
Abstract
Background:
Many children with attention-deficit/hyperactivity disorder (ADHD) demonstrate impairment in social skills. However, ADHD rarely occurs in isolation, with approximately one-third of children with ADHD having one additional disorder, and another third having two or three comorbidities. Few studies have considered the global and specific patterns of social skill performance based on comorbidity status.
Method:
Using a large dataset containing 1400 carefully phenotyped children with ADHD (ages 7–12; 28% girls) in the United States and Canada, we characterized social skill deficit profiles associated with the presence of internalizing comorbidity (depression and/or anxiety), externalizing comorbidity (oppositional defiant or conduct disorder), and both internalizing + externalizing comorbidities. All children had parent and teacher ratings of social skills on a consistent measure, and we took a nuanced approach that considered both global social skills and specific subdomains of skills.
Results:
Parent ratings indicated main and interaction effects of each comorbidity on lower social skill performance in a varied pattern. Both comorbidities were associated with poorer global social skills, responsibility, and self-control. In addition, internalizing was associated with poorer assertion, while externalizing was associated with poorer communication, cooperation, and empathy. Interaction effects suggested that the impact of externalizing overshadowed internalizing for poor responsibility and self-control; however, internalizing comorbidity attenuated the negative association between externalizing comorbidity and empathy. On teacher ratings, only externalizing comorbidity was associated with poorer global social skills, communication, cooperation, assertion, responsibility, empathy, and self-control. In addition, girls and younger children tended to have poorer global social skills (using a gender-normed standard score), while girls and older children showed better specific social skills (using a raw, not gender-normed score).
Conclusion:
Children with ADHD and these comorbidities had poorer social skills relative to children with ADHD only, as perceived by parents and teachers. There also may be different social skill profiles depending on the comorbid condition and informant. These findings may inform more personalized social skill interventions for children with ADHD.
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by developmentally inappropriate levels of inattention and/or hyperactivity/impulsivity, that affects approximately 5% of school-age children worldwide (Polanczyk et al., 2014). As a functional outcome of their disorder, many children with ADHD demonstrate poor social skills (the necessary behaviors to be successful in social situations; Gresham et al., 2001). Crucially, among children with ADHD, poor social skills are predicted by, and in turn predict, aggression over time in cascading cycles (Murray-Close et al., 2010). Given the clinical relevance of social skills, this study aimed to characterize the social skill profiles of children with ADHD in a nuanced fashion. Leveraging a large, aggregated sample of 1,400 children with ADHD across the United States and Canada, we examined how global and specific social skills manifest in children with ADHD and common comorbidities, and relate to individual characteristics like gender and age.
Social Skills in ADHD
Social skills are in-the-moment building-block behaviors of social interaction (such as taking turns or starting conversations) and are distinguished from presumed outcomes of showing social skills (such as peer acceptance). Like any other skills, social skills must be taught, learned, and practiced (Gresham et al., 2001). Importantly, the term “social skills” refers to various individual skills that can each be acquired (or not acquired), even though a global score of social skills is often reported. For example, a child may have the skill of empathy, yet struggle with self-control, illustrating that children have unique patterns of acquired skills. A global score may reflect a mix of individual skills with varying levels of proficiency, and in such a case, the global score inadequately communicates the intricacies of the child’s social profile.
Children with ADHD are well-established to demonstrate poor global social skills relative to their peers, as well as deficits in specific individual skills (Van der Oord et al., 2005). For example, the individual social skills of communication, cooperation, assertion, self-control, responsibility, engagement, and empathy are each found to be poorer in children with ADHD relative to peers (Antshel & Remer, 2003; Marton et al., 2009; Van der Oord et al., 2005). Nonetheless, some intervention literature lends credence to the idea of distinguishing between poor social skills on average and patterns of individual social skill deficits. Social skills training has been largely ineffective when the outcome measure is global social skills (Morris et al., 2021). However, children with ADHD may be more likely to show improvements on specific social skills instead, such as assertion (Antshel & Remer, 2003). Thus, focusing on the global score may dilute a specific improvement and underestimate treatment effects.
Importantly, individual characteristics like child gender and age could relate to social skills acquisition and performance. Social skills occur in an interpersonal context where the skills that are valued and expected can differ based on gender. This may be why one study of neurotypical children found that boys performed better on certain social skills (problem solving and emotional regulation) while girls demonstrated more skill in interpersonal relationships (Gaspar et al., 2018). Because boys outnumber girls with ADHD around 3:1, and girls often go undiagnosed or require a more severe presentation in order to be noticed (Hinshaw et al., 2022), how ADHD and ADHD-related impairments manifest in girls have been understudied. Finally, as children develop, they gain more opportunities to learn and practice social skills, resulting in better mastery. However, this relationship may differ by gender. Ragnarsdottir et al. (2018) found that among children aged 5–10 with ADHD, younger boys exhibited more peer difficulties than older boys, whereas age was not associated with the social profile of girls.
