
Abstract
Recent years have witnessed the unprecedented development and integration of genomics, epigenetics, transcriptomics, proteomics, and metabolomics, as well as a growing interest in novel single biomarkers and process-specific biomarker panels in human renal diseases. In a scenario currently dominated by kidney biopsy and established biomarkers such as serum creatinine, albuminuria, and proteinuria, novel biomarkers could potentially provide vital diagnostic and prognostic information and help to predict response to treatment in several clinical settings, including acute kidney injury, renal transplant, autosomal dominant polycystic kidney disease, and glomerulopathies. However, it is still uncertain whether and to what extent novel biomarkers will succeed in this difficult task. To date, they have generally failed to provide relevant information over and above what is already granted by established, cheap, and easily available biomarkers such as proteinuria, while the complexity and costs of these technology platforms are an important obstacle to their wide adoption. On the other hand, the successful implementation of anti–phospholipase A2 receptor antibodies as a diagnostic and prognostic biomarker of membranous nephropathy, as well as the huge number of ongoing collaborative efforts worldwide, should induce the nephrology community to be rather optimistic about a potential breakthrough in the management of kidney diseases over the next few decades.
Introduction: The Quest for Novel Biomarkers of Renal Disease
The availability of human genome data and novel technology advances in the fields of proteomics and metabolomics have fueled an impressive number of research projects that aim to identify biomarkers for different health issues, including renal diseases. Biomarkers could prove useful in achieving a timely diagnosis, providing prognostic information, monitoring disease progression, and predicting therapeutic response. This could be of particular relevance to nephrologists, as kidney biopsy—the current gold standard for several renal diseases—is invasive, associated with risks (particularly in patients with advanced renal insufficiency), 1 and sometimes unable to provide a clear-cut association between biopsy appearance and prognosis or response to therapy. 2 The need for novel and effective biomarkers is further exacerbated by the limitations of established biomarkers of renal disease, such as serum creatinine, albuminuria, and proteinuria. Glomerular filtration rate (GFR) measured by iohexol or iothalamate plasma clearance represents the gold standard for assessing true renal function but is unfortunately not routinely available because of the complexity and costs of measurement protocols. As a consequence, GFR is generally estimated via several creatinine-based equations, including the Cockcroft-Gault formula, the Modification of Diet in Renal Disease (MDRD) study equation, and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. 3 However, those formulas are unreliable and potentially misleading in a number of conditions that might deeply influence serum creatinine ( Table 1 ), as well as in common clinical scenarios, including acute kidney injury (AKI), 4 autosomal polycystic kidney disease (ADPKD), 5 and kidney transplant. 6 Similarly, although albuminuria and proteinuria have been associated with an increased risk of cardiovascular events 7 and end-stage renal disease (ESRD) 8 and represent a suitable surrogate biomarker in chronic kidney disease (CKD) patients, 9 the Food and Drug Administration (FDA) has generally not accepted effects on proteinuria as evidence of a drug’s effectiveness. 10
