, which could be inherently biased, particularly when parents are involved in treatment. Though parents reported positive changes in their child’s behavior, their participation in the intervention is a potential confound. To this end, data collection from various independent informants uninvolved with and naive to the study is needed (Goldstein et al., 2014). In addition, collection of more qualitative and quantitative data from parents about acceptability, engagement, and feasibility, including a post-treatment satisfaction survey or focus group and completion of weekly homework assignments, would be beneficial. As this study was implemented in a research setting, future studies should assess the feasibility of implementing the intervention in community-based settings. Finally, follow-up assessments would provide information about the durability and clinical significance of treatment gains over time (Goldstein et al., 2014; Strain & Schwartz, 2001).
In conclusion, given the current landscape of managed health care that is compounded by limited family resources and finite provider availability, the need for short-term, evidence-based SST programs that are accessible and acceptable to families has never been greater. The availability of effective SSTs in early childhood may have meaningful impact on later social-emotional health, overall development, and family functioning. Moreover, empowering parents to serve as primary agents of change may promote more robust gains during and after treatment, strengthen their sense of parenting self-efficacy, and may reinforce parents’ efforts to advocate for their children.
Footnotes
Acknowledgements
The authors thank the generous contributions of the clinical and research team at the UCLA PEERS Clinic for their steadfast support of this study, and the families who participated in this study, without whose involvement this research would not have been possible.
Authors’ Note
This study was conducted at the University of California, Los Angeles (UCLA). All authors were at UCLA during their involvement with the study.
Declaration of Conflicting Interests
Elizabeth A. Laugeson receives royalties from Routledge Publishing and John Wiley & Sons, Inc., for book sales related to the PEERS social skills curriculum.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.