
Abstract
Drug repositioning or repurposing has received much coverage in the scientific literature in recent years and has been responsible for the generation of both new intellectual property and investigational new drug submissions. The literature indicates a significant trend toward the use of computational- or informatics-based methods for generating initial repositioning hypotheses, followed by focused assessment of biological activity in phenotypic assays. Another viable method for drug repositioning is in vitro screening of known drugs or drug-like molecules, initially in disease-relevant phenotypic assays, to identify and validate candidates for repositioning. This approach can use large compound libraries or can focus on subsets of known drugs or drug-like molecules. In this short review, we focus on ways to generate and validate repositioning candidates in disease-related in vitro and phenotypic assays, and we discuss specific examples of this approach as applied to a variety of disease areas. We propose that in vitro screens offer several advantages over biochemical or in vivo methods as a starting point for drug repositioning.
Introduction
An Introduction to Drug Repositioning
Drug repositioning, drug repurposing, and new indication finding are common terms used to describe the process of generating additional clinical opportunities from pre-approval drug candidates, as well as the identification of further commercial opportunities for already marketed medicines (often after the original composition of matter patent has expired and where a new use can be exploited 1 ). Repositioning has been common practice in the pharmaceutical industry, which has traditionally explored the potential of new candidate drugs in other disease areas, through internal networking and the availability of disease-related phenotypic assays; 2 drug repositioning is by no means a recent invention. 3 There are many well-known examples of drugs, either in development or on the market, being switched to new indications based on information gained from clinical observation [e.g., sildenafil (Viagra)] or accumulated understanding of the mechanism of action [e.g., thalidomide (Thalomid)].
Drug repositioning has also recently seen a number of high-profile initiatives seeking to identify new therapeutic areas for existing drugs. Many of these have been driven by academic and not-for-profit organizations or in partnership with pharmaceutical companies, and as a response to the relative lack of new drugs being launched onto the market. Recent examples include the National Institutes of Health–National Center for Advancing Translational Sciences (NIH-NCATS)4,5 and AstraZeneca–MRC collaborations, 6 which combine grant funding to academic researchers for novel, competitive, research proposals to study the potential of clinical compounds provided by pharmaceutical companies in new disease indications. These initiatives have also been paralleled by the availability of clinical compound and drug-like molecule collections such as the NIH and Johns Hopkins clinical collections (see below). Independently of these initiatives, pharmaceutical companies such as Lilly and AstraZeneca are also making their compound libraries and assays available to the wider scientific community through open innovation (see, e.g., www.openinnovation.lilly.com and www.openinnovation.astrazeneca.com).7,8 The aims of these initiatives are twofold: first, a greater understanding of disease mechanisms via the application of clinically experienced compounds in new disease settings; and, second, the identification of new clinical uses for these compounds, which could then be developed for patient benefit more rapidly than a traditional new chemical entity (NCE).
Is There a Business Case for Drug Repositioning?
The global pharmaceutical industry is becoming more focused on a smaller number of disease areas. For example, many companies have stopped, or significantly restructured, in-house research into psychiatric disorders. 9 This focus on a smaller number of core disease areas is combined with the growth of bio-therapeutics and the advent of new approaches such as regenerative medicine. There has also been a drive toward maximizing existing medicines through line extensions or other means of life cycle management. 10 As a consequence, the breadth of disease-associated phenotypic assays available in house has reduced. Since the late 1990s and early 2000s, the industry has also seen the advent of more targeted approaches to candidate selection. The narrowing of disease area focus, combined with the tendency for research activities to occur in geographically dispersed groups, means that opportunities for in-house asset sharing may be diminishing and that there may be less active repositioning into noncore areas of unmet medical need. Systematic, and perhaps costly, organizationally complex, or time-consuming in-house drug-repositioning programs might not be supported. Thus, it is likely that more NCEs may enter clinical testing without a wider understanding of their possible utility in other disease areas.
However, this may increase the opportunity for organizations with different commercial models or disease area interests, and with access to a potentially wider portfolio of compounds, to benefit from drug repositioning. 11 In our view, from the standpoint of value generation, drug repositioning is now perhaps best suited to small and medium-sized enterprises (SMEs), not-for-profit organizations, and academic groups. Drug repositioning may also be of value in rapidly identifying clinically proven molecules that can be used in the context of personalized medicine. 12 SMEs and not-for-profit organizations may have narrow disease area interests or specific technologies, such as reformulation, that form the basis of their future intellectual property, but they are perhaps less constrained with the source of the compound. They are able to access and test a range of assets available off the shelf from commercial vendors, from Pharma partners, or through libraries compiled by, for example, the NIH (www.nihclinicalcollection.com). In the recent drug-repositioning literature, there have been numerous publications related to indications that were once part of large Pharma disease areas, such as neuroscience, as well as significant efforts in neglected, tropical, and rare and orphan disease spaces (see examples below). In addition, there have been considerable efforts by not-for-profit organizations and by government funding bodies to incentivize the identification and development of new therapeutics. Finally, large Pharma are becoming more interested in opening up their compound libraries to external parties. 8 For these reasons, drug repositioning today may be a highly attractive proposition from both a scientific/unmet-medical-need perspective as well as a commercial standpoint.
Compounds for Drug Repositioning
The assessment of compounds for use in a new disease can occur across the pharmaceutical value chain, from before a compound is nominated for clinical trials through to clinical development and launch and marketing ( Fig. 1 ). However, only after a certain point have sufficient knowledge and understanding of a compound’s pharmacology been gained for it to be considered useful as a repositioning candidate ( Table 1 ). The various high-throughput screening (HTS) libraries assembled both for traditional and for neglected and tropical diseases 13 may have the potential to identify novel pharmacophores, but, unlike hits from a repositioned compound library, they still face the challenge of drug development and associated attrition. For the purposes of this review, we will not consider efforts in the HTS, hit-finding, and lead generation spaces.
