
Abstract
Neglected tropical diseases (NTDs) are a group of 17 diseases that typically affect poor people in tropical countries. Each has been neglected for decades in terms of funding, research, and policy, but the recent grouping of them into one unit, which can be targeted using integrated control measures, together with increased advocacy has helped to place them on the global health agenda. The World Health Organization has set ambitious goals to control or eliminate 10 NTDs by 2020 and launched a roadmap in January 2012 to guide this global plan. The result of the launch meeting, which brought together representatives from the pharmaceutical industry, donors, and politicians, was the London Declaration: a series of commitments to provide more drugs, research, and funds to achieve the 2020 goals. Drug discovery and development for these diseases are extremely challenging, and this article highlights these challenges in the context of the London Declaration, before focusing on an example of a drug discovery and development program for the NTDs onchocerciasis and lymphatic filariasis (the anti-Wolbachia consortium, A·WOL).
What Are NTDs?
Neglected tropical diseases (NTDs) are a group of infectious diseases categorized by the neglect they have suffered in terms of investment in control measures, when compared with the “big three” (tuberculosis, HIV/AIDS, and malaria). The global burden of disease caused by NTDs is high, yet they have been neglected in terms of funding, research, and policy. The lack of investment in drug discovery is due, in part, to the absence of economic incentives; NTDs are diseases of the poor, and poor people cannot afford to buy drugs. The issue of poverty is central to the nature of NTDs, for these diseases not only are due to poverty but also contribute to poverty through their socioeconomic impacts. 1
The NTDs encompass a broad range of viral, bacterial, and parasitic infections. There are 17 core NTDs as defined by the World Health Organization (WHO): dengue, rabies, trachoma, Buruli ulcer, endemic treponematoses, leprosy, Chagas disease, human African trypanosomiasis (sleeping sickness), leishmaniasis, taeniasis/cysticercosis, dracunculiasis (guinea worm disease), echinococcosis/hydatidosis, foodborne trematodiases, lymphatic filariasis, onchocerciasis (river blindness), schistosomiasis, and soil-transmitted helminthiases. The control of these diseases is overseen by the Control of Neglected Tropical Diseases program at WHO, which has drawn up a roadmap of their vision and goals to eliminate five diseases (leprosy, sleeping sickness, blinding trachoma, guinea worm disease, and lymphatic filariasis) and to control five (schistosomiasis, soil-transmitted helminthiases, visceral leishmaniasis, onchocerciasis, and Chagas) by 2020. 2 All NTDs have been categorized as “tool ready,” given that there are tools (e.g., drugs) that can be implemented now, yet also “tool deficient” because many of these tools (drugs and diagnostics) and implementation strategies are inadequate to achieve the desired goals. 3 Over recent years, there has been an increased effort to address this imbalance through the formation of several public-private development partnerships and donor-facilitated consortia. Drug discovery and development opportunities in NTDs are therefore beginning to emerge to address the tool deficiency and provide the necessary intervention strategies to achieve the goals of elimination.
This article will review the recent acceleration in the global fight against NTDs, focusing on some of the challenges facing drug discovery and development for these diseases, and highlight an example of a NTD drug discovery and development program for onchocerciasis and lymphatic filariasis (the anti-Wolbachia consortium [A·WOL]).
London Declaration
In January 2012, WHO published a roadmap 4 to guide the implementation of policies and strategies relating to their Global Plan on NTDs. 2 This roadmap was launched at a high-profile event, “Uniting to Combat NTDs: Ending the Neglect and Reaching the 2020 Goals,” held in London on January 30, 2012. Nine CEOs from the pharmaceutical industry shared a stage with the director general of the WHO, Bill Gates, and political representatives of several member states to pledge to (1) sustain, expand, and extend the drug supply; (2) accelerate research and development for new treatments; and (3) increase funding to improve implementation in order to control or eliminate 10 NTDs. 5 This became known as the London Declaration on Neglected Tropical Diseases.