Social Skill Deficits Associated with ADHD and Comorbidities
ADHD rarely occurs in isolation, with approximately one-third of children with ADHD having one additional disorder, and another third having two or three comorbidities (Reale et al., 2017). Internalizing disorders (anxiety and/or depression) occur in children with ADHD at rates of 25%–49% (Spencer et al., 2007). Externalizing disorders (oppositional defiant disorder [ODD] or conduct disorder [CD]) co-occur with ADHD at rates of 30%–50% (Spencer et al., 2007). Up to 24% of children with ADHD have both a comorbid internalizing and externalizing disorder (Armstrong et al., 2015). Because comorbidity in ADHD is the norm, it is useful for researchers and clinicians to understand the implications of co-occurring conditions for children’s functioning. It has been proposed that any additional comorbidity alongside ADHD will increase the risk for problems and not provide any attenuation of impairment (e.g., Jensen et al., 1997). The current study examines how patterns of comorbidities relate to the outcome of social skills, doing so in a more nuanced way than has usually been done in the literature.
Internalizing comorbidity
Given that internalizing disorders (without ADHD) tend to be associated with poorer social skills (Rubin et al., 2009), the addition of an internalizing comorbidity could confer different impairment in social skills, relative to ADHD without internalizing comorbidity. Internalizing disorders may lead to social withdrawal behaviors which do not typically occur in ADHD (Rubin et al., 2009). However, a second possibility is that comorbid internalizing disorders might dampen impulsivity in children with ADHD (Snyder, 2013) which could result in better social skills. Still, a third possibility is that the disruptive social behaviors associated with ADHD, when combined with an over-inhibited temperament associated with internalizing disorders, may lead to hard-to-read or inconsistent social skill performance.
The research evidence for each of these possibilities is unclear, which may be attributable to studies’ tendency to examine global social skills, as opposed to considering that different patterns may exist across specific, individual skills. In some studies, after controlling for ODD symptoms, children with ADHD and comorbid anxiety demonstrate poorer social skills than children with ADHD and no anxiety (Bishop et al., 2019; cf. S. S. Lee et al., 2012). Meta-analytic evidence demonstrates that, for children with ADHD, the addition of an internalizing diagnosis may either have no impact or an exacerbating effect on global social skill deficits (Becker, Langberg, et al., 2012), indicating the need for research that parses apart the specific patterns of impairment.
The effects of comorbid internalizing disorders on social skills may be more evident for individual instead of global social skills. Feldman et al. (2017) found that, for children with ADHD, future depression symptoms were mediated by impairment in specific social skills (cooperation, assertion, responsibility, and self-control). However, this study utilized the Social Skills Rating System (SSRS; Gresham & Elliott, 1990), whereas the updated Social Skills Improvement System (SSIS; Gresham & Elliott, 2007) includes additional subscales that may offer a more comprehensive assessment of social skills. Furthermore, Feldman et al. (2017) did not investigate whether these findings extend to comorbid anxiety, in addition to depression. Findings also vary by informant; some studies report that internalizing comorbidity may be associated with poorer parent-, but not teacher- or child-, reported social skills (Jensen et al., 2001; Becker et al., 2015; Feldman et al., 2017). This could reflect a context-specific pattern of social skill impairment, again reflecting the importance of research examining these questions in a nuanced way.
Externalizing comorbidity
Externalizing disorders (without ADHD) are associated with poor social skills, likely because externalizing behaviors often involve breaking social norms or rules (Campbell et al., 2000). Relative to other comorbidities, the research is most consistent that the co-occurrence of externalizing disorders and ADHD is associated with poorer global social skills compared to ADHD without externalizing comorbidity (Booster et al., 2012; but see Becker, Luebbe, & Langberg, 2012).
Nonetheless, nuances may also exist in this association and the particular social skill may matter. Previous research has implicated poor self-control and low emotional awareness in children with ADHD and comorbid externalizing disorders (Rosen et al., 2014; Factor et al., 2016). However, it is possible that the negative association between externalizing comorbidity and social skill deficits is stronger for some specific skills relative to others. Importantly, Factor et al. (2016) employed a measure of emotional awareness that does not account for other social skills essential for daily peer interactions. Moreover, Rosen et al. (2014) focused exclusively on youth with the combined presentation of ADHD, thereby limiting the generalizability of their findings. The informant may also matter. When parents rate social impairment in their children with ADHD and externalizing comorbidity, an exacerbating effect is almost always found (see Becker, Langberg, et al., 2012). Teacher report evidence is more inconsistent. Unfortunately, most studies with both parent and teacher informants combine the reports into a composite score and/or have low sample sizes (Becker, Langberg, et al., 2012), hindering assessment of potential informant differences.
Internalizing + externalizing comorbidity
An empirical examination of social skills among children with both internalizing and externalizing comorbidities remains relatively uncommon, despite evidence indicating that this comorbidity pattern occurs in approximately one quarter of children with ADHD. This relationship may be additive such that these children have worse social skills than children with only one comorbidity, or interactive such that they have exponentially worse social skills, or interactive such that the effects of externalizing comorbidity overshadow those of internalizing. Some preliminary evidence exists for each scenario.
