
Abstract
Objective:
Parental mental health plays a critical role in the wellbeing of the family, yet few studies have examined how parental ADHD affects postpartum depression and anxiety. This study investigates the hypothesis that parent (including coparent) ADHD symptoms are associated with postpartum depressive and anxiety symptoms.
Methods:
117 mother-father dyads (half with parental ADHD) were recruited when their infants were 6 to 10 months old. Participants completed questionnaires on ADHD, depression, anxiety, and social support. Clinician-administered semi-structured interviews assessed ADHD symptoms and psychiatric histories.
Results:
Participants in ADHD and non-ADHD dyads were demographically comparable but differed in prevalence of prior mood disorder (47% vs. 24%). Individuals with ADHD had significantly higher odds of moderate-to-severe depressive (OR = 2.70, 95% CI [1.10, 6.62]) and anxiety symptoms (OR = 4.58, 95% CI [1.82, 11.53]). Parallel mixed effects models accounting for parent dyad found that self-reported and clinician-reported ADHD symptoms and prior mood disorder history were significant predictors of depressive and anxiety symptoms (p < .025). Coparent ADHD symptoms were significantly associated with postpartum mood symptoms in the self-report models only. Higher perceived social support was associated with fewer depressive symptoms, approaching or reaching statistical significance in self- and clinician-report models, respectively. Secondary analysis identified self-reported ADHD symptoms and prior mood disorder as predictors of postpartum depressive and anxiety symptoms regardless of parent sex (p < .05).
Conclusion:
Findings suggest that parental ADHD – in either parent – contributes to postpartum psychological distress. Screening and treatment of ADHD in new parents may reduce depressive and anxiety symptoms for those showing ADHD symptoms and their coparents, supporting the mental health outcomes of the whole family.
Introduction
New parenthood dramatically increases demands on parental attention and executive function, domains already impaired in adults with ADHD. Although executive function deficits in working memory, time management, and organization feature prominently in adult ADHD, evidence has also shown depression and anxiety commonly cooccur. Close to 80% of adults with ADHD have at least one comorbid psychiatric disorder, and emerging evidence suggests that maternal ADHD may confer additional risk for depression and anxiety across the postpartum period, which the American College of Obstetricians and Gynecologists defines as extending through the first year following delivery (ACOG, 2018; Andersson et al., 2023; Torgersen et al., 2006). Further study of the dynamic relationships between adult ADHD, mood disorder, and parenthood is essential to promoting the long-term wellness of families with ADHD.
One recent study of the Swedish national health record suggested that maternal ADHD may be associated with increased risk of mood disorders in the first year postpartum; among cisgender women with ADHD, as many as 16.8% received diagnoses of depression and 24.9% of anxiety in this period, compared to 3.3% and 4.6% in the general population (Andersson et al., 2023). The prenatal period is often marked by significant changes in medical management of established psychiatric diagnoses, such as ADHD, that may persist after delivery and affect postpartum mental health (Baker & Freeman, 2018). Many adults worldwide drastically reduce or cease pharmacologic treatment in pregnancy or lactation, with another Nordic population-based cohort study reporting as many as 78% to 85% of people choosing to discontinue ADHD medication in pregnancy (Cohen et al., 2023). Cessation of maternal ADHD treatment, in conjunction with rapidly rising executive function and attentional demands in pregnancy and new parenthood, further increases risk of functional impairment and disordered mood among mothers in the peripartum period. Research on the relationship between maternal ADHD and postpartum psychopathology is an emerging area of interest but has been largely limited to retrospective analysis of diagnostic codes, primarily in northern European countries. While this literature offers valuable insights into broad risk patterns, research based on administrative diagnoses is subject to underdiagnosis bias, which is particularly relevant for conditions like ADHD that are frequently underdiagnosed in adult women. Moreover, this literature lacks symptom-level granularity or insight into the role of the familial environment on postpartum outcomes.
Research exploring connections between ADHD and postpartum mood disorders among fathers is extremely limited, with only one study reporting that men with ADHD had 2.02 times higher odds of depression or anxiety in the first year of parenthood compared to those without ADHD (Dennis et al., 2022). Even less is known about the potential role of coparent ADHD in postpartum mental health. Extending study beyond maternal or paternal ADHD in isolation to examination of the parental dyad provides opportunities for understanding how ADHD in one parent may negatively affect both individuals’ mental health. Prior research suggests that individuals with ADHD and their coparents experience greater overall parenting distress than those without ADHD (Joseph et al., 2022). A growing literature on the interpersonal dynamics of neurotypical mother-father pairs has also found that mothers report greater prospective memory demands than fathers, meaning they feel a greater need to maintain memory for carrying out future actions or intentions (Einstein & McDaniel, 1990), and believe their support of coparent prospective memory is unreciprocated (Harrington & Reese-Melancon, 2022). Whereas working memory impairments associated with ADHD may contribute to parenting stress across the dyad, this gendered finding implies paternal ADHD may worsen distress for mothers above and beyond the neurotypical experience. Further research is needed to understand how ADHD in one party may be associated with adverse mental health outcomes in the undiagnosed coparent.
The present study investigates the impact of both parent and coparent ADHD on depressive and anxiety symptoms in the first year of infant life, addressing several critical gaps in the perinatal mental health literature. By studying ADHD at the symptom level, incorporating both maternal and paternal mental health outcomes, and examining the interdependence of coparent mental health, we aim to expand on a literature that has largely focused on maternal diagnoses in isolation, and to corroborate emerging evidence about paternal experiences. Using biological parent dyads with and without ADHD, we compared ADHD symptoms and established risk factors for depression and anxiety to evaluate the impact of participant and coparent ADHD on postpartum mental health and secondarily explored whether these associations differed by parent sex. We hypothesized that individuals with ADHD, or parenting alongside a coparent with ADHD, would exhibit increased higher levels of postpartum depressive and anxiety symptoms, and that greater ADHD symptom severity in either parent would be associated with more severe mood symptoms. The following analyses address the dyadic effects of ADHD on postpartum mood and anxiety, exploring the intersection of attentional, emotional, and familial vulnerabilities during early parenthood.
