
Abstract
Although transgender, nonbinary, and intersex (TNI) people are at greater risk for HIV acquisition than their cisgender counterparts, the research on HIV testing frequencies and predictors in this population is limited. Research focused on identifying HIV testing differences by gender among TNI people is especially lacking. This secondary data analysis examined differences in HIV testing frequencies by gender and identified the factors significantly associated with lifetime and recent HIV testing in a statewide convenience sample of TNI adults in the Mountain West region of the United States. Although chi-square test results indicated no significant gender differences in lifetime HIV testing, a significantly smaller proportion of nonbinary individuals reported receiving an HIV test in the last year when compared with transmasculine, transfeminine, and intersex individuals (Fisher’s exact p = 0.04). Multi-variable logistic regression results revealed that having to educate medical providers about transgender-related care was significantly associated with a higher likelihood of ever receiving an HIV testing (AOR = 2.82, 95% CI (confidence interval): [1.56–5.07], p < 0.01). Moreover, nonbinary individuals were significantly less likely to have received an HIV test in the last year (AOR = 0.30, 95% CI: [0.11–0.81], p < 0.05). These findings point to the potentially important role that provider factors may play in HIV testing for TNBI persons. Alongside recognition of the need for more empirical work to understand complex relationships identified in this study, the study results suggest that HIV testing efforts may need to focus more on expanding access to TNI individuals, including those who identify as nonbinary.
Keywords
Introduction
HIV testing is a foundational component of HIV prevention and care and serves as the gateway to HIV prevention and care service continua. 1 Frequent HIV testing not only indicates whether prevention methods are effective but also allows for early detection of HIV infection and linkage to care, which is associated with better HIV health outcomes and reduced community viral load. 2 In the United States, the Centers for Disease Control and Prevention (CDC) recommends that all individuals between the ages of 13 and 64 undergo routine HIV screening at least once in their lifetime. 3 For those at increased risk, including transgender and nonbinary (TNB) persons, the CDC advises testing at least annually, and in some cases every 3–6 months depending on ongoing risk exposures. 3 Moreover, the U.S. Department of Health and Human Services emphasized the important role HIV testing plays in reducing HIV incidence when it included the diagnosis of people with HIV as one of the four pillars of the Ending the HIV Epidemic (EHE) plan in 2019. 4
TNB individuals bear a disproportionate burden of HIV.4,5 Globally, transgender adults are 13 times more likely to acquire HIV than cisgender adults, 6 wherein an estimated 19.9% of trans women and 2.6% of trans men are living with HIV. 7 The US is no exception; though transgender individuals make up approximately 0.3% of the US population, they comprise about 2% of persons with HIV. 8 Given the disproportionately high rates of HIV in TNB people, it is critical to understand HIV testing frequencies and predictors in these populations. However, the majority of extant HIV research among transgender, nonbinary, and intersex (TNI) persons is conducted with trans women, who experience the highest prevalence of HIV among TNI individuals.9–11 Consequently, a paucity of research exists on other TNI subgroups, particularly transmasculine, nonbinary, and intersex adults.
Factors associated with HIV risk among TNI individuals
Literature suggests numerous factors are associated with HIV exposure among TNI persons. At the individual and dyad levels, these factors include sexual intercourse without a condom or under the influence of substances, having multiple and cisgender sexual partners, recent sexually transmitted infections (STIs), and stimulant use, among others.7,12–15 Other contextual or structural level factors include geographic variations (e.g., residence in Southern United States) and lower socioeconomic status.16,17 Importantly, literature suggests TNI persons can experience syndemics that can cluster in the community and lead to disproportionately greater burden of HIV infection alongside other co-occurring health disparities.