Among children with ADHD, Booster et al. (2012) found that an externalizing comorbidity contributed to poorer global social skills, with no incremental effect of the presence of a comorbid internalizing disorder. This might suggest that the impact of externalizing disorders overshadows the social impairment associated with internalizing pathology. In other words, the relationship may be interactive, with internalizing disorders showing no association with social impairment when in the presence of externalizing disorders. Conversely, other research has pointed to the importance of internalizing disorders; Newcorn et al. (2004) found that adolescent social problems were best predicted by ADHD, CD, and an anxiety diagnosis. Here, this suggests unique and additive contributions of both externalizing and internalizing disorders impacting social functioning within ADHD. Finally, there is evidence that internalizing disorders only contribute to social impairment when an externalizing disorder is also present (Booster et al., 2012). This indicates possible interactive effects of having both comorbidities such that social skill performance is exponentially worse. In sum, research to date offers several possibilities for how dual comorbidity status impacts social skill performance.
Several factors complicate the literature examining children with ADHD who have both internalizing and externalizing comorbidities. First, because prior research has predominantly examined global social skills rather than specific skill domains (Jensen et al., 2001), this approach may be particularly limiting in studies of dual comorbidities. Children with internalizing versus externalizing comorbidities may exhibit distinct patterns of social skill impairments, leading to differential associations with specific social skills. Second, most studies that examine either internalizing or externalizing comorbidities in isolation rely on the SSIS (S. S. Lee et al., 2012; Feldman et al., 2017; Rosen et al., 2014), a standardized rating scale designed to assess social skills. In contrast, studies investigating children with both internalizing and externalizing comorbidities demonstrate considerable variability in measurement approaches (Booster et al., 2012). Additionally, Becker, Langberg, et al. (2012) note the importance of attending to informant differences (e.g., parent versus teacher) and sample characterization (e.g., diagnostic groups versus internalizing or externalizing symptoms on a spectrum), as these issues are inconsistently considered. Indeed, based on meta-analytic evidence, the use of gold-standard diagnostic procedures (to assess both ADHD and comorbidities) and multiple informant sources are recommended when studying social skills in children with ADHD (Ros & Graziano, 2018).
Current Study
Using a large and well-characterized aggregated sample of 1400 children with ADHD and comorbidities, we aimed to identify both global and subscale-specific patterns of parent- and teacher-rated social skill deficits associated with ADHD only, relative to ADHD with: internalizing comorbidity (ADHD + INT), externalizing comorbidity (ADHD + EXT), and internalizing + externalizing comorbidity (ADHD + DUAL). To our knowledge, this study is the first to investigate specific social skills in such a sample. Furthermore, this study sought to extend beyond the global score to examine subscale-specific social skill patterns in children with dual comorbidities, an area that has yet to be systematically explored. Global and specific skill performance was expected to vary based on comorbidity status, with any comorbidity being worse than ADHD only, ADHD + INT being the most variably impairing, and ADHD + EXT and ADHD + DUAL being the most consistently socially impairing. Finally, we leveraged the large sample size to explore the associations of child gender and age with social skill performance.
Method
Participants
This study represents a secondary analysis of data collected from sites across the United States and Canada. Eight existing datasets from four research groups were aggregated to create a deidentified sample comprising 1,400 children aged 7 to 12 (28% girls) with clinical diagnoses of ADHD. Participants in the original datasets were recruited via a variety of means, including through schools, hospitals, the community, and self-referrals. Datasets were obtained from the University of British Columbia (UBC), the Université du Québec en Outaouais (UQO), and the University of Virginia (UVA) reflecting Research Group 1; the University of California at San Francisco (UCSF) and the University of California at Berkeley (UCB) reflecting Research Group 2; Florida State University (FSU) reflecting Research Group 3; and the Multimodal Treatment of ADHD Cooperative Group (MTA) which was conducted at seven sites across the United States and Canada, reflecting Research Group 4. Research groups reflect multiple sites of the same study or same researcher. Table 1 provides summaries for each dataset. Although some datasets were treatment studies, in all cases we used the baseline (pre-treatment) data.
Dataset Demographics.
