
Abstract
Objective:
The objective of this analysis was to describe the effects of methylphenidate-mediated symptom improvement on functional impairments in adults with ADHD.
Methods:
This is an exploratory study of self-reported functional impairment on the Weiss Functional Impairment Rating Scale (WFIRS-S) in 351 ADHD adults treated in a forced dose, double blind (DB), randomized, parallel clinical trial of a 16-hr methylphenidate stimulant (PRC-063) for 4 weeks followed by open-label (OL; N = 147) for 6 months.
Results:
During the 4-week DB period, there was a statistically significant response to medication versus placebo in the WFIRS-S domain of “work.” Forty percent of DB subjects, assigned a random dose of medication, showed functional improvement as defined by the Minimal Clinical Important Differences (MCID) of the WFIRS. At the end of DB, one third of subjects had scores below symptomatic and functional impairment thresholds and two thirds by the end of OL. Although the OL period was uncontrolled, when all subjects had been dose optimized with sufficient time for functional impairment to manifest, all WFIRS functional domains showed clinically-relevant improvements from baseline to end of the 6-month OL (p < .0001). There was a fair-to-moderate correlation between change in symptoms and change in function, but ADHD symptoms were about twice as sensitive to change. The strongest predictor of improvement in function was greater improvement in ADHD symptoms. Younger age predicted greater functional impairment.
Conclusion:
This study of the relationship between change in symptoms and functional outcome illustrates that improvement in symptoms may be associated with an almost cotemporaneous improvement in function, that increases over time. Identification of subjects who are symptom responders with residual functional impairment suggests the need for additional intervention to target residual functional difficulty. Further research needs to replicate this methodology using an individually dose optimized design to demonstrate full potential for change and to confirm the domains of functioning in adults with ADHD that are most responsive to stimulant treatment.
Clinical Trial Registration:
Introduction
ADHD in adults is common with a prevalence of 4.4% (Kessler et al., 2006) and is functionally impairing (Fayyad et al., 2017). Long-term outcomes of ADHD in adults have been demonstrated to include high risk of emergence of comorbid psychiatric symptoms and disorders, problems with high-risk activities including reckless driving and substance use, decreased educational achievement, unemployment and misemployment, and family problems including marital conflict and challenges with parenting (French et al., 2024; Hechtman et al., 2016). To prevent these deleterious outcomes, it is critical to prospectively measure both symptoms and functional impairment, and to include a psychometrically validated scale as part of assessment in both clinical and research evaluation of response to treatment. We report the first study of a randomized, double-blind (DB), placebo-controlled stimulant trial followed by a 6-month open-label (OL) follow up in adults with ADHD which measured functionality as an outcome on a psychometrically validated scale. The objective of this analysis was to examine the correlation between symptomatic response and functional outcome by identifying those domains of functioning that are responsive to medication treatment in DB and OL over time and by identifying the patient characteristics predictive of greater functional improvement.
The primary outcome of this clinical trial, improvement in ADHD symptoms as measured by clinician rating of the ADHD-5-RS, has been previously reported (M. D. Weiss, Childress, & Donnelly, 2021), as well as sleep outcomes (M. D. Weiss, Surman, et al., 2021). Active treatment was associated with greater symptom change on the ADHD-5-RS as compared to placebo, with additional, sustained improvement through 6 months of OL treatment. Most of the symptom improvement during OL occurred during the first 3 months of OL during the period in which dose optimization was occurring.
There are relatively few RCTs of stimulant treatment of ADHD in adults that have systematically included functional impairment as an outcome (Adler et al, 2021; Fredriksen et al., 2013; Surman et al., 2013), yet long-term improvements in functionality are the ultimate goals of treatment for both patients and clinicians (Fredriksen et al., 2013). Previous studies in children and adolescents examining both symptoms and function as outcomes in clinical trials of stimulant treatment have demonstrated that 19% of patients with excellent symptom response to stimulant treatment were still functionally impaired and 43% of patients who had any symptomatic improvement remained functionally impaired (M. Weiss, Childress, et al., 2018). Becker et al. (2011) systematically looked at function as an outcome and found that, out of 435 randomized controlled trials in children and youth, two-thirds (63.9%) demonstrated at least a minimum level of evidence for reducing symptoms; however, only 18.8% of treatments demonstrated evidence for reducing functional impairment, largely because functional impairment was not typically included as an outcome.
