
Abstract
Objective:
With rising numbers of adults seeking and receiving ADHD diagnoses, understanding their first-hand experiences of the diagnostic process is key for sensitive support and service design. This systematic review collates, evaluates and synthesises the existing evidence-base on lived experiences of adult ADHD diagnosis.
Method:
Keyword searches of six databases generated 10,357 citations, which were subjected to a systematic screening process that identified 21 relevant studies. Findings were analysed using thematic synthesis.
Results:
Analysis generated three overarching themes, elaborating how diagnostic experiences are shaped by adults’ Relationship with Self, Relationship with Others, and Relationship with Systems. Personally, diagnosis was widely experienced as a pivotal identity event, triggering biographical reflection that could foster greater self-compassion, but also grief, anger and identity confusion. Socially, diagnosis facilitated interpersonal understanding and communication, but also exposed adults to stigma and introduced dilemmas about diagnostic disclosure. Systemically, adults experienced the diagnostic process as beset by barriers and delays, and reported highly variable access to post-diagnosis supports or treatment.
Conclusion:
Results suggest receiving an ADHD diagnosis in adulthood is a complex relational process that can be both validating and destabilising, with variation in experiences resulting from individual biographies, interpersonal resources, stigma climates, and service structures.
Introduction
Traditionally conceptualised as a disorder of childhood, attention-deficit/hyperactivity disorder (ADHD) is now understood as a neurodevelopmental condition that frequently persists into adulthood (Song et al., 2021). Recognition of this life-course perspective in revised diagnostic criteria (Epstein & Loren, 2013), together with rising societal awareness of ADHD, has generated a marked increase in the number of adults pursuing and receiving ADHD diagnosis (Chung et al., 2019; London et al., 2025; McKechnie et al., 2023; Sasayama et al., 2022; Staley et al., 2024). Understanding this cohort’s experiences of the diagnostic process is crucial for ensuring sensitive service design and informing appropriate supports before, during, and after diagnosis. This article serves these ends by collating and synthesising existing evidence on adults’ first-hand experiences of receiving an ADHD diagnosis.
Epidemiological estimates suggest nearly 7% of adults have symptomatic ADHD, albeit with variance across countries and contexts (Song et al., 2021). However, across jurisdictions, a substantial proportion of adults who would meet diagnostic criteria remain undiagnosed (Ginsberg et al., 2014). Underdiagnosis is related to multiple factors, including limited awareness of adult ADHD among health professionals, stereotypes that frame ADHD as a disorder of hyperactive boys, and variability in symptom presentation across the lifespan (Asherson et al., 2016; Biederman, 2000; Turgay et al., 2012). Correspondingly, the likelihood of receiving a diagnosis differs across sociodemographic groups. For example, since female ADHD presentation can differ from traditional male-centric accounts of symptomatology (Williamson & Johnston, 2015), women are more likely to experience a delayed diagnosis - often after years of “camouflaging” or “masking” (i.e. deliberately modifying behaviour to hide ADHD traits (Attoe & Climie, 2023)). Individuals from ethnic minority and/or socioeconomically disadvantaged backgrounds may also face distinct barriers to diagnostic pathways (Bax et al., 2019). Moreover, many adults who are ultimately diagnosed with ADHD report previous contact with mental health services in which their difficulties were attributed to anxiety, depression, personality disorders, or other psychiatric conditions (O’Connor, Seery et al., 2022). Consequently, unrecognised ADHD is increasingly acknowledged as an important differential diagnosis within adult mental health care.
Growing public and professional awareness of adult ADHD has contributed to rising demand for adult diagnostic services, placing pressure on healthcare systems to respond effectively (Smith et al., 2024). Although clinical guidelines for diagnosing ADHD in adults exist in some jurisdictions, diagnostic practices vary substantially both within and between countries, resulting in uneven access to assessment (Ginsberg et al., 2014). In any service development, evidence regarding the lived experiences of individuals accessing those services is vital, for alignment with ethical guidelines that prioritise incorporation of expertise by experience (Gilfoyle et al., 2022; World Health Organisation, 2019), and ultimately delivering services of optimal benefit for end-users (Sartor, 2023).
Responding to the appetite for lived experience evidence, there is a burgeoning body of research that explores the first-hand perspectives of adults with ADHD (Attoe & Climie, 2023; Bjerrum et al., 2017; Ginapp et al., 2022; Long & Coats, 2022). Previous efforts to synthesise this literature have pinpointed diagnosis as a focal transition-point in people’s biographical trajectories, particularly when that diagnosis was delayed (Bjerrum et al., 2017; Ginapp et al., 2022; Long & Coats, 2022). However, the broad scope of previous reviews, which address the overall experience of living with ADHD as an adult (including, for example, symptom/treatment experiences of adults originally diagnosed as children), has inevitably limited the analytic depth with which adult diagnostic experiences specifically could be explored (Bjerrum et al., 2017; Ginapp et al., 2022). Two reviews have specifically probed experiences of adult-diagnosed ADHD, suggesting diagnosis’ key effects include access to specialist treatment, identity shifts, improved relationships, and emotionally ambivalent responses (Ginapp et al., 2022; Long & Coats, 2022). However, these reviews are rather small-scale, synthesising just 7 to 8 studies. This reflects limitations in coverage related to date (i.e. only research published before 2020, Attoe & Climie, 2023; Long & Coats, 2022); sample characteristics (e.g. just women Attoe & Climie, 2023); publication outlets (just three scientific databases, Attoe & Climie, 2023; Long & Coats, 2022); and/or method (e.g. exclusive qualitative focus (Long & Coats, 2022). A comprehensive and updated evidence synthesis specific to adult diagnostic experiences is an important and necessary step toward improving assessment practices and post-diagnostic care.
The present systematic review aimed to collate, evaluate and synthesise the existing research-base on the lived experiences, perspectives, and responses of individuals diagnosed with ADHD in adulthood. The review was guided by the research question: What characterises the lived experience of receiving an ADHD diagnosis in adulthood? The review sought to identify both points of convergence within the current evidence base and gaps that warrant further investigation.
Methods
A systematic review was completed in line with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) best-practice guidelines. The systematic review protocol was registered on PROSPERO (ref: CRD42024578269) in August 2024.
Search Strategy
The search strategy was designed in consultation with a specialist librarian. Initial searches took place using six databases (PsycINFO, PubMed, Scopus, Web of Science, EMBASE, CINAHL) in August 2024. Specialist journals and reference sections of the selected studies were manually searched for additional candidate papers.
A Boolean string was used to identify relevant articles, with search terms informed by prior research (Nayyar et al., 2025) and study aims:
“ADHD” OR “attention* deficit* and* hyperactivity* disorder” OR “attention* deficit* hyperactivity* disorder” OR “attention* deficit* disorder” * (Title & Abstract) AND adult* (Title & Abstract) AND diagnos* (Title & Abstract) AND experienc* OR perspective* OR attitud* OR recogni* OR receiv* OR realis* OR identif* OR satisfact* OR impact* OR barrier* OR facilitat* (Full text)
To reduce the number of irrelevant articles retrieved, the first three search terms were restricted to article titles and abstracts. Since initial scoping suggested much lived experience evidence was published as secondary findings rather than articles’ primary research focus, the final search term, tapping concepts related to lived experience, was widened to full text-searches.