Commonly Used Methods for Clinical Assessment of Renal Function and Their Limitations.
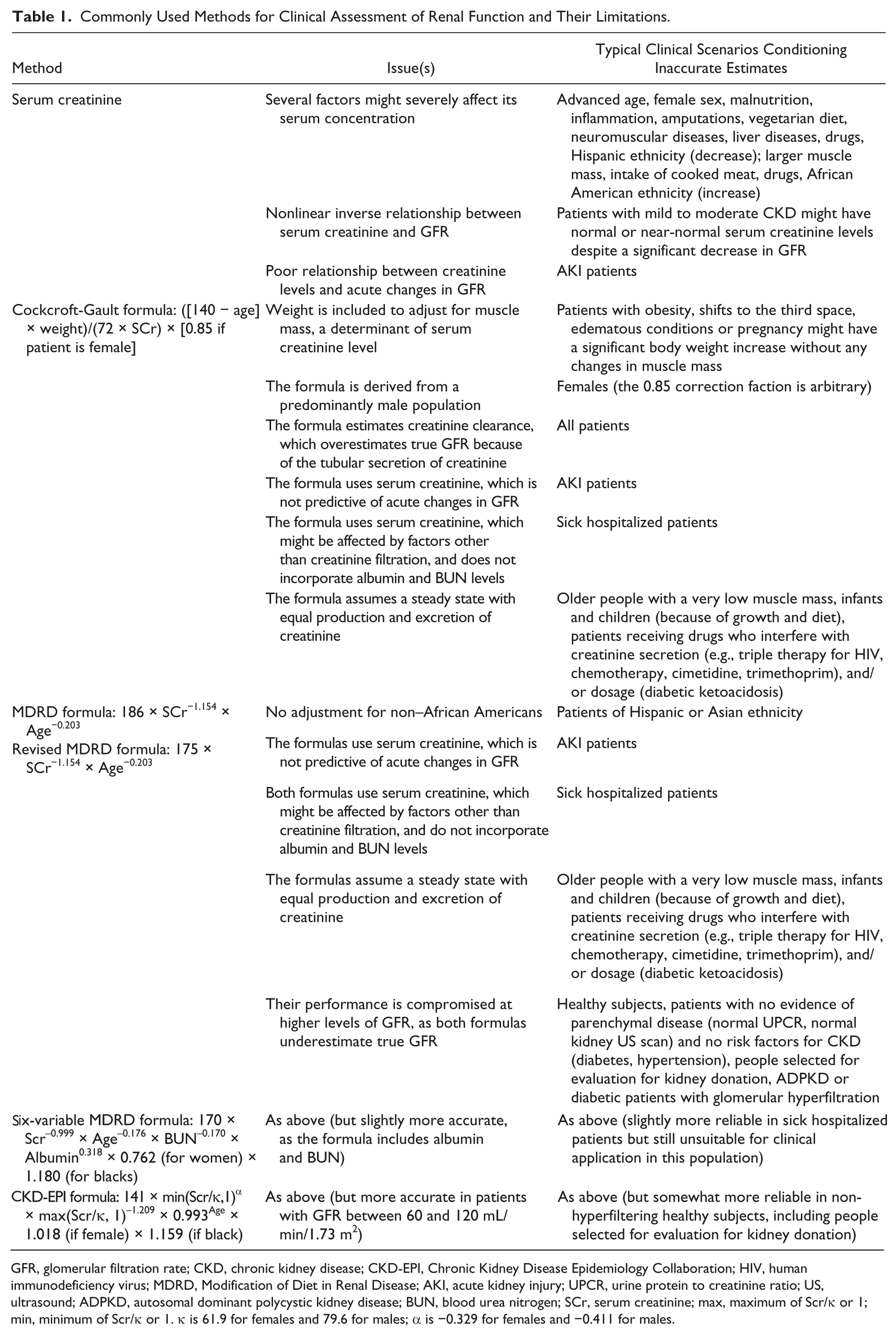
GFR, glomerular filtration rate; CKD, chronic kidney disease; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; HIV, human immunodeficiency virus; MDRD, Modification of Diet in Renal Disease; AKI, acute kidney injury; UPCR, urine protein to creatinine ratio; US, ultrasound; ADPKD, autosomal dominant polycystic kidney disease; BUN, blood urea nitrogen; SCr, serum creatinine; max, maximum of Scr/κ or 1; min, minimum of Scr/κ or 1. κ is 61.9 for females and 79.6 for males; α is −0.329 for females and −0.411 for males.
Several novel biomarker candidates are currently being evaluated in preclinical and clinical models to try to overcome the aforementioned limitations. Among the plethora of urinary and serum biomarkers, microRNAs (miRNAs) appear to be particularly promising. MiRNAs are small, noncoding RNAs that play a key role in multiple cellular functions, such as differentiation, replication, regeneration, and malignant transformation, by regulating protein levels posttranscriptionally. In sharp contrast with most RNAs, miRNAs are surprisingly stable, thus suggesting that secreted miRNAs are likely protected against RNase digestion. As a consequence, they are significantly increased in serum and other body fluids in a wide spectrum of diseases. 11 Apart from this desirable feature, circulating miRNAs can readily be detected by PCR and are relatively homogeneous, and the highly specific expression profile of most miRNAs could potentially make it possible to precisely monitor the health status of specific organs—possibly including the kidneys. Proteomic biomarkers also offer great hope for improving the current management of renal patients by achieving early detection and more accurate monitoring of several kidney conditions. 12 In fact, current proteomic tools enable thorough investigation of the human proteome, as recent advances in protein fractionation and labeling techniques are progressively making it possible to detect even the least abundant proteins. Furthermore, the field of proteomics has been enriched by analysis of posttranslational modifications and the possibility of comparing different proteomes. 13
Role of Novel Biomarkers in Human Renal Diseases
Despite the huge efforts in research, it is still unclear whether and to what extent novel serum and urinary biomarkers will be able to partly or completely replace kidney biopsy or “older” and established biomarkers and provide relevant and otherwise inaccessible information ( Table 2 ). The present review aims to provide an update on serum and urinary biomarkers encompassing a broad range of conditions, from CKD to kidney transplantation, that involve several hundred million people worldwide ( Fig. 1 ).
Established and Novel Biomarkers in Different Renal Diseases.
