
Abstract
Objective:
Depression is a major public health concern with a 19% lifetime prevalence in youth, often precipitating other concerns, including suicidal behavior, poor school performance, and worsened peer relationships. ADHD is also common among youth and frequently presents alongside major depressive disorder (MDD), with this comorbidity associated with increased impairment. More research is needed to elucidate the clinical characteristics of this comorbidity (MDD + ADHD), especially as it relates to youth with MDD and no ADHD (MDD − ADHD). The present study examined the clinical correlates of MDD + ADHD in youth and the presence of an ADHD diagnosis as a moderator of the relationship between depressive symptoms and suicidality, peer relationships, and school functioning, respectively.
Methods:
Our sample included 797 youth with MDD ages 8 to 20 years (Mage = 15.5 years) with and without ADHD.
Results:
Youth with MDD + ADHD experienced more severe depressive symptoms, higher levels of suicidality, impulsivity, and irritability, and worse academic performance compared to those with MDD − ADHD. ADHD diagnosis did not moderate the relationships between depression severity and suicidality, peer relationships, or school functioning, respectively, suggesting that having an ADHD diagnosis may not affect these outcomes in depressed youth in this way.
Conclusion:
Findings shed light on the impact of ADHD in depressed youth, which may allow for earlier and more tailored intervention efforts aimed at identifying and targeting depression, suicidality, peer relationships, and school functioning.
Introduction
Depression is a major public health issue in the United States due to its rising prevalence and associated impairment (Daly, 2022; Lépine & Briley, 2011). Major depressive disorder (MDD) has a lifetime prevalence of 19% in youth (Shorey et al., 2022), with the one-year major depressive episode (MDE) rate at 20% (Substance Abuse and Mental Health Services Administration, 2024). Of youth with MDD, 64% meet diagnostic criteria for at least one other psychiatric comorbidity (Avenevoli et al., 2015), likely contributing to poorer outcomes compared to youth with MDD alone (Henriksen et al., 2015). Extant research estimates ADHD occurs in 12% to 50% of youth with MDD (Angold et al., 1999). ADHD is also a public health concern, with an estimated 4% to 9.5% of children meeting diagnostic criteria (Mohammadi et al., 2021; Polanczyk et al., 2014; Thomas et al., 2015); 15% of these cases have clinically significant symptoms that persist into adulthood (Faraone et al., 2006). The prevalence of ADHD has also markedly increased over the past three decades (Safer, 2018; Visser et al., 2010). Thus, understanding the unique clinical correlates of the MDD + ADHD comorbidity represents a priority with implications for both assessment and intervention.
Independent of each other, MDD and ADHD are associated with deleterious mental and behavioral health outcomes. These include suicidal ideation, suicide attempts, and death by suicide (Cambridge et al., 2018; Garas & Balazs, 2020; Ljung et al., 2014; Schuler et al., 2021), suggesting a link between MDD and ADHD. Relatedly, both disorders are individually associated with irritability (Blader et al., 2016; Vidal-Ribas & Stringaris, 2021), which could serve as a pathway of apparent relationship. Furthermore, both conditions individually contribute to disruptions in social functioning (i.e., social communication deficits; attachment issues; and experiences of rejection, stigmatization, or victimization; Jaycox et al., 2009; Kupferberg et al., 2016; Ros & Graziano, 2017). These disruptions in social functioning may contribute to maladaptive alterations in developmental pathways, as well as being difficult to overcome, potentially exacerbating symptoms further (Gardner & Gerdes, 2015; Hoza, 2007). Additionally, research has revealed poor objective (i.e., grade point average) and subjective school performance and worsened reading and writing skills (Fröjd et al., 2008; Heiligenstein et al., 1996) in youth with MDD. Youth with ADHD also experience these negative academic sequalae, along with more absences and failing grades compared to those without ADHD (Frazier et al., 2007; Kent et al., 2011).
The consequences of each condition alone suggest the comorbidity may result in compounded effects. Indeed, while comorbid MDD + ADHD has been previously characterized (Biederman et al., 1998; Mayer et al., 2021), it has rarely been compared to youth with MDD alone. This gap may be due to ADHD onset typically predating depression in youth (Daviss, 2008). Extant research tends to focus most frequently on depression-related comparisons between youth with and without ADHD, irrespective of comorbid MDD status. Nevertheless, some findings have indicated that those with comorbid MDD + ADHD tend to experience increased psychosocial impairment, early onset of depression, sustained MDEs, sub-optimal school performance and high suicidality (Biederman et al., 2008; Cuffe et al., 2020; Daviss, 2008). However, especially relevant to the current study, only two studies to our knowledge compare MDD + ADHD and MDD alone. More specifically, Biederman et al. (2008) reported on adolescent females, finding that those with MDD + ADHD had more severe impairment, a higher rate of suicidality, and a greater likelihood of psychiatric hospitalization than their MDD alone counterparts. Rohde et al. (2001) found that depressed adolescents with ADHD were more likely to have a relapse in depression symptoms than those with MDD alone. To date, we are not aware of any other studies that have directly compared these two groups on relevant clinical characteristics in a large sample of youth. It also remains unclear how suicidality, peer relationships, school functioning, and resilience may be associated with MDD + ADHD comorbidity broadly, which is the goal of this study.