This watershed event represents the outcome of a progressive rebranding of NTDs to promote their place on the global health agenda, particularly in the context of meeting the Millennium Development Goals. 6
Putting the Pledge into Practice
The Impact So Far
The London Declaration on NTDs has been widely disseminated and has succeeded in placing NTDs firmly on the international global health agenda. In the year since its inception, there were increased requests to the pharmaceutical industry for drug donations, and according to their First Annual Report, 100% of all requests have been met. 7 This translates into a total of 1.2 billion treatments provided in 2012, either for preventative chemotherapy or treatment of an NTD. These treatments include the provision of albendazole or mebendazole for soil-transmitted helminths, which have increased more than fivefold during 2012, and 29 additional countries now have free access to these drugs. 7 The commitment to a sustainable drug supply has been demonstrated, and this particular bottleneck to implementation has been alleviated.
The 2020 goals are extremely ambitious, and there are many obstacles to overcome before they are achieved. The improvements to the delivery of preventative chemotherapy since the London Declaration are tangible, allowing implementation scale-up, increased coverage, and, ultimately, the alleviation of suffering in millions of people. 8 This impact should not be underestimated, but one of the major challenges now is to ensure effective distribution through accelerated scale-up. 9 Another issue, highlighted in the first annual report of the Declaration, was the projected funding gap that could prevent the realization of the 2020 goals. This amounts to approximately $300 million per year, and thus, the increased investment made by donors and governments in 2012 needs to increase further in order to meet the funding deficit. Suggested methods to increase donations include involving the private sector in endemic countries, further integration between different health and development programs, and by countries gaining access to funds already in place by including NTDs in their health plans. 7 Also, the engagement of rising economies, such as China, in the fight against NTDs could be another potential funding source. 10
There is evidence that the Declaration has instigated progress in the research and development (R&D) aspects of the commitments made (i.e., in the development of new tools and strategies). Two new diagnostic tools for sleeping sickness and lymphatic filariasis have received regulatory approval this year. 7 Also, there appears to be increased engagement with pharmaceutical companies and access to drug libraries. For example, the Drugs for Neglected Diseases Initiative (DNDi) has been given access to hundreds of thousands of compounds from eight different pharmaceutical companies during 2012. However, the R&D commitments of the Declaration were not completely defined at the London meeting, and, indeed, it has been suggested that not enough focus was given to this aspect. 11 Although access to drug libraries is obviously a great resource, the early-stage drug discovery pipeline, such as assay development, also requires investment and development. Of the 10 diseases outlined in the Declaration, only guinea worm can be eliminated using the current tools, 9 highlighting that merely increasing drug supply and distribution (assuming the funding gap is overcome) will not be enough to achieve the 2020 goals; new drugs are required.
Drug Discovery for NTDs
Although the increased donations of drugs and funding required can potentially be met through increased advocacy and commitment, the commitments to accelerating R&D for new treatments may encounter many more fundamental barriers. The complex biology of many of these parasites and their need for vectors for development and transmission makes traditional industrial-scale drug discovery programs incredibly challenging.
The general neglect that these diseases have encountered by the pharmaceutical industry has meant that basic research findings have not found their way into a drug discovery pipeline. 12 Although there has been a lot of basic research conducted investigating the biology of these organisms, which has led to the discovery of potential chemotherapeutic targets, the lack of screening platforms and translational processes have prevented drug discovery and development. Although target-based chemotherapeutic screens have been a focus of drug discovery programs in the postgenomic era, there has been a movement toward returning to phenotypic-based whole-organism screening assays. 13 This is based on the general consensus that target-based screens have been less successful than phenotypic screens in the discovery of novel drugs. 14 One of the challenges associated with drug discovery using a phenotypic screen is the subsequent identification of the target, which assists in preclinical and clinical development, primarily through the prediction of mechanism-based toxicities. 13 The advances in proteomic technologies have helped this process, but in terms of the regulatory requirements, there is actually no need to define the target of an active compound in order to move into clinical trials. 15 Because of their innate complexities, lack of validated targets, and ultimately, the profound need for new drugs to treat these diseases, phenotypic screens are particularly important in NTD drug discovery. This does mean, however, that there has been a reliance on low- to medium-throughput whole-organism assays, particularly for the helminth diseases, preventing access to a critical mass of compounds that can be investigated further.