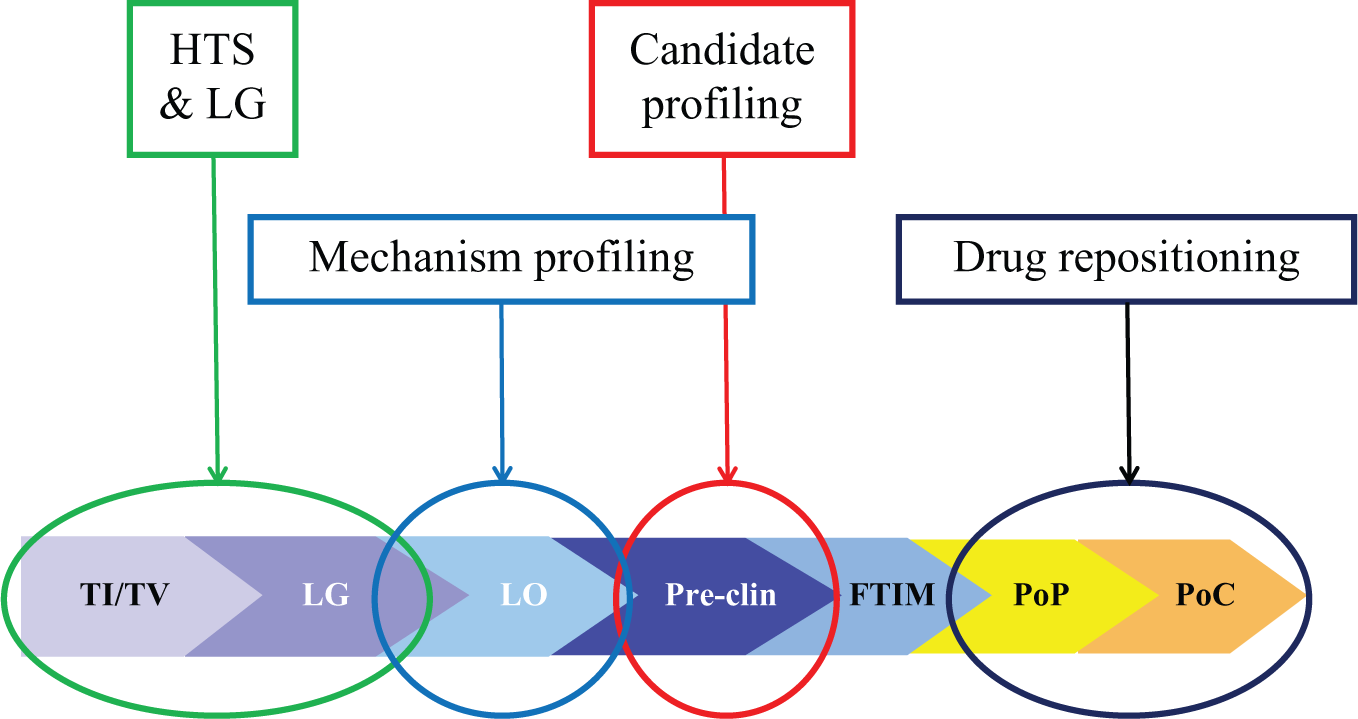
As a compound transitions from discovery through to development, the acquired knowledge and appropriateness for repositioning increase. Prior to candidate drug nomination, typically at the end of lead optimization, there is little knowledge of its effectiveness in humans, whereas after first time in man safety studies have been completed, some knowledge of its potential liabilities may allow repositioning into a new indication. However, full understanding of any repositioning outcomes requires target engagement to be established in humans, typically in proof-of-principle and proof-of-concept clinical trials. FTIM, first time in man; HTS, high-throughput screening; LG, lead generation; LO, lead optimization; PoC, proof-of-concept clinical studies; PoP, proof-of-principle clinical studies; Pre-clin, pre-FTIM preclinical studies; TI, target identification; TV, target validation.
Properties and Uses of Compound Types for Drug Repositioning.
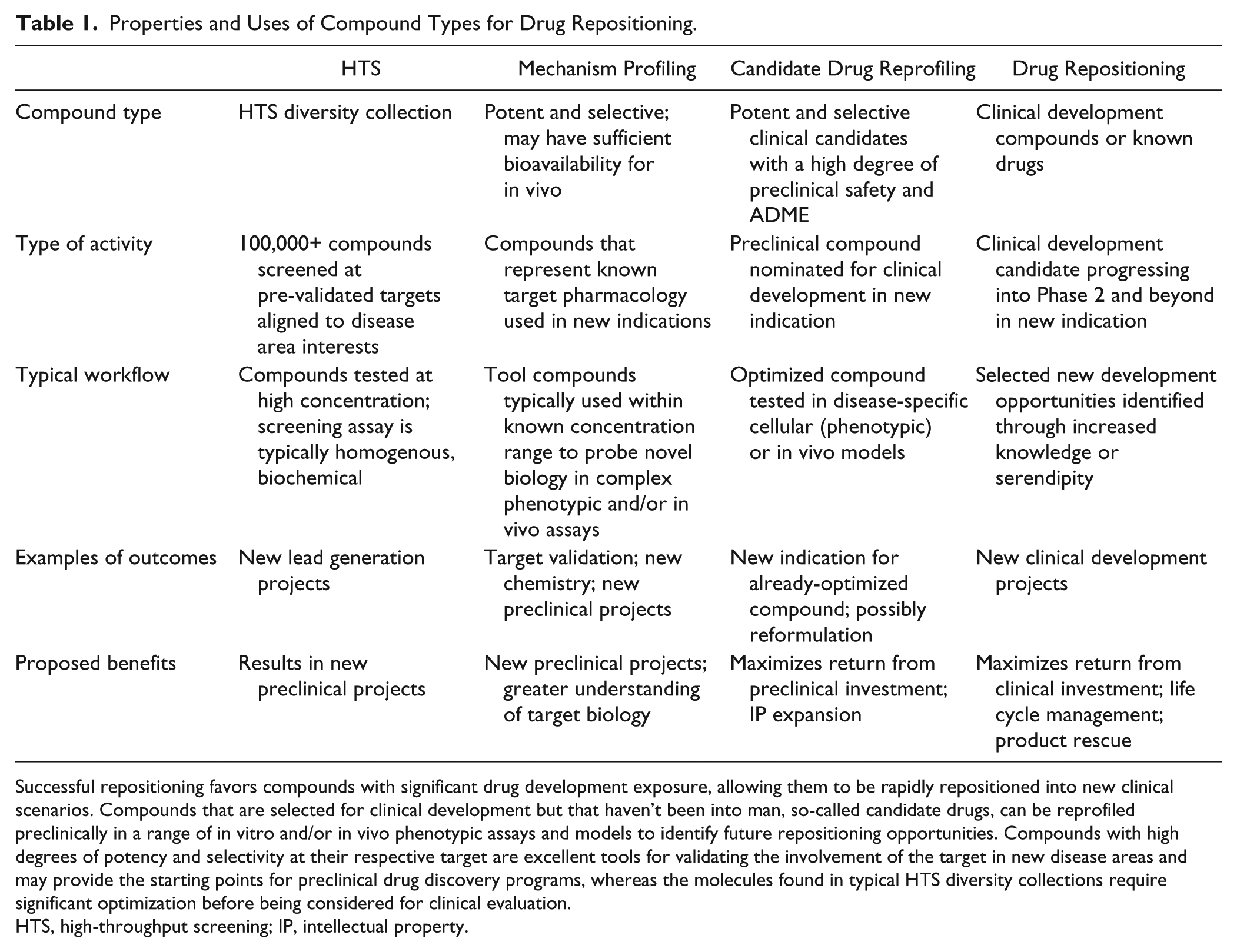
Successful repositioning favors compounds with significant drug development exposure, allowing them to be rapidly repositioned into new clinical scenarios. Compounds that are selected for clinical development but that haven’t been into man, so-called candidate drugs, can be reprofiled preclinically in a range of in vitro and/or in vivo phenotypic assays and models to identify future repositioning opportunities. Compounds with high degrees of potency and selectivity at their respective target are excellent tools for validating the involvement of the target in new disease areas and may provide the starting points for preclinical drug discovery programs, whereas the molecules found in typical HTS diversity collections require significant optimization before being considered for clinical evaluation.
HTS, high-throughput screening; IP, intellectual property.
In the context of building the requisite pharmacological knowledge and identifying new uses for existing compounds, there are three major phases that need to be considered. The first is during lead optimization, during which pharmacokinetic and ADME properties are enhanced; second, an optimized candidate drug is chosen for clinical development; and, finally, the development drug is subjected to rigorous clinical assessment to determine its suitability for launch.