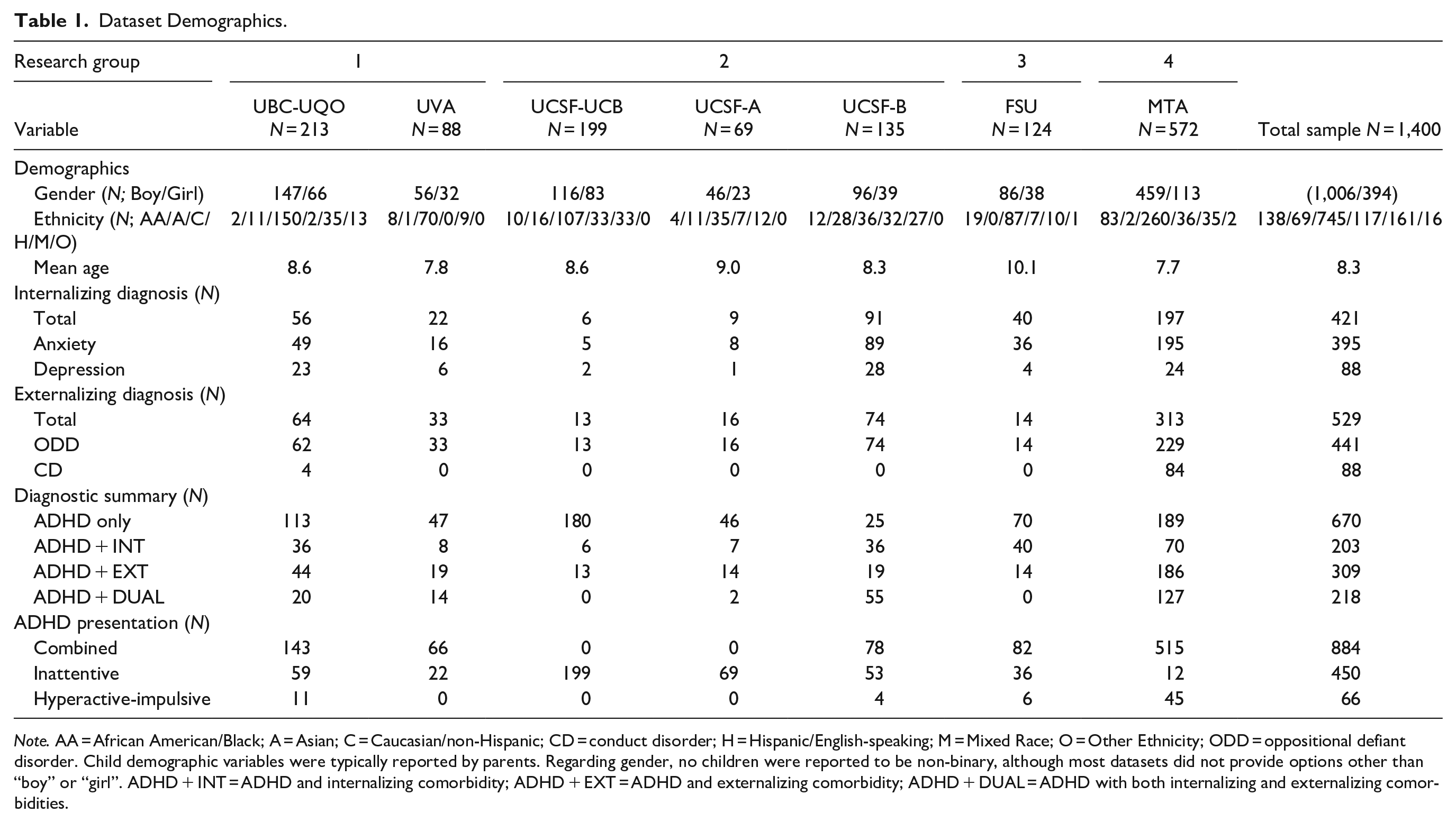
Note. AA = African American/Black; A = Asian; C = Caucasian/non-Hispanic; CD = conduct disorder; H = Hispanic/English-speaking; M = Mixed Race; O = Other Ethnicity; ODD = oppositional defiant disorder. Child demographic variables were typically reported by parents. Regarding gender, no children were reported to be non-binary, although most datasets did not provide options other than “boy” or “girl”. ADHD + INT = ADHD and internalizing comorbidity; ADHD + EXT = ADHD and externalizing comorbidity; ADHD + DUAL = ADHD with both internalizing and externalizing comorbidities.
Measures
Global and specific social skills
Each dataset contains both parent and teacher report about the child’s displayed social skills on either the SSIS (Gresham & Elliott, 2007) or its predecessor, the SSRS (Gresham & Elliott, 1990). Both scales generate a global social skills score, and also provide subscale scores reflecting specific social skills. The social skills measured cover a range of situations at home (parent form) and at school (teacher form), that involve social behaviors directed to both peers and adults. There is high convergent validity on both parent and teacher forms, and global and subscale social skills scores, between the SSRS and SSIS (see Gresham et al., 2011). All children in our sample were rated on the Elementary Form (grades K-6) of the SSIS or SSRS.
The SSIS includes 46 parent and 30 teacher social skills items. Each is rated on a 4-point scale (0 = Never, 1 = Seldom, 2 = Often, 3 = Almost Always) to indicate the frequency of the behavior. Items are summed to generate a total raw score reflecting a global score of social skills, which is converted to a standard score (M = 100, SD = 15) based on gender norms. There are seven subscales of specific social skills (communication, cooperation, assertion, responsibility, empathy, engagement, and self-control), which are raw scores and not standardized. In the SSIS norming sample (N = 4,700), the internal consistency of the total social skills score on the elementary form was .97 (teacher report) and .95 (parent report). Internal consistency for the subscales ranged from .83 to .92 (teacher report) and .74 to .86 (parent report). The 6- to 8-week test-retest reliability of the total social skills score was .84 (teacher report) and .86 (parent report), with subscale reliability coefficients ranging from .74 to .86 (teacher report) and .76 to .86 (parent report). Regarding validity, Gresham and Elliott (2007) report moderate positive correlations between parent and teacher reports for the same child, as well as between the SSIS total social skills score and subscales with the Social Skills scale on the Behavior Assessment System for Children, Second Edition (Reynolds & Kamphaus, 2006).