HIV testing among TNI individuals
The limited number of previous studies that examined demographic differences in HIV testing in TNI people reported varying results. Data from the 2015 US Trans Health Survey, the largest nationwide study of TNI persons indicated significant differences in HIV testing uptake among TNI populations. 18 Specifically, trans women and nonbinary individuals assigned female at birth had significantly higher odds of reporting never testing for HIV compared with transgender men. Importantly, 87% of the sample reported having never tested for HIV because of low-risk perception. 18 Another study using data from the same survey reported that the median county-level proportion of TNB adults who ever received an HIV test was 44%, and those who tested in the last year were 17%. 19 In contrast to previous findings, 18 HIV testing was highest among trans women, Black respondents, and persons 25 years or older. 19
In comparison, the Michigan Trans Health Survey data indicated that 26.2% of all participants had never received an HIV test, including 20.8% transfeminine, 30% transmasculine, 17.8% nonbinary assigned male at birth, and 32% nonbinary assigned female at birth individuals. 20 Moreover, a nationwide study of transgender youth found that only 15.1% had reported testing for HIV in the past year, whereas trans women were significantly less likely to test than their nonbinary and trans men counterparts. 21 The differences in these findings above underscore the need for further research on HIV testing in this population to better understand which TNI communities have the highest need for targeted interventions for HIV prevention, including HIV testing. A constant remains, however, that testing rates among TNI communities are far below the UNAIDS global target that 95% of all people living with HIV know their status by 2025. 22
Health care engagement among TNI individuals
Health care settings can serve as facilitators or barriers to health care engagement, including HIV testing, for TNI individuals. There are several identity-specific deterrents TNI individuals experience as they navigate health systems, including a lack of provider knowledge and cultural sensitivity. 23 Existing research found that experiences of anti-trans stigma and discrimination in health care settings were significant barriers to engaging in HIV preventative care.24,25 Conversely, experiences with TNI-competent providers and gender-affirming health care spaces are facilitators of health care access among TNI individuals. 26 Accordingly, previous studies have found that gender affirmation (i.e., the process of acknowledging and supporting a TNI person’s gender identity) is associated with greater involvement in the uptake of HIV prevention measures,27,28 including routine HIV testing. 29
Current study
Overall, there is a dearth of research reporting on HIV testing correlates and rates among TNI populations, including a lack of geographically specific data on HIV testing rates. Moreover, the majority of existing empirical work focusing on barriers and facilitators of health care access, including HIV preventative care, among TNI persons is qualitative. While this body of research is valuable for providing context around lived experiences, quantitative findings may generate additional support for existing qualitative work and provide a more robust argument for policymakers regarding TNI health needs, including gender-affirming care. This study contributes to the current knowledge base through a quantitative examination of differences in HIV testing among TNI people by gender and the identification of significant behavioral and health care-related predictors of HIV testing in this population.
Methods
Data source
This study is a secondary analysis of data collected in a 2022 Colorado-based cross-sectional survey of TNI adults. Participants were recruited in collaboration with Colorado’s premier LGBTQ+(lesbian, gay, bisexual, transgender, queer, and questioning) advocacy organization, [One Colorado]. A convenience sample was recruited through physical and digital distribution (e.g., email, social media posts) of flyers with a study description and survey link. Additionally, survey information was distributed through other state-based LGBTQ-focused organizations’ networks and at community gatherings. The data collection period extended from April through November 2022. The original study was approved by the University of Denver Institutional Review Board.
After data collection, a thorough data cleaning protocol was implemented to identify legitimate responses, particularly important given the increasing presence of automated programs designed to complete online questionnaires for compensation purposes (i.e., “bots”). 30 Data integrity preservation strategies included implementing CAPTCHAs, monitoring survey completion duration to remove submissions completed at implausible speeds for human respondents, and establishing a requirement that participants access the incentive survey only through the data collection instrument to prevent direct incentive access. Additionally, because incentive offerings heighten the risk of fraudulent participation, 31 supplementary verification methods were employed. Geographic coordinates were examined to exclude responses originating outside the project’s target region, while IP address analysis helped eliminate multiple submissions from identical sources. 32 The survey also incorporated attention verification items, instructing participants to select “strongly agree” as their response, 33 and requested age information in two different formats to identify inconsistent reporting. 34 Further verification involved examining open-ended responses for improbable duplicates or nonsensical content, as well as analyzing patterns in both survey metadata and structured question responses that might indicate duplicate entries. After removing participants who provided no responses beyond consent, the final analytical sample comprised 388 individuals.
Positionality
The authors of this study recognize the importance of articulating our positionality when engaging in research focused on the health of persons with marginalized identities, including diverse gender identities. Two members of the authorship team identify as nonbinary, two identify as cisgender men, and one identifies as a cisgender woman. To the authors’ knowledge, the original study team was comprised of three individuals who identify as nonbinary, one cisgender woman, and two cisgender men.
Measures
The study included two dependent variables: lifetime receipt of an HIV test and receipt of an HIV test in the past year. Lifetime receipt of an HIV test was measured with the question “Have you ever been tested for HIV (human immunodeficiency virus)?” Those who answered “Yes” to that question were asked “When were you last tested for HIV?” with response options of (1) “within the last 6 months,” (2) “more than 6 months ago by less than a year ago,” (3) “more than 1 year ago, but less than 3 years ago,” (4) “3 to 5 years ago,” or (5) “more than 5 years ago.” This variable was dichotomized for analysis, with those who responded with a 1 or a 2 considered to have received an HIV test in the last year and those who responded with a 3, 4, or 5 were considered to have not received an HIV test in the past year.