Previous studies have provided some evidence concerning the relationship between youth ADHD and suicidality. For example, positive associations between ADHD diagnosis and subsequent suicidal behavior in youth were observed in a recent meta-analysis (Garas & Balazs, 2020). An additional study revealed that children with ADHD are at increased risk of attempting suicide in adolescence (Chronis-Tuscano et al., 2010). Furthermore, Patros et al. (2013) found that inattention and hyperactivity symptoms moderated the association between depressive symptoms and suicidal thoughts and attempts, such that greater severity of core ADHD symptoms increased the risk for suicide among college students experiencing depression. While there is not a resoundingly large amount of literature in this area, we speculate that inattention and hyperactivity could conceivably increase the likelihood of acting on suicidal impulses. Another speculation is that perhaps the downstream effects of inattentiveness and hyperactivity contribute to depressive symptoms which in turn leads to suicidal ideation and behavior. Given the potential for these comorbid symptoms to confer increased risk for suicidality in depressed youth, it is critical to understand the extent to which the MDD + ADHD comorbidity may be related to experiencing suicidal thoughts and behaviors.
Additionally, there is an abundance of literature on the relationship between ADHD and peer relationships and school functioning (Frazier et al., 2007; Kent et al., 2011; Ros & Graziano, 2017), although no studies have examined the potential moderating effect of comorbid ADHD on the relationship between depression and these variables, despite their importance to depression-related outcomes. Furthermore, peer relationships and academic performance have been shown to mediate the association between depression symptoms and ADHD (Houghton et al., 2020; Humphreys et al., 2013; Powell et al., 2020). Hence, it is reasonable to anticipate that ADHD may be related to peer and school difficulties in depressed youth.
The foregoing literature review suggests that the MDD + ADHD comorbidity may be related to higher suicide rates, poorer peer connections, and worse performance in school than either disorder alone, presenting us with a public health problem requiring further understanding. By characterizing and understanding complex additive problems that youth with MDD + ADHD face, we can be better equipped to tailor treatment to youth needs alongside better trained clinicians, thereby saving families time otherwise dedicated to treating the disorders and reducing associated financial and emotional burden.
Current Study
Given the paucity of studies that directly compare youth with MDD + ADHD versus MDD − ADHD (conceivably both MDD alone and MDD plus other non-ADHD comorbidities), it is important to gain further knowledge about this presentation, which may help inform efforts to reduce suicide, improve peer relations, and foster better school performance. Using a sample of 8- to 20-year-old youth in treatment for depression and/or suicidality (Trivedi et al., 2023), we aimed to fill this gap by examining demographic and clinical correlates of youth with MDD with (i.e., MDD + ADHD) and without (i.e., MDD − ADHD) ADHD. Our aims were twofold: (1) to examine clinical correlates associated with the presence or absence of ADHD comorbidity, in addition to group differences on these clinical outcomes (i.e., suicidality, impulsivity, irritability, peer relationships, school functioning, and resilience), and (2) to determine whether the relationship between depression and relevant clinical correlates (i.e., suicidality, school functioning, and peer relationships) was moderated by the presence of comorbid ADHD. Consistent with past literature (Biederman et al., 2008), we predicted that youth with MDD + ADHD would demonstrate higher levels of suicidality compared to those with MDD − ADHD. The relationships between youth with MDD + ADHD and MDD − ADHD are less studied regarding school functioning and peer relationships, although we predicted that these outcome variables would be worse among youth with MDD + ADHD, given the associated impairments in each morbidity alone, and when compared with youth with ADHD alone (Cuffe et al., 2020; Frazier et al., 2007; Fröjd et al., 2008; Kupferberg et al., 2016; Ros & Graziano, 2017). Second, consistent with research on core ADHD symptoms (Patros et al., 2013), we predicted that ADHD diagnosis would significantly moderate the relationship between depression severity and suicidality, such that an ADHD diagnosis would significantly increase suicidality in youth with depression. Lastly, given the strong association with peer and school functioning (Frazier et al., 2007; Kent et al., 2011; Ros & Graziano, 2017), we expected that ADHD diagnosis would significantly moderate the relationship between depression and peer and school functioning, such that presence of an ADHD diagnosis would be associated with worsened peer and school functioning in youth with depression.
Method
Study Design
Data for the current study were drawn from the Texas Youth Depression and Suicide Research Network (TX-YDSRN; Trivedi et al., 2023), an initiative to improve mental health outcomes for youth and young adults across Texas. Launched in 2020, TX-YDSRN spans 12 academic medical centers in Texas and is funded by the Texas State Legislature as part of the Texas Child Mental Health Care Consortium (TCMHCC). Participants were: (1) 8 to 20 years old, (2) screened positive for depression and/or suicidality, or were in treatment for depression, and (3) possessed the ability to read, write, and speak English or Spanish sufficiently well to understand the study procedures and provide informed consent (18–20 years old) or assent (8–17 years old) with parent/legal guardian consent. Individuals were excluded from the study only if they: (1) had an acute medical or psychological condition that barred them from completing study requirements, (2) possessed acute psychosis making participation unsafe, or (3) had a parent/legal guardian who was cognitively unable to provide consent for their child under the age of 18 years (see Trivedi et al., 2023 for the sample baseline characteristics and more details concerning TX-YDSRN study procedures). Study procedures met local institutional review board requirements across all 12 sites involved in TX-YDSRN.
Participants
The present study only used data from the first 1,000 enrolled participants at their baseline visit. Of these 1,000 participants, 797 met criteria for primary MDD as determined by the Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) and were therefore included in our analyses.
Measures
Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID; Sheehan et al., 2010). The MINI-KID is a structured diagnostic interview assessing DSM-5 psychiatric disorders for children and adolescents. The MINI-KID has established good psychometric properties among children and adolescents, including evidence of convergent and discriminant validity and test-retest reliability and validity comparable to other diagnostic interviews (Duncan et al., 2018; Högberg et al., 2019). Interviews were conducted by trained coordinators, who consulted a licensed psychologist supervisor. Trained coordinators first interviewed the youth participant alone (with some exceptions due to young age), then conducted a separate interview with the parent/legal guardian. Trained coordinators then determined diagnoses following the interviews using the results from multiple informants in consultation with licensed psychologist supervisors trained in ADHD- and MDD-related differential diagnosis. The present study used the MINI-KID to determine current MDD and ADHD diagnoses. MDD + ADHD coded for comorbid current MDD and current ADHD. It was possible, but not necessary, that participants in the MDD + ADHD group had other comorbidities. MDD − ADHD coded for MDD without ADHD, meaning this group included participants with MDD alone and with MDD plus other, non-ADHD comorbidities.
