
Abstract
Objective:
ADHD and internalising symptoms such as anxiety and depression are known to be associated in adolescence and understanding the mechanisms linking them is important for improving mental health outcomes for adolescents with ADHD symptoms. Our objective was to examine these mechanisms.
Method:
In this study, we leverage a high-quality longitudinal dataset, the Millennium Cohort Study (n = 2,607 male, n = 2,791 female) to simultaneously evaluate a range of hypothesised mediating mechanisms. These include indirect effects via peer problems, conduct problems, self-esteem, injuries and accidents, relationships with parents, academic performance, risky decision-making, parental mental health, educational motivation, and general health. We used exploratory longitudinal mediation analysis with regularised structural equation modelling (regSEM) to examine 14 candidate mediators of the ADHD-internalising association across ages 11, 14 and 17.
Results:
Regularisation with lasso did not result in the de-selection of any of these mediators; however, only two were statistically significant.
Conclusion:
Results suggest there may be many mediators of small effect involved in the relation between ADHD symptoms and later internalising problems but point to self-esteem and parental mental health as priority mechanisms for further study in future causal and interventional research.
Introduction
Young people with ADHD symptoms commonly experience internalising problems such as anxiety and depression, with rates in this population exceeding those of the general population (Baxter et al., 2013; Krone & Newcorn, 2015). For example, estimates suggest that approximately 25% of young people with ADHD also meet diagnostic criteria for an anxiety disorder (D’Agati et al., 2019) and approximately 40% experience a depressive episode before the age of 30 (Meinzer et al., 2013). Illuminating the mediators of this association is important for informing interventions to reduce their co-occurrence, especially through prevention of internalising problems secondary to ADHD symptoms. Adolescence is a critical period in this respect. It is associated with a range of challenges, including increased expectations of independence, academic and social stressors, and emotional changes that can increase the risk of internalising problems (Rapee et al., 2019). These challenges may compound pre-existing vulnerabilities present among young people with ADHD symptoms.
Many and varied factors have been proposed to mediate the links between ADHD symptoms and internalising problems. Theoretical models such as the cognitive behavioural and dual failure models propose, for example, that impairments or ‘failures’ in various life domains can lead to a negative self-concept and increased risk of depression (Eadeh et al., 2017; Roy et al., 2015). Indeed, studies have suggested that facing challenges such as social skills and peer difficulties such as peer rejection, victimisation or dislike; problems with school work; difficulties in relationships with parents, and behavioural problems (Eadeh et al., 2017; Eddy et al., 2018; Feldman et al., 2017; Gordon & Hinshaw, 2017; Humphreys et al., 2013; Powell et al., 2020; Roy et al., 2015) mediate associations between ADHD symptoms and internalising problems. Other models focus on co-occurring cognitive-behavioural features of ADHD and/or internalising problems as mediators. For example, studies have identified factors such as emotion (dys-)regulation (Antony et al., 2022; Bodalski et al., 2019; Murray, Wong, et al., 2021; Seymour et al., 2012), reward processing, self-control (Feldman et al., 2017), maladaptive cognitions and cognitive-behavioural avoidance (Knouse et al., 2013), sluggish cognitive tempo (Sevincok et al., 2020), locus of control (Ostrander & Herman, 2006) and rejection sensitivity (Bondü & Esser, 2015) as mediators of ADHD-internalising problem associations. Finally, a number of studies have identified a potential role of parenting, for example, overprotective parenting (Meyer et al., 2022) or parent behaviour management (Ostrander & Herman, 2006).
Previous studies analysing mediators have, however, often found that specific mediators individually explain only a modest proportion of the association between ADHD symptoms and internalising problems (Powell et al., 2020; Roy et al., 2015). This suggests that there may be a large number of mediators each of small effect. However, because existing studies have typically focused on only a handful at a time, a comprehensive picture of their combined effects remains lacking. Further, a focus on only a handful of mediators at a time makes it difficult to infer which mediating mechanisms might be of particular importance, explaining larger unique proportions of the ADHD symptoms and internalising problems association.
More comprehensive analyses can be used to build and test more encompassing theories of the relations between ADHD and internalising problems in adolescence. They can also play an important role in the early stages of designing a research programme to illuminate intervention targets. For example, comprehensive mediation analyses in existing observational data can highlight which mediators are most promising to investigate further as intervention targets. However, even when a candidate mediator is identified, confirming a causal role is challenging and cannot typically be done conclusively without resource intensive research designs (such as randomised controlled experiments). There is thus considerable value in providing initial exploratory evidence on which mediators represent promising targets for further study before embarking on confirmatory research (Serang & Jacobucci, 2020).
Exploratory mediation within a SEM framework that implements regularisation on the mediation parameters (a technique also known as ‘regSEM’) can provide this kind of evidence. It facilitates the analysis of large numbers of mediators and uses regularisation to select only those that might be considered to have non-trivial effects. The approach has been used in several previous psychosocial health studies to facilitate mediator selection where there are a large number of candidate mediators (Ammerman et al., 2018; O’Loughlin et al., 2021). For example, Ammerman et al. (2018) used regSEM to identify a subset of 11 of 46 variables that contributed to the effects of childhood maltreatment on suicidality in females, while none of the 46 candidate variables were selected in males (Ammerman et al., 2018). Similarly, Casini et al. (2021) used regSEM to select emotion regulation mediators of the association between rejection sensitivity and the outcomes of aggression, withdrawal and prosociality (Casini et al., 2022).
These applications illustrate the value of regSEM for identifying candidate mediators for further study. In this study, we, therefore, apply the technique to identify the most promising mediators in the association between ADHD symptoms and internalising problems in adolescence in a large UK-based study with adolescent participants. The goal is not to examine which mediators are causal at this stage but to identify – using large-scale observational data – a subset of mediators that may be most relevant to further examine with more causally-tailored designs in future research (e.g., in causal mediation adjusting for confounders or interventional designs). Based on data availability and past literature we evaluated a range of candidate mediators for inclusion in our models. We use longitudinal mediation analysis given the empirical importance of modelling autoregressive effects and the conceptual centrality of temporal ordering in modelling mediating effects (Maxwell & Cole, 2007). We conducted whole-sample analyses as well as analyses stratified by sex, to explore the possibility that males and females may show different patterns of mediation in the relation between ADHD symptoms and internalising problems. This is motivated by evidence that females both with and without ADHD symptoms overall show more internalising problems (Hollingdale et al., 2023; Williamson & Johnston, 2015), Recent evidence has suggested an escalation in internalising problems in the transition to adolescence that is not observed in males (Wang et al., 2026), raising the possibility that there may also be mediating mechanisms that are more salient in females than males.