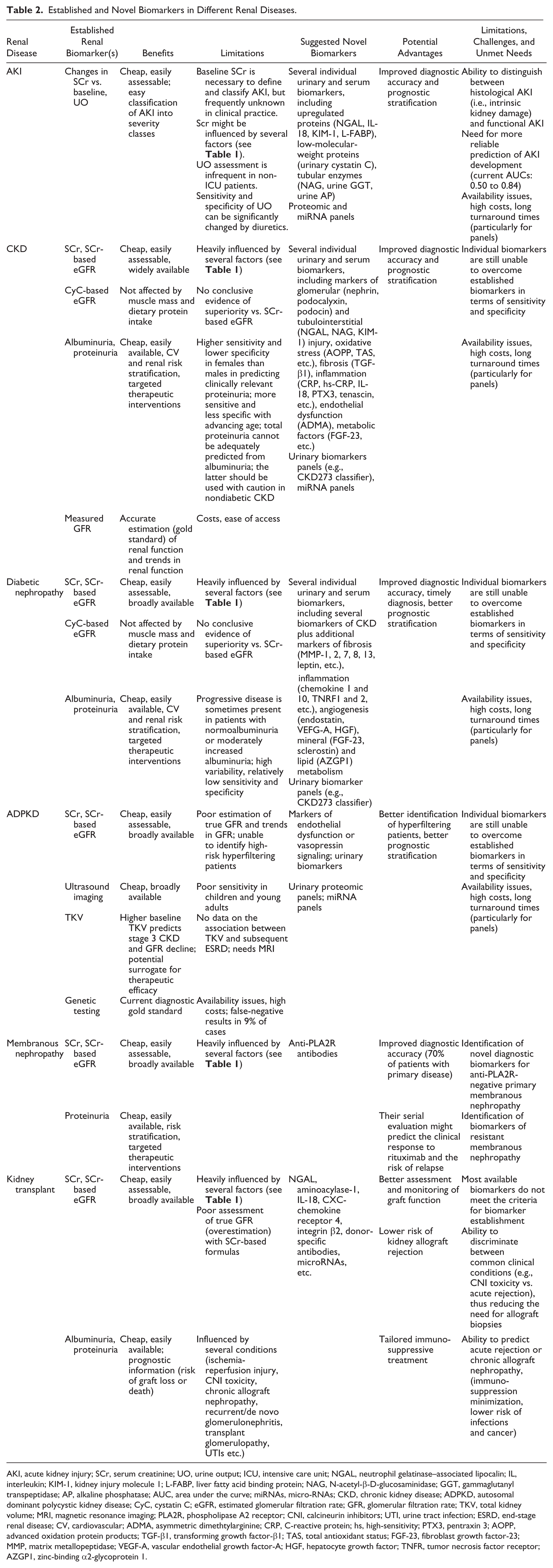
AKI, acute kidney injury; SCr, serum creatinine; UO, urine output; ICU, intensive care unit; NGAL, neutrophil gelatinase–associated lipocalin; IL, interleukin; KIM-1, kidney injury molecule 1; L-FABP, liver fatty acid binding protein; NAG, N-acetyl-β-D-glucosaminidase; GGT, gammaglutanyl transpeptidase; AP, alkaline phosphatase; AUC, area under the curve; miRNAs, micro-RNAs; CKD, chronic kidney disease; ADPKD, autosomal dominant polycystic kidney disease; CyC, cystatin C; eGFR, estimated glomerular filtration rate; GFR, glomerular filtration rate; TKV, total kidney volume; MRI, magnetic resonance imaging; PLA2R, phospholipase A2 receptor; CNI, calcineurin inhibitors; UTI, urine tract infection; ESRD, end-stage renal disease; CV, cardiovascular; ADMA, asymmetric dimethtylarginine; CRP, C-reactive protein; hs, high-sensitivity; PTX3, pentraxin 3; AOPP, advanced oxidation protein products; TGF-β1, transforming growth factor-β1; TAS, total antioxidant status; FGF-23, fibroblast growth factor-23; MMP, matrix metallopeptidase; VEGF-A, vascular endothelial growth factor-A; HGF, hepatocyte growth factor; TNFR, tumor necrosis factor receptor; AZGP1, zinc-binding α2-glycoprotein 1.
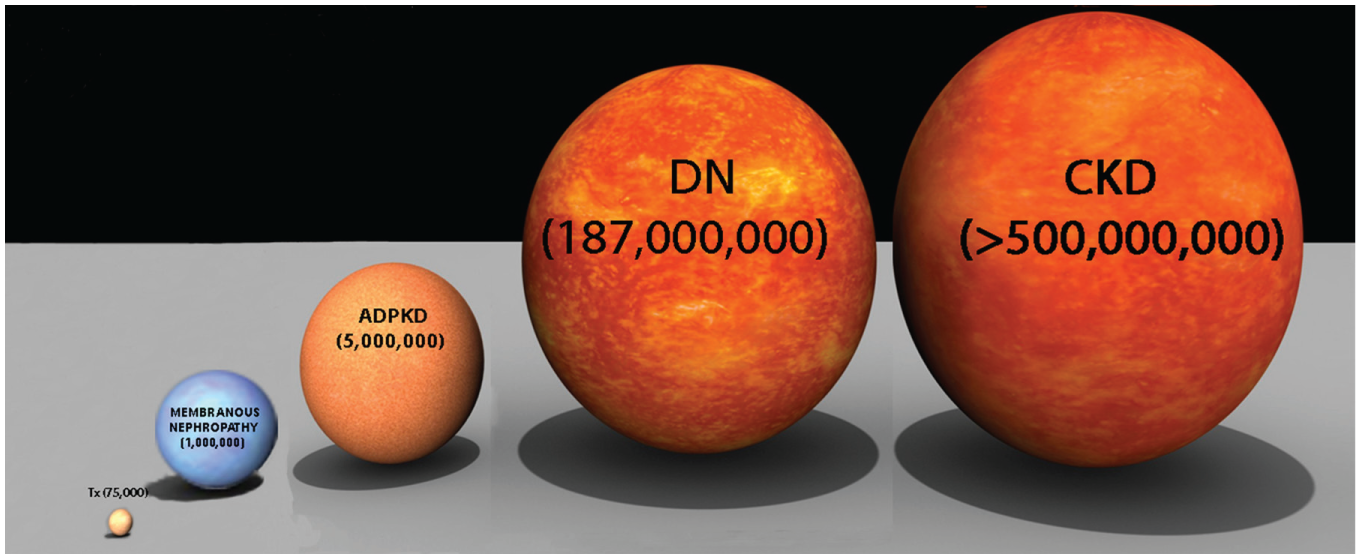
The constellation of renal diseases. Worldwide prevalence estimates for different renal diseases. CKD, chronic kidney disease; DN, diabetic nephropathy; ADPKD, autosomal dominant polycystic kidney disease; Tx, kidney transplant. Acute kidney injury is not included, as its occurrence is better described in terms of incidence: about 13.3 million cases every year (original file: https://upload.wikimedia.org/wikipedia/commons/c/cc/Star-sizes.jpg, modified under the terms of Wikimedia Commons, freely licensed media file repository).