Eligibility Criteria
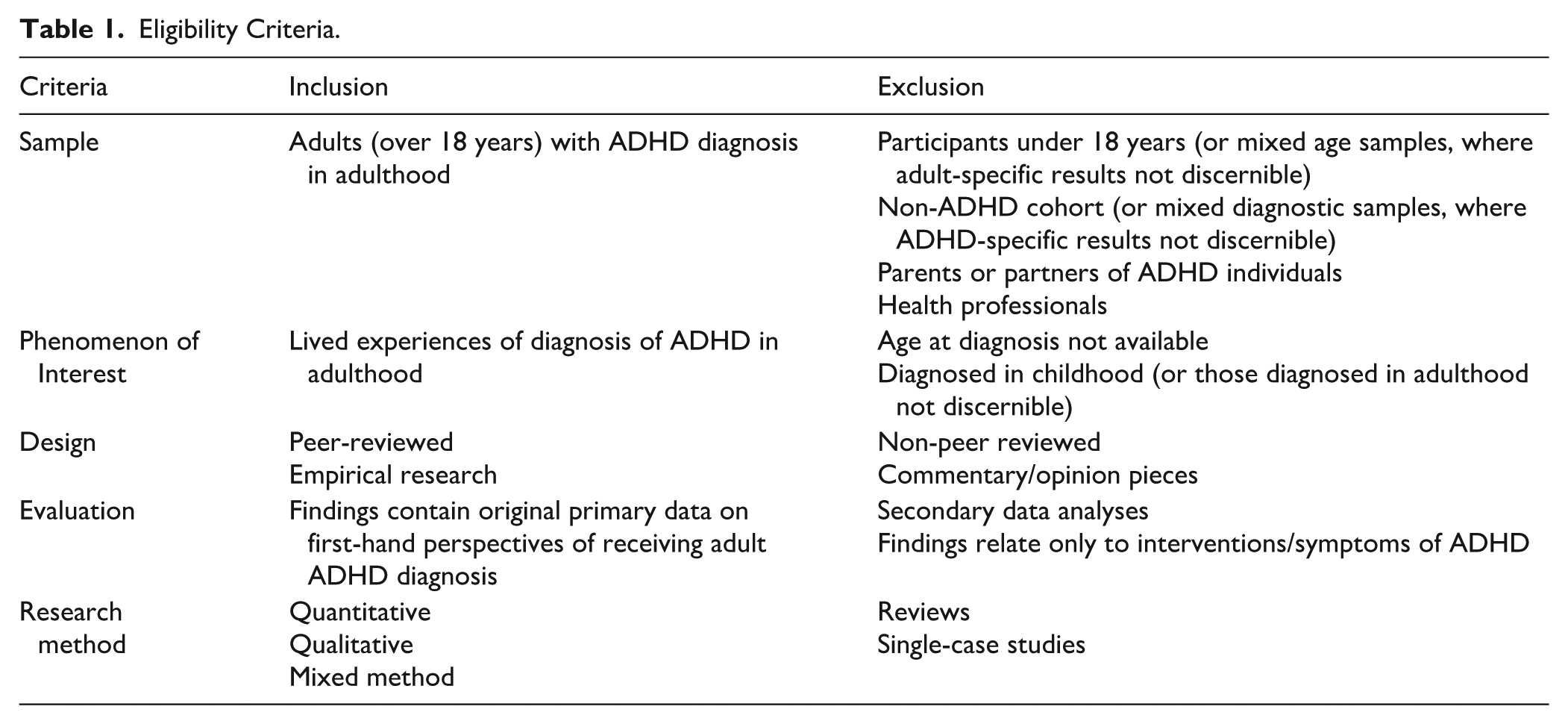
Inclusion and exclusion criteria are presented in Table 1. Team resources restricted the review to English-language publications, but no limits were set regarding publication date, research setting or methodological approach. Where studies partially met criteria (e.g. studies containing both child and adult participants, or ADHD and autism diagnoses), they were included only if the findings specific to the cohort of interest were separately identifiable in the results.
Eligibility Criteria.
Study Selection
All citations (n = 10,357) were imported into Covidence systematic review software. Duplicates were removed by Covidence (n = 6,430) or manually (n = 160), leaving 3,767 for screening. Two reviewers independently screened the titles and abstracts of all studies against predefined inclusion criteria (Table 1). Their decisions met established criteria (Landis & Koch, 1977) for “moderate” reliability (κ = 0.45); conflicts were resolved through discussion, erring on the side of including any disputed cases for further screening. Full texts for 102 studies were reviewed by both reviewers with ‘substantial’ (Landis & Koch, 1977) agreement (κ = 0.61). Where consensus about full-text eligibility was not reached (n = 8), an experienced third reviewer acted as tie-breaker.
Quality Appraisal
Since the review was open to all methods, the Mixed Methods Appraisal Tool (MMAT) was selected to assess study quality (Hong et al., 2018). The MMAT enables study rating on specific criteria, which facilitates evaluation of the strengths and weaknesses of specific studies and the literature as a whole. For example, qualitative studies are scored (“Yes” / “No” / “Can’t Tell”) according to whether: (1) there are clear research questions, (2) the collected data allow to address the research questions, (3) the qualitative approach is appropriate to answer the research question, (4) data collection methods are adequate to address the research question, (5) findings are adequately derived from the data, (6) the interpretation of results is sufficiently substantiated by data, (7) there is coherence between qualitative data sources, collection, analysis and interpretation. The MMAT discourages exclusion of low-scoring studies. Two independent raters used the MMAT to assess study quality. Raters agreed on 80.3% of judgements; the 19.7% that had initial disagreement (often due to one rater responding ‘No’ but the other ‘Can’t Tell’) were resolved by an experienced third reviewer acting as tie-breaker.
Data Extraction
Two reviewers independently extracted data relating to the study characteristics, participant information, and methods. Any findings relating specifically to the lived experience of receiving an ADHD diagnosis as an adult were also extracted. Data were charted in a separate data extraction form, designed based on Cochrane guidance (Noyes et al., 2023). Both reviewers’ extracted data were examined to ensure consensus; any disparities were resolved through discussion, with the aim of including maximal data in the final review.
Data Synthesis
Any part of studies’ Results/Findings sections, which directly pertained to the review research question, was extracted and imported into NVivo for thematic synthesis. The unit of coding was a meaningful segment of text (i.e. sentence or short passage) that conveyed a distinct idea relevant to the review question. In original qualitative studies, author-defined themes/patterns were not treated as fixed units of analysis: where an original theme contained multiple ideas, these were coded separately and could contribute to different themes in the synthesis. This allowed findings to be summarised across studies on the basis of conceptual meaning for the review research question.
Following Popay et al.’s (2006) guidelines, one researcher conducted a first round of inductive coding, iteratively refining a coding frame containing 56 descriptive codes (e.g. “Feeling different,” “Self-acceptance”). The coding frame organised codes according to whether they captured aspects specific to before-, during-, or after-diagnosis experiences. After developing a first draft of code labels and definitions, a second reviewer independently coded three quarters of the data, with coding patterns compared using NVivo’s Coding Comparison Query (O’Connor & Joffe, 2020). 44% of codes met accepted criteria for “almost perfect” reliability (κ > .8) and 36% ‘substantial’ reliability (κ > .6). Codes with “moderate” reliability (κ = .41–.6) were more tightly defined and four codes with κ > .4 were discarded prior to final coding. Following final coding, the analytic focus broadened to the level of themes, with code content and relationships reviewed in team discussion to distinguish higher-level analytic patterns.