Independent variables for this study included gender identity, sexual orientation, race/ethnicity, HIV risk behaviors, refusal of transgender-related care by a doctor, experience of needing to educate a doctor about transgender-inclusive health care, and experience of a doctor not making assumptions about a participant’s sexual behaviors. Gender identity was measured with the question “How do you describe your current gender identity?” Response options included “agender,” “genderqueer,” “genderfluid,” “intersex,” “nonbinary,” “Two Spirit,” “transgender woman,” “transgender man,” “woman,” “man,” or “a gender identity not listed above (please specify).” In our analyses, these were collapsed into four categories: transfeminine (transgender woman/woman), transmasculine (transgender man/man), nonbinary (agender, genderqueer, genderfluid, nonbinary, Two Spirit), and intersex. We recognize that intersex is usually considered a sex, not a gender. However, since it was included as an option in the question asking for participants’ gender, we treated it as a gender category. Sexual orientation was measured with the question “How do you identify your sexual orientation?” and included response options of “asexual/aromantic,” “bisexual,” “gay,” “heterosexual/straight,” “lesbian,” “pansexual,” “queer,” “same-gender-loving,” or “a sexual orientation not listed above (please specify).” As with the gender identity variable, sexual orientation was recoded into three categories for the purpose of analysis. The three categories included gay/lesbian/same-gender-loving, heterosexual/straight, and bisexual/pansexual/queer. No participants who responded to the HIV testing questions identified as asexual/aromantic. Race/ethnicity was assessed with the question “What is your racial and/or ethnic identity?” with response options of “African American/Black,” “Alaskan Native/Inuit/First Nations,” “American Indian/Native American,” “Asian/Asian American,” “Latino/a/x or Hispanic,” “Middle Eastern,” “Native Hawaiian/Pacific Islander,” “White,” or “Biracial/Multi-racial/Multi-ethnic.” For analysis, participants who selected more than one response were coded as “Biracial/Multi-racial/Multi-ethnic.”
The HIV risk behavior variable was created by adding four dichotomous variables and had a possible range of 0–4. Participant HIV risk score included condomless anal or vaginal sex in the last year, STI diagnosis in the last year, multiple vaginal and/or anal sex partners in the last year, and sex while using drugs or alcohol in the last year, all measured as 1 = “yes” and 2 = “no.”
To determine whether or not a participant had been denied transition-related health care, they were asked to report whether a medical doctor or health care provider had refused to provide them transition-related health care, with response options of “yes, in the last year,” “yes, more than a year ago,” “no,” or “I have not sought these services.” Responses to this question were dichotomized into yes if they reported ever being refused this care and no if they either did not seek these services or were not denied care. We measured the experience of needing to educate a doctor about transgender-inclusive health care, with the question “Have you ever had to educate a doctor/medical provider on how to provide you inclusive health care?” with response options of “yes, one provider,” “yes, more than one provider,” “no,” or “not applicable.” This variable was also recoded for analysis so that 0 = “no” or “not applicable,” 1 = “one time,” and 2 = “more than one time.” The experience of a doctor not making assumptions about a participant’s sexual behavior was assessed by asking participants to indicate their level of agreement with the statement “my doctor/primary care physician does not make assumptions about my sex life” with Likert responses ranging from 1 “strongly disagree” to 5 “strongly agree.”
Data analysis
Descriptive statistics were used to describe sample demographics and HIV testing frequencies (see Table 1). Chi-square analyses and Fisher’s exact tests were conducted to test for significant associations between gender and lifetime and past-year HIV test receipt. Multi-variable logistic regression was used to examine relationships between independent variables and adjusted odds of lifetime and past-year HIV testing. We set our statistical significance level to the standard p < 0.05. Data were analyzed in Stata 18.0.