While we know that symptomatic and functional improvement are moderately correlated (M. D. Weiss, McBride, et al., 2018), it is those situations in which symptoms improve but the patient remains impaired that are of particular interest to clinicians (Tarakcioglu et al., 2020). ADHD is associated with multiple and serious potential deleterious outcomes, but patients are less likely to experience these outcomes while they are on stimulant medication than when they are not (Bikic & Dalsgaard, 2018; Dalsgaard, Leckman, et al., 2015; Dalsgaard, Ostergaard, et al, 2015; Vasiliadis et al., 2024). A meta-analysis of ADHD treatments found that symptomatic improvements of 41% or greater in adults were associated with functional improvement of 0.25 SD or greater, but lesser symptomatic improvement was associated with no functional improvement or worsening of function (Buitelaar et al., 2009).
The effect size of symptom response in adults is generally lower than what is seen in children, and symptom response is a driver of functional response (Faraone, 2012). We hypothesize that stimulant treatment of adult ADHD leads to a more robust change in symptoms than in functional impairment, and that response may vary between domains. As the evaluation of ADHD requires information across the domains of attention, hyperactivity, and impulsivity (Gibbins et al., 2012), the clinical evaluation of functional impairment requires not just the total score, but also an understanding of where and when the impairment is occurring in order to develop an appropriate treatment plan (M. D. Weiss, McBride, et al., 2018). Previous research in children has demonstrated that sensitivity to change with stimulant treatment varies across functional domains on the Weiss Functional Impairment Rating Scale-Self Report (WFIRS-S), with School Learning and Behavior, Family, Social, and Risky Behaviors being responsive and Life Skills and Self-Concept more resistant to change (Stein et al., 2015). It is possible to hypothesize that stimulants provide the potential for functional improvement in some areas, but additional skills training are needed for the improvement to manifest. This is the first study to look at the comparative sensitivity to stimulant treatment of different domains of functioning in adults with ADHD.
If more were known about the patient characteristics that predict symptomatic and functional response to stimulants, this would allow for patients to be provided with a more informed perspective of their individualized likelihood of response (Weiss et al., 2010). This paper reports a post hoc analysis of functional outcome with stimulant treatment, the relationship between symptom change and functional change, domain differences in functional response, and characterization of patient predictors of functional response.
Methods
This was a multi-site study conducted at 34 sites in the USA and Canada in 2014 to 2015 (NCT02139124). The protocol was approved by either or both a central IRB and the local IRB, as required. All subjects signed written informed consent to the DB study and then to the OL study if they participated. All study procedures were executed in accordance with Good Clinical Practice (GCP) as required by the Declaration of Helsinki 1964 and later amendments and the International Conference on Harmonization Guideline for GCP of the European Agency for the Evaluation of Medicinal Products.
Subjects
Four hundred sixty-five adults 18 years or older were screened. The diagnosis of ADHD was confirmed using the Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID; Epstein et al., 2001; Epstein & Kollins, 2006). Inclusion criteria for the DB study required a baseline post-washout score of greater than or equal to 24 on the ADHD DSM-5 Rating Scale (ADHD-5-RS) administered by a clinician who was an expert in ADHD. Three hundred ten subjects were included in the study who were either treatment-naïve or who were dissatisfied with their current pharmacotherapy. All subjects had an IQ >to 80 on the Kaufman Brief Intelligence Test-2 (KBIT-2; Bain & Jaspers, 2010) and a negative pregnancy test. Subjects were excluded if they had psychiatric comorbidity requiring other treatment, a history of adverse response to stimulants, and a history of stimulant failure. Subjects with medical concerns that might be contraindications to stimulant treatment such as cardiovascular disease or requiring medication contraindicated with stimulant treatment were excluded. Inclusion criteria for the OL study included completion of DB study. OL enrolment was closed following 6 months of the DB study conduct.
Demographic and ADHD characteristics of the study populations are described in Table 1.
Demographics and ADHD Characteristics.

Note. SD = standard deviation.