Method
Participants
We used data from the waves of Millennium Cohort Study (MCS) (Connelly & Platt, 2014) taking place during participants’ adolescence (ages 11, 14 and 17). MCS is a UK-based longitudinal birth cohort study fully documented and available at: https://ukdataservice.ac.uk/. In brief, the first wave of MCS took place in 2000 to 2002 when participants were aged 9 months old. Participants were sampled using a stratified random sampling design in which individuals were clustered geographically and disproportionately sampled from the three smaller nations of the UK (Scotland, Wales and Northern Ireland), disadvantaged areas and ethnic minorities. For our main analyses, we used data from n = 5,398 participants (2,610 male, 2,788 female), reflecting the number of participants with complete data on the measures included in the current analysis. For additional analyses, the specific sample sizes are shown in the table notes. The sociodemographic information for the included subsample is provided in Table 1. To examine the impact of this selection on the representativeness of our sub-sample, we compared our sub-sample to the non-selected participants on the basis of sociodemographic variables, ADHD diagnosis and symptoms and internalising problems (see Supplementary Materials) and found that there were differences between the analytic and excluded sample on child ethnicity, parental highest academic qualifications and ADHD and internalising symptoms. Given this, where possible, sensitivity analyses including the whole sample with at least some data on the endogenous variable (n = 11,723), using FIML to address missing data are included.
Sample Demographic Characteristics for Included Versus Excluded Cases.
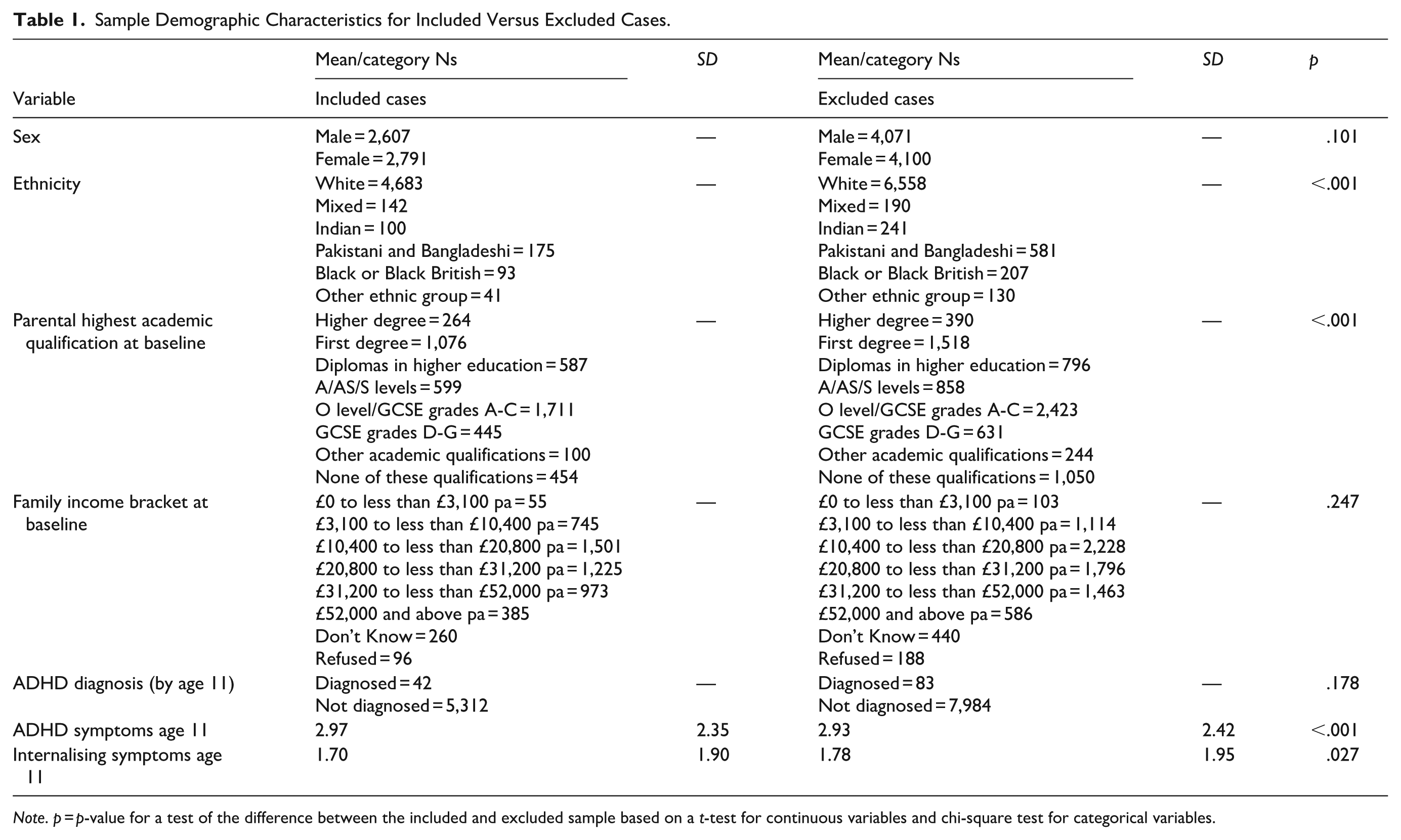
Note. p = p-value for a test of the difference between the included and excluded sample based on a t-test for continuous variables and chi-square test for categorical variables.
Measures
ADHD Symptoms
ADHD symptoms were measured with the hyperactivity/inattention subscale of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997). The SDQ is one of the most widely used and well-validated behavioural screening instruments for children (Kersten et al., 2016), including in the current sample where it has shown good psychometric properties, including a high degree of gender, informant and developmental invariance (Murray et al., 2022; Murray, Speyer, et al., 2021). Though there is some debate around the appropriate cut-point, the hyperactivity/inattention subscale has shown good discrimination with respect ADHD diagnosis (Algorta et al., 2016; Riglin et al., 2016). The subscale includes five items that refer to the last six months, with reference to the following behaviours: ‘restless, overactive, cannot stay still for long’; ‘constantly fidgeting or squirming’; ‘easily distracted, concentration wanders’; ‘thinks things out before acting’; and ‘sees tasks through to the end, good attention span’. Responses were provided on a 3-point Likert-type scale with options: not true (0), somewhat true (1) and certainly true (2). Positively worded items were reverse-coded, and item responses were summed to produce an overall hyperactive/inattentive score with higher scores indicating greater hyperactivity/inattentiveness (possible range = 0–10). We used the parent-reported version of the SDQ, as the only version available at all of age 11, 14 and 17.
Internalising Problems
Internalising symptoms were measured with the emotional problems subscale of the SDQ (described above). The emotional problems items refer to: often complaining of headaches, stomach-aches or sickness; having many worries; being often unhappy, down-hearted, or tearful; being nervous or clingy in new situations; and having many fears, being easily scared.