Results
Retrieved Studies
As shown in Figure 1, initial searches retrieved 10,357 articles. Following removal of duplicates, 3,767 were taken forward for title/abstract screening and 102 for full-text screening. The screening process ultimately produced 21 studies that met inclusion criteria.
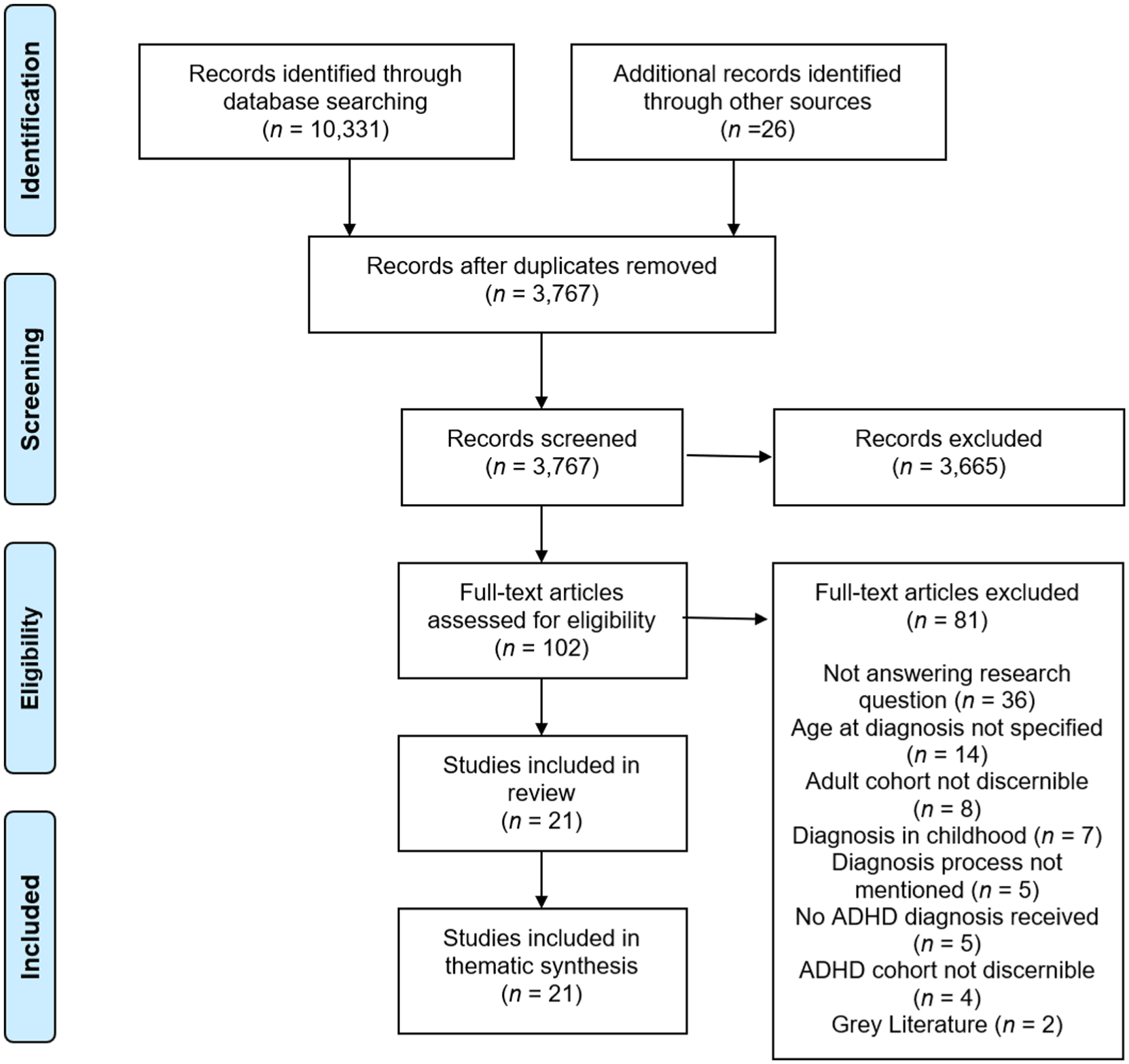
PRISMA flow diagram (Moher et al., 2009).
Study Quality
Study MMAT scores are available in Supplemental Material. The average total score was 6.5/7, with only one paper scoring lower than 5/7. All papers were deemed to have an appropriate analytic method and methodological coherence, with the vast majority exhibiting adequate data and substantiated results. The most frequently identified flaw (28.5%) pertained to absence of clear research questions.
Study Characteristics
Individual study characteristics are available in Supplemental Material. Studies contained data from a total of 397 participants, with sample sizes ranging from 3 to 71. Participant ages spanned the lifespan from 18 to 91 years. Of the 227 participants whose gender was specified, 161 (71%) were female. Participant nationality was unevenly reported, but identified cohorts were mostly from European or English-speaking countries (such as United States, United Kingdom, Australia). Race/ethnicity data were sparsely reported but suggested predominantly White/Caucasian participants. Most studies established diagnostic status through participant report; two additionally verified participants met diagnostic thresholds using standardised scales, while two recruited participants with confirmed diagnoses from clinical settings.
All data relevant to the research question were qualitative. While two studies were described as mixed-methods, the quantitative data presented were not relevant to the research question so not extracted. Data collection methods included interviews, focus groups, and internet posts. Studies employed a range of analytic techniques, most commonly thematic analysis, grounded theory and interpretive phenomenological analysis.
Thematic Synthesis
The thematic synthesis identified three overarching themes, each composed of 2 to 3 subthemes (Figure 2). Lived experiences of ADHD diagnosis could be understood in terms of its impact on adults’ Relationship with Self, Relationship with Others, and Relationship with Systems. These are outlined below, supported by illustrative participant quotes extracted from the papers.
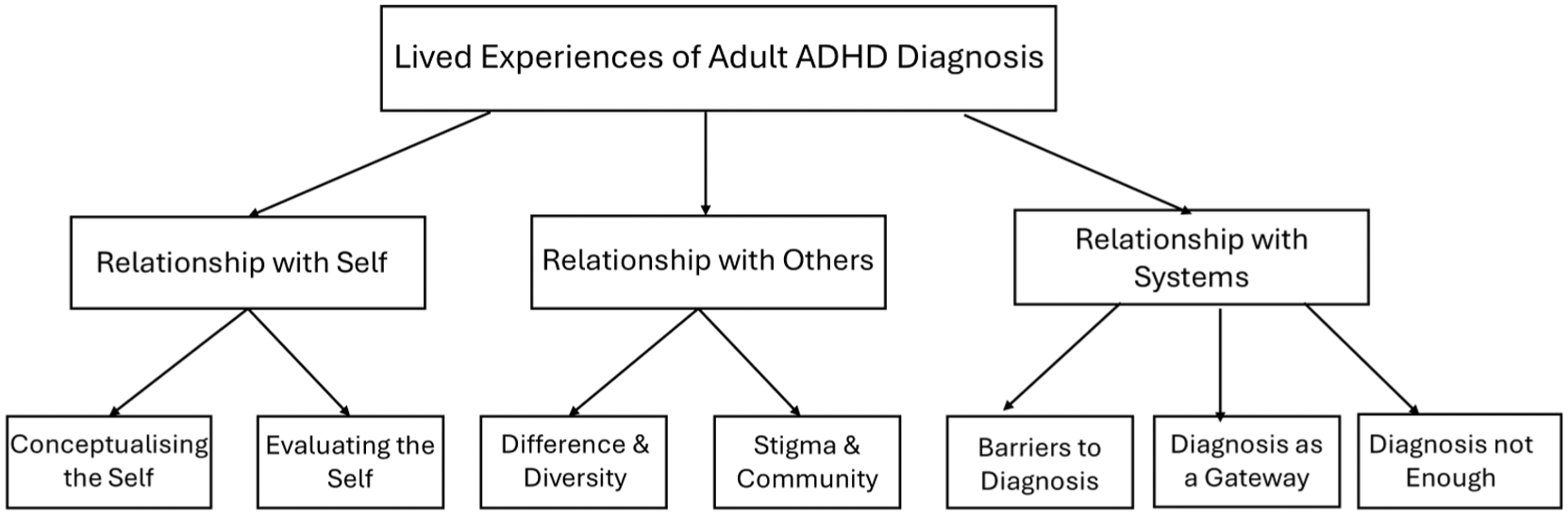
Thematic network.