Study Design
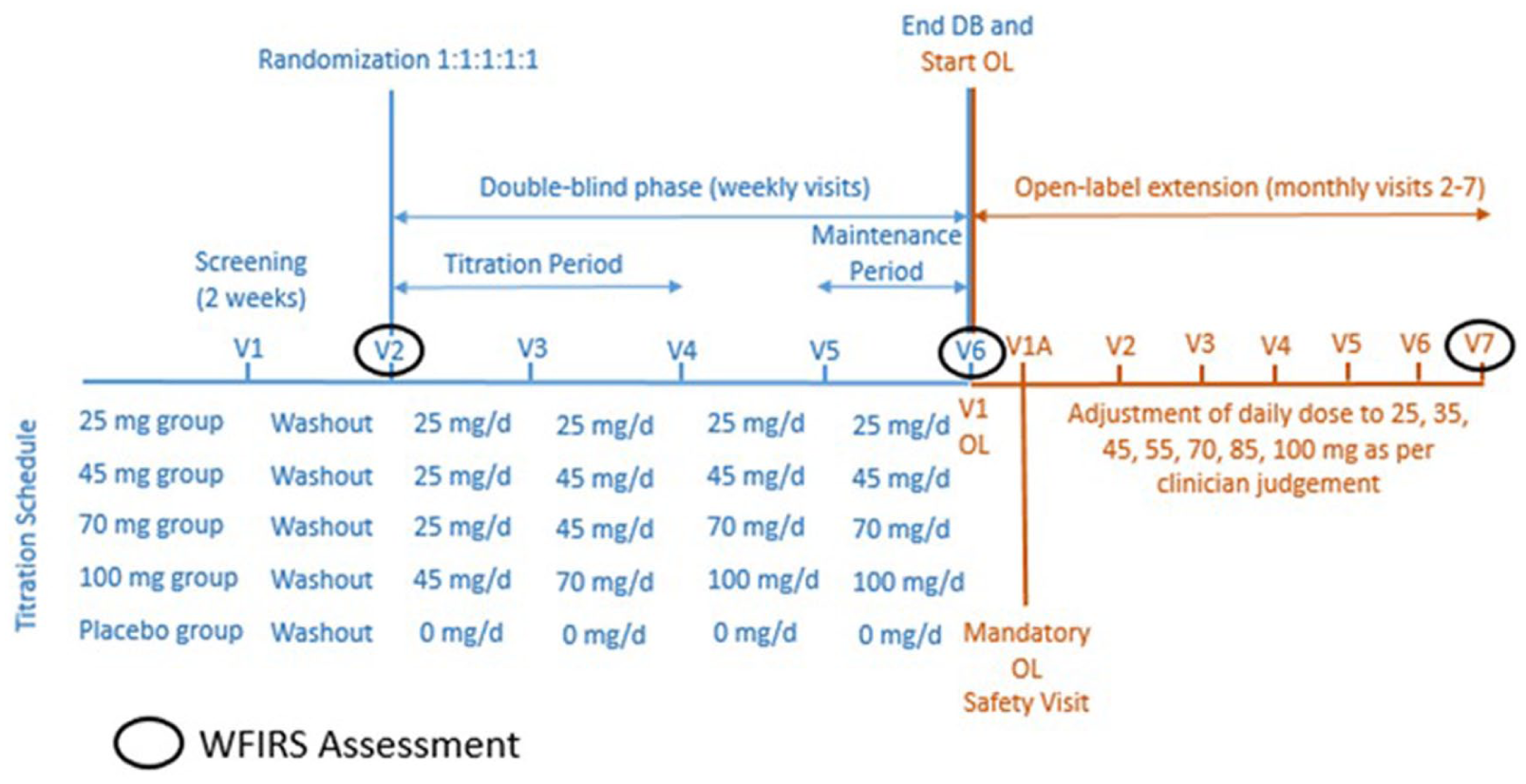
The initial 4-week trial was a forced-dose, parallel, double-blind, randomized clinical trial of a 16-hr multilayer-release methylphenidate (PRC-063) in 375 adults with ADHD. Following the screening and washout, subjects were randomized 1:1:1:1:1 to receive either 25, 45, 70, or 100 mg/day of PRC-063 or placebo. The study was not adequately powered to allow for reliable between-dose comparisons. Two hundred seventy-eight subjects received methylphenidate and 73 subjects were on placebo. One hundred eighty-four subjects entered the OL phase and 124 completed. Of those, 147 subjects had data on the WFIRS-S, 31 of whom were previously on placebo. DB doses were increased weekly over a 3-week period. The DB study lasted 2 weeks from visit 4, when titration ended, to visit 6. There were six monthly visits for those subjects who participated in the OL follow up. The CONSORT diagram for this study is available in the primary publication (M. Weiss, Childress, & Donnelly, 2021) and reproduced here (Supplemental Figure 1). The study visits are illustrated in Figure 1.
CONSORT Diagram.
Subjects who completed the DB trial from any arm were eligible to continue in a 6-month OL follow up, with enrolment limited to approximately 50% of the DB population. Thirty-eight patients entered from the placebo arm and 31 of those had data on the WFIRS-S. Blinding of the DB study was not broken until subjects completed the OL study. Patients received OL medication on the final day of the DB study, to take the following morning. During the OL, clinicians titrated the dose of medication to the point of optimal improvement, as tolerated. The OL phase consisted of weekly dose titration visits, as necessary, six monthly follow up visits, and a post treatment 14-day safety telephone check.