Participant Demographics (N = 388)
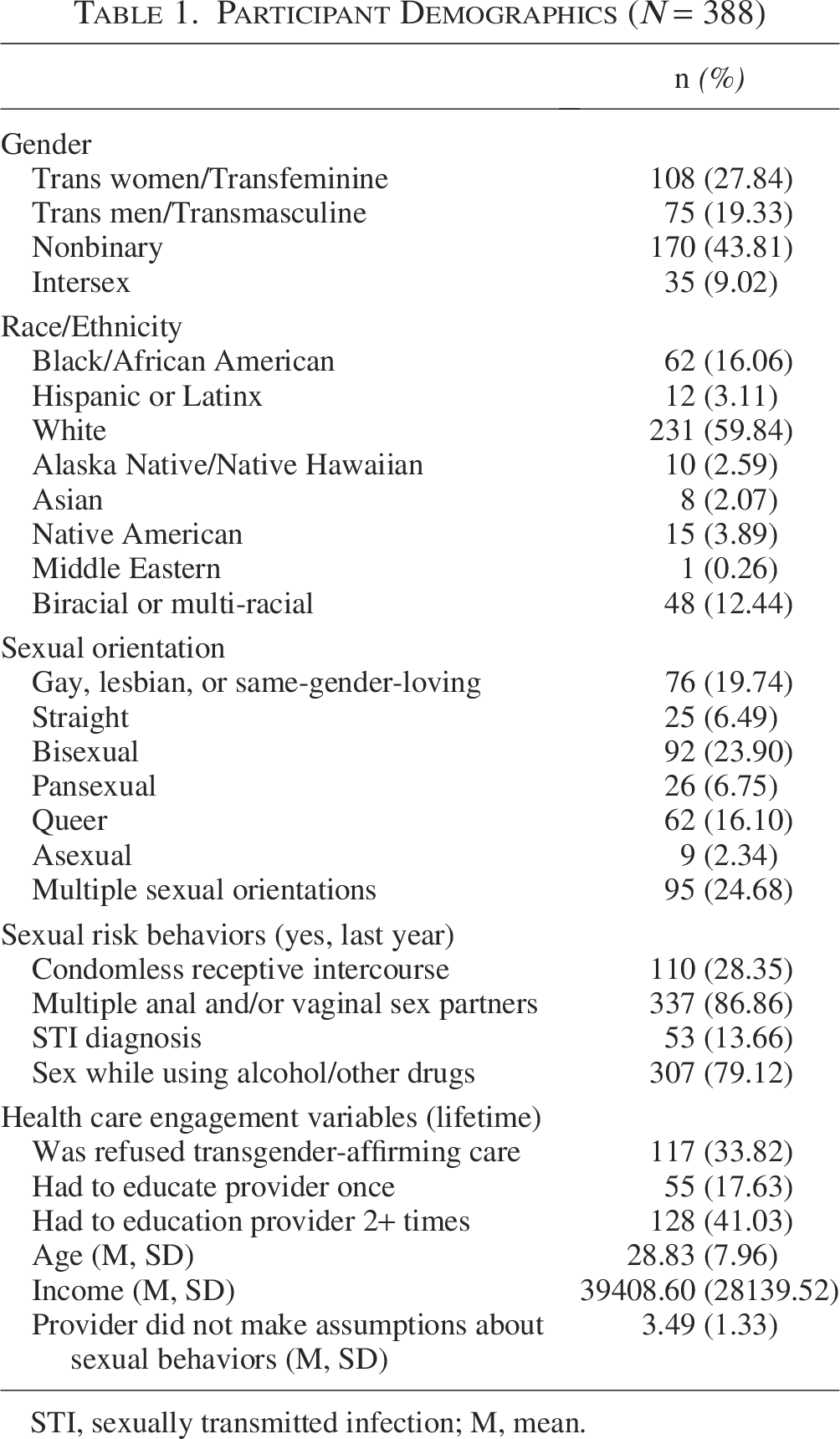
STI, sexually transmitted infection; M, mean.
Results
Slightly more than half of those who answered the question (54.15%, n = 176) reported ever receiving an HIV test. Of those who had ever been tested for HIV, 65.34% (n = 115) were tested for HIV in the past year. The frequency with which participants reported ever being tested for HIV mirrored sample composition, with the highest frequency among nonbinary individuals, followed by transfeminine, transmasculine, and intersex individuals. However, nearly the same number of nonbinary and transfeminine participants reported receiving an HIV test in the past year. Table 2 summarizes testing lifetime and past-year testing frequencies by gender.