Theme 1: Relationship With Self
Conceptualising the Self
Identity was a recurrent concern throughout participants’ accounts. Many participants characterised the journey of receiving an ADHD diagnosis in terms of exploration, clarification and transformation of their self-concept. Self-recognition via hearing about ADHD (Brod et al., 2012; Holthe & Langvik, 2017; Morgan, 2024) or learning a family-member had been diagnosed (Brod et al., 2012; Fleischmann & Fleischmann, 2012; Ghosh et al., 2016; Miller & Fleischmann, 2024; Morgan, 2024; Stenner et al., 2019; Toner et al., 2006; S. Young et al., 2008) triggered a ‘lightbulb moment’ that demarcated the start of their ADHD identity (Stenner et al., 2019).
I feel as though a new me has been born with my adult ADD diagnosis. (Fleischmann & Fleischmann, 2012)
The diagnosis itself carried a strong sense of revelation. Participants positioned the diagnosis as enabling new understanding of one’s life, illustrated in metaphors such as: the “curtain had been raised and my life makes sense now” (Morgan, 2024). While the diagnosis did not eliminate ADHD or its associated difficulties, it afforded explanation and validation of many participants’ challenges (Nielsen, 2018).
Actually, having a list of things that I find difficult – and now there is a reason why I find them difficult. . . I’m allowed to find it difficult – I’ve got ADHD (Z. Young et al., 2019)
Many participants engaged in biographical reflection on their past, with the diagnosis positioned as the point where “all the precursors of my story had converged” (Aoki et al., 2020). Almost all studies reported participants describing new retrospective insights into childhood and early life (Aoki et al., 2020; Brod et al., 2012; Fleischmann & Fleischmann, 2012; French & Cassidy, 2024; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Miller & Fleischmann, 2024; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2017, 2018; Sander-Williams, 2024; Stenner et al., 2019; Tal & Goodman, 2025; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Before diagnosis, individuals had often attributed difficulties to their own deficiencies, endorsing unfavourable labels ascribed by others or gleaned through social comparison (Fleischmann & Fleischmann, 2012; Holthe & Langvik, 2017; Miller & Fleischmann, 2024; Morley & Tyrrell, 2023; Stenner et al., 2019; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Diagnosis was described as triggering a process of “reauthoring” (Morgan, 2024), whereby individuals actively engaged in shedding unhelpful labels and reconstructing biographical narratives (French & Cassidy, 2024; Morley & Tyrrell, 2023; Stenner et al., 2019; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019).
It has effectively allowed me to just be me, so I would actually say it is freeing to a great degree. Because now I can say, this is the way I am (Z. Young et al., 2019)
Most studies described participants who believed the diagnosis facilitated greater acceptance of themselves and their experiences (Aoki et al., 2020; Fleischmann & Fleischmann, 2012; French & Cassidy, 2024; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2018; Sander-Williams, 2024; Stenner et al., 2019; Tal & Goodman, 2025; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). However, integrating the diagnosis into one’s self-concept could be cognitively challenging, particularly in maintaining a sense of continuity of one’s identity (Aoki et al., 2020; Hansson Halleröd et al., 2015; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2017, 2018; Stenner et al., 2019; Z. Young et al., 2019). Some found it difficult to separate the aspects of their identity that were relevant to vs. independent of ADHD (Aoki et al., 2020; Hansson Halleröd et al., 2015; Z. Young et al., 2019), with some concern about a tendency to “over-interpret” all aspects of their experience through the ADHD lens (Hansson Halleröd et al., 2015). The shifting ground of identity could be destabilising, prompting questions such as “who am I really?” (Aoki et al., 2020) or “who is the real me?” (Z. Young et al., 2019).
The more I learned about ADHD, the more I doubted who I was. . . Are my assumptions about myself so far, all wrong? I started to feel anxious. (Aoki et al., 2020)
The post-diagnosis evolution of self-concept was inherently emotional. Over half of the studies reported participants experiencing relief following diagnosis (Aoki et al., 2020; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2018; Sander-Williams, 2024; Tal & Goodman, 2025; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Relief was often linked to the aforementioned diversion of blame for one’s challenges from personality or character flaws to a recognised neurological condition (Aoki et al., 2020; Fleischmann & Fleischmann, 2012; French & Cassidy, 2024; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Nielsen, 2018; Tal & Goodman, 2025; S. Young et al., 2008; Z. Young et al., 2019).
For me, there was a lot of relief. I mean, I had spent my whole adult life thinking that I just wasn’t good enough. . .so hearing that it wasn’t just me and there is something else going on, I guess, yeah, it was a huge relief. (Morley & Tyrrell, 2023)
Yet the process of reconceptualising the self also triggered negative emotions. Frustration, disappointment, and anger (Hansson Halleröd et al., 2015; Morgan, 2024; S. Young et al., 2008) were triggered by the “lost time” (Hansson Halleröd et al., 2015; Z. Young et al., 2019) caused by delayed diagnosis. The post-diagnosis identity could also elicit sadness at acquiring a label connoting disorder (Holthe & Langvik, 2017; Toner et al., 2006); grief for their old pre-diagnosis self (Z. Young et al., 2019); and anxiety or hopelessness at the apparent permanence of their challenges (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Tal & Goodman, 2025; S. Young et al., 2008; Z. Young et al., 2019).
Due to these complexities, adjustment to the ADHD diagnosis was highly individualised and not linear (Aoki et al., 2020; Holthe & Langvik, 2017; Nielsen, 2018; Z. Young et al., 2019). The process of absorbing the diagnosis could take some time, and perspectives on its meaning could vary on a continual basis (Aoki et al., 2020; Morley & Tyrrell, 2023; Nielsen, 2018; Stenner et al., 2019; Tal & Goodman, 2023; Toner et al., 2006; Z. Young et al., 2019). While some participants immediately accepted that they had ADHD (Aoki et al., 2020; Stenner et al., 2019; S. Young et al., 2008), others recounted a period of doubt or denial about the diagnosis’ accuracy (Aoki et al., 2020; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Sander-Williams, 2024). This was sometimes resolved after learning more about ADHD (Nielsen, 2017; Z. Young et al., 2019). However, the specific ways ADHD was presented or conceptualised shaped responses in divergent directions. For instance, biological construals of ADHD struck some as validation of their difficulties and legitimation of their difference (Holthe & Langvik, 2017; Morgan, 2024; Nielsen, 2017); but others as fatalistic prognoses (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Tal & Goodman, 2025; Z. Young et al., 2019) of “a bad disease that I can never cure” (Holthe & Langvik, 2017).