Candidate Mediators
Full details of the candidate mediator measures are provided in Supplementary Materials. They were included if (i) they were available at both age 11 and age 14, in order to allow for the adjustment of relevant autoregressive effects in the longitudinal mediation model; (ii) prior theory or empirical studies have suggested they could plausibly act as a mediator in the association between ADHD symptoms and internalising problems in adolescence. They were: prosociality, peer problems, conduct problems, self-esteem, injuries and accidents, closeness of relationship with primary caregiver, academic performance, risk-taking behaviours on the Cambridge Gambling Task (CGT), parental mental health and educational motivation.
Statistical Procedure
Exploratory Mediation Analysis
We followed the exploratory mediation analysis with SEM procedure described by Serang et al. (2017), modifying it for longitudinal analysis. We first specified a full SEM model in which age 17 internalising problems were regressed on age 14 mediating variables and age 11 ADHD symptoms (the ‘direct’ effect) and age 14 mediating variables were regressed on age 11 ADHD symptoms. The 14 indirect effects were calculated as the products of the coefficients for the regression of internalising problems (age 17) on the relevant mediator (age 14) and the regression of that mediator on ADHD symptoms (age 11). We additionally included the regression of age 17 internalising problems on age 14 internalising problems and ADHD symptoms and the autoregressive and cross-lagged effects of ADHD symptoms, internalising problems and mediators across the age 11 to age 14 lag. We did not include the mediators at age 17 given our focus on their role as mediators and because not all mediators were available at age 17. Where relevant, latent variable measurement models for constructs were used (i.e., for ADHD symptoms, internalising problems, prosociality, peer problems, conduct problems, self-esteem and parental mental health). The full model specification can be seen in the R code: https://osf.io/ap95r
Figure 1 provides a simplified example of the multiple path mediation model fitted. Paths a1-ak label the paths from ADHD symptoms to the mediators, paths b1-bk label the paths from the mediators to internalising problems, and c′ is the direct effect from ADHD symptoms to internalising problems. From the a and b parameters, indirect effects via each mediator (shown in bold) are derived by finding the product a*b. The total effect of ADHD symptoms on internalising problems is then the sum of the indirect effects and c′.
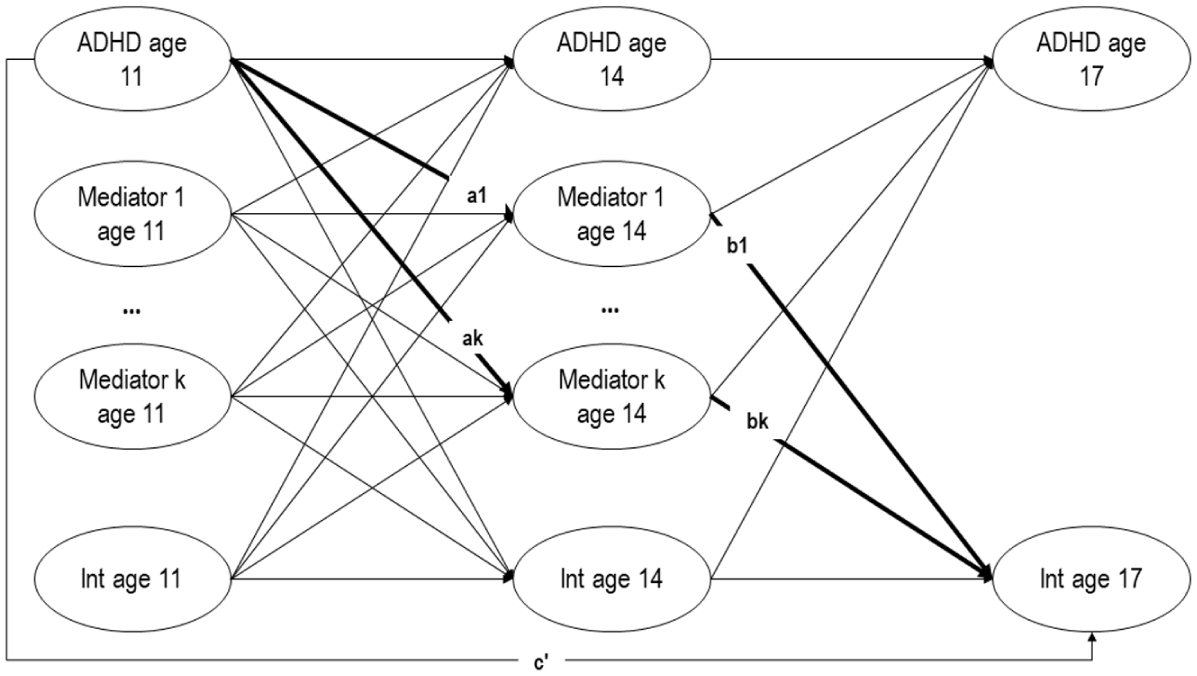
Simplified path mediation model.
In the approach proposed by Serang et al. (2017), the above-described multiple mediation model is fit using regularised SEM (‘RegSEM’) (Jacobucci et al., 2016). Regularised SEM incorporates a penalty term into the maximum likelihood function used for model fitting:

where
First, all continuous variables were standardised to have a mean of 0 and variance of 1 (for the constructs specified using latent variables the latent variable variance was fixed to 1). Next, the tuning parameter value was found by testing 100
Results from the final models are reported in terms of the direct and indirect effects, with the fully standardised indirect effect used as an effect size measure. The fully standardised indirect effect is here defined as:

This is equivalent to the product of standardised regression coefficients and is recommended over measures such as the ‘proportion of mediated effect’ because it has fewer limitations/ more desirable properties as an effect size metric (Lachowicz, 2017). It can be interpreted in a similar way to the standardised regression coefficient and represents the expected standard deviation (SD) change in the outcome variable (internalising problems) for a one SD increase in the predictor (ADHD symptoms) via the relevant mediator variable.
Analyses were first run on the whole sample, followed by male and female subsamples, the latter to explore the possibility that there are different mediating mechanisms in males versus females.
Results
Descriptive Statistics
Descriptive statistics are provided in Table S1 of Supplementary Materials.
Initial Models with No Regularisation in Whole Sample
R code is provided at: https://osf.io/ap95r. For reference, SEMs fit without any regularisation are provided in Table 2 (complete case analysis) and Table 3 (FIML analysis). The complete case analysis yielded three significant mediators: self-esteem (β = −.092, p < .001), risk adjustment (β = −.009, p = .034) and parental mental health (β = −.02, p = .002). When fitting this model with FIML to utilise the whole sample (n = 11,723), the pattern of results was very similar, with significant mediating effects for self-esteem and parental mental health. Risk adjustment, which was on the margins of statistical significance in the complete case analysis was not significant in the FIML analysis.
Indirect Effects Prior to Regularisation for Complete Case Analysis in Whole Sample.