The SSRS consists of 39 parent and 30 teacher social skills items, each rated on a 3-point frequency scale (0 = Never, 1 = Sometimes, 2 = Very Often). There is a global score of total social skills, reflecting the sum of all items, converted to a gender-normed standard score. There are four subscales of specific social skills (cooperation, assertion, responsibility, self-control) on the parent form, and three on the teacher form (cooperation, assertion, self-control); subscales are raw scores and not standardized. The SSRS does not contain the subscales of communication, empathy, or engagement on either parent or teacher form. In the SSRS norming sample (N = 4,170), the internal consistency of the total social skills score on the elementary form averaged .94 (teacher report) and .87 (parent report), with subscale internal consistency ranging from .86 to .91 (teacher report) and .64 to .79 (parent report). The 4-week test-retest reliability of the total social skills score was .85 (teacher report) and .87 (parent report), while subscale reliability coefficients ranged from .75 to .88 (teacher report) and .77 to .84 (parent report). Gresham and Elliott (1990) also report positive correlations between the total score and subscales with parent and teacher ratings of social competence on the Child Behavior Checklist (Achenbach & Edelbrock, 1983) and the Harter Teacher Rating Scale (Harter, 1982), respectively.
Data Reduction
Due to small differences in the subscale items and the response metric between the SSIS and SSRS, each subscale raw score was converted into a proportion score reflecting how many points out of the possible maximum were endorsed (e.g., 60% of maximum). These proportion scores allow for direct comparison between the SSIS and SSRS subscales. The SSIS and SSRS yield standardized scores for the total social skills score, so comparison was not an issue.
Procedures
Dataset selection
The inclusion criteria for datasets in the current study were: (a) well-characterized sample of elementary school-aged children (ages 7–12) clinically diagnosed with ADHD, (b) parent and teacher ADHD rating scale data, (c) parent and teacher SSIS or SSRS global and subscale scores, and (d) comorbidity diagnostic status variables. Deidentified datasets were obtained through a variety of means including the National Institute of Mental Health Data Archive access, listserv postings, and word-of-mouth. A university research ethics board approved each data transfer.
Diagnostic procedure for ADHD and comorbidities
Table 2 shows the procedures used by each site to diagnose ADHD and comorbidities in their respective samples. All children in all datasets had a validated ADHD diagnosis based on DSM criteria (i.e., DSM-IV, DSM-IV-TR, or DSM-5) when the data were collected. Each site used rigorous methods and gold-standard procedures, including multi-informant interview and questionnaire data. No site excluded children based on comorbidity status, and symptoms of anxiety, depression, ODD, and CD were obtained for all children. Overall, comorbid diagnoses were made using best estimates and consensus diagnostic practices and each data collection site’s procedures were comparable. We considered children to have a comorbid internalizing disorder if they had an anxiety and/or depressive disorder. 1 We considered children to have a comorbid externalizing disorder if they had ODD or CD.
Dataset Diagnostic Procedures.