The recent technological advances in automated microscopy have begun to affect drug discovery for NTDs. For the helminth diseases, these advances have the capacity to increase throughput by replacing laborious and often subjective manual microscopic observation (recently reviewed by Paveley and Bickle 16 ). High-content imaging has been used to develop a screen for Schistosoma parasites. Algorithms were developed to characterize morphological damage and changes in the motility of schistosomula, the larval stage of the parasite, within 384-well plates. This high-content screen (HCS) has been validated against 10,041 compounds with demonstrated congruence with visual inspection. 17 Another HCS for helminths has been developed using an automated motion-based platform. The WormAssay has been tested for use with Brugia malayi worms (a causative agent of lymphatic filariasis) and has also been demonstrated to be compatible with schistosomes, 18 indicating that it could be applicable to many macroparasites. For some protozoan parasites, such as Trypanosoma brucei, which causes African sleeping sickness, high-throughput screening (HTS) has been possible19,20 without the need for high-content imaging. However, for other protozoa such as Trypanosoma cruzi (Chagas disease)21,22 and Leishmania species,23,24 HCS offers the opportunity to improve and build on previous screens through its ability to test compounds against more clinically relevant stages of the life cycle.
Key differences may exist in drug sensitivity between different life-cycle stages. This has recently been demonstrated with screening assays targeting Leishmania. Only 4% of hits defined using a promastigote (i.e., the stage found in the insect) screen were hits in the intracellular amastigote (the stage found in the human) screen. 24 Perhaps more importantly, 50% of those compounds demonstrated to be active against the amastigote stage had not been demonstrated as active in the promastigote screen, highlighting the problem of false-negatives when using an inappropriate screen. Although the presence of false-positives in a screening program is not ideal, most of these will likely be eliminated in subsequent screening models within the screening funnel. On the other hand, false-negatives, potentially interesting compounds, would be discarded at the first step. In another recent study, an axenic amastigote screen was compared with an intracellular HCS. Again, a high number of false-positives was observed with the screen using the free-living parasites, but in this case, the resulting hits in both screens were the same, indicating that the problem of false-negatives can be negated. 23 There is potential for this axenic assay to act as a prescreen prior to using the more technically challenging intramacrophage assays. 25 Nevertheless, the Leishmania donovani intracellular screen has been validated, and screening of 200,000 compounds has been completed, although it is, as yet, unpublished.15,24 This number is greater than the total number of compounds that has historically been tested against visceral leishmaniasis, a disease that is fatal if left untreated, demonstrating the progress that can be made with adequate investment and collaboration. 15
Although the definition of the biological target of an active compound is not necessarily required in drug discovery for NTDs, the drug discovery process must be conducted in line with a target product profile (TPP) for each particular disease. This drives the drug discovery process to be as streamlined as possible to provide a useful product at the end. For example, prerequisites for all NTD drugs are that they should be low cost, not require a cold chain, and be easily distributable within the health infrastructure available in affected countries (i.e., single-dose oral formulations are preferred). Depending on the currently available treatments for a particular disease, TPPs outline the minimal and desirable qualities that are required for a novel chemical entity (NCE) to progress. A treatment currently being rolled out for treatment of visceral leishmaniasis in certain areas, through an agreement between Gilead and WHO and funding from the Department for International Development, UK, is liposomal amphotericin B. 8 It is interesting to note that this drug would not even meet the minimal TPP put in place by DNDi for NCEs in development. 26 This is true for the majority of drugs on the market to treat NTDs, once again highlighting the neglect that these diseases have suffered and the paradigm shift that has taken place over the past decade to improve matters.
It is clear that there are many difficulties associated with drug discovery for the NTDs, but progress has been made against both the protozoan and helminth parasites. Many collaborative discovery programs are ongoing and the increased profile afforded to NTDs since the London Declaration will hopefully provide a window of opportunity to establish more such programs. One ongoing program that aims to address some of the issues described above, such as screening throughput and capacity, access to drug libraries, use of appropriate models, and the use of TPPs to direct screening activities, is the A·WOL consortium, which focuses on drug discovery for filariasis.