Methods
Study Overview
The current study presents a secondary analysis of postpartum mental health among a group of biological parent dyads (paired mothers and fathers) with and without parental ADHD, originally enrolled with their newborns in one of two prospective studies about early predictors of childhood ADHD. Measurement of a variety of peripartum mental health outcomes in both mothers and fathers provided a unique opportunity to examine associations between parental ADHD and depressive and anxiety symptoms across the parenting dyad at 6 to 10 months postpartum. The primary research objectives were to:
Our study design also allowed pursuit of several secondary aims. First, depression and anxiety outcomes were modeled separately to identify potential differences in predictors (including parental ADHD) of postpartum depression versus anxiety. Second, we evaluated whether findings differed between mothers and fathers. Finally, the availability of both participant-reported and clinician-reported measures of ADHD at the symptom level enabled parallel models as a sensitivity analysis for the robustness of any ADHD-related findings. Given the relatively small sample size and limited prior research on coparent ADHD, this methodological redundancy was intended to guard against overinterpretation of findings.
Participants
Participants were 234 parents from southwestern Pennsylvania, representing the full cohort of 117 cisgender, biological mother-father dyads enrolled across the Pittsburgh ADHD Risk in Infancy Study (PARIS; n = 144, 50% in ADHD dyads) and New(born) PARIS study (n = 90, 42% in ADHD dyads). These studies enrolled parent dyads, half with and half without parental ADHD, to longitudinally examine early predictors of childhood ADHD. Participants were recruited through locally posted flyers and an online research registry either in pregnancy or immediately postpartum (New(born) PARIS) or when their infants were 6 to 10 months old (PARIS). Both parent studies shared data collection procedures, staffing, and measures used in the present analyses, and differed primarily in the enrollment timing and secondary recruitment strategies. PARIS additionally recruited eligible families via hospital-distributed postcards, whereas New(born) PARIS also employed in-person recruitment on the postpartum hospital floor and social media advertisements. Of total dyads with parental ADHD (47%), at least one parent met DSM-5 criteria for childhood ADHD with persistence into adulthood; 24 mothers and 36 fathers met criteria, including five dyads in which both parents had ADHD. Families were excluded if their infant was born before <37 weeks gestation, or with low birthweight (<5 lbs 8 oz) or prenatal exposure to illicit substances, determined by mother and father report. Participant characteristics are shown in Table 1.
Participant Characteristics.
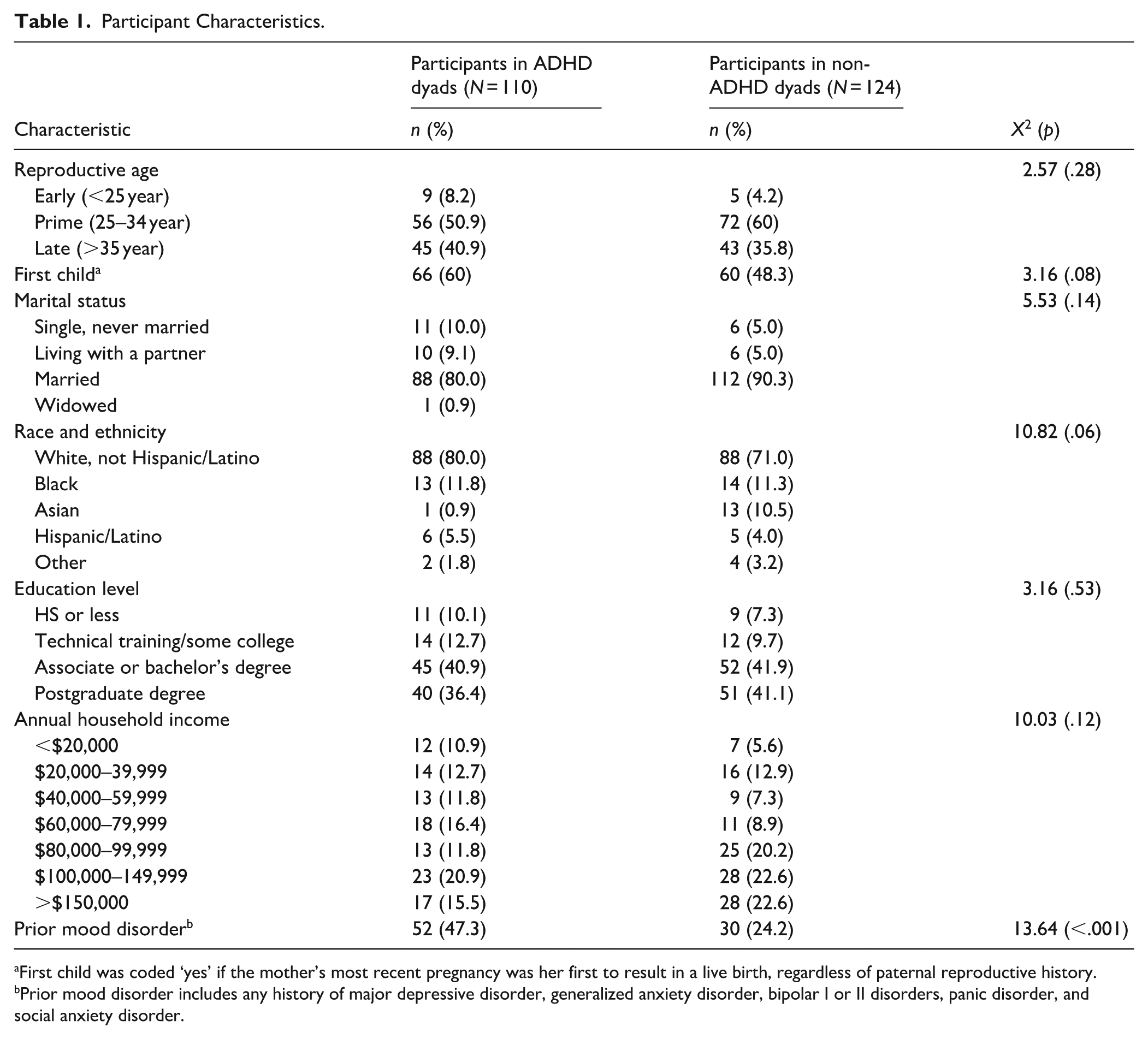
First child was coded ‘yes’ if the mother’s most recent pregnancy was her first to result in a live birth, regardless of paternal reproductive history.