Bivariate Associations Between Gender and HIV Testing (n = 325)
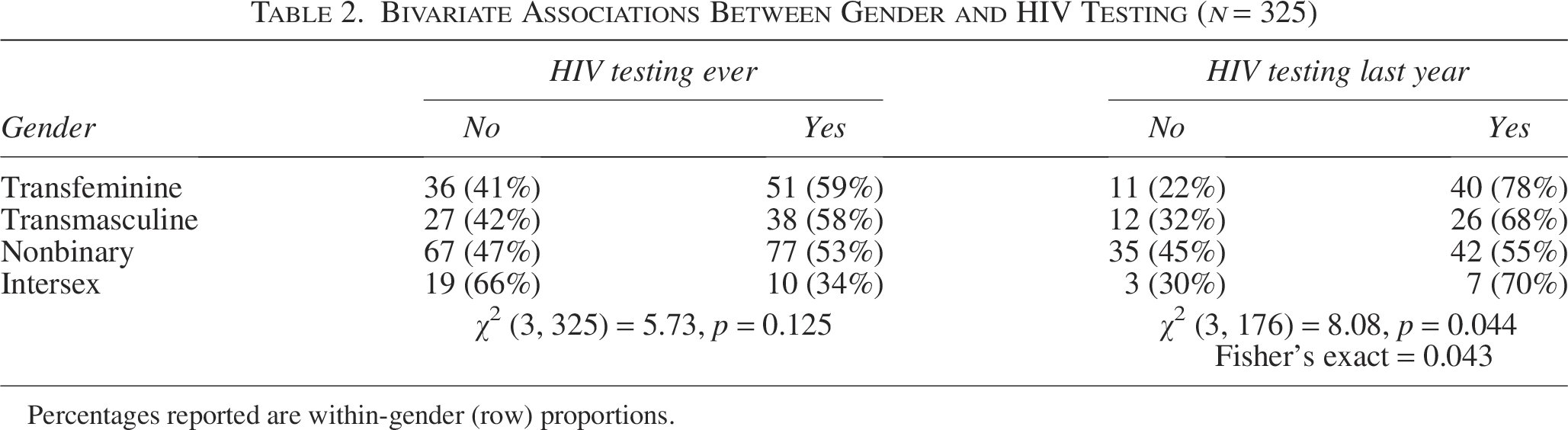
Percentages reported are within-gender (row) proportions.
Chi-square analysis indicated no significant differences in lifetime testing for HIV by gender (χ2 (3, 325 = 5.73, p = 0.13)). However, there was a significant difference in HIV testing in the last year by gender (χ2 (3, 176 = 8.08, p < 0.05; Fisher’s exact p = 0.04)). Among participants who had ever received an HIV test, slightly more than half (55%) of those who identified as nonbinary reported receiving a test within the last year, compared with 68% of transmasculine participants, 70% of intersex participants, and 78% of transfeminine participants.
Multiple logistic regression results of the model predicting likelihood of ever receiving an HIV test demonstrated that, controlling for all other variables in the model, those who had to educate health care providers once (AOR = 2.71, 95% CI: [1.29–5.69], p < 0.01) or more than once (AOR = 2.82, 95% CI: [1.56–5.07], p < 0.01) about providing transgender-related medical care were more than twice as likely to have ever been tested for HIV. Results also indicated that participants who self-identified as American Indian or Alaska Native were 86% less likely to have ever been tested for HIV than participants who identified as Black or African American. The model did not indicate a significant association between gender, sexual orientation, HIV risk, or lack of assumption of sexual behaviors from doctors and the likelihood of ever being tested for HIV.
The second multiple logistic regression model predicted HIV testing in the last year among individuals who reported ever receiving an HIV test. Controlling for all other variables in the model, those participants who identified as nonbinary were approximately 70% less likely to have received an HIV test than transfeminine participants (AOR = 0.30, 95% CI: [0.11–0.81], p < 0.05). In addition, those who identified as White (AOR = 0.16, 95% CI: [0.04–0.63], p < 0.01) or Biracial/Multiracial/Multiethnic (AOR = 0.17, 95% CI: [0.03–0.84], p < 0.05) were approximately 83–84% less likely to have received an HIV test in the past year compared with participants who identified as Black or African American. No other variables in the model were significantly associated with the likelihood of receiving an HIV test in the last year. Table 3 provides a summary of all logistic regression results.