Evaluating the Self
Across studies, individuals recounted a lifetime of negative self-image and poor self-esteem. Participants described themselves in terms such as “failed human” (French & Cassidy, 2024) or “faulty human being” (Z. Young et al., 2019). They attributed this poor self-worth to undiagnosed ADHD, which was equated with persistent struggle, perceived under-achievement, and negative feedback or pejorative name-calling from others (Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Matheson et al., 2013; Miller & Fleischmann, 2024; Morgan, 2024; Morley & Tyrrell, 2023; Stenner et al., 2019; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008). In the absence of diagnosis, individuals had internalised negative judgements of others (Fleischmann & Fleischmann, 2012; Holthe & Langvik, 2017; Matheson et al., 2013; Miller & Fleischmann, 2024; Morley & Tyrrell, 2023; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019).
I always thought that what they said about me during childhood was right, that I WAS stupid, nothing, unworthy, and that’s what my brothers thought of me. In the past I felt inferior, worthless, I really wanted to learn and succeed but I couldn’t understand why I always failed. (Miller & Fleischmann, 2024)
Numerous studies cast the diagnosis as enabling a shift towards more favourable self-evaluation (Ginapp et al., 2023; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Morley & Tyrrell, 2023; Toner et al., 2006; Z. Young et al., 2019). Participants implied that objectification of one’s difficulties into the defined entity of ADHD helped to insulate self-image from one’s failures (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Nielsen, 2017, 2018; Stenner et al., 2019; Tal & Goodman, 2023; S. Young et al., 2008; Z. Young et al., 2019), removing the self-recrimination to which they were previously susceptible (Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Nielsen, 2017, 2018; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Following the diagnosis, participants reported being less inclined to self-directed anger and judgment (Sander-Williams, 2024), cultivating more compassion in their self-assessments (Fleischmann & Fleischmann, 2012; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2018; Stenner et al., 2019; Z. Young et al., 2019).
The capacity for self-forgiveness . . . letting go of all the negative feelings you’ve been carting around about yourself for all these years.” (Fleischmann & Fleischmann, 2012)
Moreover, the diagnosis, and exposure to neurodiversity discourses that characterise ADHD as natural variation rather than deficit, served as the basis for some individuals to elaborate a distinctly celebratory self-concept. In seven studies, participants actively focused on strengths they associated with ADHD, such as creativity, quick thinking, passion, and capacity for multi-tasking (Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Miller & Fleischmann, 2024; Tal & Goodman, 2023; Z. Young et al., 2019). This new self-belief facilitated forward-looking confidence and hope for the future (Fleischmann & Fleischmann, 2012; Morgan, 2024; Toner et al., 2006; S. Young et al., 2008).
[I’m] feeling very empowered and ready for the next part of my life (Fleischmann & Fleischmann, 2012)
Though typical, this journey from impaired to empowered self-concept was not universal. Some studies depicted a minority who reported maintaining positive self-esteem prior to diagnosis, often through strategies such as focusing on their strengths, developing resilient coping mechanisms, and ignoring negative feedback (Henry & Hill Jones, 2011; Miller & Fleischmann, 2024; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008). Another minority position construed previous struggles as beneficial despite their unpleasantness, since they provided evidence of strength and resilience that buffered their self-image (Stenner et al., 2019; Z. Young et al., 2019). Gratification at having received the diagnosis was linked with its retrospective amplification of the challenges they had faced, and hence the achievement of surmounting them (Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; S. Young et al., 2008).
I’m grateful that I got it [the diagnosis] in the end . . . I’ve been searching for my entire life and trusted that someone would finally understand that something isn’t right (Hansson Halleröd et al., 2015)
Theme 2: Relationship With Others
Difference & Diversity
Across studies, participants reported feeling “different, unusual” (Henry & Hill Jones, 2011) prior to receiving the ADHD diagnosis (Aoki et al., 2020; Brod et al., 2012; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Morgan, 2024; Morley & Tyrrell, 2023; Sander-Williams, 2024; Stenner et al., 2019; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). This sense of difference from others had been intuited from personal experiences of disconnection, and reinforced by other people (often family, friends or teachers) comparing them unfavourably to peers or siblings (Fleischmann & Fleischmann, 2012; Holthe & Langvik, 2017; Matheson et al., 2013; Miller & Fleischmann, 2024; Sander-Williams, 2024; Stenner et al., 2019; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Others’ lack of empathy or understanding was often conveyed through pejorative labels, such as “lazy” or “stupid” (Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Morgan, 2024; S. Young et al., 2008).
The diagnosis did not erase this sense of social difference; indeed, the diagnosis could amplify the sense of difference already felt. The subjective meaning of this difference changed, however: having an apparent reason for one’s divergence was felt to legitimise it (Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Nielsen, 2017; Tal & Goodman, 2023; Toner et al., 2006; Z. Young et al., 2019).
Yes, it is unfair, but at least now I know and I don’t feel like a fool when I’m putting in the same amount [of effort] and not getting the same results. (Z. Young et al., 2019)
Nevertheless, appreciating the source of one’s perceived difference necessitated sometimes difficult decisions. Some ruled themselves out of, or experienced others advising them against, particular opportunities or ambitions, due to a belief they were unsuited to someone with ADHD. This bred a sense that people with ADHD were different not just in day-to-day functioning, but in future life-prospects.
They told me it would be very difficult for me to have a management position . . . I’m not like everyone else, I have ADHD, I might not manage this because that’s what everyone around me and my psychologists are saying (Hansson Halleröd et al., 2015)
Social difference was not always a negatively valanced property, however. Three studies showed participants celebrating the principle of neurodiversity, embracing their uniqueness and the original perspective it offered them (Nielsen, 2017; Stenner et al., 2019; Tal & Goodman, 2023).
It’s having a colored TV, while everyone else sees life in black and white (Tal & Goodman, 2023)
Stigma & Community
Stigma was frequently identified as an important variable impacting responses to diagnosis (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Morley & Tyrrell, 2023; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Specific named manifestations of stigma included misconceptions/misinformation about ADHD, and ADHD’s trivialisation and/or sensationalism in popular media (Holthe & Langvik, 2017; Morley & Tyrrell, 2023; Toner et al., 2006). Some participants had internalised these cultural narratives into self-stigma (Hansson Halleröd et al., 2015; Morgan, 2024; Z. Young et al., 2019). Self-stigma fostered trepidation about the diagnosis due to fears about devaluation and restricted life opportunities (Hansson Halleröd et al., 2015).
It was knowing that it was right but wishing that it wasn’t. It fit completely, but at that stage I felt a kind of a stigma towards it and I don’t know where that came from other than the fact it was classed as a disorder, an illness, or whatever, a condition and that in itself puts a stigma on it. (Z. Young et al., 2019)
Stigma emerged as a key factor in decisions about revealing one’s diagnosis to others (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019). Some feared diagnostic disclosure would trigger differential treatment, judgement and discrimination (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morley & Tyrrell, 2023; Toner et al., 2006; S. Young et al., 2008). There were also concerns that their diagnosis would be disbelieved or deemed an excuse for underachievement (Holthe & Langvik, 2017; Z. Young et al., 2019).