Prior mood disorder includes any history of major depressive disorder, generalized anxiety disorder, bipolar I or II disorders, panic disorder, and social anxiety disorder.
Procedures
Participants participated in a research visit to assess for history of psychiatric disorders through the Structured Clinical Interview for DSM-5 Disorders (First et al., 2016) and verify participant-reported ADHD diagnoses using the Conners’ Adult ADHD Diagnostic Interview (CAADID; J. Epstein et al., 2001) shortly after their enrollment. These clinical assessments were conducted by master’s or doctoral-level clinicians, research-trained to assess if participants had history of mood disorder prior to enrollment (defined here as ever meeting criteria for major depressive disorder, generalized anxiety disorder, bipolar I or II disorders, panic disorder, or social anxiety disorder) and to evaluate ADHD across the lifespan. Parents also completed demographic questionnaires and measures of social support (on enrollment), and surveyed on symptoms of ADHD, depression, and anxiety (at 6–10 months postpartum) remotely using Qualtrics (Provo, UT). Informed consent was obtained prior to study participation. All families were compensated for their time and study protocols were approved by the University of Pittsburgh Institutional Review Board.
Measures
Mother and Father ADHD Symptoms
The Barkley Adult ADHD Rating Scale (BAARS-IV) is an 18-item questionnaire quantifying adult symptoms of inattention, hyperactivity, and impulsivity over the previous 6 months, which can be completed via self- or other-report (Barkley 2011). In prior work, the BAARS-IV has demonstrated excellent internal consistency (.95), test–retest reliability (.75), and strong convergent validity with the ADHD Symptom Rating Scale (Caroline et al., 2024). When infants in this sample were 6 to 10 months old, participants completed self-report ratings of their own ADHD symptoms (Crohnbach’s α = .94) and other-report ratings of their coparents’ symptoms (Crohnbach’s α = .93), such that both mothers and fathers offered ratings of themselves and their partners. Items are rated from 1 to 4 (range: 18–72) and total ADHD symptom scores were analyzed.
The Conners’ Adult ADHD Diagnostic Interview, Part II (CAADID) is a semi-structured, clinician-administered interview assessing ADHD symptoms and impairment in childhood and adulthood, with moderate test-retest reliability for adult and childhood report (.67–.69) and significant correlation between clinical interview and self-reported symptoms (.50–.52; J. N. Epstein & Kollins, 2006). In the present study, clinicians were blinded to any self- or coparent-reported ADHD symptom measures (i.e., BAARS-IV) prior to CAADID administration. Participants were identified as having ADHD (yes, no) if they met DSM-5 criteria for any presentation (6+ symptoms in childhood and 5+ symptoms in adulthood with impairment across the lifespan), and total symptom counts (range: 0–18) were used in regression analysis.
Depressive and Anxiety Symptoms
The Patient Health Questionnaire-8 (PHQ-8) is a brief 8-item self-report tool measuring severity of depressive symptoms in the previous 2 weeks with excellent sensitivity and specificity (Kroenke et al., 2009; Kroenke & Spitzer, 2002). Scores range from 0 to 24, with scores of 10 or greater indicating moderate-to-severe symptoms. The PHQ-8 differs from the PHQ-9 in its omission of one item on self-injurious/suicidal thoughts found to have low predictive accuracy for suicide risk; the PHQ-8 has similar specificity and minimally reduced sensitivity compared to the PHQ-9 (Wu et al., 2020) and strong internal consistency in our sample (Crohnbach’s α = .89). Additionally, a recent meta-analysis of PHQ-9 use in perinatal populations found it to be a highly sensitive (.84) and specific (.81) measure with significant convergent validity with the Edinburgh Postpartum Depression Scale (.59; Wang et al., 2021).
The Generalized Anxiety Disorder-7 (GAD-7) is a brief 7-item self-report tool measuring severity of generalized anxiety symptoms in the 2 weeks preceding assessment with excellent internal consistency across general and perinatal populations (≥.89) and significant convergent validity with other measures of self-esteem and resilience (Gόmez-Gόmez et al., 2024; Löwe et al., 2008; Lutkiewicz et al., 2024; Spitzer et al., 2006; Vogazianos et al., 2022). Scores range from 0 to 21, with scores of 10 or greater indicating moderate-to-severe symptoms (Crohnbach’s α = .93).