Medication Treatment
PRC-063 (MPH-MLR) is a once-daily, extended-release formulation of methylphenidate hydrochloride with a rapid onset of action with an initial peak at 1.6 hr and a second, higher peak at 12.5 hr for an approximate 16-hr duration (Katzman et al., 2020; Zhu et al., 2023). Plasma levels slowly decline with residual levels of 18% at 24 hr post-dose. PRC-063 is marketed as Foquest® in Canada and was available as Adhansia XR® in the USA.
Measures
ADHD
Outcome of ADHD symptoms was based on clinician rating of ADHD symptoms on the ADHD-5-RS (DuPaul et al., 2016) as assessed during subject visit based on subject interview and self and observer reports using the Conners’ Adult ADHD Rating Scale as collateral information.
Functional Impairment
Functional impairment was measured using the Weiss Functional Impairment Rating Scale—Self Report (WFIRS-S). The WFIRS-S rates how the patient feels their emotional and behavioral symptoms impact their level of functioning in the following domains: Family, Work, School, Life Skills, Self-Concept, Social, and Risky Activities. There are 69 items, and items that are not relevant to that individual are rated as “not applicable” and not included in the final mean score. Calculation of mean scores for each domain allows for comparison across domains, and between each domain and overall change. The scale has been found to have robust psychometric properties as well as sensitivity to change (Canu et al., 2020, Hadianfard et al., 2019; Haugan et al., 2021; Micoulaud-Franchi et al., 2019; Takeda et al., 2017; M. D. Weiss, McBride, et al, 2018), including high internal consistency, good discriminant validity to distinguish clinical and non-clinical populations, and moderate divergent validity with symptoms.
Statistical Analyses
No power analyses were done for the secondary outcomes which were exploratory, and no Bonferroni correction was done for multiple analyses.
Functional response to medication treatment was analyzed in the DB by two-sample t-test comparing change on WFIRS total score and each domain for active treatment vs. placebo in the intent-to-treat population.
Descriptive statistics were used to look at the percent change in each domain and the total change score. The correlation between symptom change and functional change was analyzed with SAS PROC CORR at the group level by domain and for the total score. Differences in response at the group level were compared with interindividual differences using a scatter plot.
The Wilcoxon rank-sum test was used to compare median WFIRS-S score changes for PRC-063 and placebo in the DB study and median WFIRS-S scores at baseline and end of study for subjects who completed the OL study.
In the DB study, pre- to post-treatment effect sizes were calculated for WFIRS score changes as the mean score change divided by the standardized deviation (SD) and for differences in WFIRS score changes between PRC-063 and placebo as the mean difference divided by the pooled SD.
Pearson correlation coefficients and p-values were calculated for the associations between mean changes in WFIRS-S scores and ADHD-5-RS total score.
Percentages of subjects achieving improvement above the Minimal Clinically Important Difference (MCID) of ≥0.25 points on WFIRS-S Total Score and ≥6.6 points on ADHD-5-RS total score were calculated (Storebø et al., 2015; Zhang et al., 2005). Percentages of subjects below cut off scores based on WFIRS-S Total Score (≤0.65 points) and ADHD-5-RS total score (≤18 points) were also calculated. Cohen’s Kappa was calculated to quantify the agreement between the proportions of subjects achieving the MCID and excellent response based on WFIRS-S Total Score and ADHD-5-RS total score (Storebø et al., 2015; Zhang et al., 2005).
Multiple linear regression models were created to identify predictors of improvements in WFIRS-S Total Score during the double-blind and open-label studies. The dependent variable was mean WFIRS-S Total Score change, and the independent variables were age, race, sex, body mass index, time since diagnosis of ADHD, baseline ADHD-5-RS total score (model for double-blind study only), ADHD-5-RS total score at end of double-blind study (model for open-label study only), ADHD-5-RS total score change, ADHD subtype, prior ADHD medication, and treatment assigned in the double-blind study.
Results
Subject Disposition
Four hundred sixty-five subjects were screened of which 351 were eligible to participate in the DB study, of which 73 were randomized to placebo. A total of 184 entered the OL follow up and 124 completed the OL follow up.
ADHD Symptom Response
47.5% of subjects were rated as “improved” or “very much improved” on the Clinical Global Impressions—Improvement scale at the end of the DB study. Symptoms continued to improve throughout the OL phase with 14% of improvement occurring in the last 4 months of OL.
Change in Function
Change scores on the WFIRS-S total and subscale scores from the DB study are reported in Table 2 and displayed in Figure 2(a). The only domain during the DB study which was statistically significantly superior to placebo was the domain of Work (p = .007). During the double blind, there was a trend towards a statistically significant difference in WFIRS Total score from 0.31 in active treatment and 0.12 with placebo (p = .07).
Change in Median WFIRS-Self Score over Time during Double-Blind Phase.