{kind=link}
Acute Kidney Injury
AKI is a major public health issue worldwide, with an estimated 13.3 million cases every year. The burden is particularly high in developing countries, where the annual incidence is estimated to be 11.3 million cases. 14 It has been estimated that one of five adults and one of three children develop AKI during a hospital stay worldwide. 15 AKI has been associated with increased risk of short- and long-term mortality, CKD, and ESRD,16–18 even more evident in older patients or those with preexisting CKD. 19 In hospitalized patients, AKI requiring renal replacement therapy (RRT) doubles the long-term risk of mortality and causes a 28-fold increase in the risk of stage 4 to 5 CKD. 20 Moreover, even small increases in serum creatinine during hospital stays have been linked with significantly increased in-hospital mortality, increased length of hospitalization, and higher hospital costs. 21 In the United Kingdom alone, AKI affects between 262,000 and 1 million emergency hospital admissions per year, of which one in four will die, and costs the National Health Service (NHS) £434 to £620 million/year—more than it spends on breast, lung, and skin cancer combined. 22 Similarly, despite significant improvements in individual patient outcomes over the past two decades,23,24 AKI requiring RRT greatly increases the risk of in-hospital mortality in different clinical settings, including patients undergoing cardiovascular surgery 25 or admitted into intensive care units (ICUs). 26 In light of the above, several research groups have tried to identify serum and urinary biomarkers for diagnosis and the prognostic stratification of AKI. However, to date, biomarkers have failed to achieve any additional benefit compared to the traditional approach in clinical decision making. 27 A recent systematic review identified 87 studies on serum and urinary biomarkers of AKI, organized according to five clinical settings: emergency department, critically ill patients in the ICU, cardiac surgery, contrast-induced nephropathy, and pediatrics. The diagnostic and prognostic performance of the biomarkers was extremely heterogeneous, ranging from completely negative to over-optimistic. 27 This disappointing scenario might be explained by a number of issues, including the broad array of definitions of AKI, the widely different clinical settings, and the difficulty in making a distinction between histological AKI (i.e., intrinsic kidney damage) and functional AKI. In the ICU setting, some authors have also tried to improve the diagnostic and prognostic performance of biomarkers by using a panel of different biomarkers rather than individual ones. In particular, Metzger and coworkers 28 have tested the diagnostic accuracy of 20 urinary peptides in a blinded validation set of 20 ICU patients and 31 stem cell transplantation patients. The proteomic marker pattern was able to detect AKI up to 5 days prior to the increase in serum creatinine, compared to a number of individual markers of AKI, including neutrophil gelatinase–associated lipocalin (NGAL) and urinary kidney injury molecule (KIM-1, interleukin-18, and serum cystatin C). Unfortunately, availability issues, high costs, and long turnaround times are likely to outweigh any potential benefits from this panel. More recently, a pilot study investigated a set of miRNAs as potential biomarkers of AKI in ICU and post–cardiac surgery patients. The miRNA panel had a high diagnostic value, with the area under the curve (AUC) values between 0.9 and 1 at receiver operating characteristic (ROC) analysis, a discriminative power higher than any novel AKI biomarker. Although encouraging, these preliminary results need to be validated by large prospective cohort studies. 29 Finally, a number of novel biomarkers, such as KIM-1 and clusterin, are currently being investigated in human drug-induced AKI. In particular, urinary KIM-1 increases may be detected after exposure to several nephrotoxic agents, even in the absence of any changes in serum creatinine concentrations, and it has received regulatory endorsement as a sensitive biomarker of AKI during early drug development. 30
Chronic Kidney Disease
CKD is a complex spectrum of functional and structural changes that gradually progress to ESRD. According to the Kidney Disease Improving Global Outcomes (KDIGO) 2012 guidelines, CKD is defined by the presence of abnormalities of kidney structure or function for >3 months and classified based on cause, GFR category, and albuminuria category (CGA staging). 31 The rate of progression of CKD is extremely variable—from years to decades—and might largely be due to independent risk factors, including high blood pressure, proteinuria, and phosphate. 32 CKD affects 8% to 16% of the global population 33 and puts a huge burden on health care systems, due to increased cardiovascular morbidity and mortality, progression to ESRD requiring RRT, and CKD-associated complications such as anemia, 34 mineral bone disorder and fractures, 35 and cognitive decline. 36 As a consequence, there is a huge interest in identifying new serum and urinary biomarkers for the early diagnosis, prognosis, and management of CKD. To date, however, all novel individual biomarkers have failed to overcome more established biomarkers, such as serum creatinine or urinary albumin and protein. Despite their limitations,37–39 those “older” biomarkers are cheap, easy to assess, and almost universally available, thus representing the cornerstone of large-scale cardiorenal screening and management strategies, 40 as well as valuable surrogate end points for clinical trials. 9 On the other hand, a recently published study on 273 specific urinary peptides (CKD273 panel), including fragments of extracellular matrix and blood-derived proteins, showed a mild improvement in detecting and predicting progression of CKD compared to the combination of albuminuria and baseline eGFR (AUC = 0.831 vs. 0.758). 41 However, at present, these findings are insufficient for generating a new paradigm of renal function monitoring, given the constraints of the study design (cross-sectional), the limited mechanistic information, the unknown performance in older people, and the absence of data on hard renal end points, including ESRD. 42