Prior to, and indeed during much of, the lead optimization phase, there is probably insufficient knowledge of a compound’s pharmacology and pharmacokinetics to warrant repositioning (
Fig. 1
However, such compounds will almost always be proprietary and therefore unlikely to be available for external repositioning. A possible exception is in oncology, in which there is considerable sharing of compounds with academic and not-for-profit groups. Of note are recent attempts by some Pharma companies to make such compounds available through open innovation or peer-to-peer initiatives;8,14 however, of the majority of compounds tested in humans, many, if not most, will probably never be tested again for use in other indications.
At present, SMEs and academic or not-for-profit organizations are most likely to seek repositioning candidates from currently marketed drugs, and although this is a rich source of potential new medicines, the commercial value of the invention is more limited due to the availability, or lack thereof, of patent protection for the chemistry itself. Many of these are now available commercially as off-the-shelf collections 15 or from academic consortia such as the Rare Disease Repurposing Database [RDRD; a NIH library of US Food and Drug Administration (FDA)-approved drugs], the NIH Clinical Collection and Clinical Collection 2 (www.nihclinicalcollection.com), and the Johns Hopkins Clinical Compound Screening Initiative (www.jhccsi.org). 16
Properties of an Ideal Repositioning Candidate
To be a truly effective drug-repositioning candidate, we believe a compound should ideally have the following characteristics, which are summarized in Table 2 . The candidate should not require further chemical optimization; it should be “clinically experienced” (i.e., it has passed safety evaluation appropriate to the initial indication and been studied for clinical efficacy with positive biomarker outcomes); and, finally, it should be active in the new indication in the same concentration range as for the original disease. New indications requiring, for example, reformulation for topical administration, or that stem from secondary pharmacology observations may provide extremely fruitful repositioning opportunities; however, they also likely to require significant additional regulatory or safety assessment.
Properties of a Drug-Repositioning Candidate Compound.