A·WOL
Background
Lymphatic filariasis and onchocerciasis, which together infect more than 150 million people, are two NTDs included in the list of 10 NTDs targeted for elimination or control by 2020. Filariasis is one of the leading causes of global disability due to the severe pathologies that can present; lymphatic filariasis causes lymphedema, which can lead to elephantiasis, whereas onchocerciasis has severe skin manifestations and can cause blindness. Both diseases have benefited from mass drug administration (MDA) programs using donated drugs over decades.27,28 Nevertheless, meeting the goals of elimination has been hampered by several factors, including the lack of a safe macrofilaricide, which targets the long-lived adult worms.29,30
Similar to other parasitic infections, drug discovery for filariasis is hampered by the complexity of the life cycle, which includes insect intermediate hosts, and the consequent difficulty in testing potential drug candidates against the target organism. The standard screening strategy for anti-filarial drug discovery (WHO-TDR) begins with screening microfilariae from Onchocerca lienalis isolated from cattle skins and subsequent screens using adult worms and mouse and jird models. 31 The in vitro components of this pipeline have recently been part of a wider integrated screening strategy with other NTDs, and hits from a 10,000-compound library have been demonstrated. 32 Throughput for adult worm in vitro screens is relatively low, highlighted by the authors’ comment that it is difficult to screen more than 1000 compounds against adult worms in a year, because of the difficulty in sourcing parasite material. A microfilarial screen is thus used as a filter to remove general filariae-inactive compounds. The readout for both microfilariae and adult worm assays uses an assessment of motility by microscopic observation. The recent development of the WormAssay imaging system allows the automation of the measurement of motility, and this has been paired with automated liquid dispensing to create an adult worm in vitro screen with much higher throughput. 18 Again, the limiting factor is the number of adult worms that can be produced from animal hosts.
Targeting Wolbachia
One approach, which has delivered proof-of-concept for delivering macrofilaricidal activity, is to target the Wolbachia bacterial endosymbiont with antibiotics. 33 These bacteria are essential for multiple components of the nematode life cycle, including larval growth, development, embryogenesis, and, ultimately, survival of the adult worm, 34 making Wolbachia a valuable chemotherapeutic target. Removal of Wolbachia results in permanent sterilization and the protracted death of the adult worms, which ultimately delivers an excellent safety profile. Furthermore, by targeting Wolbachia, off-target species such as the related Wolbachia-free Loa loa are not affected, thus eliminating the risk of severe adverse events in relation to L. loa death that currently hampers delivery of MDA in co-endemic areas. 35
The benefits of an anti-Wolbachia macrofilaricidal drug would be to (1) reduce program time frames, (2) provide an alternative treatment for reduced efficacy or resistance to existing drugs, (3) be useable in L. loa co-endemic areas without risk of severe adverse events, (4) improve morbidity management, and (5) complement existing MDA strategies in “hot spot” foci or residual populations in MDA end-game scenarios, where test and treat strategies become more cost-effective and deliverable than MDA. All of these benefits are achievable using the antibiotic doxycycline, but the duration of treatment required and associated contraindications in children younger than 8 years and in pregnant women have prompted the search for a novel anti-Wolbachia drug. The A·WOL consortium is a group of academic laboratories and pharmaceutical industrial partners established in 2007 to discover and develop new and existing anti-Wolbachia drugs 36 (reviewed in Taylor et al. 33 ). One of the main objectives of the program has been to screen focused and diversity-based libraries for anti-Wolbachia activity, and given the difficulties associated with adult nematode screening, both in vitro and in vivo, a new approach was required to maximize throughput.
Anti-Wolbachia Screening
The first step of the A·WOL program was to develop a Wolbachia cell-based assay as a primary in vitro drug-screening tool. This was first validated in a 96-well format with a quantitative PCR readout to quantify the Wolbachia 16S rRNA gene copy number following treatment. 37 Using this primary screen, A·WOL has been able to screen in excess of 12,500 compounds from focused libraries, including registered drugs from the human pharmacopeia, NCEs, and natural products, against Wolbachia, delivering more than 640 hits, and this validated assay has been proven to be transferable to different research laboratories within the A·WOL consortium. Moreover, this assay has been further optimized and validated in an automated HCS assay using a 384-well format with a high-content imaging readout (Operetta; PerkinElmer, Waltham, MA) increasing throughput 10-fold (Taylor et al., unpublished data; Fig. 1 ). This assay development has further encouraged industrialization of this process through a collaboration between A·WOL and AstraZeneca as part of a shared commitment to the World Intellectual Property Organization’s WIPO RE:Search program against NTDs. 38 This open-access HTS project has created opportunities to access leading automation and screening technologies to screen a carefully curated chemical library of 1.8 million druglike and leadlike compounds to allow unprecedented access to drive hit discovery for these NTDs and others.