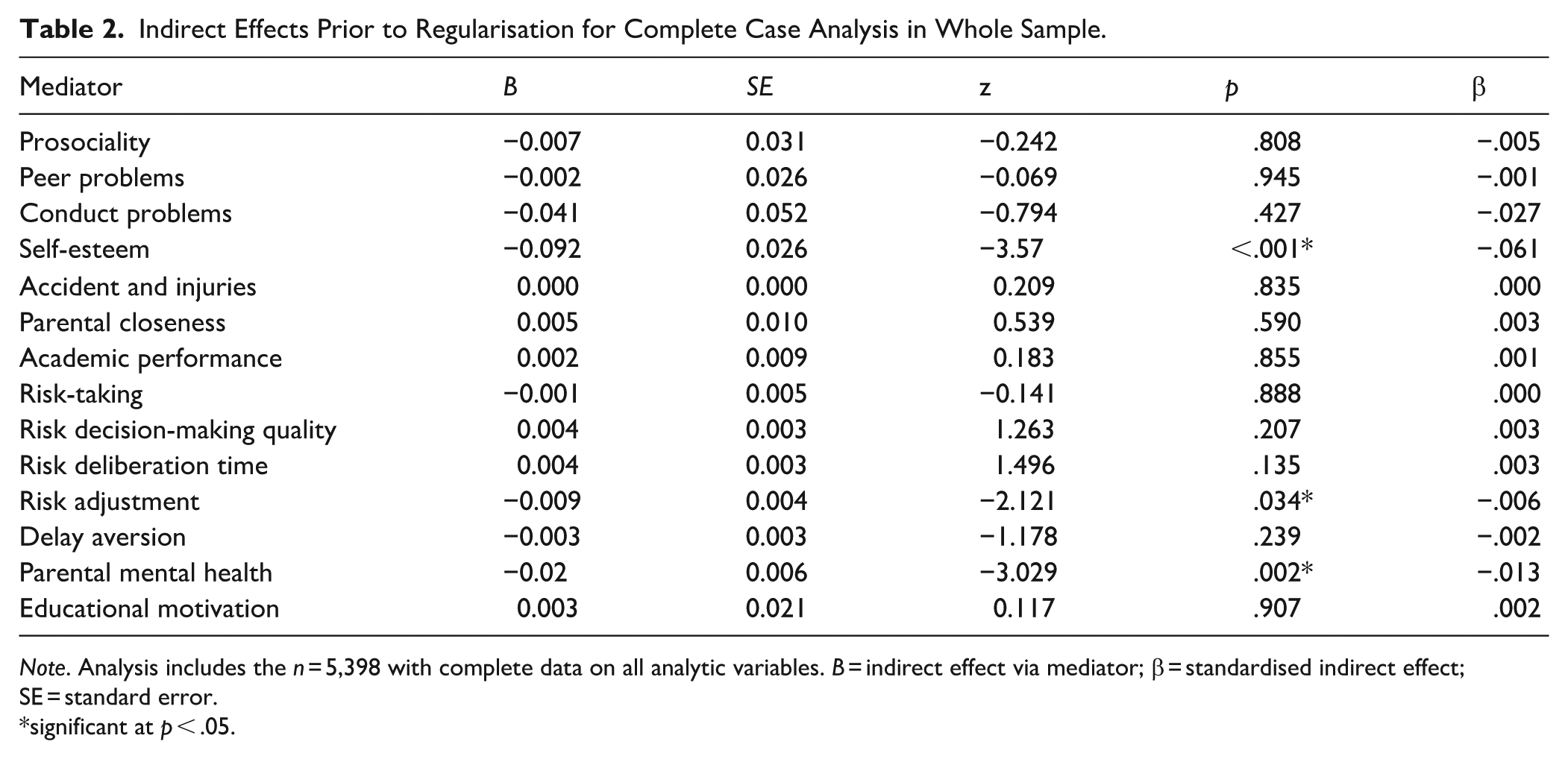
Note. Analysis includes the n = 5,398 with complete data on all analytic variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
significant at p < .05.
Indirect Effects Prior to Regularisation Using FIML in Whole Sample.
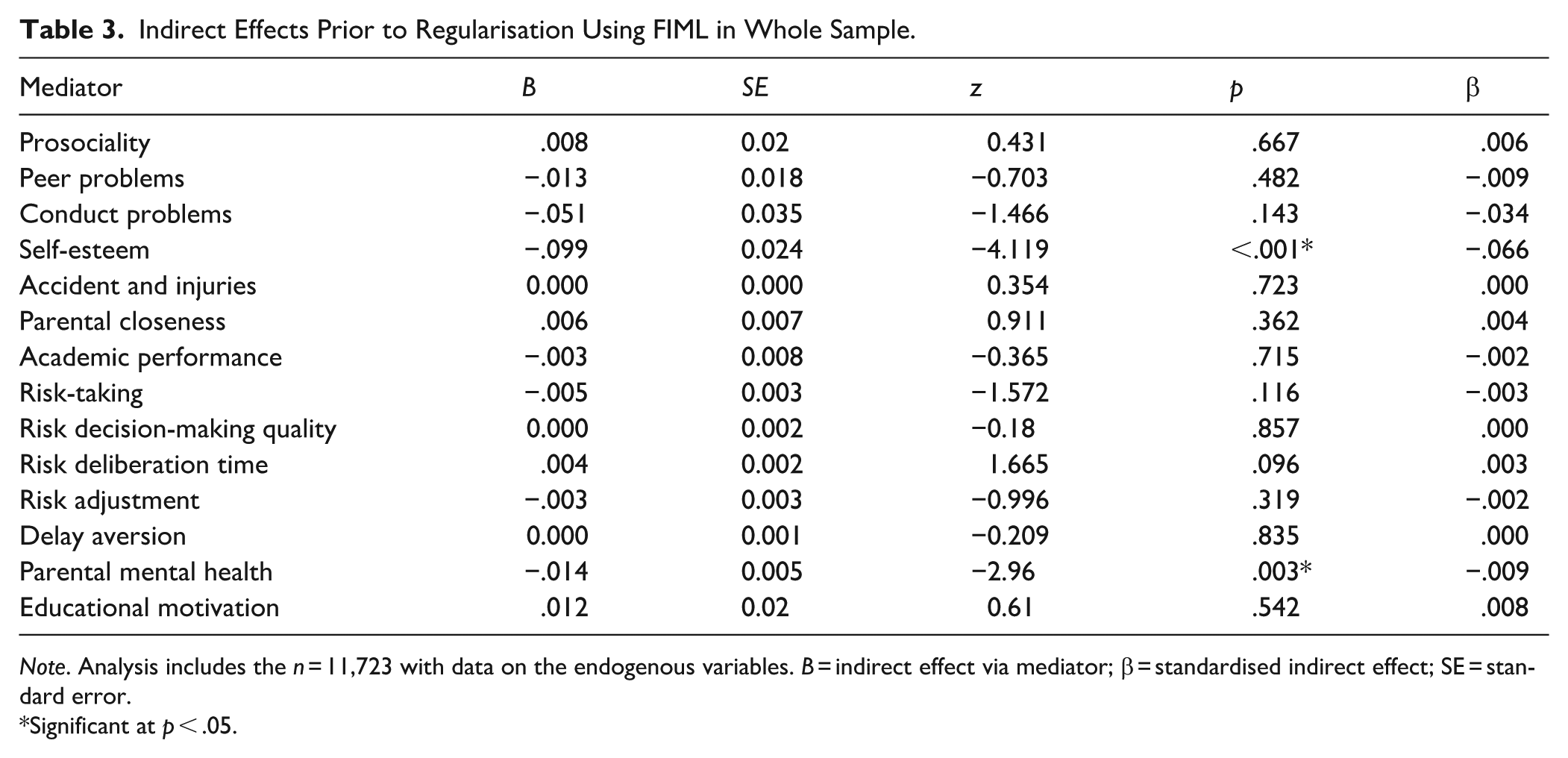
Note. Analysis includes the n = 11,723 with data on the endogenous variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
Significant at p < .05.