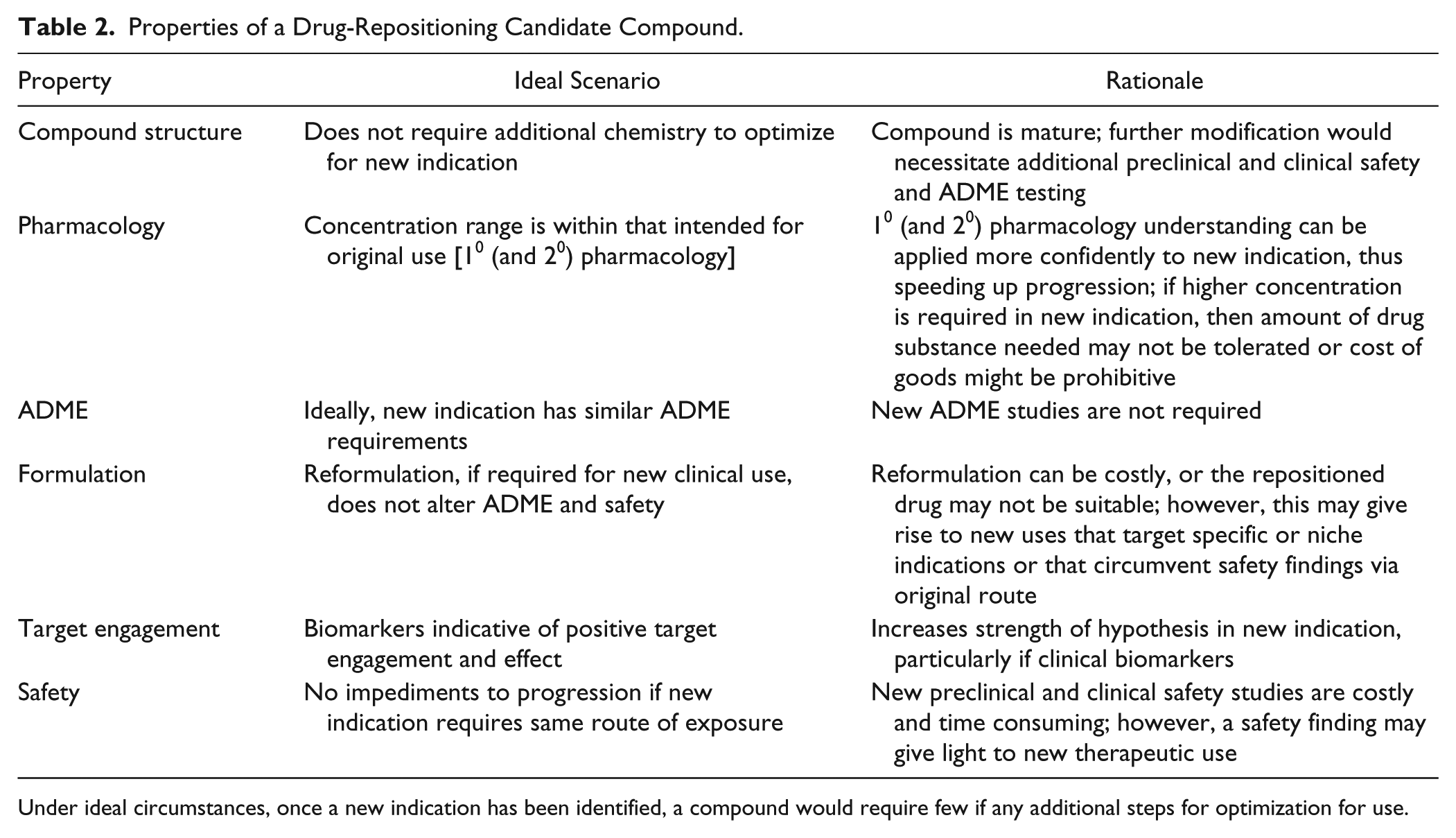
Under ideal circumstances, once a new indication has been identified, a compound would require few if any additional steps for optimization for use.
Drug-Repositioning Methods
Having considered what features might make an ideal drug-repositioning candidate, we can turn to the types of methods typically used for their identification; these range from blinded hypothesis-free or serendipitous screening through to knowledge-based approaches requiring significant bio- or chemo-informatics infrastructure.
Informatics Solutions for Drug Repositioning
Searching for “drug repositioning review” in PubMed (search carried out March 2014) returned 121 publications, the majority of which are related to computational methods. 17 In a recent review, Jin and Wong 18 (2014) outlined several such methods and suggested processes to prioritize repositioning activities based on disease area and compound knowledge; these techniques require at least some knowledge of the compound’s pharmacology or mode of action.19,20 A significant benefit of the use of informatics to prioritize compounds for testing is that the initial selection can integrate both disease and compound knowledge and significantly reduce the number of compounds tested, thereby reducing cost. 21 For example, Vazquez-Martin et al. (2011) have used a computational systems biology approach to identify metformin and chloroquine as agents with the potential to reduce cancer stem cells in premalignant tumor models. 22
Once computationally identified, the prioritized com-pound(s) will need to be tested in a biological assay, preferably one that has proven translational ability. Such phenotypic assays have the advantage that compounds can be tested at concentrations relevant to their known pharmacology and in relation to standards of known efficacy. In a recent groundbreaking study, Sirota et al. 23 described a novel method in which publicly available gene signatures from a wide number of diseases were simultaneously compared with those arising from the perturbation of model cellular systems by a range of well-known prescription medicines and other compounds. Pairs of compounds were identified that had complementary but opposite signatures (i.e., a disease gene signature and a compound that caused the opposite cell perturbation to correct it). These compounds were then tested in biologically relevant cell or in vivo models, yielding a number of novel repositioning candidates. 24 In a study using a similar approach, Hoenhdorf et al. (2012) 25 combined publicly available phenotypic and drug action data from the PhenomeNET and PharmGKBV databases to propose new disease associations for the rare and orphan diseases cystic fibrosis and chronic lymphocytic leukemia.
The use of computationally directed drug repositioning demonstrates the great potential of this approach; however, the repositioned drug is often effective in the new indication only at much higher concentrations. We would argue that in these circumstances, the outcome is primarily target validation rather than identification of a potential drug-repositioning candidate, because the drug itself may need to be modified or a new compound identified to reduce drug load or the potential for unwanted secondary pharmacology. This does not negate the valuable information gathered on the role that a particular target might play in a new disease, but any further repositioning would probably require refinement of the chemical starting point to provide a suitable candidate for clinical testing.
Drug Repositioning through In Vitro Biological Screening
For the purposes of this review, in vitro, ex vivo, or phenotypic assays are defined as those that model some aspect of disease biology in cells or tissues derived from an experimental species or humans, and that provide a reason to believe that activity has translatable relevance. In other words, these are not recombinant cell lines with an overexpressed target of the type that would be used to screen or rank sets of compounds for activity during lead generation campaigns. Given this, it is nevertheless possible that activity, even when compounds are tested at concentrations relevant to the known or primary pharmacology, may not be attributable to that pharmacology and may represent a new mode of action.
In vitro assays have the following benefits when used to identify repositioning activity: Direct knowledge is gained in relation to a potential new disease setting; multiple compounds with different modes of action can be tested and, depending on the throughput of the assay, over a full concentration–effect range; it allows for serendipitous, or hypothesis-free, assessment of compounds; and it provides data-driven choices for subsequent evaluation in more complex phenotypic or in vivo tests.