Novel biomarkers are generally identified from experimental studies before investigation in clinical studies. As renal cells use a broad range of signaling pathways to regulate their activity, experimental studies have focused on different pathophysiological processes, including glomerular and tubulointerstitial injury, metabolic factors, endothelial dysfunction, oxidative stress, inflammation, and fibrosis.12,43 Among this extensive and ever growing list, a few compounds showed some promise as biomarkers of CKD progression—particularly serum and urinary NGAL 44 —or kidney function, CKD progression, and associated cardiovascular risk, particularly cystatin C.45,46 However, further qualification is needed in different and larger populations before any biomarkers can used in daily clinical practice. The prospective Canadian Study of Prediction of Death, Dialysis and Interim Cardiovascular Events (CanPREDDICT) is currently trying to provide new evidence of the association between several traditional biomarkers (eGFR, urine albumin creatinine ratio [uACR], hemoglobin, phosphate, and albumin) and novel biomarkers—asymmetric dimethylarginine (ADMA), N-terminal pro–brain natriuretic peptide (NT-pro-BNP), troponin I, cystatin C, high-sensitivity C-reactive protein (hsCRP), interleukin-6 (IL-6), and transforming growth factor β1 (TGFβ1)—and RRT, cardiovascular (CV) events, and death in CKD patients. This information could then be used to better understand biological variation in outcomes, to develop clinical prediction models, and to inform enrollment into interventional studies, which may lead to novel treatments. 47
ADPKD
ADPKD is an inherited systemic disorder that affects 12 million people worldwide and accounts for 8% to 10% of ESRD patients requiring RRT. 48 About 85% of patients carry germline mutations in the PKD1 gene, while PKD2 gene mutations have been reported in the remaining 15% of cases. 49 The hallmark phenotype of ADPKD is the progressive enlargement of both kidneys, caused by the sustained expansion of multiple cysts originating from any segment of the renal tubule, which gradually replace normal renal parenchyma.50–52 So far, clinical management of ADPKD has mainly focused on conservative therapies and treating complications. 53 As happened in other fields of nephrology, recent years have seen an extensive search for biomarkers that could play a diagnostic and prognostic role in ADPKD patients. Classically, ADPKD diagnosis relied on detecting cysts by ultrasound scan in patients with a family history of ADPKD. 54 Unfortunately, ultrasound imaging has poor sensitivity in children and young adults, particularly in the presence of PKD2 mutations. As a result, ADPKD cannot be excluded by renal ultrasound in patients younger than 30 years, and even genetic testing may be inconclusive, as screening of ADPKD patients fails to detect mutations in up to 9% of cases. 55 Higher baseline height-adjusted total kidney volume (TKV) may predict the onset of stage 3 CKD and GFR decline, but unfortunately there are no data on the association between TKV and the risk of ESRD. 56 In addition, the inverse association between GFR and kidney volume is greatly variable in individual ADPKD patients, thus limiting the role of GFR as a biomarker. 57 In this context, proteomic analysis of urine could play an important role in diagnosing and managing ADPKD by detecting multiple changes in the expression and processing of proteins. 58 In particular, a recent multicentric study characterized the urinary peptidomic pattern of subjects with relatively early stages of ADPKD. In total, 657 peptides with significantly altered excretion were identified, of which 209 could be sequenced by tandem mass spectrometry. A diagnostic biomarker model based on the 142 most consistent peptide markers achieved a sensitivity of 84.5% and a specificity of 94.2% in an independent validation cohort of 251 ADPKD patients from five centers and 86 healthy controls. 59 In addition, the authors were able to identify a number of biomarkers for disease severity and progression and to develop a proteomic severity score that aimed to predict height-adjusted total kidney volume (htKTV). However, the diagnostic biomarker model showed lower sensitivity in young patients and in patients with the PKD2 genotype, a limit shared with ultrasound imaging. Thus, unfortunately, the usefulness of this biomarker approach in daily clinical practice is questionable, as renal ultrasound scan is very accurate in patients with the PKD1 genotype aged 30 years or older and certainly more easily available and less costly. Other authors have tried a different approach by profiling urinary microRNAs in 20 ADPKD patients and 20 matched CKD patients, in an attempt to identify suitable biomarkers of ADPKD progression. 60 Interestingly, several specific microRNAs in cellular and extracellular (exosome) specimens were present only in ADPKD patients. In particular, the authors hypothesized that decreased levels of mir-1(4) and mir-133b(2) might play a role in the pathogenesis of ADPKD, thus making them potential biomarkers for disease progression and therapeutic response. However, large-scale prospective studies are needed to corroborate these preliminary findings.