Regularised Models in Whole Sample
After discarding any models with tuning parameters that did not converge (which included all models with a
Initial Models with no Regularisation in Male and Female Subsamples
The indirect effects from sex-stratified SEMs without regularisation are provided in Tables 4 and 5 (complete case and FIML analyses respectively). Following the analyses in the whole sample that suggested that any
Indirect Effects Prior to Regularisation Using Complete Case Analysis in Male and Female Sub-samples.
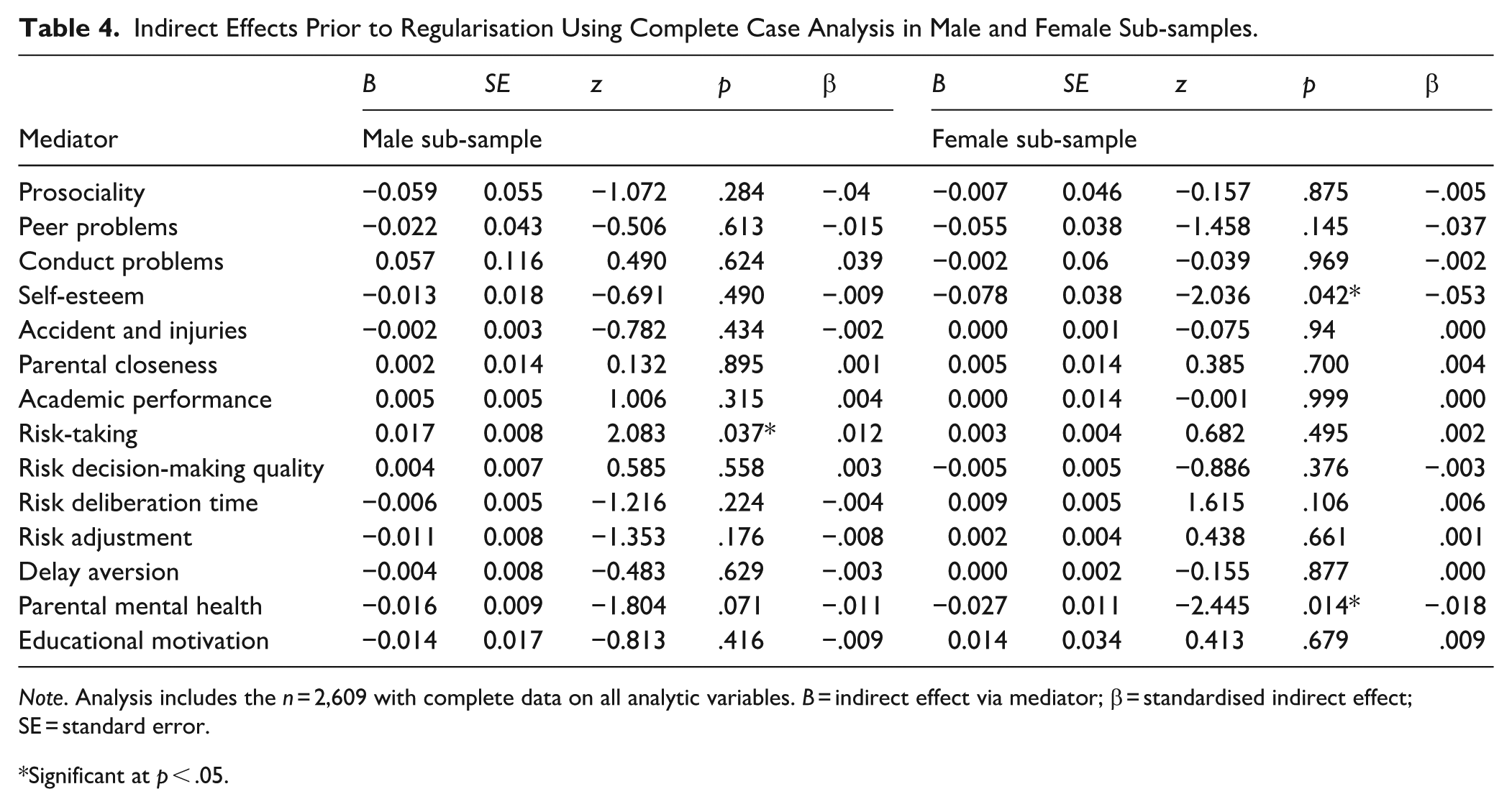
Note. Analysis includes the n = 2,609 with complete data on all analytic variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
Significant at p < .05.
Indirect Effects Prior to Regularisation Using FIML in Male and Female Sub-samples.