The examples given in the various disease areas discussed below use a wide range of cell-based assay types, typically in 96-well formats, which differ markedly in their outcome and throughput when compared to, for example, biochemical or in vivo assays.
Various whole-organism phenotypic assays are being increasingly used both for drug screening and for repositioning. The use of in vivo models in general and mouse models in particular has been extensively reviewed26,27 and is outside the scope of this review. However, plate-based screening technologies have been applied to both larval zebrafish (Danio rerio)28,29 and the nematode worm Caenorhabditis elegans (C. elegans), 30 and are being extensively used in drug discovery, with this use now extending to drug repurposing. Zebrafish are an animal species that are particularly amenable to be used as a model system in many aspects of drug discovery. 31 Zebrafish develop rapidly, they can be stably maintained for a number of days in a variety of multiwell plate formats,32,33 their genome has been sequenced, 34 and their morphology allows them to be studied using readily available imaging systems. In particular, their transparency during the larval stage of development greatly facilitates noninvasive use of optical imaging techniques, as does their permeability to small-molecule drugs, for which behavior and responses to many compounds have been modeled. 35 In a similar fashion, the nematode worm C. elegans also has been used in drug discovery36,37 and has been a key model system for a host of biological processes. 38
Examples of the use of zebrafish in drug repositioning include studies of pancreatic disease, 39 tobacco dependence, 40 and hearing impairment. 41 Rovira et al. 39 developed transgenic zebrafish in which pancreatic β-cell differentiation as well as Notch signaling, a critical pathway in pancreatic development, 42 could be observed; This was aided by a novel well plate system that allowed lateral views of swimming larvae. 39 From 3131 compounds in the Johns Hopkins clinical library, screened at a final concentration of 20 µM, they identified 18 that affected islet formation, of which six were positive when retested. Two FDA-registered compounds in particular were the focus of additional work: tetraethylthiuram disulfide (Disulfram), which is prescribed for the treatment of alcohol abuse, and mycophenolic acid (MPA), which is used as an immunosuppressant. As well as being potentially repositionable drugs, mechanistic work also aided the characterization of two unique pathways in β-cell differentiation in the zebrafish, including downregulation of guanosine triphosphate production and retinoic acid biosynthesis.
Cousin and colleagues (2014) 40 have used the zebrafish platform in an initially more targeted way. They evaluated the behavior of 39 FDA-approved medications, which had been vetted by a physician for the likelihood that they would be prescribed to treat tobacco dependence based on their side effect profile and contraindications in the target population; many of the test compounds were for CNS targets, indicating the potential to penetrate the blood–brain barrier. The reward pathways and many of the receptors involved, such as those for nicotinic acetylcholine, are conserved in zebrafish, 43 making them a useful species in which to study dependence. The 39 compounds were tested for their ability to modify a CNS-mediated locomotor response, 44 in which either nicotine or ethanol was the stimulant. Six compounds were active with two, apomorphine and topiramate, affecting both nicotine- and ethanol-induced behavior.
In a final example, Vlastis et al. (2012) 41 used a zebrafish model to screen for inhibitors of the known inner ear mechanosensory hair cell toxins neomycin, gentamicin, kanamycin, and cisplatin; loss of these inner ear hair cell structures is known to be involved in hearing impairment and balance disorders. Zebrafish express hair cell structures along their lateral lines that have comparable structure and physiology to mammalian inner ear hair cells45,46 and are considered to be a suitable model of inner ear hair cell loss. Zebrafish also have the advantage of being amenable to study in 96-well plate formats using imaging endpoints. The authors screened an FDA-approved drug library of 640 compounds and identified 10, including the selective estrogen receptor modulators tamoxifen and raloxifene, which are able to protect hair cell loss in response to the above toxins. Tamoxifen and raloxifene were further studied, and the data generated indicated that their protective effects were not as a result of their known pharmacology; similar data were obtained for the other related active compounds.
Clearly, the studies described here and others47,48 in zebrafish, alongside those using C. elegans,49,50 show the potential opportunity of these whole-organism multiwall-based phenotypic assays for drug repositioning.
In Vitro Screening: Specific Disease Areas
We will discuss in vitro repositioning as applied in two broad areas. First are tropical and neglected infectious diseases (NTDs), which include diseases such as tuberculosis, malaria, and a variety of viral, protozoan, fungal, and helminthic infections. Second are the majority of other conditions, which can be further subdivided into those that have proven poorly tractable to conventional HTS-led drug discovery, such as CNS disorders; or those that have multiple genetic components, such as cancer and rare or orphan diseases.
Neglected Tropical Diseases
Diseases prioritized for action by the World Health Organization include tuberculosis, malaria, dengue fever (viral), buruli ulcer (mycobacterial), and a range of diseases that, unlike the infectious diseases of developed countries, are caused by eukaryotic parasites—unicellular kinetoplastid protozoa or multicellular helminths (flukes, tapeworms, and nematodes). The World Health Organization estimated that up to 1 billion of the world’s population are affected by one or more NTDs, and the resulting sickness and long-term disability impede economic productivity, perpetuating the cycle of deprivation. 51 There remains a great need for more efficacious and safer treatments for several of the NTDs; for an overview, see the Global Health Primer (www.globalhealthprimer.org/Diseases). These diseases are, of course, “neglected” because those who need them are unable to pay the economic cost of treatment, and there is no prospect of recovering research and development (R&D) costs. Funds for R&D into NTDs come from philanthropic organizations, research councils, and governments. Pharmaceutical companies have been generous in providing in-kind help, and especially in sharing compounds via, for example, the Drugs for Neglected Diseases Initiative. The World Intellectual Property Organization’s Re:Search Initiative has worked with industry to overcome perceived intellectual property barriers and facilitate sharing of patented compounds in a spirit of open innovation.