Podocytopathies
The glomerulus is the functional unit of the kidney that produces the ultrafiltrate from the afferent blood flow, and it is a selective filter that ultimately determines which compounds will be further processed throughout the nephron. Traditionally, the glomerular filtration barrier has been described as a three-layer structure: the capillary endothelium, the glomerular basement membrane (GBM), and the visceral epithelium, made up by podocytes, terminally differentiated cells whose foot processes encircle the GBM. More recently, a large number of experimental studies highlighted the importance of at least two additional layers, the endothelial surface layer 61 and the subpodocyte space, 62 as well as the key role of podocytes as both the regulators of glomerular development and the determinants of proteinuria and progressive glomerulosclerosis. 63 Unsurprisingly, a large number of urinary biomarkers of podocyte injury have been investigated so far, including proteins (synaptopodin, podocin, podocalyxin, nephrin, mindin, CD59, CD80, complement receptor 1, glomerular epithelial protein 1, etc.), podocyte-specific mRNAs, the exosomal transcription factor WT1, and podocalyxin-positive granular structures. 64 In addition, slit diaphragm proteins have been suggested as potential biomarkers given their important role in regulating both podocyte function and structure, through complex interplay with the podocyte actin network.65–67 All the aforementioned biomarkers, however, need further evaluation in large clinical studies.
Diabetic Nephropathy
Diabetic nephropathy, one the most feared long-term complications of diabetes mellitus, is heralded by the persistence of moderately increased albuminuria (formerly called microalbuminuria; albumin excretion rate: 30–300 mg/24 h; albumin-to-creatinine ratio: 30–300 mg/g). 68 The subsequent development of severely increased albuminuria (formerly called macroalbuminuria; albumin excretion rate >300 mg/24 h or albumin-to-creatinine ratio >300 mg/g) 68 is typically paralleled by a progressive decline in GFR, which eventually results in the development of ESRD. Diabetic nephropathy is still the leading cause of ESRD requiring RRT in most of the wealthiest countries countries, including the United States, European Union, and Japan,69,70 despite a trend toward incidence stabilization that is not evident in poorer countries.71,72 Diabetic nephropathy occurs in 25% to 40% of diabetic patients within 20 to 25 years of disease and often coexists with some degree of diabetic retinopathy, 73 the leading cause of legal blindness, 74 and a staggering increase in CV morbidity and mortality, 75 to the point that most patients with diabetic nephropathy will die of CV diseases before progressing to ESRD.76,77 The increased risk of renal and CV complications eventually results in a hefty socioeconomic burden, particularly in specific ethnic groups 78 and in low- or middle-income countries, where most ESRD patients do not have access to RRT. 79
As a result, timely diagnosis and early therapeutic intervention might halt or significantly slow the progression of diabetic nephropathy toward ESRD and ensure substantial socioeconomic benefits, particularly in developing countries and newly industrialized countries, such as China and India. 80 In addition, albuminuria is a nonspecific marker, as it may increase in other kidney diseases, such as hypertensive nephrosclerosis 81 and interstitial nephritis, 82 as well as in other common diseases, such as congestive heart failure.83,84 Finally, the slope of renal function decline in diabetic nephropathy is not always proportional to the progression in albuminuria.85,86 Thus, there is an unmet need for a novel biomarker that might allow early detection of diabetic nephropathy with higher accuracy and better prognostic evaluation.
In this regard, urinary biomarkers are particularly attractive, as a large volume of urine can be collected noninvasively. A large number of urinary compounds have been investigated, including urinary microRNAs, 87 exosomes, 88 and markers of epithelial-mesenchymal transition,89,90 tubulointerstitial damage,91–93 increased glomerular permeability,94,95 extracellular matrix,96–98 and podocyte damage.99,100 To date, none of those urinary biomarkers have been shown to be equal or superior to the current gold standard of moderately increased albuminuria. Despite this, the future implementation of a urinary proteomic-based classifier might potentially enable the timely identification of early stages of diabetic nephropathy, even before the onset of moderately increased albuminuria.101–103 In particular, the PRIORITY (Proteomic prediction and Renin angiotensin aldosterone system Inhibition prevention Of early DN In TYpe 2 diabetic patients with normoalbuminuria) trial is currently evaluating the usefulness of a urinary peptide-based classifier composed of 273 different urinary peptides (CKD273) for detecting individuals at high risk of developing diabetic nephropathy. 104 Among serum biomarkers, cystatin C, 105 fibroblast growth factor (FGF)–21, 106 FGF-23, 107 and soluble tumor necrosis factor receptors 108 have been recommended as novel biomarkers for predicting the progression of diabetic nephropathy but need to be validated by large-scale studies.