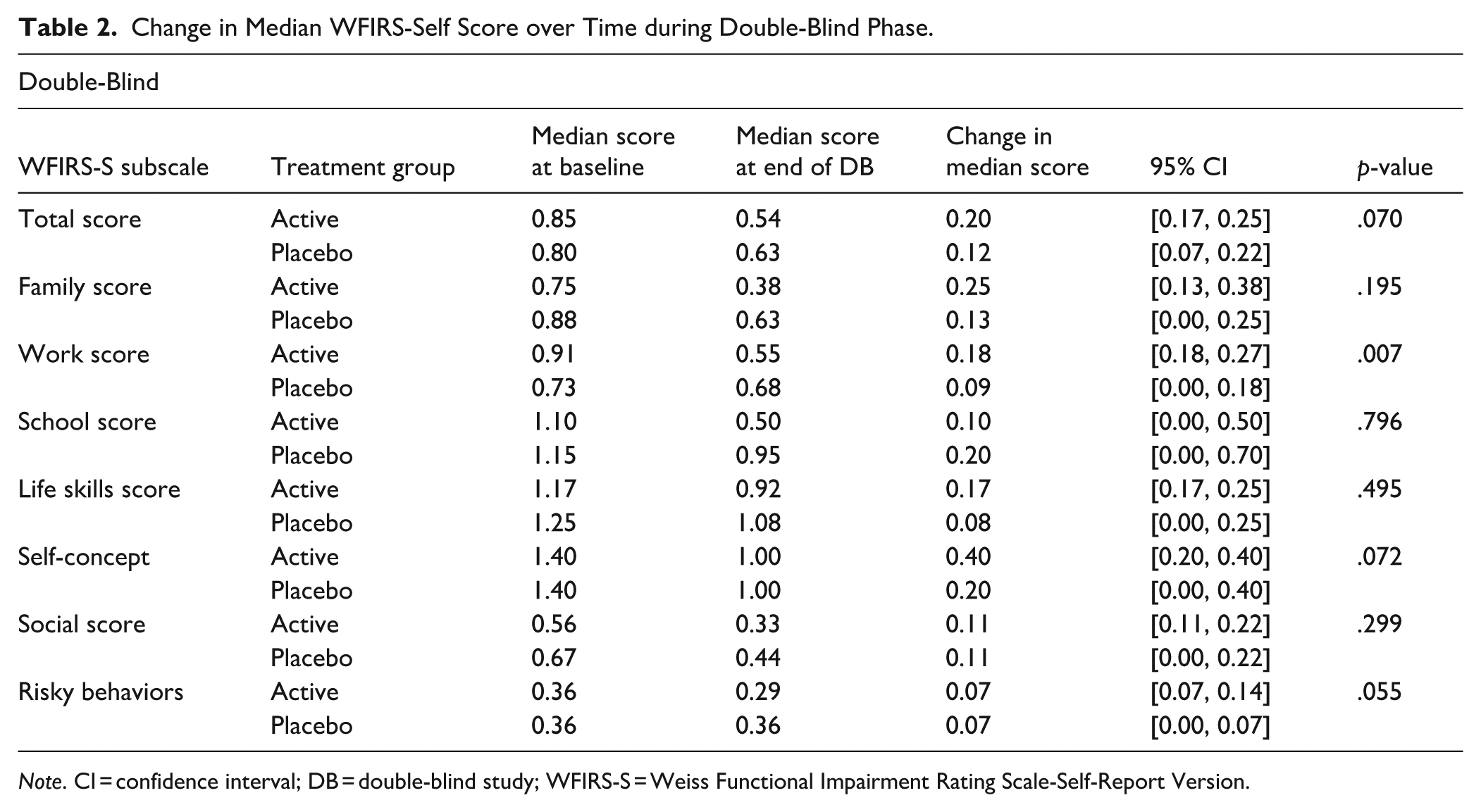
Note. CI = confidence interval; DB = double-blind study; WFIRS-S = Weiss Functional Impairment Rating Scale-Self-Report Version.

(a) Change in functional impairment over time during double blind treatment and (b) change in functional impairment over time during open label dose optimization.
Change scores on the WFIRS-S total and subscale scores from the OL study are reported in Table 3 and displayed in Figure 2(b). When treatment was optimized over the duration of the OL treatment phase, there was a statistically significant improvement from baseline to endpoint from a median of 0.89 at baseline to 0.41 at end of OL, for a change score of 0.38 which is 1.4 times the MCID (p < .001).
Change in Median WFIRS-Self Score over Time during Open Label Phase.