Although there have been some notable large-scale primary screening efforts (e.g., 6 million compounds screened by Medicines for Malaria Venture, leading to an open-access “box” of leads) 52 the cost of de novo drug discovery is such that, given the absence of commercial returns, it is logical that nongovernmental organizations and academics have been very actively attempting to repurpose existing mature compounds for NTDs. The repurposing approach has many advantages (covered in detail elsewhere in this article) and also some specific challenges when applied to the NTD field. First of all is throughput: High-throughput, biologically relevant screening assays do not exist for all NTDs. The smaller number of mature compounds available for screening, normally up to a few hundreds, is a good match to the rather low throughput of some biologically relevant phenotypic screens (e.g., for parasitic nematodes). Second are drug targets in NTDs: Because causative agents of many NTDs are eukaryotic, there is a realistic possibility that drug target classes in the pathogens may overlap with the targets of the diseases in Pharma pipelines. Some important pathogen targets are known empirically, and efforts to prioritize possible targets computationally continue53,54 (also see the TDR Targets database: www.tdrtargets.org). It has proven productive to screen panels of mature compounds that are active on related mammalian targets. Good examples of this approach include inhibitors of cysteine proteases, HMGCoA reductase, and a variety of kinases. Cysteine proteases have important physiological roles in eukaryotic pathogens (mammals would have serine proteases instead in some of the biological contexts). Inhibitors of mammalian cathepsins are potent against Trypanosoma cruzi (Chagas disease), Plasmodium spp. (malaria), 55 and hookworm. 56 The parasite enzymes have been cloned and expressed, and parallel biochemical and phenotypic screening is useful to provide correlative evidence of mode of action and to compare potencies against the pathogen target with data on the human target. HMGCoA reductase inhibitors have been shown to have activity against schistosoma parasites (www.wipo.int/research/en/collaboration), and investigation of their potential continues.57,58 Kinase inhibitors, many of which have been developed in the pharmaceutical industry as oncology treatments, are promising targets in parasitic protozoa, which have related kinases, 59 for example kinetoplastid protozoa. 60
An alternative approach is serendipitous screening of panels of mature compounds in whole-pathogen assays; for example, Gloeckner et al. (2010) 61 used the Johns Hopkins Clinical Collection to identify Closantel, a veterinary antihelmintic, as active on Onchocerca volvulus, the nematode that causes river blindness; whereas Abdulla et al. (2009) 62 have identified compounds that have hit- and lead-like properties for the treatment of schistosomiasis. This approach has the potential to reveal new mechanisms and/or identify candidates directly, without initially depending on knowledge of parasite target biology (which is less well investigated than mammalian target biology). Compound panels can be selected on the basis of compound quality and availability and/or may be enriched for classes of targets known to exist in pathogens. The evolutionary distance of NTD parasites from humans limits the confidence with which target validity can be deduced from activity data, and it ought not to be assumed that a compound that produces a phenotypic effect in a cell assay is acting via the target for which the compound was originally discovered. If mode of action is considered important, then the target in the pathogen will need to be identified experimentally.
The compounds being tested will be pharmacologically active in humans. Equal or greater potency in pathogens will be a fortunate accident, except for the most highly conserved targets. High sequence or active site conservation may be associated with essentiality fundamental cellular functions. For example, human cyclin-dependent kinase can regulate the yeast cell cycle, and elucidating this mechanism of cell cycle control depended on discoveries in yeasts, sea urchins, and human cells. 63 Of course, cell cycle inhibition as a side effect in humans would raise safety concerns. Therefore, we could expect that further chemical optimization would be unavoidable when repurposing such compounds for pathogens. Nevertheless, the prospects for direct repositioning are more hopeful than they might appear. Drug candidates intended to treat chronic human conditions could, depending on primary pharmacology, be sufficiently tolerable to treat infections. Other compounds that would not be desirable for chronic human administration (e.g., those with cytochrome p450 activity) could be tolerable for short courses of treatment and/or for use in populations that, unlike the aging inhabitants of the most affluent countries, are unlikely to be receiving multiple medications. For example, benznidazole is used successfully to treat Chagas disease in spite of its suboptimal properties. 64 Systematic screening of publicly available drugs and candidate drugs recently yielded promising leads for dysentery caused by the protozoa Entamoeba and Giardia. 65 One lead was the antirheumatic compound aurofin, which has been used as a human treatment for more than 20 years. 66 Similarly, clinical experience with inhibitors of cathepsin K showed that such compounds are well tolerated when administered chronically, 67 so there is good reason to be optimistic that antiparasitic cysteine–protease inhibitors will also prove to be well-tolerated treatments. Fortuitously, the ADME properties might favor activity in the pathogen. Pathogens might be less able than mammals to transport particular compounds out of their cells—ivermectin is a classic example of a compound that would be unsafe in mammals were it not an excellent substrate for the multidrug transporter P-glycoprotein.68,69 Such helpful quirks of comparative biochemistry cannot, of course, be relied on. The projects that delivered the drug candidates will have generated large numbers of related compounds, and screening these should at least provide some understanding of comparative structure–activity relationships of the pathogen target versus the human target. Divergence between pathogen and human target active-site sequence might make it possible to design parasite-specific compounds even when the side effects of the parent candidate drug might not be acceptable. An example is the redesign of epidermal growth factor receptor compounds to give selectivity for Trypanosoma brucei kinases.70,71 Aurora kinase inhibition is currently being pursued as a cancer treatment; however, intrinsic mechanistic side effects limit the dose and duration of treatment of inhibitors of the human enzymes. Related kinases are important for mitosis in the malaria parasite Plasmodium; 72 selectivity for the parasite over host cells will be essential. This should be achievable through a combination of analogue screening and rational design. 72
CNS Disorders
There is much in vitro and in vivo evidence that drugs designed for use in a wide range of non-CNS disorders have activity in CNS models. However, many of these CNS-focused repositioning examples have primarily arisen from specific hypotheses or serendipity, such as the use of the antiviral drug adamantine 73 for early-onset Parkinson’s disease, rather than screening efforts. The examples discussed here, which have used an in vitro platform to identify novel active compounds, come primarily from neurodegenerative diseases.