Patient Health Questionnaire for Adolescents (PHQ-A; Johnson et al., 2002). The PHQ-A is a self-report questionnaire, completed by youth, comprised of nine items measuring depression severity over the past 2 weeks. The items are rated from 0 (not at all) to 3 (nearly every day), with higher scores indicating elevated depression severity. The PHQ-A has demonstrated excellent psychometric properties among adolescents, including optimal sensitivity and specificity of detection (Nandy et al., 2023; Richardson et al., 2010).
Concise Health Risk Tracking-Self-Report (CHRT-SR; Trivedi et al., 2011). The CHRT-SR is comprised of 16 items measuring the severity of suicidal ideation and risk over the past 7 days. Items are rated from 0 (strongly disagree) to 4 (strongly agree), with higher scores indicating elevated suicidal ideation and/or risk. The CHRT-SR is comprised of four subscales including measures of propensity, thoughts, irritability, and impulsivity. The CHRT-SR has demonstrated excellent model fit, internal consistency, and reliability among youth (Mayes et al., 2018).
Concise Associated Risk Tracking Scale (CAST; Trivedi et al., 2011). The CAST is a self-report questionnaire measuring five domains including anxiety, mania, irritability, insomnia, and panic. Items are rated on a 5-point Likert scale including “strongly disagree,” “disagree,” “neither agree nor disagree,” “agree,” and “strongly agree.” The CAST has been shown to be a valid measure of the mentioned domains and depressive associated symptoms (Minhajuddin et al., 2020). The present study only utilized the irritability domain (five items) of the CAST, where higher scores indicate increased irritability.
Patient-Reported Outcomes Measurement Information System 25-item Pediatric (PROMIS-25; Dewalt et al., 2013). The PROMIS-25 is a self-report questionnaire featuring six quality-of-life domains/subscales regarding the past week. These domains include physical mobility, anxiety, depression, fatigue, peer relationships, and pain interference. The PROMIS-25 has demonstrated strong internal consistency and retest-reliability (Bevans et al., 2017). The present study utilized only the peer relationships subscale in youth (age 8 – 17), which is rated from 0 (never) to 4 (almost always), with lower scores indicating worse peer relationships. Given the adult version of the PROMIS does not include a peer relationships subscale, subjects aged 18 to 20 years were not included in analyses involving the PROMIS. Hence, only 616 of the 797 meeting criteria to be included analyses were <18 years old and therefore expected to have data on the PROMIS pediatric peer relationship scale.
Social Adjustment Scale-School Module Self-Report (SAS-SR; Weissman, 1999; Weissman et al., 1978). The SAS-SR is comprised of 54 items, although the present study used only the 6-item subscale measuring school functioning/performance over the last 14 days. Higher scores indicate worse functioning in academic settings. The SAS-SR has been found to have strong internal consistency and test-retest reliability (Bosc et al., 1997). Additionally, only participants who were currently attending school at least half of the time completed the SAS-SR. Of the 797 included in analyses, 608 were currently attending school at least half the time and expected have completed the SAS-SR.
The 10-item Connor-Davidson Resilience Scale (CD-RISC-10; Connor & Davidson, 2003). The CD-RISC-10 is comprised of 10 items measuring an individual’s ability to function despite adversity encountered throughout life. Items are rated from 0 (not true at all) to 4 (true nearly all the time) and higher scores correspond with greater resilience. The CD-RISC-10 has demonstrated good internal consistency and strong construct validity (Campbell-Sills & Stein, 2007).
Data Analyses
Data were summarized for MDD + ADHD and MDD − ADHD groups, both operationalized using the MINI-KID. Categorical outcomes are presented as frequencies and percentages. Given that the proportion of missing data was not extensive (<7%), we did not engage statistical imputation methods and report findings on a completer sample analysis (see Table 1 for specific details regarding missingness for study variables). Continuous outcomes are presented as mean ± standard deviation (SD). T-tests or Chi-square tests were used to compare the two groups on relevant variables. Pairwise standardized differences are reported as Cohen’s d. For multinomial chi-squares (i.e., categorical variables), Cramer’s v was usedto measure effect size. The Phi coefficient was used for binomial variables. Lastly, to determine whether the presence of comorbid MDD + ADHD moderated the effect of depression severity (PHQ-A) on suicidality (CHRT-SR), peer relationships (PROMIS), and school functioning (SAS-SR), multivariate linear regression analyses were conducted. All models controlled for age, race, sex, ethnicity, and presence of comorbid psychiatric diagnosis besides ADHD or MDD. For the first model, the PHQ-8 (i.e., PHQ-A without the one item assessing suicidality) was used for depression severity, as opposed to the entire PHQ-A, to ensure suicidal ideation was not accounted for in both the independent and dependent variables. Dichotomous presence/absence of comorbid ADHD was the proposed moderator. For all moderation models, we mean-centered the data and computed the interaction variable using the centered variables to adjust for potential issues regarding multicollinearity. All analyses were completed using SAS 9.4. Significance levels were set at p < .05.
Demographics and baseline measures of depressed youth with and without ADHD.