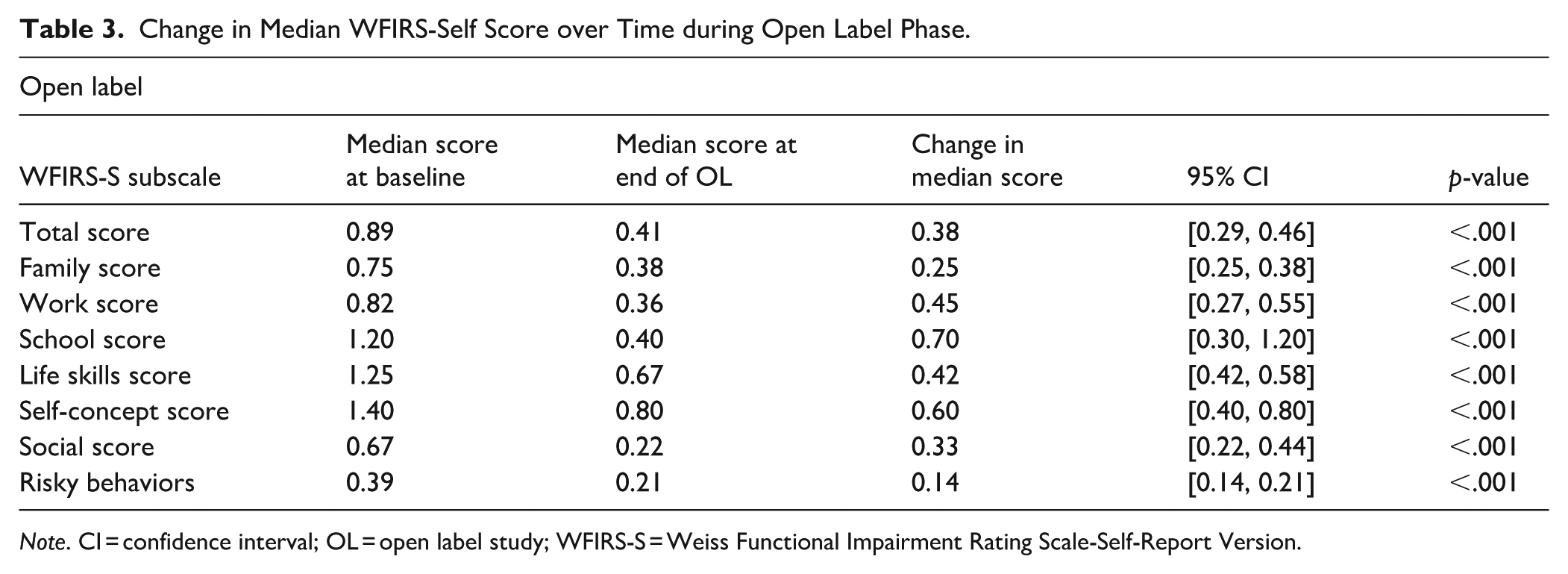
Note. CI = confidence interval; OL = open label study; WFIRS-S = Weiss Functional Impairment Rating Scale-Self-Report Version.
Relationship Between Change in Symptoms and Change in Function
Improvement was defined as the percentage of subjects who improved by at least the MCID on both the ADHD-5-RS Total Score (change score of 6.6 points) and the WFIRS-S (change score of 0.25). Of subjects receiving active medication, 39.6% showed improvement in both symptoms and functioning, 33.8 % showed improvement in symptoms without improvement in function, while only 4.3% showed improvement in functioning if symptoms did not improve. While the relationship between improvement in symptoms and functioning was stronger for those on placebo (Cohen’s Kappa = .39) than those on stimulant (Cohen’s Kappa = .28), only 26.0% of subjects on placebo showed improvement in both symptoms and functioning and 43.8% did not show improvement on either measure. For active treatment, correlations between improvement in symptoms and improvement in function were statistically significant and generally moderate across all domains ranging from .39 to .58 (p < .001). For placebo treatment, correlations ranged from .33 to .59 and were statistically significant, with the exception of the School domain (Pearson Correlation = .15, p = .655). In OL, there was a continued moderate correlation between optimal improvement in symptoms and functioning, whereby 66.7% of subjects experienced both functional and symptomatic improvement (Cohen’s Kappa = .34, p < .001).
Demographic Predictors of Functional Improvement
A full model was run with age, sex, race, BMI, ADHD-5-RS score at baseline, ADHD-5-RS change in DB, ADHD type, prior ADHD medication. In the DB phase, for each 12-point improvement in ADHD-5-RS score (approximately twice the MCID), the improvement in total WFIRS-S score increased by 0.22 points on the WFIRS-S Scale (approximately one MCID), assuming all other variables remained constant (p < .001). Every 10-year increase in the age of the patient decreased response on WFIRS by 0.07 points (p = .046). There were no statistically significant associations found between sex, race, BMI, or ADHD subtype and the magnitude of functional response.