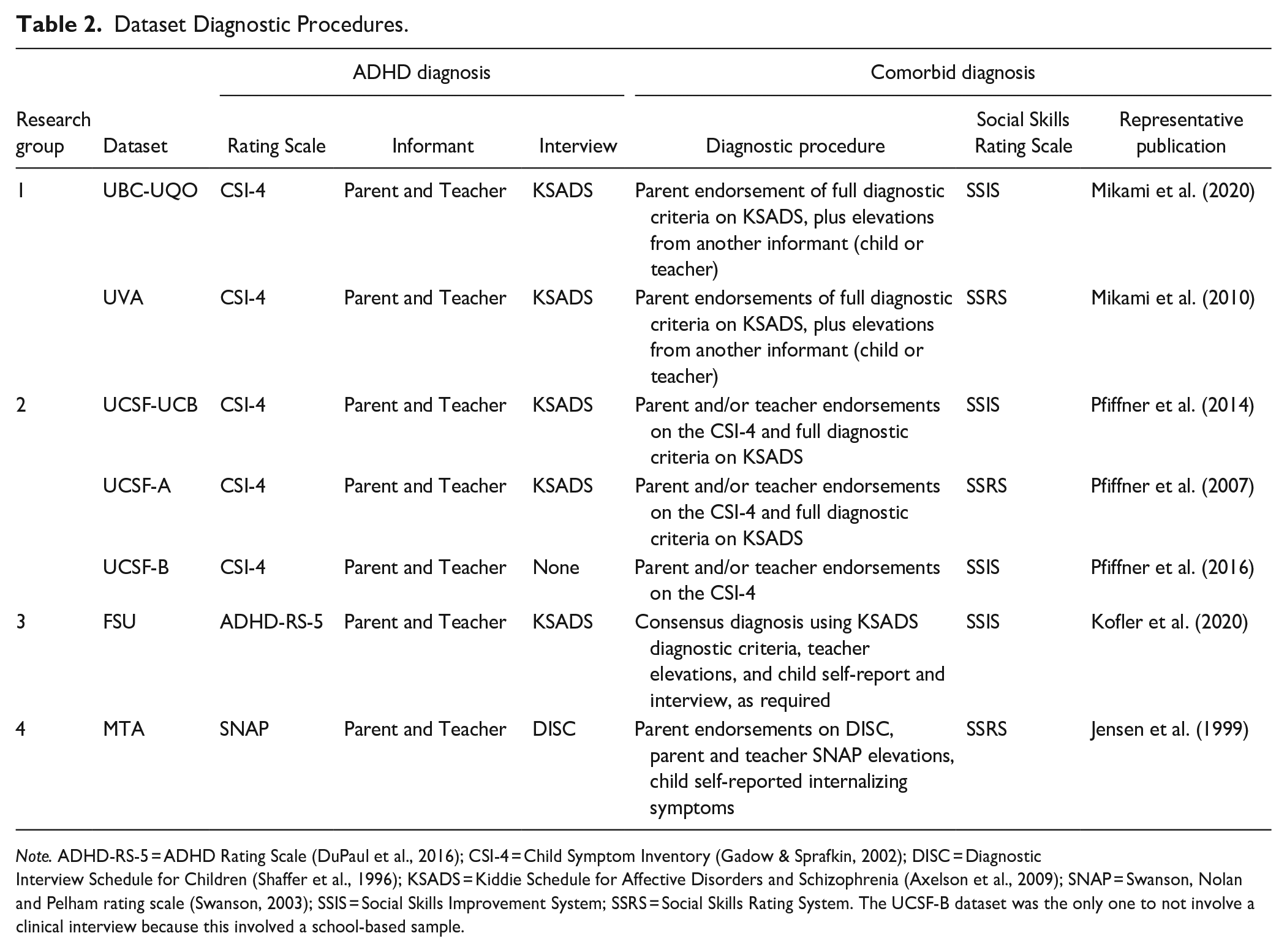
Note. ADHD-RS-5 = ADHD Rating Scale (DuPaul et al., 2016); CSI-4 = Child Symptom Inventory (Gadow & Sprafkin, 2002); DISC = Diagnostic Interview Schedule for Children (Shaffer et al., 1996); KSADS = Kiddie Schedule for Affective Disorders and Schizophrenia (Axelson et al., 2009); SNAP = Swanson, Nolan and Pelham rating scale (Swanson, 2003); SSIS = Social Skills Improvement System; SSRS = Social Skills Rating System. The UCSF-B dataset was the only one to not involve a clinical interview because this involved a school-based sample.
Data Analytic Plan
The 1,400 participants in the current study all came from datasets where the research team had data on both parent and teacher forms of the SSIS (671 participants) or SSRS (729 participants), comorbidity status, age, and gender. Small numbers of participants were missing data on individual SSIS/SSRS subscales, or the global score (which was unable to be computed if a subscale was missing); see Table 3. Missing data were handled by listwise deletion.
Descriptive Statistics.
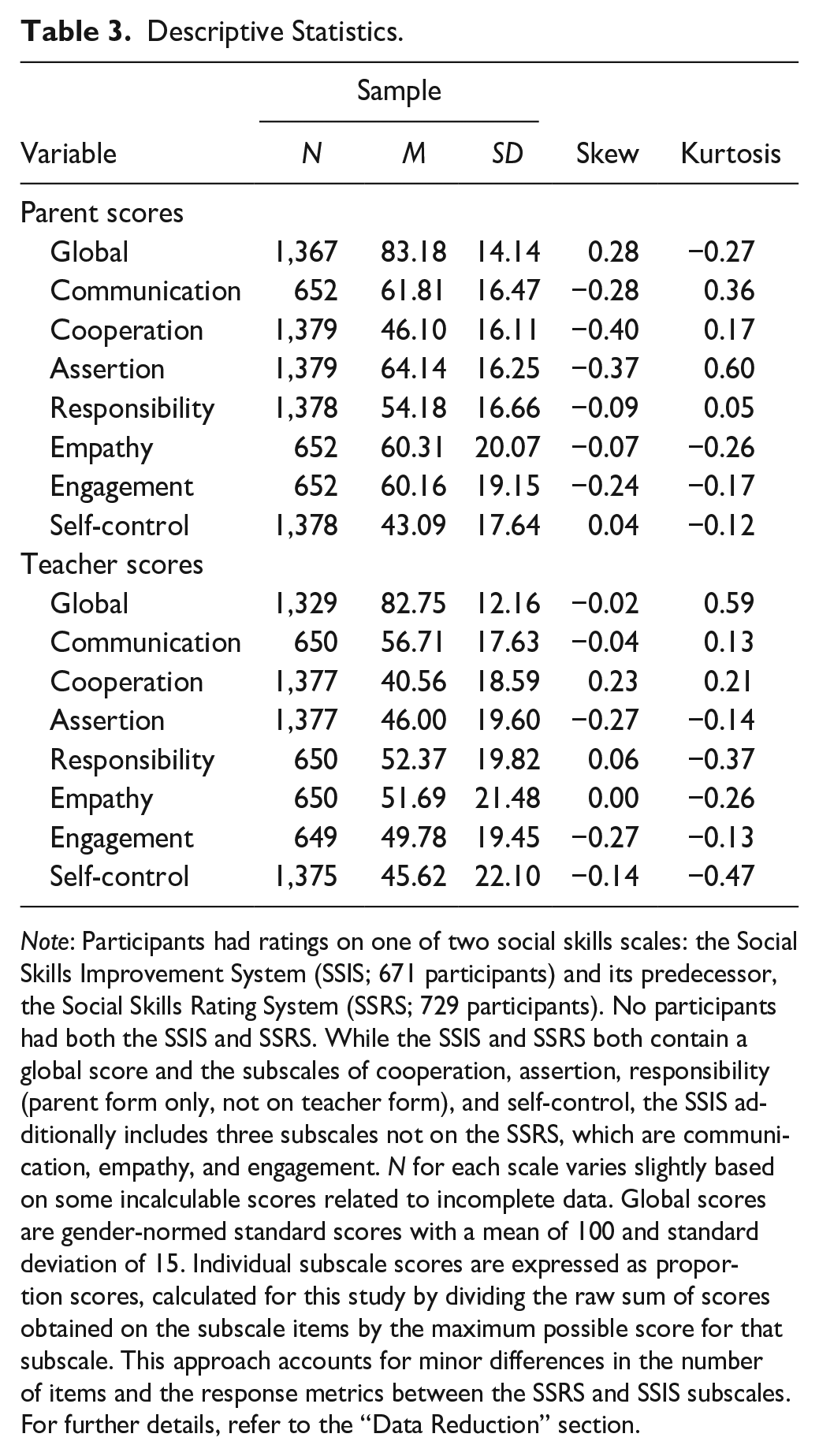
Note: Participants had ratings on one of two social skills scales: the Social Skills Improvement System (SSIS; 671 participants) and its predecessor, the Social Skills Rating System (SSRS; 729 participants). No participants had both the SSIS and SSRS. While the SSIS and SSRS both contain a global score and the subscales of cooperation, assertion, responsibility (parent form only, not on teacher form), and self-control, the SSIS additionally includes three subscales not on the SSRS, which are communication, empathy, and engagement. N for each scale varies slightly based on some incalculable scores related to incomplete data. Global scores are gender-normed standard scores with a mean of 100 and standard deviation of 15. Individual subscale scores are expressed as proportion scores, calculated for this study by dividing the raw sum of scores obtained on the subscale items by the maximum possible score for that subscale. This approach accounts for minor differences in the number of items and the response metrics between the SSRS and SSIS subscales. For further details, refer to the “Data Reduction” section.