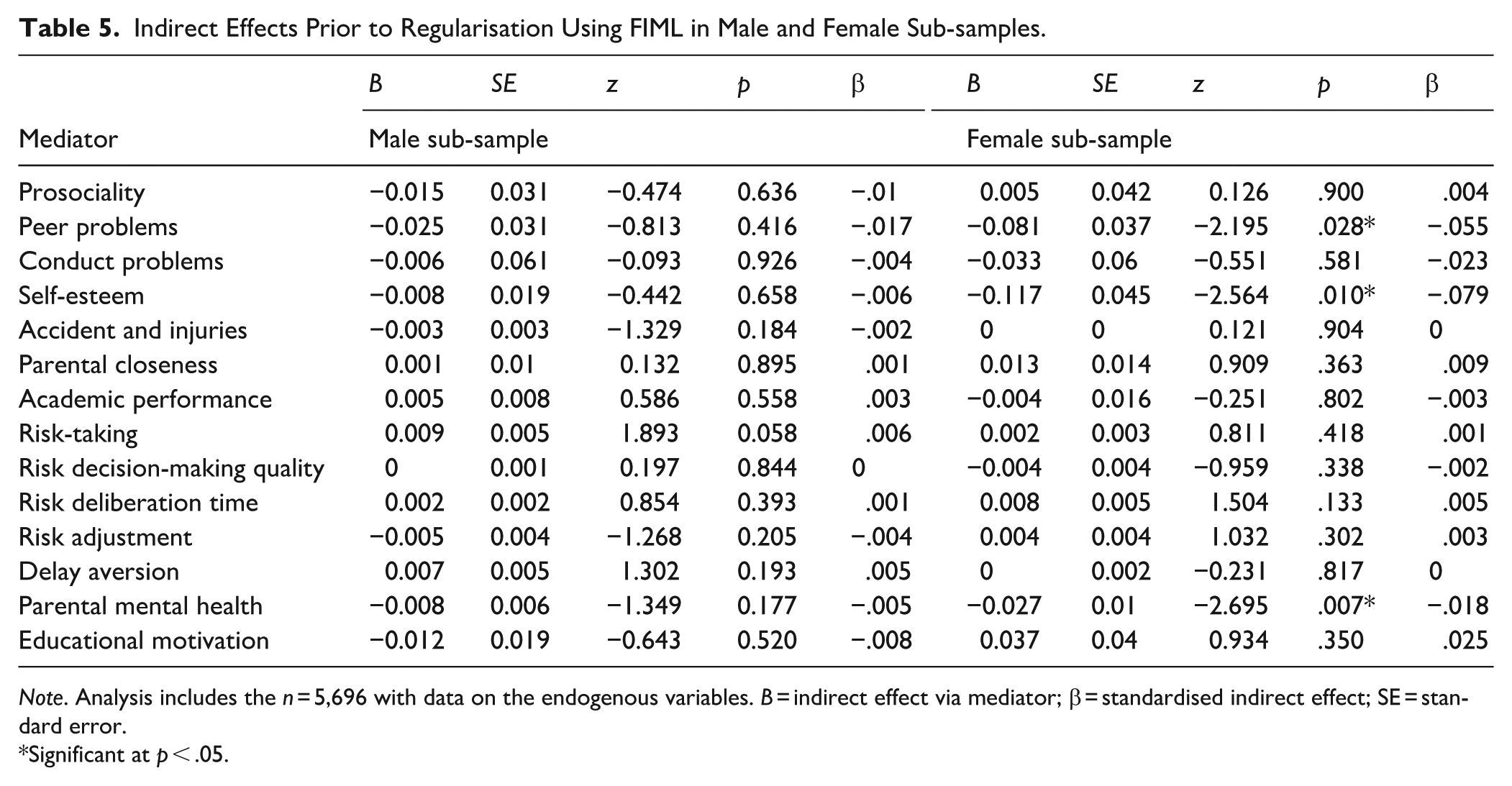
Note. Analysis includes the n = 5,696 with data on the endogenous variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
Significant at p < .05.
In the female sub-sample, the significant mediating effects via self-esteem (B = 0.078, p = .042) and parental mental health (B = −0.027, p = .014) seen in the whole-sample analyses were present but there were no other significant mediating effects. The direct effect was non-significant (B = 0.093; p = 230). In the female sub-sample, FIML analyses the direct effect of ADHD symptoms on internalising problems was also non-significant (B = 0.114, p = .092) and there were three significant mediators: peer problems (B = −0.081, p = .028), self-esteem (B = −0.117, p = .010) and parental mental health (B = −0.027, p = .007).
Regularised Models in the Male and Female Subsamples
Tuning in the male sub-sample yielded an optimal
Indirect Effects for the Final Regularised Models Using Complete Case Analysis in the Male and Female Subsamples.
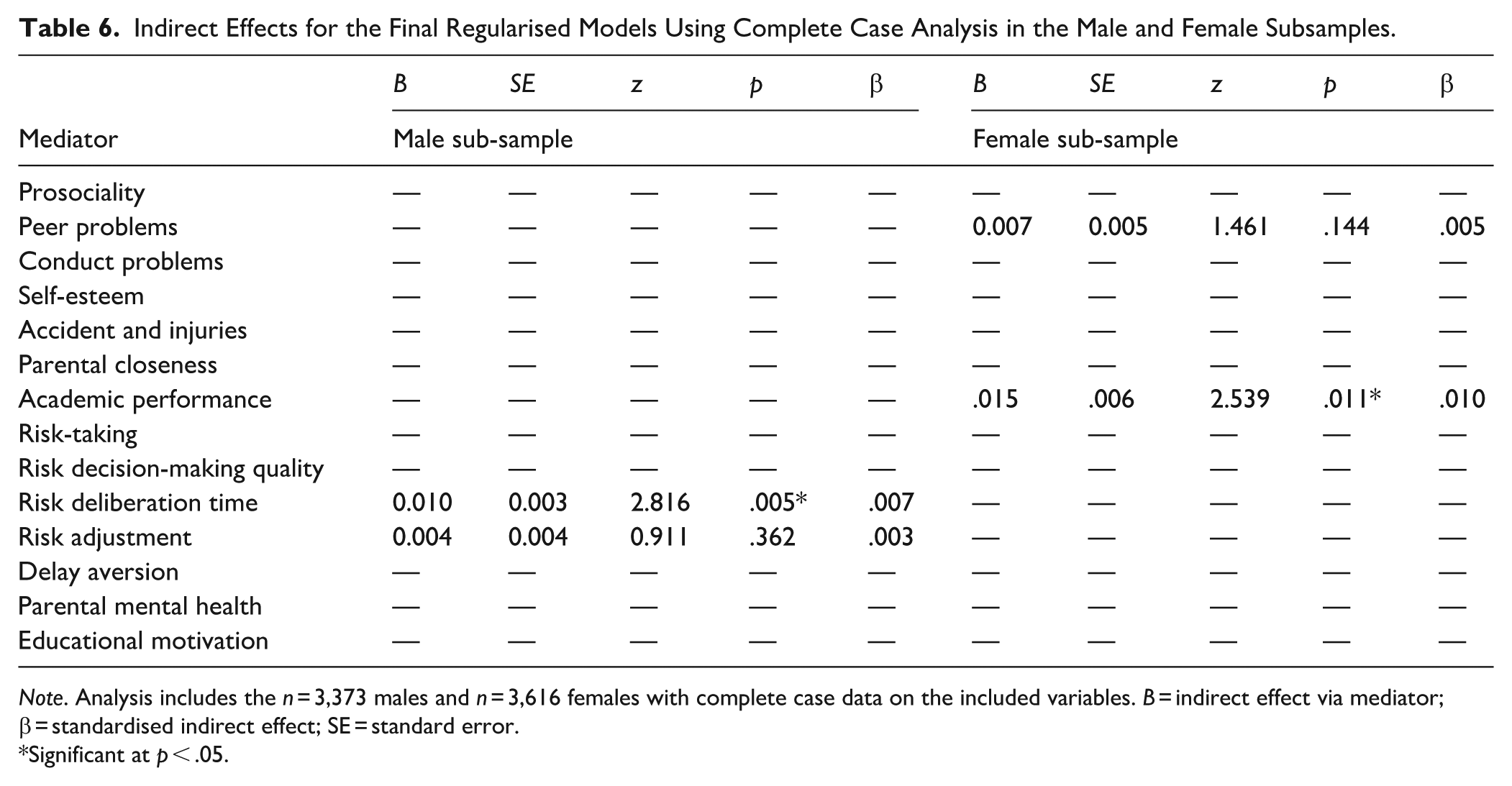
Note. Analysis includes the n = 3,373 males and n = 3,616 females with complete case data on the included variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
Significant at p < .05.