Discussion
This is an exploratory analysis of functional response to stimulant treatment in adults with ADHD with the objective of determining the overall and domain-specific improvement in functioning with stimulant treatment, the time course of improvement, the nature of the relationship between symptom and functional response, and patient predictors of response.
We were able to detect statistically significant improvement in “Work” within 4 weeks during the DB period as compared to placebo, despite the very short time frame and 89% of subjects receiving suboptimal doses due to the randomized, parallel, fixed dose design. The “work” subscale assesses items such as problems with getting your work done efficiently, problems keeping a job, getting fired from work, problems with being late and problems working to your potential. There was a trend to improvement in overall WFIRS-S score and marked improvement in all domains during the subsequent OL period which matched the time course of dose optimization. The Risky Activities domain, which measures rare, but salient events, surprisingly showed a trend to response during the DB (p = .055). This is consistent with the few studies of functional response to stimulants in adults (Surman et al., 2013). In some ways this is reassuring as impairment in ability to work and high-risk behaviors are the two areas which might be considered to cause the greatest morbidity over the life span. Change scores for Family (p = .19), School (p = .796), and Social (p = .299) are of interest since the domains of school and family are particularly sensitive to treatment in children (Stein et al., 2015). Adults with ADHD may not self report family issues, or if younger in age, may not be living in family situations. They will not report school functioning if it is not applicable due to not attending school. The DB results may be an underestimation of potential functional response, since symptom response was modest because of the double blind, randomized, parallel design in which a large majority of patients were on sub-optimal doses. Given that all domains showed a robust response over 6 months of OL dose optimized treatment, the take home message for clinicians is that stimulant treatment of adults with ADHD can be anticipated to lead to functional improvement in most patients and optimized functional impairment over time in more than half of patients. It is also clear from this study that while symptom and functional response are moderately correlated in both children and adults, the domains of functioning that are most responsive to treatment vary across the life cycle, as expected given the developmental differences in demands for school, family, work, socialization, and risk across the life cycle.
The data from the OL study should be interpreted with caution, as there was no blinding or placebo control, although there is merit in analyzing the OL study as it is similar to clinical practice. Placebo response, or nonspecific improvement with treatment, may have partially contributed to the OL outcomes, but placebo response tends to occur early in treatment, whereas the time course of functional improvement in the OL phase followed the time course of dose optimization. Not surprisingly, the more robust the symptom response, the better the functional response. Given the relevant MCIDs, this means that to obtain the minimal clinically important functional response, twice the minimal clinically important symptomatic improvement is required. This information represents a potent, patient-centric guide to include in the psychoeducation of ADHD patients regarding what they can anticipate from stimulant medication management. In total, 33.8 % of subjects showed improvement in ADHD symptoms without improvement in function, while only 4.3% of subjects showed improvement in functioning if symptoms did not improve. This suggests measurement of both functional and symptom outcomes is important to capture a complete picture of treatment outcome. The evaluation of symptoms alone may be a relatively weak method of determining if a patient is actually being optimally treated. Symptom change may be more immediate and more sensitive to medication treatment, but robust symptom change is associated with the functional response that is the more meaningful target of treatment.
A strength of this study is that we used psychometrically validated measures of both symptoms and function, and that the functional measure includes domain scores. Most clinical trials have relied on the CGI as a measure of overall patient response, which does not adequately distinguish functional from symptomatic changes, and does not report those areas that are improved or those areas that still need further intervention.
This study demonstrates that improvement in functioning—arguably the more meaningful, actual target of treatment—was associated with significant improvements in symptoms across the full spectrum of response. We identified that a majority of patients achieved both symptomatic and functional improvement at the end of OL, an outcome that matches closely to the clinical outcomes of interest to patients in practice. Replication of this research with individualized dose optimization and longer periods of observation would bolster our confidence in providing realistic estimates of functional outcomes when educating patients about anticipated outcomes of stimulant treatment.
Our data on patient predictors of functional response are consistent with what would be expected clinically. The greater the severity of initial symptoms, and the greater the improvement in symptoms, the greater the anticipated improvement in the functional impairment driven by those symptoms. If the clinician’s goal is to improve functioning, then our data suggests we need to target optimization of symptom response, along with assessment of those domains that do not respond and require additional treatment, or non-medication intervention. An important predictor of resistance to change in function was patient age. Patients who are older and have developed dysfunctional habits that have become more entrenched and persistent over time will be more resistant to change. Awareness of these positive and negative predictors of outcome allows the clinician to personalize information provided to patients about what they can anticipate from treatment.