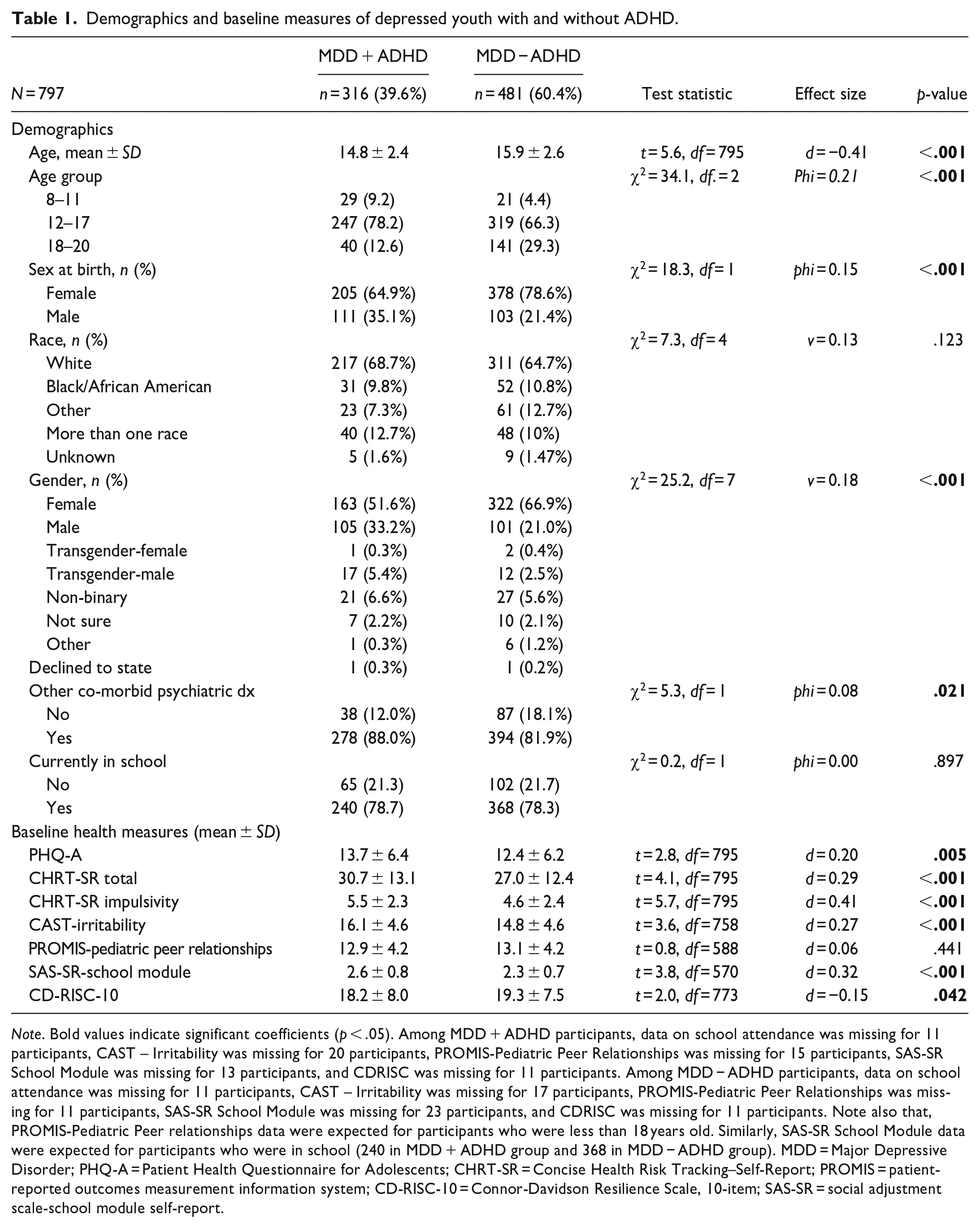
Note. Bold values indicate significant coefficients (p < .05). Among MDD + ADHD participants, data on school attendance was missing for 11 participants, CAST – Irritability was missing for 20 participants, PROMIS-Pediatric Peer Relationships was missing for 15 participants, SAS-SR School Module was missing for 13 participants, and CDRISC was missing for 11 participants. Among MDD − ADHD participants, data on school attendance was missing for 11 participants, CAST – Irritability was missing for 17 participants, PROMIS-Pediatric Peer Relationships was missing for 11 participants, SAS-SR School Module was missing for 23 participants, and CDRISC was missing for 11 participants. Note also that, PROMIS-Pediatric Peer relationships data were expected for participants who were less than 18 years old. Similarly, SAS-SR School Module data were expected for participants who were in school (240 in MDD + ADHD group and 368 in MDD − ADHD group). MDD = Major Depressive Disorder; PHQ-A = Patient Health Questionnaire for Adolescents; CHRT-SR = Concise Health Risk Tracking–Self-Report; PROMIS = patient-reported outcomes measurement information system; CD-RISC-10 = Connor-Davidson Resilience Scale, 10-item; SAS-SR = social adjustment scale-school module self-report.
Results
Of all participants, 583 (73.2%) identified their sex-at-birth as female, 528 (66.3%) were White, 342 (43%) were Hispanic, and the sample had a mean age of 15.5 years (range 8–20 years). Our sample included 50 children aged 8 to 11 years, 566 adolescents aged 12 to 17 years, and 181 emerging adults aged 18 to 20 years. Of 797 youth and young adults that met diagnostic criteria for MDD, nearly 40% (n = 316) also met criteria for ADHD. Details on demographics and functional outcomes are included in Table 1. Youth with MDD + ADHD tended to be younger than those with MDD − ADHD, consistent with a small to medium effect size (d = -0.41, p < .001). A small effect was found for sex-at-birth (phi = .15, p < .001), with female participants being less likely to endorse a comorbid psychiatric disorder. There was no statistically significant difference based on race. A small effect was found for gender (v = .18, p < .001) such that youth who identified as boy more often had MDD + ADHD. Over 80% of both MDD + ADHD (88%) and MDD − ADHD (82%) groups had other comorbid diagnoses, and while statistically significant, the effect size was negligible (phi = .08, p = .021) between groups.