Social Support
The Maternal Social Support Index (MSSI) is a 21-item questionnaire about support with household chores and childrearing, and contact with neighbors, family members, significant others, and friends, with moderate internal consistency (.60–.63) and strong test-retest reliability (.72; Pascoe et al., 1981, 1988). Scores range from 1 to 19. While the instrument was originally validated for use with mothers across the perinatal period (Pascoe et al., 1982, 1988), we adapted it by substituting gender neutral language in Items 6 to 8 (e.g., “husband or boyfriend” replaced by “spouse or significant other”); mothers and fathers in our sample reported similar overall social support (Mfathers = 14.28, SD = 2.29; Mmothers = 14.29, SD = 2.50; Crohnbach’s α = .49).
Analysis
Primary outcomes were postpartum depressive and anxiety symptom scores, and the main predictors of interest were maternal and paternal ADHD symptoms, as captured by both participant-reported (BAARS-IV self-/other-report) and clinician-reported (CAADID) ratings. Intercorrelations and descriptive statistics were calculated for all variables.
A series of linear mixed-effects models with maximum likelihood estimation were used to regress depressive and anxiety symptom scores for individual participants on the primary predictors and covariates (including age, income, social support, and prior mood disorder history), while accounting for the clustering by parent dyad. Self-reported and clinician-reported ADHD ratings were assessed in parallel models and a Bonferroni correction applied such that α = .025. Secondary analyses examined differential results by parent sex (α = .05). Although hierarchical modeling was considered as an alternative approach, it was not pursued due to concerns that it would reduce statistical power and increase risk of overinterpretation in this exploratory study, as well as the lack of clear a prior theoretical basis for specifying order of predictors. All analyses were performed with SPSS software version 27.0 (Chicago, IL).
Subsequent univariate analysis assessed the independent effects of predictors on dichotomized outcome variables, using a cutoff score ≥10 on the PHQ-8 or GAD-7 to indicate moderate-to-severe depressive or anxiety symptoms, respectively. Low versus moderate/high social support was dichotomized as a score ≤25th percentile in our sample.
Results
Participants were predominantly White (75%), highly educated (80% had at least a college degree), and almost all were married or unmarried but cohabiting with a partner (92%). Although a greater proportion of participants in ADHD dyads had a history of mood disorders based on clinical interview (47% vs. 24%), no significant group differences were observed across other demographic variables, including dyads reporting first-time motherhood status (Table 1). Table 2 shows intercorrelations among study variables. Participant- and clinician-reported ADHD symptoms were strongly associated, with correlations between analogous BAARS-IV and CAADID scores for participants and coparents ranging from .62 to .78 (p < .001). Participants’ self-reported ADHD symptoms weakly correlated with their ratings of coparent ADHD symptoms, supporting inclusion of both as independent predictors in the participant-report ADHD regression models. Participant and coparent ADHD symptoms were moderately associated with prior mood disorder, but these associations did not rise above .32 (p < .05). Both self-reported (BAARS-IV) and clinician-reported (CAADID) coparent ADHD measures were also weakly negatively associated with social support (p < .05). Higher participant CAADID scores were weakly correlated with lower household income (p < .05). Associations between remaining independent variables did not rise above .50, validating inclusion in regression analysis.
Intercorrelations.
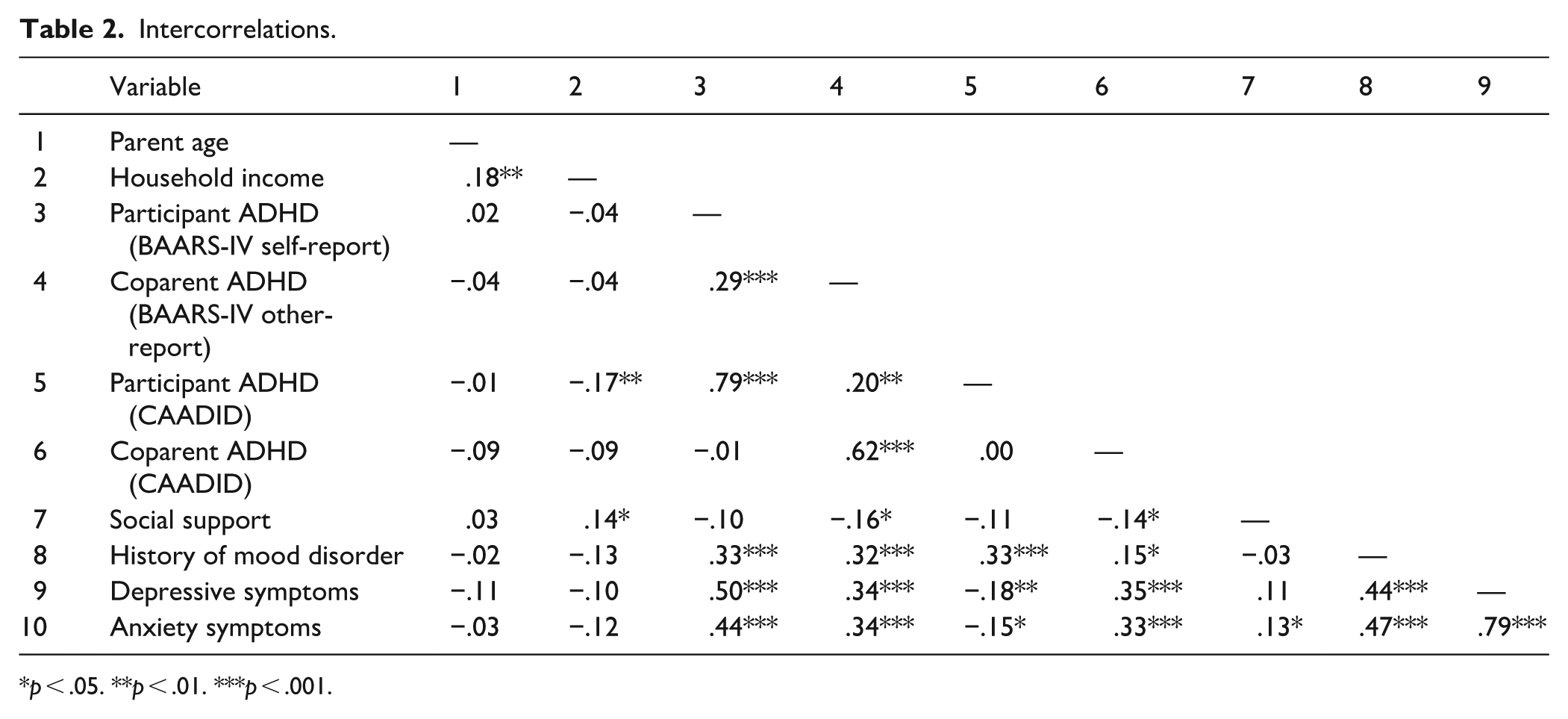
p < .05. **p < .01. ***p < .001.