Membranous Nephropathy
Primary (“idiopathic”) membranous nephropathy (MN) is the leading cause of nephrotic syndrome in white adults, is more common in men than in women, and is most commonly diagnosed during the fourth or fifth decade of life. 109 Primary MN is a chronic disease, characterized by spontaneous remissions—particularly during the first 2 years after onset—and relapses. At 8 years, about 25% of patients reach ESRD requiring RRT; furthermore, nephrotic patients who do not progress toward ESRD have a higher risk of developing CV events. For patients with primary MN, anti–phospholipase A2 receptor (PLA2R) antibodies are a promising diagnostic 110 and prognostic 111 biomarker. These nephritogenic antibodies bind to a 180-kDa M-type transmembrane phospholipase A2 receptor located on podocytes. Anti-PLA2R antibodies are present in about 70% of adult patients with primary MN, 110 making them a powerful tool for differentiating between primary and secondary MN and monitoring disease activity and response to therapy. 112 In addition, familiar clustering of primary MN has been described in different ethnicities, including Caucasians113,114 and Asians, 115 and has been taken to suggest that genetic factors may play a role in the production of anti-PLA2R antibodies. In light of this, a recent study aimed to investigate the relationship between treatment effect, anti-PLA2R antibodies, and genetic polymorphisms in 132 consecutive patients with primary MN and persistent nephritic syndrome, treated with the anti-CD20 monoclonal antibody rituximab. Among the 81 patients with anti-PLA2R antibodies, lower anti-PLA2R antibody titer at baseline and full antibody depletion at 6 months after rituximab strongly predicted remission over a median follow-up of 30.8 months. Notably, all 25 complete remissions were preceded by full anti-PLA2R antibody depletion. Those findings strongly suggest that serial evaluation of circulating anti-PLA2R antibodies might help to predict both the clinical response to rituximab and the risk of relapse in patients with primary MN and longstanding nephrotic syndrome. 111 In patients with primary MN, urinary biomarkers have no clear prognostic value because of the poor sensitivity and specificity, the small sample size of the studies, and the lack of adequately powered qualification studies.116–121
Other Glomerular Diseases
In immunoglobulin A (IgA) nephropathy, both serum galactose-deficient IgA1 (Gd-IgA1) 122 and antiglycan antibodies targeting the hinge region of Gd-IgA1 123 have been suggested as diagnostic and prognostic124,125 biomarkers. However, family studies showed that a number of asymptomatic relatives of IgA nephropathy patients might have elevated levels of Gd-IgA1 in the absence of any renal involvement, consistent with the hypothesis that the abnormal O-glycosylation of the IgA1 “first hit” is not sufficient per se to induce IgA nephropathy. 126 Moreover, other studies failed to confirm any association between serum Gd-IgA1 and the magnitude of proteinuria in children with IgA nephropathy. 127 Thus, further studies are needed to evaluate whether and to what extent a combination of serum Gd-IgA1 and antiglycan antibodies—a likely candidate for the “second hit” 123 —plays any diagnostic or prognostic role in IgA nephropathy. To date, no urinary biomarkers showed any clinical applicability in IgA nephropathy, despite the use of novel approaches such as urinary RNA profiling 128 and the extensive study of several compounds, including urinary markers of complement activation129,130 and urinary IgA1-containing immune complexes. 131
Focal segmental glomerulosclerosis (FSGS) should not be viewed as a single disease but rather as a histologic pattern of renal damage that initially affects the glomerulus and the tubulointerstitium. 132 The hallmark of primary (idiopathic) FSGS is podocyte injury, while secondary FSGS might occur as a result of genetic mutations, viral infections, drugs, reduced renal mass, hypertension, and obesity. 133 At least in some cases, FSGS might be caused by a circulating permeability factor; among several candidate molecules, the soluble urokinase receptor (suPAR) recently emerged as a promising diagnostic biomarker, as suPAR is increased in about two-thirds of patients with primary FSGS. 134 In addition, high suPAR levels before transplantation have been associated with an increased risk of FSGS relapse after transplant. Finally, suPAR might play a prognostic role, as a reduction in circulating suPAR after immunosuppressive treatment could be predictive of proteinuria reduction and complete remission.135,136 Unfortunately, suPAR has poor overall sensitivity in secondary FSGS and might be normal in one-third of subjects with primary FSGS or even more—up to 45%. In addition, a nonspecific increase in suPAR might occur in advanced CKD, ESRD, proinflammatory states, and malignancies.137,138 Thus, current assays—including those using urinary biomarkers 139 —cannot be recommended for daily clinical practice. More recently, the levels of urinary microRNAs (miR196a, miR-30a-5p, and miR-490) were found to be increased in active FSGS but not in healthy controls or in patients with FSGS in remission. In addition, after steroid treatment, their levels were lower in steroid-responsive patients but remained unchanged in steroid-resistant patients. 140 Unfortunately, the decrease in urinary microRNAs was paralleled by a reduction in proteinuria, so these novel urinary biomarkers failed to achieve any advantage over this “older” but cheap and easily accessible biomarker.
In lupus nephritis, putative prognostic biomarkers141–145 failed to precede the onset of proteinuria, thus resulting in confirmation rather than prediction of damage.