Indirect Effects for the Final Regularised Models Using FIML in the Male and Female Subsamples.
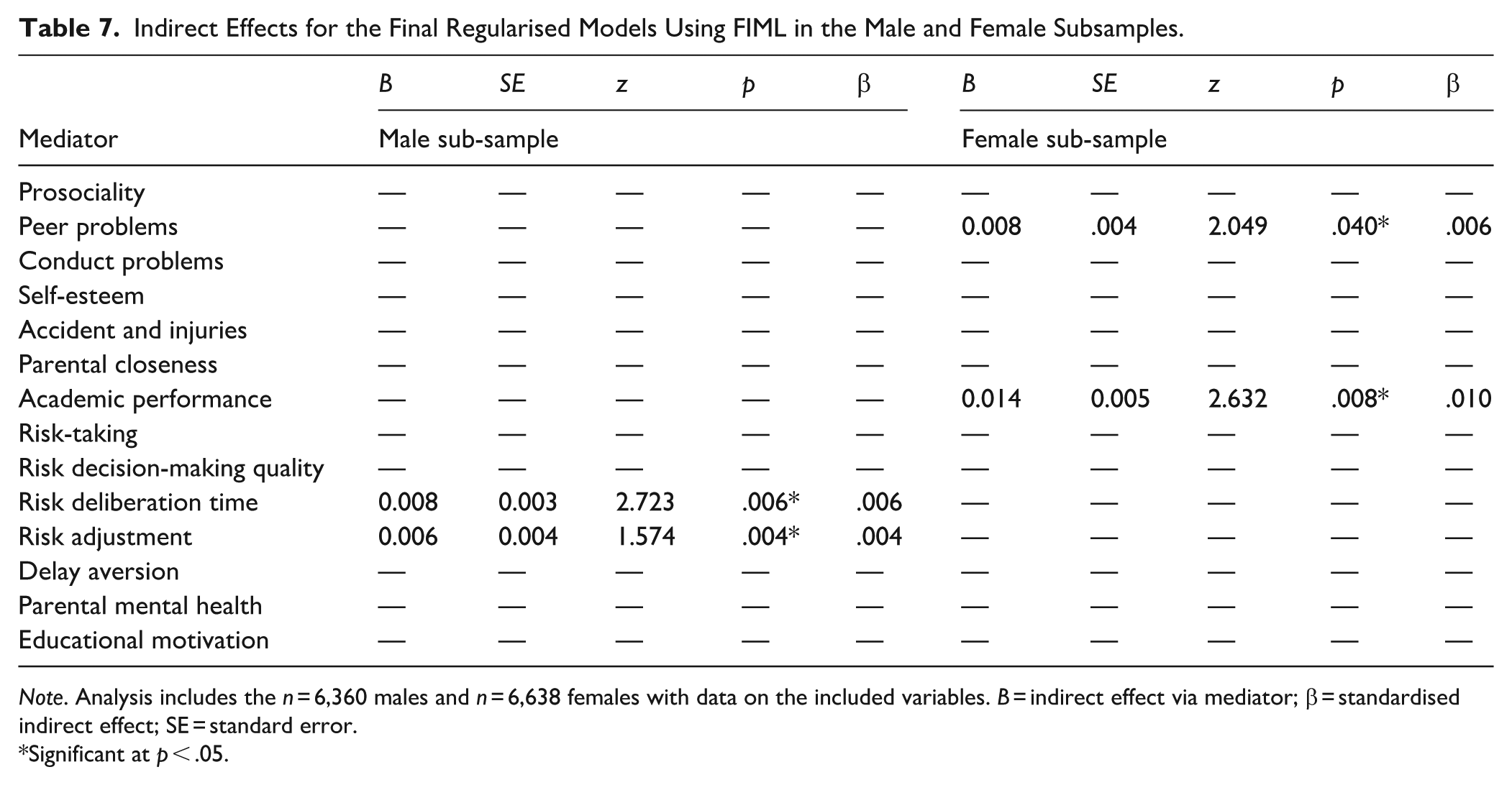
Note. Analysis includes the n = 6,360 males and n = 6,638 females with data on the included variables. B = indirect effect via mediator; β = standardised indirect effect; SE = standard error.
Significant at p < .05.
In the female sub-sample, the tuning phase yielded an optimal
Discussion
The present study provided an exploratory analysis of 14 candidate mediators in the association between ADHD and internalising symptoms across adolescence. Lasso within regularised SEM selected all candidate mediators in whole sample analyses; however, only two (self-esteem and parental mental health) were statistically significant in both the FIML and complete case analysis variants. This pattern of findings (with standardised indirect effects all < |.10|) is consistent with the idea that there may be many mediators of small effect contributing to the links between ADHD symptoms and later internalising problems in adolescence. Self-esteem and parental mental health: the only two robustly significant mediators, are indicated as priority targets for further study in interventional research. However, there were also some indications of sex differences in mechanisms which merit exploration in future studies. Specifically, in male adolescents, risk-taking tendencies on a gambling task tended to be selected by lasso and/or statistically significant, whereas in female adolescents, self-esteem, parental mental health and peer problems were selected or significant across the models.
The whole-sample findings of the current study imply that focusing on just a handful of mediators to address the links between ADHD symptoms and internalising problems will provide only a limited piece of the full picture. However, from a practical perspective there are difficulties in measuring and modelling large numbers of mediators simultaneously. Space is at a premium in data collections and researchers will typically need to keep the number of measures as few as possible to minimise participant burden, especially for young people with ADHD or ADHD symptoms (Murray et al., 2023). In providing a means to apply principled variable selection to large models, regularised SEM in pre-existing high quality data may help to optimise the use of limited space in studies by pointing to the most promising mediators to measure (Serang et al., 2017). By providing preliminary indications of which candidate mediators may be involved in the ADHD-internalising problems association, our findings can help focus the resources of more rigorous but resource intensive research designs on mediators that are likely to be the most promising. This includes longitudinal research with suitable controls for both time-invariant and time-varying confounding, causal mediation analyses, or experimental designs, which are typically expensive and logistically challenging to implement (Imai et al., 2010; Keogh et al., 2018; Streeter et al., 2017).