Descriptive statistics are summarized in Table 3. Dyads with and without ADHD were compared on all measures, with participants in ADHD dyads reporting greater ADHD, depressive, and anxiety symptoms (p < .001, moderate effect sizes) and lower social support (p < .05, small effect size). Fifteen percent (n = 17) of parents in ADHD dyads met thresholds for moderate-to-severe depressive and anxiety symptoms, compared to 3% and 4% (n = 5, 4) of non-ADHD dyads. There were no statistically significant differences in maternal and paternal ADHD symptoms (self-reported or clinician-reported), mood symptoms, or social support, however, mothers rated their coparents’ ADHD symptoms higher than fathers did (26.97 ± 10.43 vs. 24.17 ± 6.48, p < .05). Additionally, mothers’ ratings of paternal ADHD appeared more strongly correlated with fathers’ self-reported symptoms (r = .63, p < .001) than the reverse (r = .46, p < .001), though this did not reach statistical significance (z-score = 1.84, two-tailed p = .07).
Descriptive Statistics and Comparison Between Participants in ADHD and Non-ADHD Dyads.
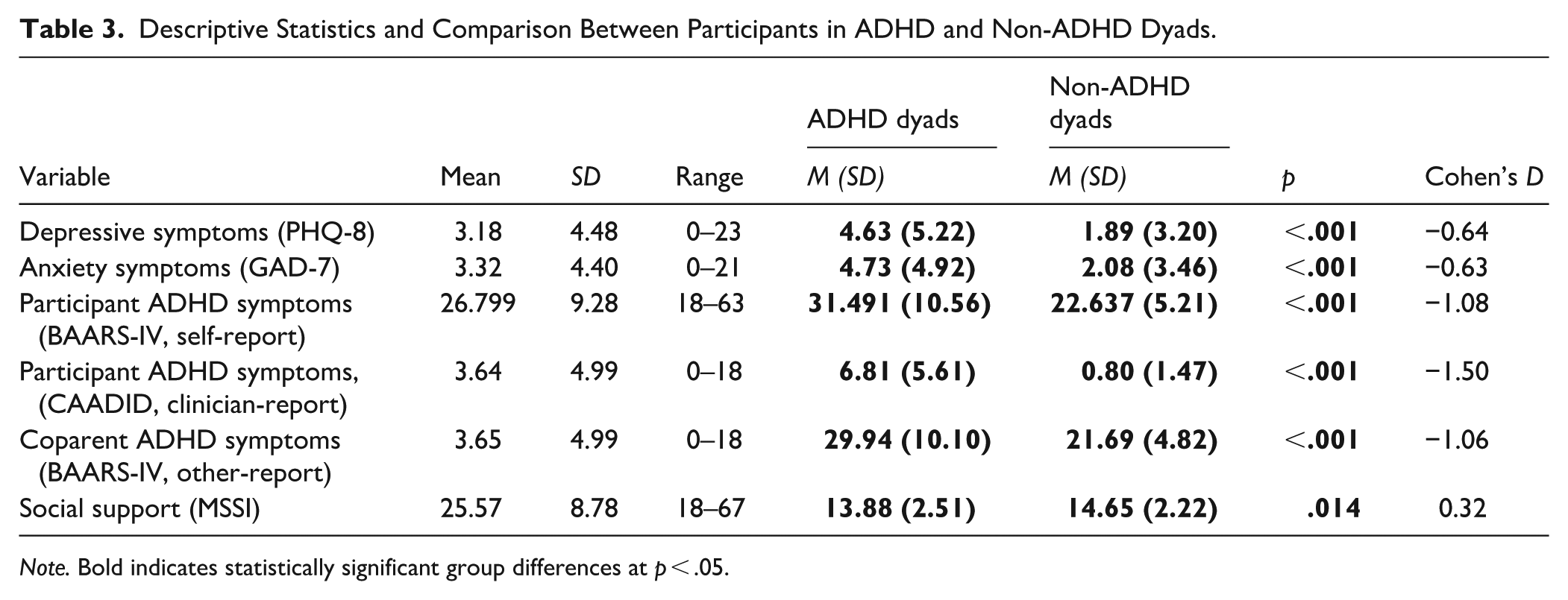
Note. Bold indicates statistically significant group differences at p < .05.
Models Predicting Depressive and Anxiety Symptoms
Table 4 presents the results of the primary analysis. Unconditional modeling of depression and anxiety outcomes revealed statistically significant random intercept clustering by parent dyad (p < .001) with intraclass correlations (ICC) of .27 and .20, respectively, supporting the use of mixed modeling. Participant ADHD symptoms and history of prior mood disorder were positively associated with depressive and anxiety symptoms across both participant-report and clinician-report ADHD models (p < .025). Coparent ADHD symptoms, however, predicted depressive and anxiety symptoms in the participant-report ADHD models only (p < .025). Social support was negatively associated with depressive symptoms in the clinician-report model but did not reach statistical significance (p < .05) in the self-report model.