An a priori power analysis using GPower v3.1 (Faul et al., 2007) found that to detect small effects (f = .10) with power = .95, α = .05 and with four groups (ADHD only, ADHD + INT, ADHD + EXT, ADHD + DUAL), the required sample size is N = 1,302. Thus, this study is well-powered for the analyses involving the global score and the subscales that are present on both the SSIS and SSRS; however, the sample size is 671 for the subscales that are present on the SSIS only and not the SSRS.
Data analyses were conducted using R Studio. Participants were nested within Research Group in all models, to account for potential differences between data collection sites. The nested model was a significantly better fit than a complex model for both parent (p < .005) and teacher (p < .005) rated social skills. For each social skill outcome variable, a model was conducted for parent-rated social skills and then repeated for teacher-rated social skills. To test group differences in the outcome variable of the global social skills total score, an ANCOVA was conducted with two dichotomous predictors: internalizing comorbidity (0 = not present, 1 = present) and externalizing comorbidity (0 = not present, 1 = present). Child age and gender were included as covariates, to examine how social skills relate to these characteristics. The main effect of each predictor tested the incremental effects of having an internalizing or externalizing comorbidity on social skill performance, relative to having ADHD without that comorbidity. We also tested the statistical interaction between the presence of internalizing and externalizing comorbidities. Analyses were repeated for each specific social skill subscale.
Results
Descriptive Statistics
Sample means, standard deviations, skew, and kurtosis for the variables of global social skills, and specific subdomains, are in Table 3. For each comorbidity group, global social skill means were lower (indicating poorer skills) than the SSIS and SSRS norming samples (M = 100; SD = 15). Supplementary Table 1 shows the mean and standard deviations for each social skill separated by comorbidity group. Supplementary Table 2 shows that the bivariate correlation between parent and teacher ratings was low for global social skills (r = 0.24) and for the specific subscales (r = 0.15-0.37), though in line with what was found in the norming samples (Gresham & Elliott, 1990, 2007). This supported conducting separate models for parent-reported and teacher-reported social skills.