There are several limitations to this study. (1) In assessing adults for functional impairment in association with ADHD, we are using self-report rather than observer report, which may underestimate impairments that have been present life-long and are interpreted by the patient as “their normal.” (2) Additionally, the majority of adults with persistent ADHD will also have developed comorbid mental health disorders which contribute to functional impairment and cannot easily be distinguished from impairment driven specifically by ADHD symptoms. (3) Evaluation of function was a secondary outcome in this pivotal trial, while symptoms were the primary outcome. The primary study was not powered for evaluation of differences in response between dose, so all analyses are limited to drug versus placebo. (4) A methodological limitation of the DB study was that 89% of subjects were randomized to sub-optimal doses as compared to the doses used in the dose optimized OL study, and therefore not able to capture the full potential of dose optimized treatment. These study results suggest that improvement in symptoms translates into real life change in function, but does not tell us much about how much change is possible with optimal treatment, nor about potential domain-to-domain differences in response overall and with time. (5) The 4-week time period of the DB phase was potentially shorter than the time required for the patient to either achieve or observe and report functional change. (6) The absence of a placebo control during the OL period means that we do not know the extent to which these robust outcomes represent a nonspecific response to treatment, versus greater time on treatment or optimized dosing.
Strengths of the study include that this is the first targeted study of functional outcomes in stimulant treatment of adults and included both a short DB phase and a long OL follow up to be able to look at time to initial functional response, and optimization of functional response over time. One advantage of a design in which patients were not optimized is that a wide spectrum of response was observed. This means that our evaluation of the correlation between symptoms and functioning is relevant to the full range of responses and not just individuals who have a robust response. Descriptives of the relationship between domain response and symptom response and within group analyses comparing older subjects or subjects who have or have not had prior treatment would not be expected to be impacted by these limitations.
Conclusions
Further research using psychometrically valid measures of functional outcomes in the treatment of adults with ADHD will allow us to provide personalized psychoeducation about functional treatment response. Replication and further research using some of the methodology described here regarding functional improvement with ADHD treatment can offer a useful framework for a more patient-centric approach to measure outcomes. From a research standpoint, our results illustrate a more conservative estimate of the potential impact of stimulant treatment. From a clinical standpoint, identifying patients who look like they are treatment responders because they are less symptomatic, even though they remain functionally impaired, opens up the clinical opportunity to treat to optimal functional response.
Supplemental Material
sj-docx-1-jad-10.1177_10870547261440452 – Supplemental material for An Exploratory Study of Functional Outcome in Stimulant Treatment of ADHD in Adults
Supplemental material, sj-docx-1-jad-10.1177_10870547261440452 for An Exploratory Study of Functional Outcome in Stimulant Treatment of ADHD in Adults by Margaret D. Weiss, Jeffrey H. Newcorn, Pratap Chokka, Marc Cataldo, Sailaja Bhaskar and Graeme A. E. Donnelly in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to thank Genesis Research for data analysis, Ruta Zurkevicius, Parissa Sadri, Joseph Reiz, and Zoltan Harsanyi for study development and administration.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of IRB Services (Aurora, ON; protocol code 063-010 and 063-012 on January 29, 2014).
Author Contributions
Conceptualization, MW, PC, MC, GD, and SB; methodology, GD; formal analysis, MC and GD; investigation, MW and PC; writing—original draft preparation, MW; writing—review and editing, JN, GD, MW, MC, and PC; supervision, SB; project administration, GD. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Purdue Pharma (Canada) and Adlon Therapeutics.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Purdue Pharma (Canada) was involved in the design of the study; in the collection, analyses and interpretation of data; in the writing of the manuscript, and in the decision to publish the results. MW has consulting fees from Revibe, Peri; speaker fees and expenses from Cooper Medical School; United Kingdom Adult ADHD Network, Canadian Attention Deficit Resource Alliance, American Academy of Child and Adolescent Psychiatry, and OASIS; thesis review payment from University of Dublin; and royalties from Multi-Health Systems.
In the past two year, JHN has been a consultant/advisory board member for AGB Pharma, Cingulate Therapeutics, Lumos, Mentavi Health, Otsuka, Signant Health, Supernus, Tris; he received research support from MindTension and Supernus; honoraria for disease state lectures from Abbott, Apsen, Knight Therapeutics, Medice, Supernus and Otsuka, and served as a consultant for the US National Football League.
PC has received grants and research support from Janssen and Lundbeck; speaker fees and expenses from Abbvie, Elvium Life Sciences, Janssen, Lundbeck, Otsuka, and Takeda. MC is an employee of Purdue Pharma L.P, Stamford, CT. SB is an employee of Imbrium Therapeutics L.P. a subsidiary of Purdue Pharma L.P., Stamford, CT. GAD is an employee of Elvium Life Sciences.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.