Models Predicting Parental Depressive and Anxiety Symptoms.
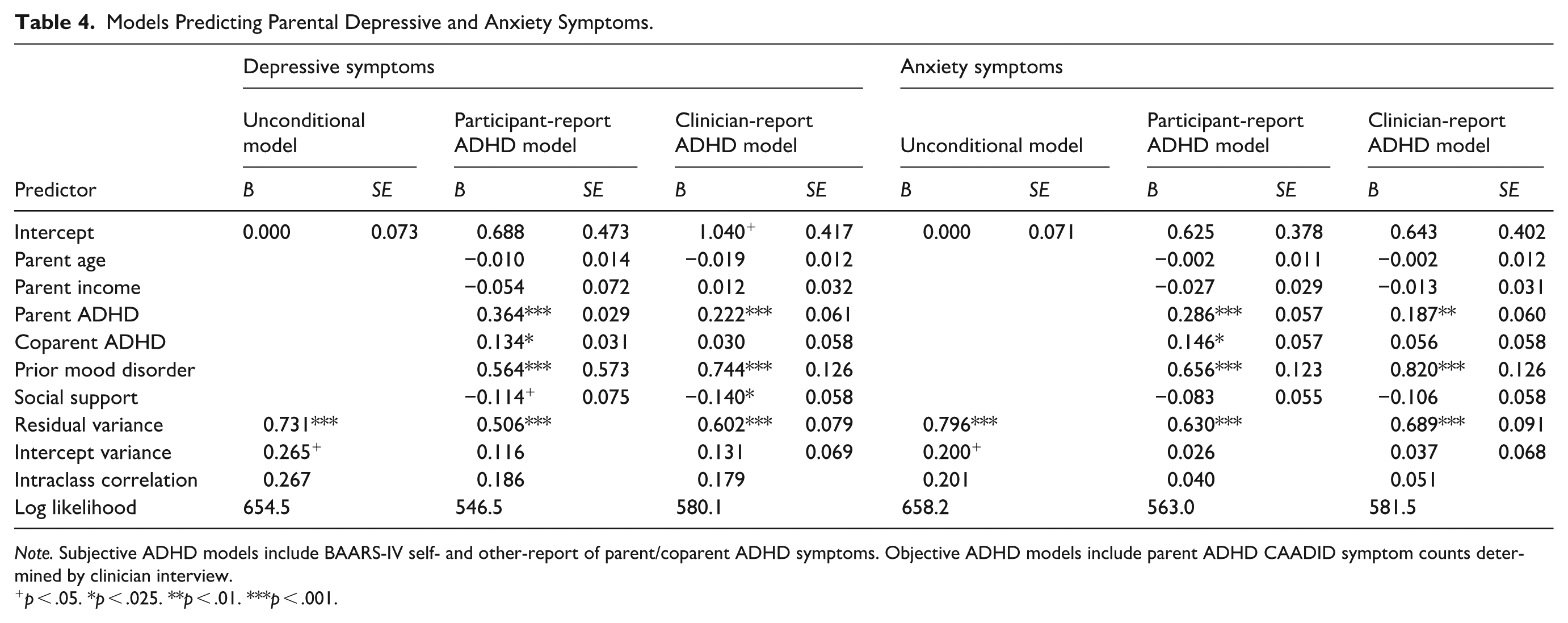
Note. Subjective ADHD models include BAARS-IV self- and other-report of parent/coparent ADHD symptoms. Objective ADHD models include parent ADHD CAADID symptom counts determined by clinician interview.
p < .05. *p < .025. **p < .01. ***p < .001.
Given significant differences in average maternal and paternal, but not clinician, ratings of coparent ADHD (as above), secondary analysis was performed using the self-report ADHD model only. Modeling of mothers and fathers separately (Table 5) demonstrated that regardless of parent sex, participant ADHD and prior mood disorder were significantly associated with both depressive and anxiety symptoms (p < .001). Among mothers, age was also negatively related to depressive symptoms (p < .01).
Differential Results by Parent Sex.