If the findings of the present study are confirmed by these designs, they would suggest that interventions to reduce the risk of developing co-occurring internalising problems among adolescents with ADHD may be most effective if they address multiple mechanisms. These may include cognitive-behavioural features associated with ADHD (e.g., risk-taking tendencies), socio-environmental stressors (e.g., school and peer problems) and their impacts (e.g., self-esteem). However, some mediators appeared to be particularly key based on the present analysis. In particular, self-esteem and parental mental health emerged as having the largest unique effects. These findings are consistent with developmental cascade models which propose that difficulties associated with ADHD can undermine young people’s self-esteem and lead to an increased risk of anxiety and depression (Roy et al., 2015). It is also consistent with previous research, including that in the current sample which found that ADHD symptoms relate to the development of lower self-esteem in adolescence (Russell et al., 2025). Taken together, these findings suggest benefits to addressing self-esteem as an intervention target among adolescents with ADHD symptoms. Whilst effective interventions for self-esteem exist, further work is needed to adapt/tailor and evaluate their effects specifically for adolescents with ADHD symptoms (Niveau et al., 2021), including their impact on internalising problems.
The mediating effects of parental mental health are also consistent with previous findings suggesting that adolescent ADHD symptoms are related to poorer parental mental health (Ko & Jeong, 2024) which has in turn been linked to young person mental health (Speyer et al., 2022). Such findings are consistent with the idea that whole family system interventions (Lagdon et al., 2021; Moltrecht et al., 2024) may be an optimal approach for families with members experiencing ADHD symptoms. Similarly, screening parents of adolescents with ADHD symptoms for mental health symptoms to facilitate intervention provision could help contribute to the prevention of adolescent mental health symptoms.
However, our findings also suggested that different mechanisms may be relatively more/less important in male versus female adolescents. Overall, the findings for females largely corresponded to the ‘dual failure’ model in which difficulties in the academic and social domains which impact self-concept and ultimately engender internalising problems (Roy et al., 2015). Yet for males, it was the risk-decision making variables that tended to be selected or significant across the models. While ADHD-related differences in risk-taking behaviour and strategies have been observed in previous research (Dekkers et al., 2020), their role in internalising problems remains to be clarified.
Other of our findings on sex differences are consistent with previous research. The fact that peer problems emerged as a significant mediator in females only aligns with the proposal that the peer problems associated with ADHD may be more impactful for females because they place greater importance on and tend to have more intimate peer networks characterised by higher levels of peer attachment than males (Kok et al., 2016). Consistent with this, one previous longitudinal study found a significant mediating effect of peer problems in the relation between ADHD symptoms and depression (7% mediation for peer dislike and 3% mediation for victimisation) in females but not males (Roy et al., 2015). The finding of a mediating effect of parental mental health in females only, is similarly consistent with previous analyses suggesting that female adolescent internalising symptom may be more closely related to parental mental health than male’s (Zhu et al., 2023). Finally, the finding of a mediating effect of self-esteem in females only is consistent with previous research suggesting that low self-esteem may be more prominent in girls compared to boys with ADHD (Kok et al., 2016). The consistency of these findings with previous theory and empirical evidence helps to bolster the idea that they are priority mediating mechanisms for further study in female adolescents with ADHD.
Limitations
It is important to consider the limitations of the present study. First, not all possible mediators that merit exploration were included due to data availability. Mediators such as emotion dysregulation, sluggish cognitive tempo, rumination, and executive functions are also likely to play a mediating role and would be valuable to include in future comprehensive mediation analyses (Broletti et al., 2024; Kandeğer et al., 2023). The idea that the inclusion of mediators was incomplete in the present study is also consistent with the significant direct effect in the whole-sample and male-specific analyses that remained after including the 14 indirect effects. There were also some measurement limitations in the mediators, for example, some were measured with a single item that could not capture the complexity of the concepts involved. Further, the measures of ADHD symptoms and internalising problems in the sample do not offer separate subscales for different symptom domains, therefore, it is not possible to distinguish mediators in the relations between inattention versus hyperactivity/impulsivity and anxiety versus depression symptoms. As regards the representativeness of the sample, although MCS was collected according to a complex survey design, design-adjusted models (incorporating weighting, stratification and clustering variables) are not readily implementable in the context of regularised SEM. As such, the analyses were not design-adjusted and may therefore be limited in their generalisability to the underlying UK population. Similarly due to the computation time involved in the tuning phase, we used complete case analysis for this; however, we did fit all initial and final models with FIML as well to check there were no major discrepancies indicative of strong bias in the complete case analyses. Finally, we did not have a sufficiently large subsample of adolescents diagnosed with ADHD to conduct meaningful subgroup analyses within this group only. Extending the present research to clinically diagnosed samples would be a valuable future direction to establish the extent to which the same mediators emerge as significant among those with ADHD.
Conclusions
Based on longitudinal mediation analyses with lasso-based variable selection there are likely to be a large number of mediators with small effects responsible for linking ADHD symptoms to internalising problems. Key mediators were self-esteem and parental mental health and these represent priority mediators for further study in interventional research. There was also evidence for different mechanisms in males versus females, with risk-taking variables of key importance in the former and academic and social difficulties of key relevance in the latter.
Supplemental Material
sj-docx-1-jad-10.1177_10870547261419589 – Supplemental material for Identifying Candidate Mediators Linking ADHD Symptoms and Internalising Problems in Adolescence: An Exploratory Longitudinal Mediation Analysis
Supplemental material, sj-docx-1-jad-10.1177_10870547261419589 for Identifying Candidate Mediators Linking ADHD Symptoms and Internalising Problems in Adolescence: An Exploratory Longitudinal Mediation Analysis by Aja Louise Murray, Katie Dryburgh and Edmund J. S. Sonuga-Barke in Journal of Attention Disorders
Footnotes
Ethical Considerations
The MCS data collections received full ethical approval from the National Health Service MultiCentre Research and Ethics Committee at each wave.
Consent to Participate
Informed consent was obtained in relation to all data used in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research described within this report was supported by a Medical Research Foundation (MRF) grant (Reference: MRF-001-0014-RG-MURR-C0932)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The Millennium Cohort Study is deposited with the UK Data Service: UK Data Service
Code Availability
Code is available on OSF: OSF | Identifying candidate mechanisms linking ADHD symptoms and internalising problems in adolescence: An exploratory mediation analysis
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.