Logistic Regression Predicting Odds of HIV Testing
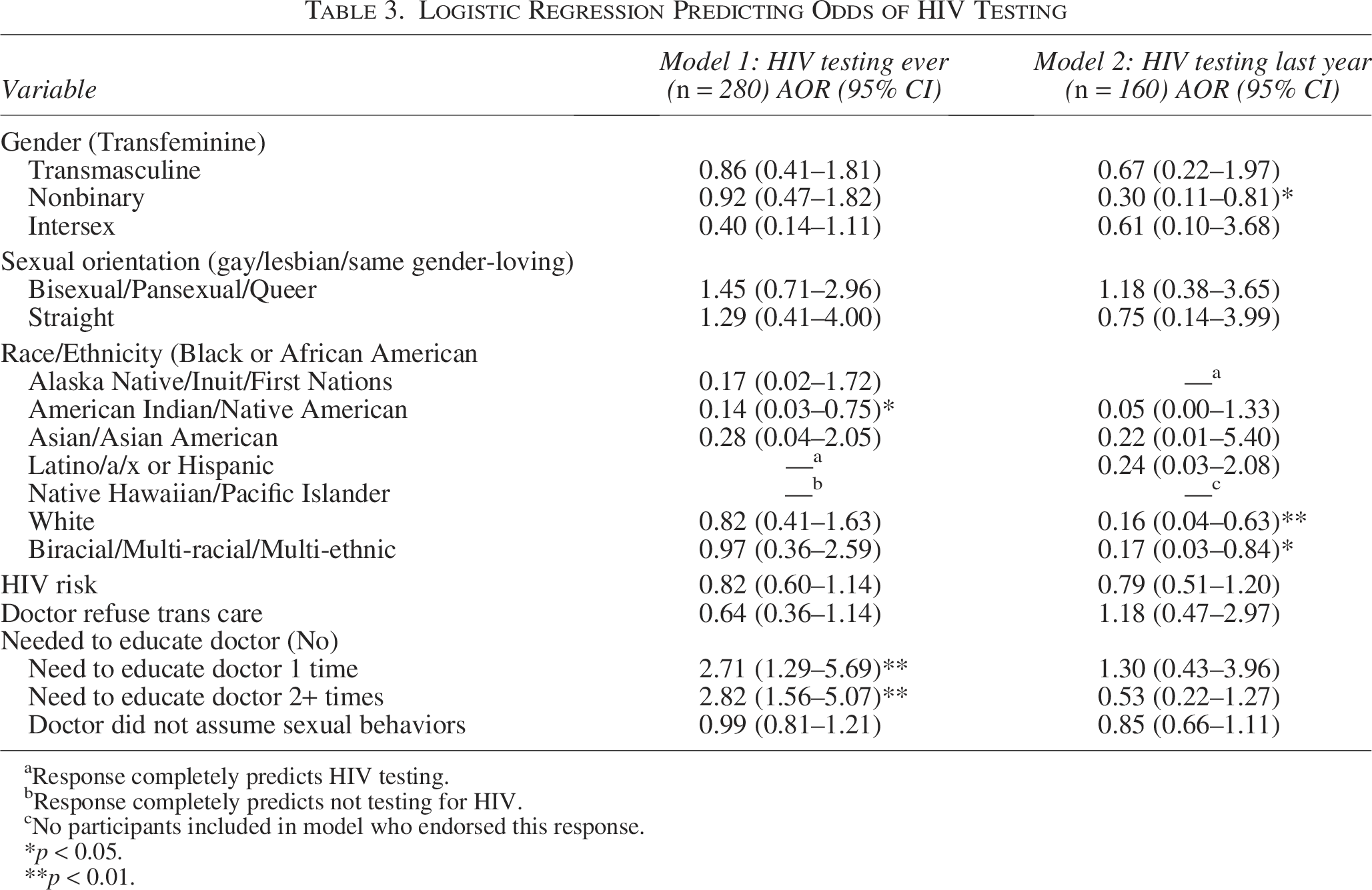
Response completely predicts HIV testing.
Response completely predicts not testing for HIV.
No participants included in model who endorsed this response.
p < 0.05.
p < 0.01.
We conducted post hoc chi-square analyses to elucidate the multiple logistic regression results. Regarding the results for the model predicting the likelihood of lifetime HIV testing, hypothesized that perhaps those participants who reported recent visits to medical providers were both more likely to have ever received an HIV test and to report having to educate their medical providers about inclusive care. To test this hypothesis, we first examined the relationship between seeing a medical provider in the last year and ever receiving an HIV test. A significantly greater proportion of those who reported seeing a medical provider in the last year also reported ever receiving an HIV test (66.5%) than those who did not see a medical provider (25%; χ2 (1, 317 = 46.77, p = 0.00)). We then examined the relationship between seeing a medical provider in the past year and reporting ever needing to educate a medical provider on inclusive care. We again found a significant relationship (χ2 (2, 304 = 15.59, p = 0.00)), where a greater proportion of participants who visited a medical provider in the past year reported ever needing to educate a medical provider on inclusive care (67%) than those who did not visit a provider in the past year (43%).
We also performed post hoc analysis to better understand our multi-variable logistic regression model, finding that nonbinary participants were significantly less likely to receive an HIV test in the last year. We hypothesized that fewer nonbinary individuals may have recently engaged in health care, especially gender-affirming care, during which an HIV test may have been offered, than their transfeminine counterparts. Results of post hoc chi-square analyses demonstrated significant differences in the proportion of participants who saw only a general medical provider (χ2 (3, 207 = 14.57, p = 0.002)) and only a gender-affirming medical provider (χ2 (3, 207 = 22.45, p = 0.000)) in the past year by gender. A great proportion of nonbinary participants (58%) reported seeing a general medical provider in the past year, when compared with transfeminine participants (27%). However, a smaller proportion of nonbinary participants (10%) reported seeing a provider for gender-affirming care in the past year when compared with transfeminine participants (43%).