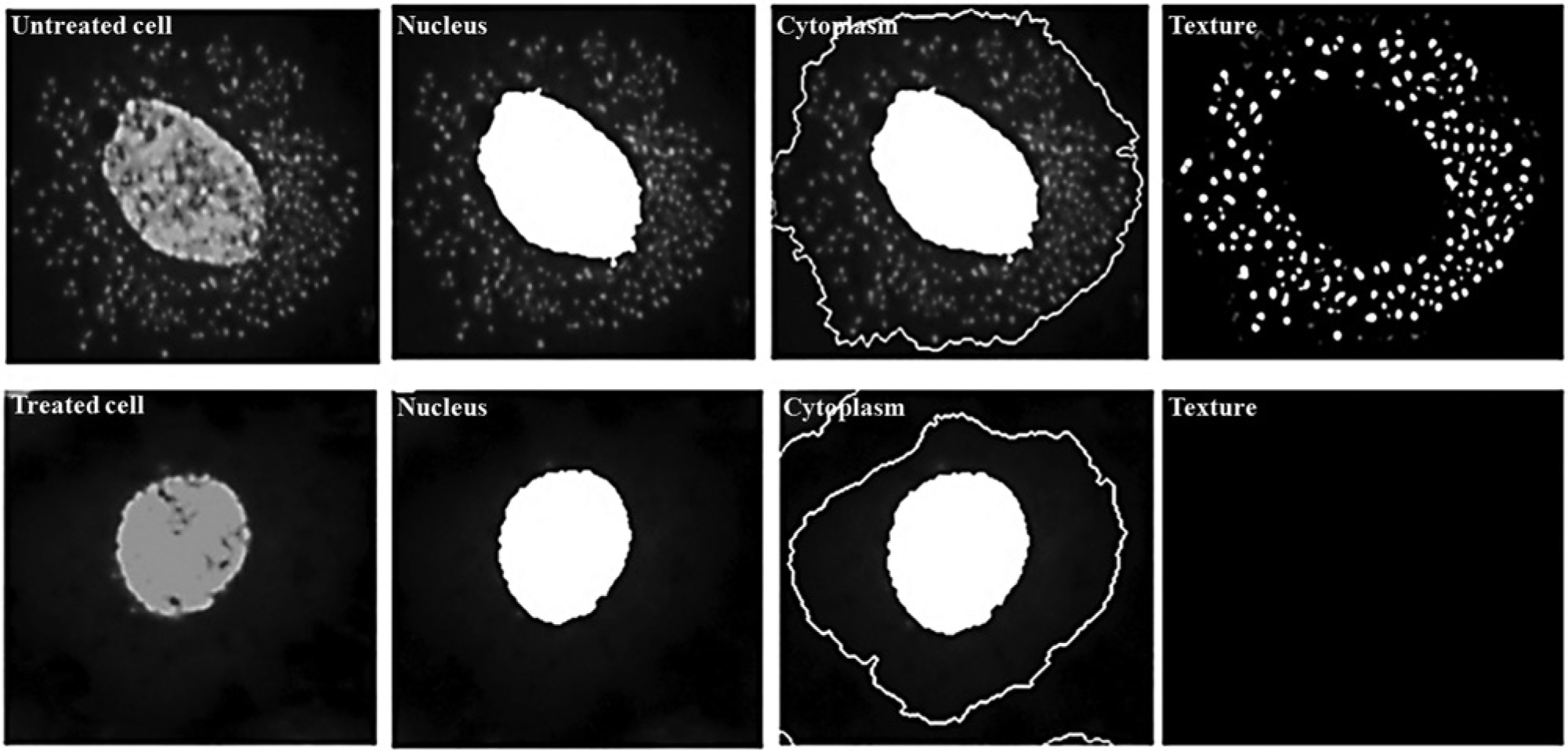
A·WOL cell-based screen. The top panel shows an example of an untreated cell containing Wolbachia (small spots), and the bottom panel shows a cell that has been cleared using a Wolbachia-active drug. High-content imaging software (Harmony/Operetta; PerkinElmer) is used to find cells based on the nuclei, find the surrounding cytoplasm, and then analyze the texture of the cytoplasm to define whether a cell is infected or uninfected.