I think that people think ADHD is sort of a made-up excuse for being unfocused and undisciplined, that it just takes self-control or something. I don’t think that people think ADHD is as real as anxiety and depression (Holthe & Langvik, 2017)
Worry about skeptical reactions to diagnostic disclosure was salient for this late-diagnosed cohort, many of whom were women whose profile or presentation diverged from prevailing ADHD stereotypes (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Morley & Tyrrell, 2023).
their picture of ADHD is something else. . . I don’t fit into their picture (Hansson Halleröd et al., 2015)
Such concerns necessitated a careful decision-making process about whether to disclose the diagnosis to others (Z. Young et al., 2019). Stigma-based fear meant some chose to continue masking their difficulties (Ginapp et al., 2023; Toner et al., 2006). Masking was generally described as cognitively taxing and emotionally exhausting, and linked with mental health difficulties and a sense of “inauthenticity” (Morgan, 2024; Sander-Williams, 2024; Toner et al., 2006).
Participants described their lives prior to diagnosis as prone to interpersonal challenges, including isolation and difficulties forming and maintaining relationships (Fleischmann & Fleischmann, 2012; Henry & Hill Jones, 2011; Matheson et al., 2013; Morgan, 2024; Morley & Tyrrell, 2023; Sander-Williams, 2024; Toner et al., 2006). Many observed improved relationships following diagnosis, which offered a means of communicating and helping others understand their experience (Aoki et al., 2020; French & Cassidy, 2024; Hansson Halleröd et al., 2015; Morgan, 2024; Z. Young et al., 2019). Participants acknowledged and appreciated the ongoing support of family, friends and partners (Aoki et al., 2020; Holthe & Langvik, 2017; Morley & Tyrrell, 2023; Z. Young et al., 2019). Moreover, the diagnosis proved the basis for some to build new relationships. Five studies recorded participants benefiting from entry into an “ADHD community,” where they could share experiences and knowledge with similar others (Fleischmann & Fleischmann, 2012; French & Cassidy, 2024; Holthe & Langvik, 2017; Toner et al., 2006; Z. Young et al., 2019).
How important community is and finding other ADHD people. Because I felt so lonely all my life, I felt so different and I just felt like I was just a failure and a weirdo [. . .] And just finding other people that just get you [. . .] we get each other (French & Cassidy, 2024)
Theme 3: Relationship with Systems
Barriers to Diagnosis
Most studies recorded experiences of barriers and delays to accessing an adult ADHD diagnosis. While studies crossed multiple jurisdictions, recurrent issues included inaccessible pathways to specialist services (Matheson et al., 2013; Morgan, 2024) and poor understanding of ADHD and best practice guidelines among health professionals (Morgan, 2024; Toner et al., 2006; Z. Young et al., 2019). Adult diagnostic services were not available in all areas, and where they existed often involved long wait times (Brod et al., 2012; Morgan, 2024; Morley & Tyrrell, 2023; Stenner et al., 2019; Z. Young et al., 2019)
seeking medical care as a person with ADHD is not ADHD friendly (Morgan, 2024)
Approximately half of studies made reference to participants receiving other diagnoses prior to ADHD (Aoki et al., 2020; Brod et al., 2012; French & Cassidy, 2024; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Matheson et al., 2013; Morgan, 2024; Morley & Tyrrell, 2023; Stenner et al., 2019; Toner et al., 2006). Many participants reported previous engagements with child or adult mental health services, which did not identify ADHD as a concern (Fleischmann & Fleischmann, 2012; Matheson et al., 2013; Morgan, 2024). Co-occurring mental health difficulties were common, and numerous participants had also been diagnosed with mood or anxiety disorders (Holthe & Langvik, 2017; Morgan, 2024; Morley & Tyrrell, 2023; Toner et al., 2006). Multiple women expressed concerns that gender-based stereotyping made them particularly vulnerable to misdiagnosis or missed diagnosis (French & Cassidy, 2024; Holthe & Langvik, 2017; Morgan, 2024). Participants differed in how they understood the relationships between ADHD and other diagnoses. Some saw these as genuinely comorbid disorders, with the other disorder perhaps overshadowing ADHD symptoms and contributing to diagnostic delay; others saw mood and anxiety disorders as secondary consequences of undiagnosed ADHD; others saw the non-ADHD diagnoses as straightforward errors or misdiagnoses (Aoki et al., 2020; Brod et al., 2012; Ginapp et al., 2023; Holthe & Langvik, 2017; Matheson et al., 2013; Morgan, 2024; Morley & Tyrrell, 2023).
I think that was why my ADHD got missed as the focus was always on my binge-eating, my alcohol use, and my self-harm and I suppose, for me, that was the right thing to do, maybe, as the interventions that I had probably saved my life (Morgan, 2024) if they had just dug a bit deeper, they would have seen that what they thought was anxiety was me trying to control my ADHD, trying to deal with the stress that having ADHD causes. So yes, I was anxious, but it was because of my ADHD and because they focused only on the anxiety, they missed the ADHD (Morgan, 2024) Although I had been dealing with my difficulties as indications of other diseases for a long while, all my past experiences could be explained by ADHD. (Aoki et al., 2020)
Barriers to diagnosis continued to emerge even when participants had reached the stage of clinical assessment. Numerous participants reported feeling unheard, misunderstood, or dismissed for inconsistency with stereotypical ADHD profiles (Morgan, 2024; Morley & Tyrrell, 2023; Tal & Goodman, 2023). However, others had more positive experiences, painting the diagnostic process as one of the first settings where there they felt validated (Morgan, 2024; Stenner et al., 2019).
Diagnosis as a Gateway
For many, diagnosis marked an important transition-point in terms of practical resources and entitlements. The diagnosis served as a gateway for access to specialist supports and treatment options (Hansson Halleröd et al., 2015; Miller & Fleischmann, 2024; S. Young et al., 2008). Such resources included clinical treatment (Brod et al., 2012; Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Matheson et al., 2013; Morley & Tyrrell, 2023; Nielsen, 2017; S. Young et al., 2008), coping skill development (Aoki et al., 2020; Fleischmann & Fleischmann, 2012; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Morley & Tyrrell, 2023; Nielsen, 2017, 2018; Toner et al., 2006) and environmental adaptations (Aoki et al., 2020; Ginapp et al., 2023; Hansson Halleröd et al., 2015; Miller & Fleischmann, 2024; Toner et al., 2006). These supports were generally positively appraised, helping adults manage stressors and improve educational and occupational performance (Aoki et al., 2020; Ginapp et al., 2023; Miller & Fleischmann, 2024; Morley & Tyrrell, 2023; Toner et al., 2006; Z. Young et al., 2019).
A further consequence of the diagnosis, raised in most studies, was access to stimulant medication (Aoki et al., 2020; Brod et al., 2012; Fleischmann & Fleischmann, 2012; Ghosh et al., 2016; Hansson Halleröd et al., 2015; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2017, 2018; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008; Z. Young et al., 2019) . Most who had tried medication viewed its impact on their lives as positive, reporting it helped ease the burden of ADHD and mitigate its secondary impacts on their mental health (Aoki et al., 2020; Fleischmann & Fleischmann, 2012; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Morgan, 2024; Morley & Tyrrell, 2023; Nielsen, 2018; Tal & Goodman, 2023; Toner et al., 2006; S. Young et al., 2008).
It [pharmacological treatment] felt like doors were opening all over my mind, things were clear, my thoughts weren’t so scattered, and I felt alive. (Fleischmann & Fleischmann, 2012)
However, a minority expressed disappointment in the side-effects or long-term efficacy of medication, particularly when it was offered as a standalone treatment (Holthe & Langvik, 2017; Matheson et al., 2013; Morgan, 2024; Nielsen, 2017, 2018; S. Young et al., 2008).