Finally, we conducted a Fisher’s exact test to examine the significant differences in the likelihood of HIV testing by race/ethnicity demonstrated in both multi-variable logistic regression models. A cross-tab revealed that 60% of Black/African American participants, 38% of American Indian/Native American participants, 70% of White participants, and 74% of Biracial/Multi-racial/Multi-ethnic participants reported visiting a medical provider in the last year. However, these differences were not statistically significant according to Fisher’s exact test (p = 0.08).
Discussion
It has been previously established that TNI communities tend to report HIV testing rates lower than the UNAIDS target of 95%. The findings of our study further illuminate the low testing rates among TNI, with nearly half of our sample reporting not receiving an HIV test in their lifetime. Notably, our sample reported higher rates of lifetime testing than studies using the US Trans Survey (USTS).18,19 Contrarily, participants in the Michigan Trans Health Survey had higher rates of lifetime testing compared with our sample. 20 The higher rates of lifetime HIV testing reported by participants in the Michigan Trans Health Survey could be partially explained by the analytic sample in that study being limited to those who reported ever engaging in sexual activity in their lifetime. Still, the variation of lifetime testing prevalence across studies and samples suggests a potentially context-contingent nature of testing rates. As would be expected, past-year testing rates (n = 115) were lower than lifetime testing rates (n = 176) in our study. Collectively, our findings may suggest a gap in common knowledge about recommended HIV testing frequencies among TNI populations.
There was considerable variation across genders for both ever being tested or being tested in the last year for HIV, consistent with previous literature. 19 A greater proportion of transfeminine (59%, n = 51 out of 87), followed by transmasculine (58%, n = 38 out of 65), nonbinary (53%, n = 77 out of 144), and intersex (34%, n = 10 out of 29) individuals reported ever being tested for HIV. Our analysis supported no significant differences across gender for lifetime testing. The relatively high percentage of lifetime testing among transfeminine individuals in our sample is not congruent with previous research, which reports that transfeminine people often rank lower than most other subgroups in TNI communities within the context of HIV testing.18,20,21 However, a higher prevalence of HIV testing among trans women compared with TNI persons with other gender identities has been documented in a geographical examination of HIV testing prevalence using the 2015 USTS dataset. 19 Notably, Tordoff and colleagues 19 found that trans women were more likely to test for HIV in most EHE priority jurisdictions 35 but not all, pointing to the potential role of geography.
Additionally, among participants who had ever been tested for HIV, a high percentage of transfeminine (78%, n = 40 out of 51), followed by intersex (70%, n = 7 out of 10), transmasculine (68%, n = 26 out of 38), and nonbinary (54%, n = 42 out of 77) individuals reported being tested for HIV within the past year. Our analyses supported that there was a statistically significant variation across genders within the context of past-year HIV testing. One possible explanation for significantly lower rates of HIV testing in the last year among nonbinary participants is that significantly fewer nonbinary participants accessed gender-affirming care in the past year compared with transfeminine participants, a finding from our post hoc analyses. Previous studies have demonstrated that transgender individuals who engage in gender-affirming care are more likely to engage in regular HIV testing.20,36 It may be that gender-affirming care providers are more aware of increased HIV and STI risk for TNI individuals at a population level and so are more likely than general practitioners to offer HIV screening to their TNI patients. A second plausible explanation is that the lower prevalence of HIV testing among nonbinary individuals is indicative of lower perceived risk for HIV compared with transfeminine individuals.18,19 Together, these findings suggest that HIV testing and prevention messaging that targets TNI people who are not engaged in gender-affirming care, including nonbinary individuals, may be a key component to increasing regular HIV testing in this population. Moreover, general medical providers could help increase regular HIV testing in this population by offering HIV testing during medical visits.
Our findings also support the previously empirically established notion that identity-specific health care adversities impact HIV testing engagement. 37 Our findings painted a complex picture of how identity-specific adversities impact HIV testing uptake. Notably, we found that participants who had to educate either one or more than one provider on transgender-related medical care were more than twice as likely to have ever been tested for HIV. This finding might appear to contradict previous research underscoring the detrimental effect of knowledge gaps among providers. 38 However, the positive outcome of this adversity might be reflective of increased health care usage. Our post hoc analyses indicate that a significantly greater proportion of individuals who reported visiting a medical provider in the last year reported receiving an HIV test in their lifetime and needing to educate their medical provider in order to receive gender-affirming care. This suggests that the significant relationship between needing to educate one’s provider and lifetime HIV testing may be a function of regular access to health care and, perhaps, increased health literacy that TNI individuals often need to successfully navigate the US Health care system. This hypothesis could not be fully explored in the current study due to limitations in available data. However, this may be an important question to investigate in future research.