A·WOL is now targeting analogs and near-neighbor chemistry of hit compounds to investigate the structure-activity relationship and screening of large diversity-based libraries (150,000- to 500,000-compound libraries) to expand the structural diversity of anti-Wolbachia chemotypes. These extensive screening activities have to date generated six independent lead chemotypes based on equivalent or improved potency over doxycycline in the in vitro and in vivo models (measured as absolute potency or duration of treatment to deliver Wolbachia elimination), chemical tractability, and prior experience with the chemical class. These lead series are now progressing through a rigorous lead optimization and candidate selection process as part of the A·WOL II Macrofilaricide Drug Discovery program, using iterative cycles of medicinal chemistry and biological testing to deliver at least one novel preclinical candidate and a chemically distinct backup, aligned with the A·WOL-established TPP for a new anti-Wolbachia–based macrofilaricide.
Hits from the primary in vitro cell-based screening assay are selected based on their efficacy against Wolbachia, reproducibility, and, if using registered drugs, the TPP as defined by A·WOL to include oral formulation and the safe use in children and pregnancy. These selected hits are then moved down the screening pipeline into both in vitro and in vivo nematode screening ( Fig. 2 ). In vitro nematode screening, using either adult male Onchocerca gutturosa 39 or B. malayi, 37 is performed to verify that hits are effective against nematode Wolbachia. For in vivo nematode screening, established animal models of filarial infection are used and include Litomosoides sigmodontis larvae in mice 40 and B. malayi adult worms in Mongolian jirds. 