Youth with MDD + ADHD reported greater depression (d = 0.20, p = .005) and suicidality (d = 0.29, p < .001), and worse school functioning (d = 0.32, p < 0.001) than youth with MDD − ADHD, all consistent with small effects. A statistically significant difference was observed on the CHRT-SR domain of impulsivity (d = 0.41, p < .001) with a medium effect size and the CAST domain of irritability (d = 0.27, p < .001) consistent with a small effect size, such that youth with MDD + ADHD experience higher impulsivity and irritability. A statistically significant difference was found between groups on resilience (d = -0.15, p = .042), with less than small effect sizes, such that youth with MDD + ADHD scored slightly lower (i.e., worse). No group differences were found for peer relationships.
The association between depression severity and suicidality was not moderated by the presence of ADHD, as demonstrated by a non-significant interaction effect (p = .201), as seen in Table 2. The same was indicated by non-significant interaction terms for peer relationships (p = .533) and school functioning (p = .554). Examining the p-value for interaction effect in all three models, there is no evidence that the ADHD diagnosis moderated the relationship of depression severity (PHQ-A) with suicidality (CHRT-SR), peer relationships (PROMIS), and school functioning (SAS-SR).
Linear Regression Examining the Association of ADHD With Suicidality, School Functioning and Social Relationships.
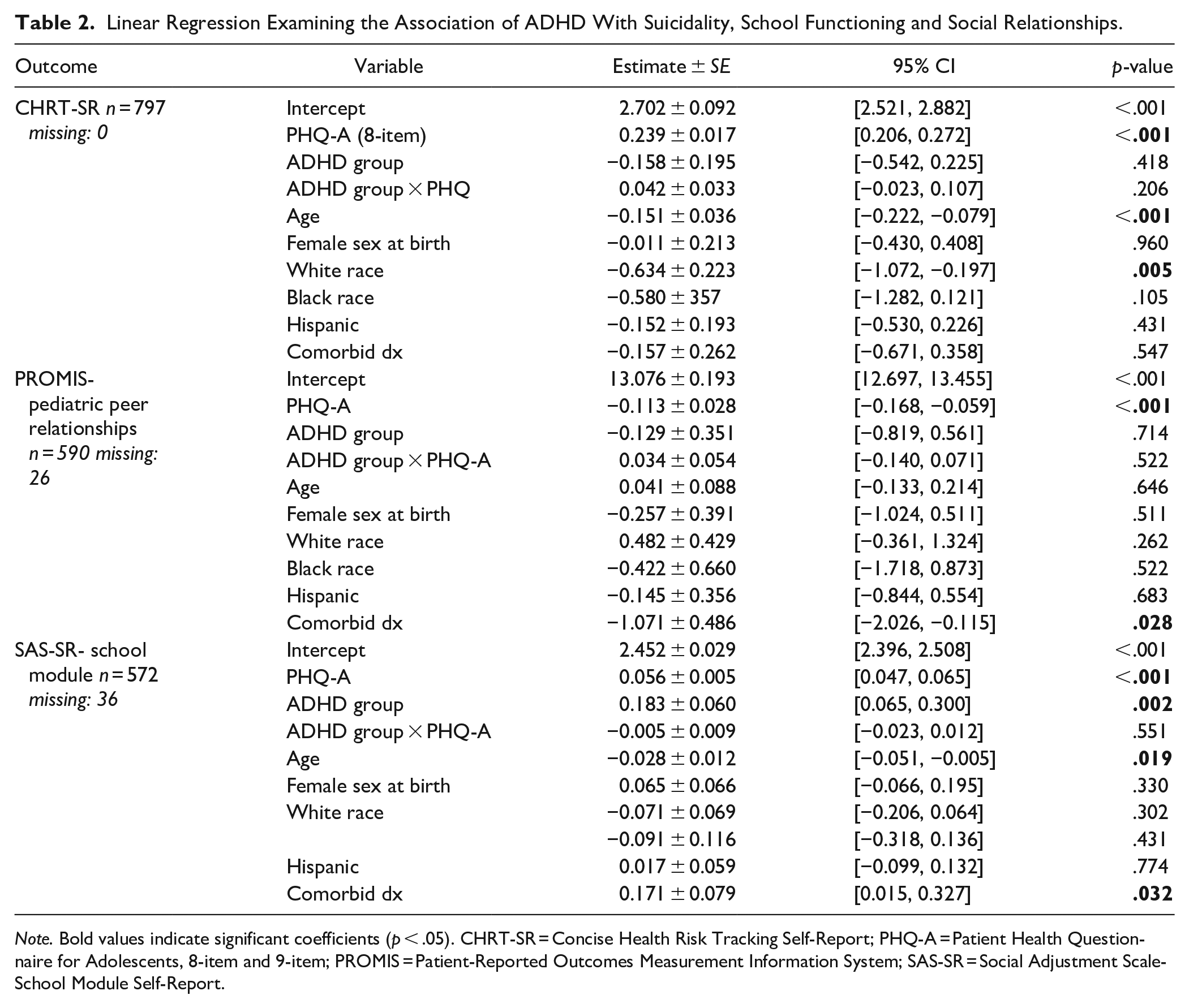
Note. Bold values indicate significant coefficients (p < .05). CHRT-SR = Concise Health Risk Tracking Self-Report; PHQ-A = Patient Health Questionnaire for Adolescents, 8-item and 9-item; PROMIS = Patient-Reported Outcomes Measurement Information System; SAS-SR = Social Adjustment Scale-School Module Self-Report.