Diagnosis not Enough
In some studies, participants lamented that the diagnosis marked the end, rather than beginning, of their engagement with specialist services. Having received the diagnosis, support in understanding and acting on that new knowledge was sometimes acquired from online forums and social media rather than clinical services (Morgan, 2024; Sander-Williams, 2024). An inaccessibility or non-existence of adult services in some jurisdictions left individuals feeling distressed and helpless (Matheson et al., 2013; Toner et al., 2006). Some participants reported that the diagnosis was not succeeded by any follow-up, help or treatment (Hansson Halleröd et al., 2015; Morgan, 2024; Sander-Williams, 2024; Toner et al., 2006).
Then [after being diagnosed] they just dismissively sent me away with nothing. (Hansson Halleröd et al., 2015)
For some who did receive post-diagnostic support, available interventions were primarily medical in nature (Matheson et al., 2013; Morgan, 2024; Nielsen, 2017). Some individuals’ post-diagnostic support comprised only a prescription for medication, with no further avenue for professional advice or psychological therapy (Hansson Halleröd et al., 2015; Morgan, 2024; Toner et al., 2006). Others received some follow-up care until their medication was deemed stable, at which point regular support ceased (Morgan, 2024). Numerous participants articulated a desire for a more holistic approach to care, with particular focus on psychosocial support (Hansson Halleröd et al., 2015; Matheson et al., 2013; Morgan, 2024).
Discussion
Recent years have seen growing acknowledgement of the lifelong course of ADHD, rising prevalence of diagnoses ascribed in adulthood, and increasing momentum behind the development of adult-specific assessment and support services. In this context, the present evidence synthesis is timely, offering a valuable resource for researchers, clinicians, policymakers, and adults at various points of the diagnostic pathway. Results showed that, far from a self-contained clinical classification, diagnosis was a highly relational experience. Responses to diagnosis were shaped by existing relationships with self, others, and systems; while the new diagnosis reconfigured each of those relationships in turn. For individuals at the centre of these relational networks, diagnosis could present both challenges and benefits.
This review collates the most comprehensive evidence-base to date regarding the experience of receiving a diagnosis of ADHD in adulthood. Prior reviews of experiences specific to adult-diagnosed ADHD included just 7 to 8 studies (Attoe & Climie, 2023; Long & Coats, 2022). Reflecting expansion of included databases, populations, methods, and timespans, the current review synthesised nearly three times as many studies. Notably, one-third of included studies postdated the literature synthesised in prior reviews, whose evidence-base ended in 2020 (Attoe & Climie, 2023; Long & Coats, 2022). This evidences both the current momentum in this research space and the timely nature of this review. While certain findings echo those identified in previous syntheses, affirming the consistency of these trends (Attoe & Climie, 2023; Bjerrum et al., 2017; Ginapp et al., 2022; Long & Coats, 2022), the expanded evidence-base considered in this review adds nuance and extends insights regarding experiences of adult ADHD diagnosis.
The first theme identified by the thematic synthesis highlighted wide empirical consensus that implications for self-concept and identity lay among the most personally salient aspects of diagnostic experiences. Across studies, receiving a diagnosis was described as a profound turning-point in individuals’ self-understanding, spurring both cognitive and emotional reappraisal of the self. Consistent with research on other psychiatric diagnoses (Downey et al., 2025; Nayyar et al., 2025; O’Connor, Seery et al., 2022), self-recognition in the diagnosis catalysed a process of biographical ‘reauthoring’ (Morgan, 2024), with participants reinterpreting their life history through a new lens. Many studies documented a retrospective shift in attribution patterns, with the diagnosis diverting blame for perceived failures from personal inadequacies to a neurological condition. Often, this fostered greater self-compassion, and a shift from impaired to improved self-concept was ascribed to the diagnosis.
While the potential of a diagnosis to enhance self-image has been highlighted by prior evidence syntheses (Attoe & Climie, 2023; Long & Coats, 2022), the greater range of evidence considered in this review sheds new light on the complexity of this process, problematising any straightforward narrative of diagnosis instigating a linear improvement in self-esteem. Contradicting prior suggestions of a unidirectional sequence of adjustment to a diagnosis (Murphy & LeVert, 1995), integration of ADHD into self-concept was iterative and dynamic, with people vacillating between acceptance and doubt over time. Disruption to one’s identity triggered uncertainty about the boundaries of the “ADHD self” and concerns about over-pathologising their experiences. Emotional responses were layered and ambivalent: people experienced relief from self-understanding, validation, and absolution from blame, but also regret for missed past opportunities and diminished future prospects. Large individual variation was also evident, with adjustment to the diagnosis shaped by prior self-concept, social feedback, and interpretative frameworks that could mean different things to different people. These dynamics cast diagnosis as neither uniformly liberating nor inherently destabilising, but as trigger for an ongoing, negotiated process of identity reconstruction.
The second theme constructed diagnosis as a socially embedded process that can both alleviate and produce relational strain, driving change in relationships with both specific and generalised others. Participants reported a longstanding feeling of social difference, which the diagnosis could amplify but reframe. While prior reviews have outlined the ways ADHD symptoms can affect interpersonal relationships (Attoe & Climie, 2023; Bjerrum et al., 2017; Ginapp et al., 2022; Long & Coats, 2022), an important extension of this analysis was to highlight the distinctive role of diagnosis in reshaping relationships. Studies suggested the diagnostic label often functioned as a social resource, providing a linguistic tool that individuals could use to communicate their perspective and secure new understanding from others. However, a diagnosis could also raise new interpersonal dilemmas. Participants were highly sensitive to prevailing stigma around ADHD, which they feared would transfer to them should they be so labelled (O’Connor, Brassil et al., 2022). This made disclosing one’s diagnosis to others an emotionally fraught decision. For this late-diagnosed cohort, many of whom women who diverged from ADHD’s typical male-centric profile and had reached functional adulthood without a diagnosis, fear of disbelief or trivialisation of the diagnosis compounded anxiety around disclosure. As a result, despite the resources many had invested in acquiring the diagnosis, some choose to conceal it in social situations.
Participant accounts suggested that for some, stigma exposure was mitigated by connection with an ADHD community, which offered validation, belonging, and relief from isolation. The importance of diagnosis as a platform for elaborating valued social identity is well-established in the mental health and neurodiversity literature, for example in relation to autism (Cooper et al., 2021; Maitland et al., 2021; Nayyar et al., 2025). However, the pertinence of neurodivergent identities and communities was less pervasive in this literature than in similar reviews of research on adult autism diagnosis (Nayyar et al., 2025). In this ADHD evidence-base, diagnosis’ impact on personal and interpersonal relationships was more prominent than community relations. With the origins of the neurodiversity movement heavily associated with autism (Kapp et al., 2013), it is possible that its concepts and cultures have not yet assimilated so broadly into the ADHD community, though this could evolve in the future (Urquhart et al., 2025).
The final theme outlined participants’ experiences of navigating healthcare and other systems across the diagnostic journey. While the studies traversed multiple jurisdictions, pre-diagnosis barriers and hurdles were a common thread, with difficult pathways to diagnosis the norm rather than exception. The demands of navigating complex and distributed service bureaucracies likely pose a particular cognitive challenge for this population (Morgan, 2024). A notable contribution of this review is to highlight many participants’ belief that early engagements with mental health services delayed rather than expedited ADHD diagnosis, through misdiagnosis with or ‘overshadowing’ by emotional difficulties. This resonates with prior literature suggesting diagnostic shifts are a common feature of journeys through mental health services, which can divert clinical and emotional trajectories in impactful ways (Høj Jørgensen et al., 2023; O’Connor et al., 2020; O’Connor, Seery et al., 2022; O’Connor & McNicholas, 2020).