41 The primary in vivo screening model with L. sigmodontis allows for rapid screening of compounds and yields a visible and quantifiable phenotype of growth-retarded larvae. The secondary in vivo model with B. malayi uses a human filarial nematode and evaluates reduction of Wolbachia loads associated with macrofilaricidal activity and effects on female fertility. Both in vivo models measure reductions in Wolbachia load following treatment as their primary endpoint ( Fig. 2A ). Recently, the A·WOL program has further refined the screening funnel to maximize throughput ( Fig. 2B ) and validated an in vivo screening assay using the B. malayi infection in immunodeficient mice, which allows the testing of drug effects on both L3-L4 larval development and on adult worms (Turner and Taylor, unpublished data). This model requires less compound, is more rapid, and is more amenable to pharmacokinetic(PK)/pharmacodynamics (PD) analysis than the traditional jird model, with the benefit of linking efficacy and PK/PD in the same species. This validated screen is now being used as part of the A·WOL II Macrofilaricide Drug Development program to optimize combinations of registered anti-Wolbachia drugs.
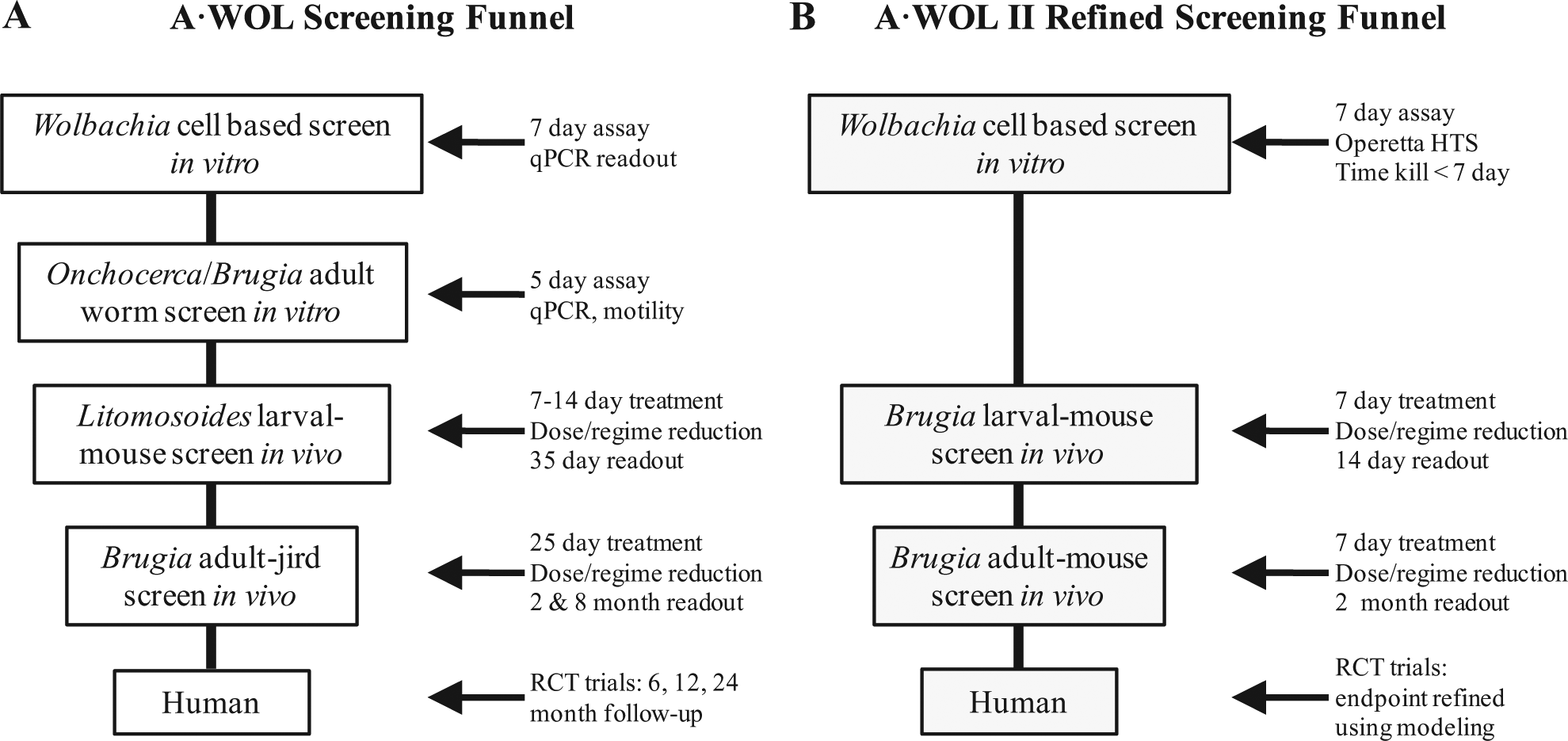
A·WOL screening funnels. Original funnel developed by A·WOL (
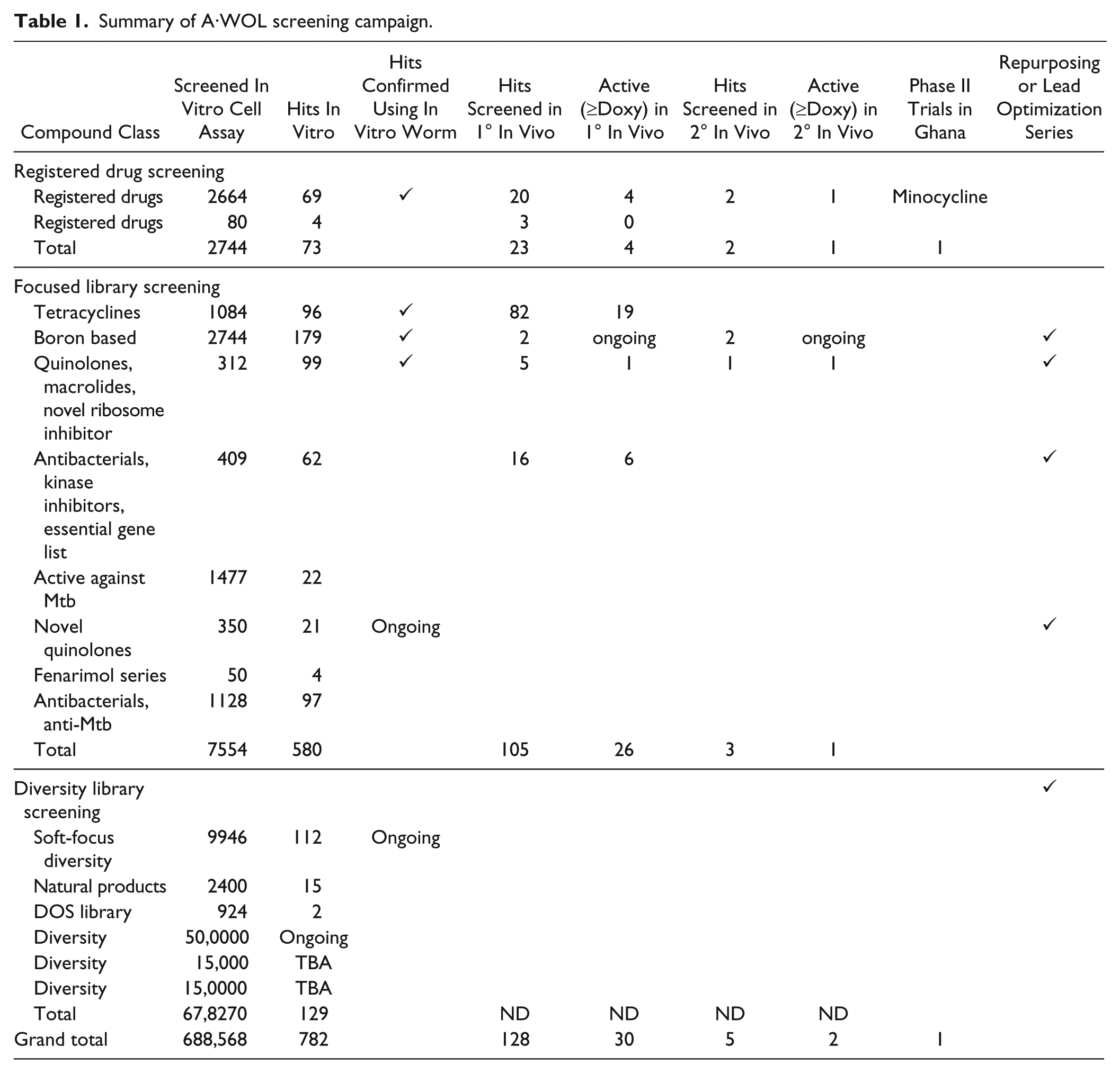
The A·WOL screening approach has included targeted focused drug libraries selected based on known and bioinformatically predicted essential gene targets. 42 Hits from focused library screening have yielded several lead compounds/drugs, which are progressing through the screening funnel. Target-based screening of validated targets, including 5′-aminolevulinic acid dehydratase43–45 and pyruvate phosphate dikinase, 46 has failed to deliver hits with sufficient potency or tractability compared with the whole-organism cell-based screen. The A·WOL approach to macrofilaricidal drug discovery by using a phenotypic Wolbachia assay has generated hundreds of hit compounds, which reproducibly translate with good efficacy throughout the screening pipeline ( Table 1 ).
Summary of A·WOL screening campaign.