Discussion
The present study had two central aims: (1) to evaluate group differences between youth with MDD with versus without comorbid ADHD in demographic and clinical factors and (2) to examine whether an ADHD diagnosis would affect the relationship between depression severity, and relevant clinical variables (i.e., suicidality, peer relationships, and school functioning). Overall, 39.6% of youth with MDD had comorbid ADHD in this sample, a rate on the higher end of observed ranges (Mohammadi et al., 2021; Polanczyk et al., 2014; Thomas et al., 2015). Youth with comorbid MDD + ADHD were more likely to be male and younger than youth with MDD − ADHD. This is consistent with data that ADHD often presents more prominently in younger children (De Rossi et al., 2023) due to a gradual decline of symptom severity across the lifespan (Franke et al., 2018). Additionally, boys typically behaviorally express ADHD more than girls (Loyer-Carbonneau et al., 2021) and are more likely to be referred for ADHD testing (De Rossi et al., 2022). Youth with MDD + ADHD reported more severe depression, greater suicidality, impulsivity, and irritability, and worse school functioning than youth with MDD − ADHD. Youth with MDD + ADHD also reported less resilience, though this effect was weak. No differences were found for peer relationships or suicidal propensity between youth with MDD + ADHD and MDD − ADHD. Finally, we found no evidence that an ADHD diagnosis significantly moderated (i.e., affected) the relationship between depression severity and suicidality, peer relationships, or school functioning.
Our results showed youth with MDD + ADHD experienced elevated depressive symptoms compared to the MDD − ADHD group. This could be due to ongoing impairment from ADHD functioning as a risk-factor for elevated depression (Gnanavel et al., 2019). Indeed, two studies found that impairment in social relationships and school functioning mediated the relationship between ADHD symptomology and later depressive symptoms (Herman et al., 2007; Ostrander et al., 2006). Humphreys et al. (2019) found that ADHD symptoms are associated with an increased number of stressful life events experienced by youth. Thus, it is plausible that in youth with depression, comorbid ADHD could lead to more stressful life events above and beyond those experienced by depressed youth without ADHD. Taken together, we speculate that ADHD symptoms contribute to increased challenges in youth’s lives, which in turn leads to elevated depressive symptoms. Another explanation for the greater depression in MDD + ADHD youth could be the complexity of overlapping psychiatric disorders and limited treatment access and options for this more complex presentation (Daviss, 2008). Finally, the link between depression and ADHD may be explained by the construct of irritability (Eyre et al., 2017), typically associated with externalizing psychopathology. Indeed, in this sample, youth with MDD + ADHD endorsed elevated irritability, thus it is plausible that increased irritability in depressed cohorts could be a marker for ADHD.
Consistent with our hypotheses and aligned with extant findings (Biederman et al., 2008; Garas & Balazs, 2020), youth with MDD + ADHD reported greater suicidality. Within the domains of suicidality and ADHD, youth with MDD + ADHD, unsurprisingly, also reported higher impulsivity. This may be linked to the inherent short-term risk for suicide that impulsivity presents. Indeed, ADHD-combined type (ADHD-C) has been linked to increased frequency of suicidal ideation and overall suicide risk compared to youth with ADHD-inattentive type (Austgulen et al., 2023; Chronis-Tuscano et al., 2010). However, it is unclear whether impulsivity, a core ADHD symptom, is the primary catalyst of increased suicidality in youth with ADHD. Risk factors for suicidal behavior also include school failure (Castellví et al., 2020), a greater number of negative life events (Serafini et al., 2015), and poor parental relationships (Fotti et al., 2006), all of which are linked to youth with ADHD (Deault, 2010; Humphreys et al., 2019; Kent et al., 2011). Conversely, presence of comorbid ADHD may broadly reflect increased risk secondary to compounded psychiatric burden. That is, comorbid psychiatric disorders broadly may increase risk for suicide attempts (Goldston et al., 2009).
Youth with MDD + ADHD also reported worse school functioning, consistent with past literature revealing that youths with that comorbidity are more likely to perform worse in school than those with only a mood disorder (Cuffe et al., 2020). While depression frequently presents with symptoms that overlap with ADHD (e.g., concentration problems and restlessness), comorbid ADHD may further impinge on performance. Youth with MDD + ADHD also reported relatively lower resilience than their MDD − ADHD counterparts, but with small effect sizes. Protective factors (resilience) and risk factors (diagnoses) are often inversely related (Dvorsky & Langberg, 2016), so it follows that the group with comorbid diagnoses would demonstrate lower resilience. Group differences on depression severity, suicidality, and school functioning also had small effects, which should be considered when interpreting findings. Finally, it is worth noting that approximately 20% of our sample endorsed not currently being in school, and thus did not complete the SAS-SR. Since we did not collect data concerning reasons for school non-attendance, the extent to which participants endorsed adaptive (e.g., graduated high school and gainfully employed, currently on summer break) versus maladaptive (e.g., dropped out of high school or college due to ADHD-related impairments) reasons for school non-attendance remains unknown. This sampling bias is a limitation, especially given research suggesting that individuals with ADHD are more likely to drop out of school (Fried et al., 2013; Sibley et al., 2021).
Contrary to our hypotheses, youth with MDD + ADHD and MDD − ADHD did not experience differences in peer relationships. This is surprising given literature linking ADHD to peer related impairment (Bagwell et al., 2001; Hoza, 2007; Hoza et al., 2005; Ros & Graziano, 2017). This disconnect may be due to discrepancy between self-report and actual competence among youth with ADHD, also known as positive illusory bias (Reinke et al., 2023; Owens et al., 2007). Indeed, Normand et al. (2021) found that peers of youth without ADHD reported more conflict and less positive relationships than their ADHD counterparts. However, results should be interpreted in light of known limitations of self-report of internal states among youth (De Los Reyes & Epkins, 2023). Additionally, despite our findings, it is plausible that youth with MDD + ADHD may be further ostracized if they have more externalizing symptoms than youth with MDD − ADHD, although it could be that youth with MDD − ADHD already deal with peer relationship issues where an ADHD diagnosis does not incur further dysfunction.