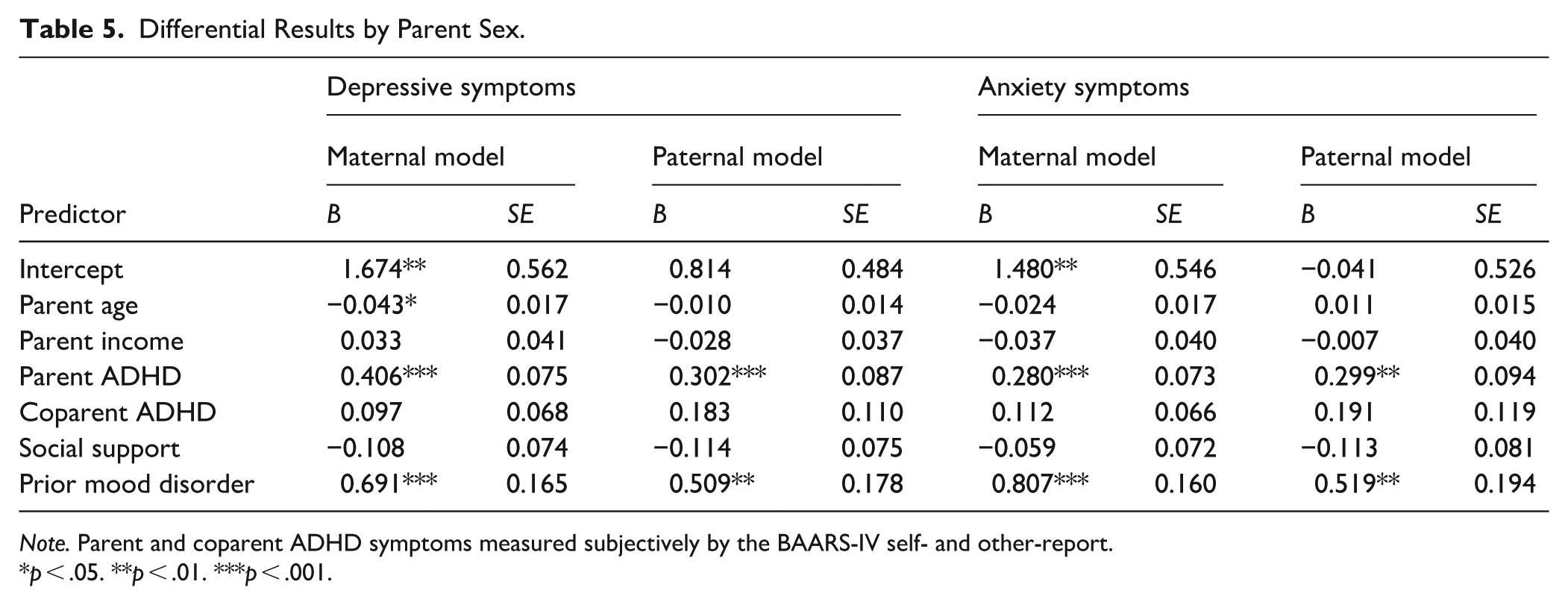
Note. Parent and coparent ADHD symptoms measured subjectively by the BAARS-IV self- and other-report.
p < .05. **p < .01. ***p < .001.
Univariate Analysis
Univariate analysis showed that having an ADHD diagnosis or history of prior mood disorder increased odds of developing moderate-to-severe depressive symptoms (OR = 2.70, 95% CI [1.10, 6.62]; OR = 14.98, 95% CI [4.28, 52.43]) and anxiety (OR = 4.58, 95% CI[1.82, 11.53]; OR = 13.97, 95% CI [3.98, 49.09]). Those who reported low social support were also more likely to experience moderate-to-severe depressive symptoms (OR = 0.27, 95% CI [0.11, 0.67]). Remaining variables were not statistically significant independent predictors of postpartum depressive and anxiety symptoms (Supplemental Table 1).
Discussion
This study investigated the association of parental ADHD with mental health in the first year of infant life and has several strengths, including the use of a family-centered approach reflecting interpersonal dynamics in the parenting environment. The dyadic study design allowed us to analyze ADHD symptoms and mental health outcomes for both parents. To the best of our knowledge, this study is the first to simultaneously explore the putative relationship between ADHD and postpartum mood symptoms in both birthing and non-birthing parents or to assess coparent ADHD as an environmental risk factor for postpartum psychopathology. In this study, depressive and anxiety symptoms were modeled separately to facilitate examination of the distinct impacts of parent and coparent ADHD on these outcomes. However, the similarity of findings across these constructs suggests substantial overlap in how depression and anxiety were influenced by predictor variables, highlighting the potential value of using a combined measure, such as the Edinburgh Postnatal Depression Scale, in future studies and clinical settings to more efficiently capture shared variance or screen for families at risk.
Associations found between symptoms of ADHD, depression, and anxiety supported our hypothesis that participant ADHD and postpartum mood symptomology would be positively correlated. Results are consistent with previous literature noting increased postpartum depression in mothers with ADHD diagnoses or symptoms during pregnancy, and studies finding that women with ADHD may experience greater vulnerability to hormone-related mood disorders throughout their lifetimes (Andersson et al., 2023; Dorani et al., 2021; Jones et al. 2018). Moreover, the analogous relationship between ADHD and postpartum mood among the fathers in our sample echoes recent findings from a cohort of Canadian fathers (Dennis et al., 2022). The robustness of the association between participant ADHD symptoms and postpartum mood symptoms (regardless of parent sex) to dichotomous and dimensional analyses supports the likelihood that this relationship rises to a level of clinical significance, and further suggests parental ADHD diagnoses may serve as clinically useful targets for antenatal intervention in the future. However, recent research has shown that a significant proportion of those diagnosed with childhood ADHD experience a fluctuating course of ADHD symptoms throughout adulthood (Sibley et al., 2022). The stress of becoming a parent has the potential to exacerbate ADHD-related impairments in a variety of individuals, including those with previously remitting or subthreshold symptoms, underscoring the importance of developing a nuanced understanding of how ADHD symptom severity relates to postpartum mood irrespective of diagnostic status.
Coparent ADHD symptoms were also associated with depressive and anxiety symptoms, but only when those ADHD symptoms were participant-reported rather than clinician-reported. Although prior literature has not described the effects of coparent ADHD on postpartum mental health, this aligns with our current understanding of coparent mood disorders and relationship stress as key risk factors for postpartum depression in both mothers and fathers (Clifford et al., 2024; Estlein & Shai, 2023). The transition to parenthood drastically increases individual and shared responsibilities within the family unit and may disrupt interpersonal dynamics, particularly if one coparent is struggling with heightened executive dysfunction and emotional dysregulation associated with ADHD. These results took prior mood disorder into account which suggests that postnatal depression and anxiety experiences are above and beyond preexisting vulnerability. We also noted an inverse relationship between social support and depressive symptoms in both univariate and regression analyses, implying increasing social support could potentially mitigate negative impacts of coparent ADHD across the parental dyad.