Nevertheless, the synthesis indicated that for many adults, diagnosis identified them within systems in way that opened new opportunities and entitlements. Participants’ perspectives on specialist supports they received after diagnosis, including psychotherapeutic, environmental, and medication-based interventions, was largely positive. However, some reported post-diagnosis supports comprising solely medication prescriptions; this was generally seen as insufficient, with participants articulating a desire for more holistic supports. Moreover, multiple studies documented reports of participants whose service engagement ended at diagnosis, with no further follow-up offered.
Clinical Implications
The evidence synthesis conducted for this review underscores the profound subjective significance of receiving an ADHD diagnosis in adulthood, and the human cost of ADHD services’ continued orientation towards children. Participants’ accounts consistently highlighted barriers encountered when seeking to access assessment in adulthood. These findings point to the need for sustained investment in specialist adult ADHD diagnostic services, including assessment approaches that are sensitive to late presentation, gendered and socio-cultural differences, and the heterogeneity of adult symptom expression.
Ethically, resourcing diagnostic services requires parallel investment in post-diagnostic support. Both between and within studies, participants reported uneven availability of ADHD interventions. Some reported no access to any post-diagnosis support, while many others were offered only medication-based treatment. While participants who had tried medication generally saw it as beneficial, there was consistent desire for more holistic psychotherapeutic and environmental-based support. Importantly, such care should address not only the ADHD symptoms themselves, but also the social and emotional fallout of receiving a late diagnosis. The diagnosis can bring to the surface lifetime struggles with self-blame, impaired self-esteem, and relational strain, and accommodating the diagnosis into one’s identity can be a complex emotional process involving both relief and regret. Therapeutic supports might consider incorporating biographical narratives, acceptance and self-compassion into therapeutic programmes to support people in adapting to their diagnosis. Sensitivity to individual variability in diagnostic responses is key: while some individuals may follow a straightforward ‘impaired to empowered’ narrative, this is not a universal or linear trajectory, and the preference of some to keep their diagnosis at a psychological distance should be respected. Post-diagnostic provision should also be sensitive to other mental health challenges that may be active, whether resulting from independent comorbid difficulties or residual effects of undiagnosed ADHD.
The review also drew attention to the real harms of limited and stereotyped understandings of ADHD among healthcare professionals and the wider public. Gatekeepers such as primary care providers require targeted training that emphasises the diversity of adult ADHD presentations and the empirically outdated nature of traditional ADHD prototypes. Parallel awareness-raising initiatives aimed at employers, educators, and the general public may help reduce stigma, support openness around diagnostic disclosure, and mitigate doubts surrounding the legitimacy of late diagnoses.
Limitations of the Literature
The evidence reviewed was generally appraised as high quality, and the consistency with which patterns emerged across studies affords confidence in their robustness. However, the review identified limitations of the existing evidence-base, remediation of which should be priorities for future research. First, the literature is dominated by qualitative analyses, predominantly of interview-based data. While these methodological approaches were appropriate for generating rich insight into lived experience, and were generally evaluated as high-quality, a mature literature requires a rounded evidence base. The absence of quantitative research constrains estimation of the prevalence of specific diagnostic experiences and their association with longer-term outcomes. Second, the available evidence lacks socio-demographic diversity. Most studies emanated from high-income countries, with women over-represented, and sparse reporting of participants’ racial, ethnic, or socio-economic characteristics. Research inclusive of more diverse populations, including those facing multiple and intersecting forms of marginalisation, is essential to avoid reproducing inequities in whose diagnostic experiences are documented and understood. It is also key to understanding the factors that predict diverging responses to late diagnosis: for instance, age and cohort effects likely make ADHD diagnosis at 20 years and diagnosis at 70 years very different experiences. Third, a paucity of longitudinal evidence makes it difficult to track how experiences of diagnosis evolve over time. Participants’ own recollections portray adjusting to a diagnosis as a complex, extended process; but reliance on retrospective report compromises the reliability and detail of such accounts (Downey et al., 2025). Regular follow-up of participants across the diagnostic process would provide greater granularity regarding specific support-needs, and identify the trajectories at highest risk of poor long-term outcomes.
Limitations of the Review
This review made numerous advances beyond previous evidence syntheses (Attoe & Climie, 2023; Long & Coats, 2022), with a more expansive search strategy generating a larger number of studies, which covered more diverse samples and settings. However, limitations of the available data constrained analytic options. While the review was originally open to all study designs, no quantitative evidence was identified, leaving thematic synthesis the only available analytic route. Inconsistent reporting of individual-level data meant it was not possible to conduct formal subgroup analyses, for instance to explore how experiences differed by gender or age. Team resources restricted inclusion to English-language outputs, limiting the international scope of the review, while collapsing studies from different jurisdictions made it difficult to disentangle the influence of specific national or healthcare contexts on results. Restriction of scope to peer-reviewed journal articles may have excluded relevant insights from books, grey literature or clinical reports. Further evidence may have been missed due to limitations of the search-terms or their pragmatic restriction to title and abstract searches. However, risks of bias were mitigated through multiple steps including preregistration, supplementary searching of reference lists and key journals, involvement of multiple reviewers with inter-rater checks, use of specialist software, and rigorous approaches to data extraction and synthesis.
Conclusion
As rates of adult ADHD diagnosis continue to rise, this review provides a timely synthesis of lived experience evidence with clear implications for research, policy and practice. For adults considering assessment, the findings help them anticipate the potential gains and challenges associated with diagnosis, supporting informed and prepared action. For clinicians, the review highlights the transformative potential of diagnosis alongside its emotional and relational risks, underscoring the importance of sensitive assessment practices and robust post-diagnosis support. For policymakers, the findings expose persistent gaps in adult-oriented ADHD services from the perspective of end-users. As many jurisdictions move towards expanding adult ADHD provision, there is a critical opportunity to design services informed by lived experience from the outset. Continued high-quality research centring adults’ first-hand accounts of diagnosis will be crucial to ensure evolving systems truly serve the populations for whom they are designed.
Supplemental Material
sj-pdf-1-jad-10.1177_10870547261455946 – Supplemental material for A Systematic Review of Lived Experiences of Receiving a Diagnosis of ADHD in Adulthood
Supplemental material, sj-pdf-1-jad-10.1177_10870547261455946 for A Systematic Review of Lived Experiences of Receiving a Diagnosis of ADHD in Adulthood by Lucy McGill, Isabella Jardim-Lalor and Cliodhna O’Connor in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors acknowledge the contribution of Sophia Lenz to data analysis.
Ethical Considerations
As a systematic review of published research, this study did not require ethical approval.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: LM, COC; data collection: LM; analysis and interpretation of results: LM, IL, COC; draft manuscript preparation: LM, COC. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funding was sourced for the purpose of this research. However, LM and IJL are funded by the Health Service Executive (HSE) and this research was completed in partial fulfilment of course requirements for the Doctorate in Clinical Psychology at University College Dublin (UCD). Funders had no role in study design, collection or analysis of data, or the decision to submit the research for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available on request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.