Comorbid ADHD diagnosis did not significantly moderate the relationship between depression severity and suicidality. This finding contradicts Patros et al. (2013) who found a moderating effect of ADHD on this relationship. Three key differences in Patros et al. (2013) and our study include (1) Patros et al. (2013) sample consisted of only college students, while ours was primarily adolescents, (2) our sample included youth with MDD whereas Patros et al. simply measured depression among those with ADHD, and (3) while we used an ADHD diagnosis, they investigated continuous ADHD symptom severity as a moderator. Thus, one explanation for our contradictory results could be that when ADHD symptomology manifests in adulthood (such as in Patros et al., 2013), there are more serious consequences across all domains (e.g., mental health, physical health, socioeconomic outcomes, etc.; Agnew-Blais et al., 2018). This limits the generalizability of Patros et al. to youth samples. Additionally, recent findings have argued in favor of a dimensional understanding of ADHD (symptom severity; Drechsler et al., 2020), as opposed to a categorical diagnosis.
We did not find a moderating effect of ADHD on the relationships between depression and suicidality, peer relationships, nor school functioning, respectively. Null findings with regard to depression and peer functioning are especially unsurprising given the lack of group differences between MDD + ADHD and MDD − ADHD groups on peer relationships. With these and the group difference findings in mind, it seems that ADHD comorbidity in youth with MDD does not impact social domains. It may be the case that MDD already presents such a significant barrier in social relationships that ADHD has no further effect. Although, as stated previously, this finding may be due to positive illusory bias seen in youth with ADHD (Becker, 2020; Colomer et al., 2020). Additionally, lack of significant findings between depression and both peer relationships and school functioning may be due to the previously mentioned debate on a dimensional (symptom severity) versus categorical (diagnosis) approach to ADHD. It is possible that by dichotomizing ADHD we lose variability in symptom presentation and severity while introducing measurement error (Fisher et al., 2020). Further research may extend on the relationship of dimensional versus categorical ADHD assessments.
Limitations
The present study has several limitations. First, our sample only included youth with depression warranting treatment and may not generalize to youth with low to moderate depression. Relatedly, conceptual challenges regarding shared overlap between ADHD and depression in terms of concentration difficulties and attentional control (Keller et al., 2019) may have inadvertently contributed to the potential for false positives in either of the respective diagnoses. While multi-informant (i.e., parent and youth separately) diagnostic interviewing was used to strategically parse apart these related clinical phenomena, the extent to which inattention symptoms were able to be sufficiently distinguished from cognitive sequelae of depression remains an empirical question worthy of future research. Second, data is only reflective of a single timepoint, so the directionality of relationships remains unclear. While we were unable to examine temporality in this cross-sectional study, further research that examines the longitudinal trajectory of ADHD and depression symptoms, including the potential temporal precedence of ADHD and depression (or vice-versa), is warranted. Third, outside of the MINI-KID, only self-report measures were used to collect data, possibly contributing to mono-method bias. Fourth, it is worth noting that the lack of significant group differences found in the present study could represent a Type 2 error in the sense that our categorical operationalization of ADHD– compared to dimensional conceptualizations– may have resulted in sub-optimal representation of the dynamic nature of the construct (Fisher et al., 2020). Fifth, due to the primary focus of the TX-YDSRN research consortium on youth depression, data were not collected regarding youth psychiatric treatments for ADHD. Failure to control for ADHD mediation status presents as a limitation. That being said, the fact that youth participants met criteria for clinically significant ADHD on the MINI regardless of medication status lends credence to the ADHD-related clinical acuity of our sample. Finally, our sample was largely female and White, which limits generalizability to varied populations. However, the sample was largely Hispanic, reflecting the ethnic diversity of Texas.
With these limitations in mind, the current study contributes to our understanding of MDD + ADHD in youth. Our findings shed light on the prevalence and impact of MDD + ADHD on suicidality, peer functioning, and school functioning. Our results also offer several implications for practicing clinicians. First, clinicians should be aware of the increased risk of depression, suicidality, and poor school functioning in youth with MDD and comorbid ADHD. Evidence-based assessments should be readily deployed to monitor symptom presence and treatment response. Second, determining personalized treatment pathways for ADHD in the presence of depression would enhance patient outcomes. For example, further research is necessary to understand evidence-based treatment algorithms for treating each condition with psychotherapy and pharmacotherapy, and how this differs depending on factors like primary diagnostic status, other comorbidities, and socio-demographic factors. Relatedly, additional research should be conducted to determine how to best treat or sequence treatment for individuals with this complex comorbidity. Finally, knowledge about this comorbidity can inform development and implementation strategies that may enhance functional improvement such as social engagement or academic supports. Overall, this study offers guidance to address the growing public health concern of youth depression and ADHD. In addition to investigating treatment pathways, it will be important for future research to continue examining this comorbidity pattern within a longitudinal design to better understand how these relationships may change over time, as well as putative mediators and moderators.