In addition to differences by gender and needing to educate one’s doctor, our findings indicated that participants who identified as American Indian/Native American, White, or Biracial/Multi-racial/Multi-ethnic were significantly less likely to engage in HIV testing when compared with their Black/African American counterparts. Unlike our post hoc tests for other findings, nonsignificant chi-square test results indicated that these findings could not be potentially explained by significant racial/ethnic differences in medical provider visits. However, similar to findings related to gender, the significantly higher likelihood for HIV testing among Black/African American TNI participants may be partially explained by greater perceived risk of HIV by participants and health care providers. Additional research with a larger sample size is needed at the intersection of race/ethnicity and gender to elucidate these findings and inform targeted HIV screening and prevention interventions.
The current study offers clarity on the lifetime HIV testing rates of TNI within the Colorado context. The findings suggest that more targeted and robust HIV prevention and intervention efforts can be beneficial in Colorado, especially for TNI communities. Based on the findings of the current study, in addition to extant literature on the topic, providers would likely benefit from continued education on how to address expectations of identity-based stigma and build rapport with TNI-identified patients. Also important to note, intersex participants in our sample reported the lowest frequency of ever having been tested for HIV. This finding must be interpreted with caution, as very little literature exists on HIV prevalence or testing patterns among intersex individuals. Most HIV research on gender-diverse populations has focused on trans women, with far fewer studies including intersex people as a distinct analytic group.10,39 Consequently, evidence-based recommendations for health care providers remain underdeveloped. Future research might benefit from exploring multi-level factors of health care influence among TNI populations. Prospective or otherwise longitudinal studies might offer unique perspectives to HIV testing uptake efforts.
The current study had many strengths. To our knowledge, the current study was the first to empirically examine rates of HIV testing among TNI communities in Colorado. As such, the findings of the current study have important policy implications. Our results demonstrate a need for increased governmental attention to the state, as rates of testing were found to be lower than national averages. For example, policies at both state and federal levels significantly impact access to HIV prevention services (and gender-affirming care) for TNI individuals. 39 Historical and recent legislative shifts, including bans on gender-affirming care and restrictions on trans-inclusive health care policies, exacerbate barriers to essential services.39,40 Addressing these systemic barriers is essential to improving HIV testing rates and ensuring equitable access to prevention and care for TNI populations. However, given the current US political climate, broad federal action may be unlikely in the near term. More immediate progress may come from provider-level strategies, including expanding continuing medical education on gender-affirming and HIV-related care and partnering with LGBTQ+ health centers to enhance provider competency and patient trust. 41
As with any study, the current study had several limitations. First, our findings are limited to Colorado and may not be generalizable beyond that context. Given data were collected via convenience sampling, the representativeness of the underlying sample may be limited. For example, only three individuals who identified as two-spirit completed the survey, and they were collapsed into the nonbinary category for analysis. Related, data were collected primarily online; TNI individuals who do not have access to required technological resources may be underrepresented. An additional limitation is the omission of sex assigned at birth from the data collection instrument. In the absence of that data, we were unable to perform analyses to examine differences in HIV testing by sex assigned at birth, which may be particularly relevant for the nonbinary and intersex participants in the study sample. Finally, due to the cross-sectional nature of the data, findings are associational, limiting any potential causal inferences.
The literature on gender differences in HIV testing in TNI population remains inconsistent, with some studies identifying lower testing rates among transfeminine individuals 21 while other studies finding the opposite.18,19 The high variation across TNI gender subgroups, paired with inconsistent findings across studies, point to complex sources of influence on TNI HIV testing rates. Despite plausible explanations discussed in this study and others, there remains a paucity of research on TNI HIV testing influences. Our findings underscore a pronounced need for continued empirical attention on the topic to inform strategies for increasing HIV testing in this population.
Authors’ Contributions
D.R.G.: Conceptualization, methodology, formal analysis, writing—original draft, project administration, and visualization. A.O.: Writing—original draft. C.S.: Writing—original draft. D.L.D.: Writing—original draft. T.M.: Writing—original draft.
Footnotes
Acknowledgment
The authors extend their gratitude to each participant who contributed data to the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by a grant from the University of Denver Public Good Fund.