Kidney Transplantation
Kidney transplant is the most desired and cost-effective RRT modality for ESRD patients. However, despite significant advances in surgical techniques and postoperative care over recent decades, and even though kidney transplants unequivocally offer the best survival and quality of life for successful candidates across all demographic groups, broad applicability has been limited by a relative shortage of available organs, graft rejection, and side effects of immunosuppressant drugs. 146 In principle, effective implementation of biomarkers could enable better assessment and monitoring of graft function, minimize the risk of kidney allograft rejection, and allow tailored immunosuppressive therapy in kidney transplant recipients. 147 Unfortunately, despite the identification of several putative biomarkers, including NGAL,148,149 aminoacylase-1, 150 interleukin-18, 151 CXC-chemokine receptor 4, chemokine (C-C motif) ligand 5, integrin β2, 152 donor-specific antibodies, 153 and microRNAs,154,155 most data from experimental and clinical studies failed to be translated into daily clinical practice. This unsatisfactory scenario might partly be explained by the short follow-up times and the lack of reliable end points in qualification studies. For example, although numerous formulas have been developed to estimate renal function from biochemical, demographic, and anthropometric data, prediction equations do not allow a rigorous assessment of renal function in kidney transplant recipients. In a group of 81 renal transplant recipients enrolled in the Mycophenolate Mofetil Steroid Sparing (MYSS) trial, 12 different prediction equations were carried out in all patients at months 6, 9, and 21 after surgery and compared with GFR measurement by plasma iohexol clearance as the reference method. All equations showed a tendency toward GFR overestimation; moreover, a significantly higher rate of GFR decline, ranging from −5.0 to − 7.4 mL/min/1.73 m2/y, was estimated by all the equations compared to iohexol clearance (−3.0 mL/min/1.73 m2/y). 6 Along the same lines, the intrinsic variability in synthesis or tubular secretion of serum creatinine makes it a poor marker of true renal function in the transplant setting. 156 An additional issue is that most of the compounds proposed as biomarkers in human renal transplantation do not fully meet the criteria for biomarker establishment, including evaluation in an independent set of samples; appraisal in different clinical settings to allow the identification of sensitivity, specificity, and negative and positive predictive values; and the assessment of interpatient variability and reproducibility. 157
In conclusion, the broad use of genomics, epigenetics, transcriptomics, proteomics, and metabolomics will probably translate into a major breakthrough in the management of kidney diseases over the next decades. At the moment, however, the complexity and costs of these technology platforms represent formidable obstacles to their usage in everyday clinical practice. Thus, we concur with De Vriese and Fervenza 2 that, with the exception of serum anti-PLA2R antibodies in most cases of primary membranous nephropathy, novel biomarkers have no additional value compared to conventional ones such as creatinine, albuminuria, and proteinuria. This scenario is likely justified by the fact that until recently, several research groups have focused their efforts on single serum or urinary biomarkers rather than a combination of different biomarkers. Indeed, any single biomarker of disease will always be hindered by the high degree of intra- and interpatient variability in each specific disease and each sample type, 158 especially in urine, wherein the intraindividual reproducibility of the results during the day might be as low as 70%. 159 On the other hand, a combination of biomarkers could be more robust and specific 160 and potentially lead to the generation of different diagnostic, prognostic, or therapeutic response patterns. In support of this statement, albeit preliminary, the recently suggested diagnostic accuracy of a miRNA set in AKI patients highlights that the use of biomarker panels is probably the right way forward. 29 Finally, there is an unmet need for novel and broad data integration approaches that might effectively deal with the large amount of information generated by the “omics” tools, improve the comparability of study results across different populations, and confirm or reject findings across studies. 161 This crucial step in biomarker discovery becomes even more apparent in light of the fact that many of the available studies have been performed in small patient groups, thus resulting in a poor degree of overlap between proposed biomarkers among different studies. The large amount, complexity, and heterogeneity of data have led several research groups to create multicentric consortiums for qualifying serum and urinary biomarkers. For example, in the recent Clinical Trials in Organ Transplantation-01, a multicenter observational study in 280 adult and pediatric renal transplant recipients, low urinary CXCL9 protein at 6-month follow-up identified the individuals least likely to develop future acute rejection or a decrement in estimated GFR between 6 and 24 months posttransplant from urine obtained from stable allograft recipients.162,163 The NEFRONA project is currently recruiting over 2000 CKD patients into a prospective observational study aimed at investigating the relationship between biomarkers, cardiovascular events, and mortality, 164 while the Canadian Study of Prediction of Risk and Evolution to Dialysis, Death and Interim cardiovascular Events Over Time (CaNPREDDICT) is assessing a number of biomarkers in about 2500 patients with moderate to advanced CKD over a 36-month follow-up period. 165 Moreover, the Nephrotic Syndrome Study Network (NEPTUNE), the CureGN prospective cohort study, the EURenOmics study, the UK registry for rare renal diseases (RADAR), and the European Renal cDNA bank are studying several biomarkers in patients with different glomerular diseases. 166 We hope that all of those collaborative projects will eventually succeed in qualifying novel and effective diagnostic, prognostic, and therapeutic response biomarkers for kidney diseases—hopefully in a few years.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.