Footnotes
Acknowledgements
The authors would like to thank the patients, clinics, staff, and colleagues who made this project possible. We acknowledge the TX-YDSRN teams from the following sites: University of Texas Southwestern Medical Center: Graham J. Emslie, Betsy D. Kennard, and Laura Stone; Baylor Medical Center: Jasmine Arriaga, Erica Buckland, Kate Foshee, and Nisha Oruganti; Texas A&M University System Health Science Center: Tri Le, Olga Raevskaya, and Jessica Christian; Texas Tech University Health Science Center Lubbock: Jennifer Hudnall, Robyn Richmond, Anuththara Lokubandara, and Victoria Johnson; Texas Tech University Health Science Center El Paso: Zuber Mulla, Alejandro Fornelli, and Caitlin Chanoi; University of Texas at Austin Dell Medical School: Lexi Hughes, Tyler Wilson, Sophia Syed, Olivia Askew, Santiago Jimenez, Fernanda Pena Lozano, Michelle Lagrone, and Eric Gonzales; University of Texas Health San Antonio: Annelise Flores, Sofia Ballesteros, Abigail Cuellar, and Presley Pargin; University of Texas Rio Grande Valley: Cynthia Garza, Diana Chapa, Dernay Coley, and Alessandra Rizzo-Esposito; University of Texas Health Science Center Houston: Cesar A. Soutullo, Giovana B. Zunta-Soares, Sofia Galarza-Estrella, and Sydney Solberg; University of Texas Health Science Center Tyler: Jamon Blood, Colten Jones, Kiley Schneider, Pamela Thurman, and Preston Washburn; University of Texas Medical Branch: Michaella Petrosky, Layla Kratovic, and Akila Gopalkrishnan; University of North Texas Health Science Center: David Farmer, Summer Ladd, Nicki Ahmuada, and Madelyn Guerra.
Data Availability Statement
Data from the Texas Youth Depression and Suicide Research Network (TX-YDSRN) are not publicly available.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mr. Upshaw, Dr. Spencer, Dr. Pinciotti, Mr. Zhyrov, Dr. Minhajuddin, Mr. Castillo, Dr. Abacan, Dr. Slater, Dr. Walker, Dr. Martin, Dr. Shahidullah, Dr. Harper, Ms. Guerra, and Dr. L. Goodman have no declarations of financial interest. Dr. Blader has served as a consultant and speaker for Supernus Pharmaceuticals. Dr. Soares has served as an advisor or consultant for Johnson & Johnson and Alkermes. He participated in research funded by Relmada, Sunovion, Mind Med, and Compass Pathways. Dr. W. Goodman receives royalties from Nview LLC and OCDscales, LLC. Dr. Wakefield serves as an Executive Committee Member of the Texas Child Mental Health Care Consortium. Dr. Trivedi has provided consulting services to Acadia Pharmaceuticals, Alkermes Inc., Alto Neuroscience Inc, Axsome Therapeutics, BasePoint Health Management LLC, Biogen MA Inc, Cerebral Inc., Circular Genomics Inc., Compass Pathfinder Limited, Daiichi Sankyo Inc., GH Research, GreenLight VitalSign6 Inc, Heading Health, Janssen Pharmaceutical, Legion Health, Merck Sharp & Dohme Corp., Mind Medicine Inc., Myriad Neuroscience, Naki Health Ltd., Neurocrine Biosciences Inc., Noema Pharma AG, Orexo US Inc., Otsuka America Pharmaceutical Inc., Otsuka Europe LTD, Otsuka Pharmaceutical Development & Commercialization Inc., Praxis Precision Medicines Inc, PureTech LYT Inc, Relmada Therapeutics Inc., SAGE Therapeutics, Signant Health, Sparian Biosciences, Titan Pharmaceuticals, Takeda Pharmaceuticals Inc, WebMD. He has received grant/research funding from NIMH, NIDA, NCATS, American Foundation for Suicide Prevention, Patient-Centered Outcomes Research Institute (PCORI), Blue Cross Blue Shield of Texas, SAMHSA, and the DoD. Additionally, he has received editorial compensation from Elsevier and Oxford University Press. Dr. Storch reports receiving research funding to his institution from the Ream Foundation, International OCD Foundation, and NIH. He is a consultant for Brainsway and Biohaven Pharmaceuticals. He owns stock less than $5,000 in NView. He receives book royalties from Elsevier, Wiley, Oxford, American Psychological Association, Guildford, Springer, Routledge, and Jessica Kingsley.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was funded by the Texas Youth Depression and Suicide Research Network (TX-YDSRN), a research initiative of the Texas Child Mental Health Care Consortium (TCMHCC). The TCMHCC was created by the 86th Texas Legislature and, in part, funds multi-institutional research to improve mental health care for children and adolescents in Texas. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding organizations. The TX-YDSRN is implemented under the leadership of the central UT Southwestern HUB (Madhukar H. Trivedi, M.D., Principal Investigator; Sarah M. Wakefield, M.D., Medical Director (Texas Tech University Health Science Center Lubbock); Abu Minhajuddin, PhD, Data/Statistics Lead; and Lynnel C. Goodman, PhD, Operations/Scientific Lead). This work was also supported in part by funding of The Baylor College of Medicine Intellectual and Developmental Disabilities Research Center (P50HD103555) from the Eunice Kennedy Shriver NICHD. The contents of this publication do not necessarily reflect the views or policies of the NIH. The mention of trade names, commercial products, or organizations does not imply endorsement by the US Government.
Ethical Approval
The “Hub” of the study was UT Southwestern in Dallas, Texas, with 12 “Nodes” across the state of Texas where data would be collected. All study procedures were first approved by the Institutional Review Board (IRB) at UT Southwestern, the IRB of record. Subsequently, study procedures were approved at all 12 Nodes by respective IRB’s. Additionally, stakeholders in the community constituted each sub-site, which were clinics in the community of each Node. If necessary, approval was received at each sub-site’s IRB for recruitment.
Informed Consent
Electronic informed consent (18–20 years old) or assent and legal guardian consent (8–17 years old) was obtained for each participant in the registry. Informed consent/assent was obtained via an electronic data capture system (REDCap).