Statistical significance of coparent ADHD in the self-report, but not clinician-report ADHD models is likely due in part to underlying differences in the two ADHD measures regarding time frame, reporter, and severity; the CAADID notes symptom counts across adulthood, whereas the BAARS-IV specifically queries symptom count and severity in the 6 months prior to assessment. Additionally, while clinicians may be better equipped to differentiate normative from nonnormative behaviors in ADHD assessments, participants may offer a more accurate contemporary picture of their coparents’ ADHD symptoms by virtue of greater firsthand exposure to coparents in activities of daily living. Alternatively, parents struggling with postpartum depressive symptoms may report greater coparent ADHD symptoms because of cognitive distortions associated with emotional dysregulation. Individuals with depression and anxiety are more likely to produce negative interpretations of ambiguous, or even positive, situations (Hirsch et al., 2016; Kube et al., 2020), and the magnitude of this negativity bias has been found to vary with the severity of mood symptoms (Lee et al., 2016). It is possible that through the lens of such cognitive distortions, participants with disordered mood might find coparent ADHD particularly disruptive and rate their ADHD symptoms more severely.
Secondary analyses revealed that statistically significant predictors of postpartum depressive and anxiety symptoms were largely the same for mothers and fathers, with participant ADHD symptoms and prior mood disorder history associated with postpartum mood symptoms regardless of parent sex. Across all regression analyses, prior mood disorder represented the strongest correlate of either depressive or anxiety symptoms compared to other variables, including parent or coparent ADHD, which is consistent with the wealth of literature identifying lifetime history of depression, anxiety, or other psychiatric disorders as the greatest known predictor of postpartum depression (Guintivano et al., 2018). Similarity in maternal and paternal predictors of postpartum depression has been found in previous studies, which generally identify aggregate psychiatric history, coparent psychopathology, and social support as primary risk factors among all parents (Anding et al., 2016; Da Costa et al., 2019; Guintivano et al., 2018; Matthey et al., 2000). The association between maternal age and postpartum depressive symptoms aligns with previous findings in the literature (Silverman et al., 2017) but may also be accounted for by the small but statistically significant age disparity (<1.5 years) among mothers and fathers in our sample.
While our study design offered several advantages (e.g., both parents interviewed, ADHD diagnosis confirmed using standardized assessments, specific developmental window infrequently studied), the generalizability of these findings is limited by other study characteristics. Because we chose to investigate depressive and anxiety symptoms as separate outcomes, measures utilized (PHQ-8 and GAD-7) were not specific to the postpartum period, meaning some aspects unique to postpartum psychopathology, such as intrusive thoughts or worries of harming the infant, were not captured by these analyses. The relative socioeconomic and racial homogeneity of our sample, which was predominately White and highly educated, limits our ability to generalize results to more diverse populations. We also recognize that childrearing occurs in many configurations that may or may not revolve around the biological parent dyad, and caregivers in different, including nonnuclear, family structures may experience the stresses of parenthood differently. Because all participants identified as cisgender, results may not be generalizable to the gender-diverse community or those in non-heterosexual relationships. However, the study established parent/coparent ADHD as a predictor of postpartum mood symptoms in the overall sample and it is likely this association may be present regardless of parent gender or gestational status, given additional stressors associated with minoritized identities. Finally, we were unable to study potential effects of ADHD medication on postpartum mood given only 5% of the overall sample endorsed ongoing pharmacologic treatment of ADHD.
Conclusions
Overall, these findings demonstrate that parental ADHD contributes to poorer postpartum mental health across the parental dyad, suggesting optimization of ADHD symptoms during the perinatal period may be critical to parental wellness. As ADHD is increasingly recognized and diagnosed in people of reproductive age, supporting this population requires a more nuanced understanding of the frequency and severity of symptoms throughout the transition to parenthood. Identification of which specific experiences of parenthood are most impaired by ADHD symptoms may provide targets for individualized interventions to benefit the mental health of parents with ADHD and their coparents, supporting familial resilience.
Supplemental Material
sj-docx-1-jad-10.1177_10870547261438170 – Supplemental material for Unmasking Potential Impacts of Parent and Coparent ADHD on Mental Health in the First Year Postpartum
Supplemental material, sj-docx-1-jad-10.1177_10870547261438170 for Unmasking Potential Impacts of Parent and Coparent ADHD on Mental Health in the First Year Postpartum by Elyse G. Mark, Leslie A. Rajendran, Lindsay Taraban, Michelle A. Wilson, Brooke S. G. Molina and Heather M. Joseph in Journal of Attention Disorders
Footnotes
Ethical Considerations
This research study was conducted with approval from the University of Pittsburgh Institutional Review Board (STUDY19070377 and STUDY19040368).
Consent to Participate
Informed consent for data collection and publication was obtained from all individual participants included in the study.
Author Contributions
All authors made substantial contributions to the conception or design of the work. Data collection: Michelle Wilson, Elyse Mark, Heather Joseph. Methodology: Elyse Mark, Heather Joseph, Brooke S. G. Molina. Formal analysis and investigation: Elyse Mark. Writing – original draft preparation: Elyse Mark, Leslie Rajendran. Writing – review and editing: Heather Joseph, Lindsay Taraban, Michelle Wilson, Brooke Molina. Funding acquisition: Heather Joseph, Elyse Mark, Lindsay Taraban. Supervision: Heather Joseph and Brooke Molina. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by: the Klingenstein Third Generation Fellowship in ADHD (Joseph); American Academy of Child and Adolescent Psychiatry (AACAP), Young Investigator Award (Joseph); National Institutes of Mental Health (NIMH), MH121585 (Joseph); National Center for Advancing Translational Sciences, TR001856 (Joseph); University of Pittsburgh Clinical and Translational Science Institute, TSI UL1 TR001857 (Joseph); NIMH, MH018269 (Taraban); NIMH, T32 MH01895 (Mark), and AACAP Summer Medical Student Fellowship (Mark).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author* upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.