In a recent wide-ranging review, Corbett et al. (2012) 74 highlighted the potential for drug repositioning into Alzheimer’s disease. Using literature analysis, they evaluated the preclinical and, when available, clinical evidence and suggested a number of compounds and associated mechanisms that might be worthy of future study. Of particular note was the effect of calcium channel blockers (CCBs). In one clinical trial, nitrendipine, a widely used antihypertensive and angina drug, appeared to reduce the risk of developing dementia in a cohort of subjects older than 60 years by up to 55%. 75 Preclinical studies have indicated that CCBs are able to reduce the production and oligomerization of Aβ as well as improve cell survival. Corbett et al. (2012) went on to highlight an in vitro study 76 whereby nine CCBs prevented Aβ production in a cell model, although the concentrations required were higher than those used therapeutically for cardiovascular disease. In addition to the activity of CCBs, angiotensin receptor inhibitors, glucagon-like peptide 1 (GLP1) analogues, tetracycline antibiotics, and retinoids were also implicated. In another study focusing on Alzheimer’s, Hayes et al. (2013) 77 screened a panel of 89 FDA-approved oncology drugs in a Chinese hamster ovary (CHO) cell line expressing the amyloid precursor protein 751WT. Aβ production was reduced in response to bis-chloroethylnitrosourea (BCNU; Carmustine; BiCNU), a licensed chemotherapeutic used for the treatment of a number of tumor types, including Hodgkin and non-Hodgkin lymphomas. Importantly, the effect of BCNU was also translated in vivo; in an APdE9 mouse model, in which the mice are predisposed to the generation of amyloid plaques, total amyloid plaque burden was significantly reduced after chronic (60-day) administration in comparison to vehicle-treated littermates. In a different neurodegenerative disorder, Parkinson’s disease, the Michael J. Fox Foundation (https://www.michaeljfox.org) has brought considerable focus to the potential of drug repositioning, with research grants being awarded to a number of programs, such as for the study of amitriptyline, a tricyclic antidepressant, and of GLP1 agonists and DPP4 inhibitors, which are used to treat type 2 diabetes. 78
Finally, as mentioned above, outside the use of screening methods, there are examples of drug repositioning in CNS disorders that have proven particularly intractable, such as for ischemic stroke. 79 Hess and Fagan (2010), 80 for example, have shown that the broad-spectrum antibiotic minocycline is an effective adjunct to the use of tissue plasminogen activator (tPA) in a rat model of ischemic stroke, and this observation has been clinically tested with benefit being observed in combination with aspirin in male patients. 81 However, in a number of clinical trials, the blood pressure–lowering effects of angiotensin-II antagonists, such as candesartan, have not proven beneficial, 82 indicating that, at least for stroke, the source of the drug is no predictor of success in humans.
Oncology
Preclinically, many in vitro tumor models have been screened with drug-like or FDA-approved libraries of compounds with the accompanying identification of repositioning hits. For instance, Jachan et al. (2013) have shown that tricyclic antidepressants may have utility in non–small cell lung cancer; 83 Pessetto et al. (2013) identified two compounds from a screen of 796 FDA-approved drugs for their ability to inhibit the proliferation of metastatic gastrointestinal stromal tumor; 84 while a number of compounds from an FDA clinical library were identified as sensitizers of tumor necrosis factor-α (TNF-α)-related apoptosis-inducing ligand (TRAIL), indicating potential as chemotherapeutic agents. 85
Among other examples of the use of in vitro screening models to reposition existing drugs into oncological disorders, the following are noteworthy due to the diversity of compounds tested and the potential for near-term therapeutic utility. Using a library of 1600 annotated clinical compounds (Pharmakon 1600 from MicroSource Inc.) initially tested at 10 µM, Nygren et al. (2013) 86 identified mebendazole, an antihelminthic drug used to treat gut worm infections, as having cytotoxic activity in the RKO and HCT 116 colon cancer cell lines. To determine the mechanism of this cytotoxic activity, mebendazole was tested against a panel of kinases; this revealed potent inhibitory action against Abl and BRAF. The same group also reported a case study in a patient with refractory metastatic colon cancer whose metastases were significantly reduced by twice-daily dosing with the standard antihelminthic dose of mebendazole.
To identify novel potential therapies for prostate cancer, Platz et al. (2011) 87 screened the Johns Hopkins Drug Library (JHDL) of 3187 compounds, of which 1811 are FDA-approved drugs, against two prostate cancer cell lines, LNCaP and PC3, which are androgen-insensitive and androgen-sensitive, respectively. In their primary screen, Platz and colleagues measured the ability of the JHDL compounds (5 µM) to inhibit overall DNA synthesis and cell proliferation using a 96-well plate-based assay [3H]-thymidine incorporation. Actives were followed up against a larger panel of prostate cell lines, and concentration–response data generated. Of these, digoxin, a cardiac glycoside commonly used for heart failure and arrhythmia, was found to have antiproliferative activity. To validate the potential for digoxin in prostate cancer, data from a longitudinal epidemiological analysis of risk factors for cancer in men were used in addition to a detailed questionnaire of those deemed eligible for this study. Their analysis, taking into account a variety of other compounding factors, indicated that digoxin use was associated with an approximate 25% reduced risk for developing prostate cancer in this cohort of men. 87
A final example of the use of in vitro screening methods for drug repurposing in oncology is the identification of statins, in combination with standard of care, as inhibitors of glioblastoma cell proliferation. 88 Glioblastomas are particularly difficult to treat, having a high incidence of mortality, 89 and are also considered as orphan diseases with relatively little associated drug development. 90 Importantly, an additional constraint for a repositioned drug would be the need for compounds to cross the blood–brain barrier, increasing the challenge involved. Jiang et al. (2014) screened a collection of 446 compounds available from the NIH Clinical Collection library in a U87 glioblastoma cell line, monitoring effects on cell proliferation. 88 The most potent compounds, determined by ranking IC50 values, were subsequently retested against three additional glioma cell lines and also against a number of stem cell lines derived from patient material. Alongside a number of known anti-neoplastic agents, two statins, pitavastatin and cerivastatin, were found to be active. When subsequently screened in combination with low doses of chemotherapeutic agents such as irinotecan, pitavastatin significantly increased their effectiveness. The authors suggested that use of pitavastatin in combination with irinotecan may be useful for patients who develop side effects to chemotherapy such as diarrhea or neutropenia, allowing a reduction in the dose of chemotherapeutic while maintaining efficacy.