The outputs from the initial A·WOL program are now under development as part of A·WOL II Macrofilaricide Drug Discovery & Development programs. Fifty hits from diversity library screening have undergone cheminformatic analysis to select the best hit series, representing six independent chemotypes. Three templates have been selected for hit-to-lead optimization, with an additional three backup templates. A·WOL is currently running a head-to-head evaluation of the three series with the intention of identifying the most promising template for final lead optimization.
The A·WOL approach has circumvented one of the main barriers to drug discovery for filariasis, which is common to many NTDs: screening throughput and capacity. The use of an anti-Wolbachia cell-based screen to filter active compounds into a streamlined in vivo cascade and aligning those actives against a well-defined TPP that addresses the needs of the target population improve the prospects for the discovery of a novel macrofilaricide. Further development of nematode-based cell lines and screening assays are under way to extend this option to direct macrofilaricidal drug discovery.
The London Declaration has served to place NTDs firmly on the global health agenda. It also acknowledged that, with the exception of guinea worm, further tools (drugs or diagnostics) are required to deliver the goals of elimination or control. Getting pharma to give open access to drug libraries to achieve this is an important and impressive achievement. However, if the goals of the NTD community are to be realized, further investment and recognition of the contribution of academic groups in terms of expertise domain with these complex organisms, and working in collaboration with industry to develop robust and relevant screening assays, is going to be essential to realize the opportunities presented by pharma reengaging with NTDs in producing the next generation of NTD drugs.
Footnotes
Acknowledgements
We thank the members of the A·WOL consortium for their contributions to the program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The A·WOL consortium is supported by a grant from the Bill and Melinda Gates Foundation awarded to the Liverpool School of Tropical Medicine.