In spite of these well-documented programs of in vitro screening, searching in both the literature and clinical trials databases finds few clinical examples described as being from drug repositioning, although experience suggests that there must be many more. At the time of writing, using the search terms drug repositioning or drug repurposing combined with cancer or tumor brought back only one study report on ClinicalTrials.gov: a Phase 1 study of the HIV protease inhibitor nelfinavir 91 (see below). Possible reasons for this may be due to differences in terminology (i.e., oncologists do not usually describe the exploitation of a pathway, e.g. cell cycle, across diverse tumor types as “repositioning”). Furthermore, oncology project workflows use experimental approaches that might be described as “reprofiling” in other disease contexts. One example is human tumor cell panels and xenografts to identify likely tumor types and organs affected before approaching the clinic, in addition to the opportunity to conduct small, early-phase trials in different tumors before pivotal human trials are designed. Because of such factors, it may not be apparent that repositioning is a routine practice in the development of novel cancer treatments.
In contrast, there are unequivocal examples of drugs discovered for indications other than cancer being repositioned into oncology. Perhaps the best-known example is the use of thalidomide and its structural derivate lenalinomide (Revlimid) for the treatment of multiple myeloma. 92 Under-standing the potential of these drugs came about as a result of many years of studying both their molecular mechanisms and effects in a variety of diseases. The recognition that thalidomide was able to exert immuno-modulatory effects came via its use as a sedative in leprosy patients suffering from erythema nodosum leprosum (ENL). ENL produces painful skin lesions and other systemic effects, and at the time it was intractable. However, patients treated with thalidomide showed significant reduction in the number of lesions. 93 Thalidomide was later shown to inhibit angiogenesis, via suppression of TNF-α, 94 and ultimately to be effective in multiple myeloma. 95 Another example of clinical data informing repositioning in the oncology field is the potential for use of metformin, a widely used glucose-lowering drug.96,97 Metformin targets activated protein kinase (AMP), which is an important regulator of tumor suppressor genes such as LKB1. In a variety of cell models, and in vivo, metformin is able to reduce cell proliferation 98 as well as inhibit cancer stem cell production.99,100 Finally, the antiretroviral drug nelfinavir, which is used in the treatment of HIV and which is an inhibitor of the PI3K–Akt–mTOR pathway, is the subject of a number of additional clinical oncology studies. 91
Rare and Orphan Disease Indications
We described above the value of compound repurposing for those neglected tropical diseases in which R&D is neglected due to lack of commercial return, even though each of the NTDs affects large populations. In the case of the rare or orphan diseases, commercial incentives are again insufficient to power large-scale efforts, although for different reasons. According to Sardana et al. 101 (2010), the FDA recognizes 6000 rare and orphan diseases. In the United States, the NIH Office of Rare Diseases Research classifies these as diseases from which fewer than 200,000 individuals suffer. Only a small minority of these diseases has been of interest to the bio-pharmaceutical industry: The small populations affected offer poor prospects of commercial return, and the low prevalence and sometimes geographic dispersion of sufferers, many of whom are children, hinder efficient clinical trials. Many of these diseases are caused by infrequent genetic disorders and loss-of-function mutations in specific proteins that may not be amenable to small-molecule therapies. It is logical, therefore, that repositioning can be a more attractive approach than de novo compound discovery. In addition, it may also be particularly fruitful to combine computational approaches in orphan diseases as a means of identifying repositioning opportunities and also for target validation. 102 The literature reports a number of approaches aimed at generating frameworks to identify both druggable targets and repositionable drugs for rare diseases.103,104
Summary and Conclusions
Despite the recent prominence of drug-repurposing studies that use an in silico filter to reduce the number of molecules required for assay, the use of in vitro screening to reposition compounds into new indications, as reviewed here, remains a significant and important methodology.
As we have noted, this approach has a number of benefits. It is precisely because it does not select for potential actives before the initial screening round that in vitro repositioning is open to both the serendipitous and the mechanistic identification of compounds from any of the target classes or compound families that are available to the investigator. 105 Indeed, in some disease areas, an in vitro screen may be the most useful starting point for drug repurposing. This may be particularly true when traditional target validation–based approaches have had limited success, such as in the case of some CNS disorders; when new targets have been identified but have limited clinical validation, such as in certain cancers; or when completely new approaches are required due to the interaction of host and pathogen genomes. The outcome of an initial screen can then be focused and refined to determine the nature of the biological activity in the new disease area. These data can be added subsequently to existing in silico models to improve their predictivity. 105
As the use of zebrafish models exemplifies, each new area of emerging biology offers opportunities to repurpose existing drug candidates, and we would expect this to continue. For example, the emergence of stem cell technologies, and the concomitant potential to derive cell lines with increased translational relevance, could open up a whole new vista for in vitro–based screens, further expanding their role as key methods for drug repurposing.
Changes to commercial and institutional infrastructure may also increase both the relevance and viability of drug-repositioning projects. As the bio-pharmaceutical industry continues to reshape, and as collaborations between private companies and between private and publicly funded entities become more diverse and open, 8 new and distinctive ways of working will evolve that will be particularly suited to repurposing compounds via in vitro screening. If so, then we can expect drug repurposing to generate significant new treatments for areas of unmet medical need.
Footnotes
Acknowledgements
The authors would like to thank Dr. Peter Simpson (Screening Sciences, AstraZeneca) for his thoughtful insights and suggestions during the preparation of this review and Arwel Pritchard for kindly reviewing the final article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.