Global Social Skill Performance
All ANCOVA results and effect sizes can be found in Table 4. When the Benjamini-Hochberg procedure was applied to adjust the false discovery rate considering the number of comparisons being tested (Benjamini & Hochberg, 1995), all results survived correction. The global social skills scores reflect standardized, gender-normed scores.
Group Differences in Parent and Teacher Reported Social Skills.
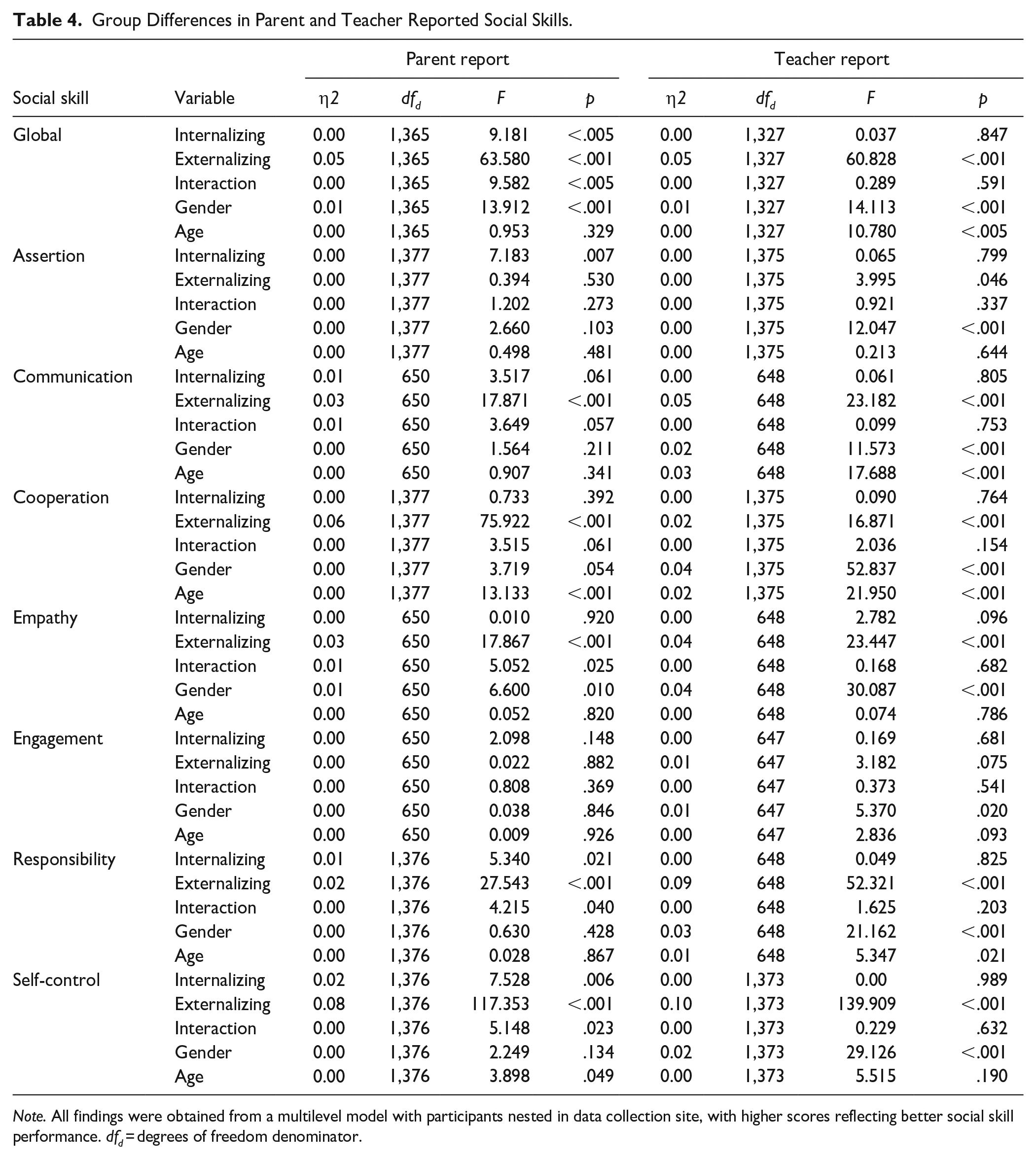
Note. All findings were obtained from a multilevel model with participants nested in data collection site, with higher scores reflecting better social skill performance. dfd = degrees of freedom denominator.
Parent ratings
Parents rated global social skills as more impaired for the ADHD + INT group (F1,1365 = 9.181, p < .001) as well as for ADHD + EXT group (F1,1365 = 63.580, p < .001), relative to children with ADHD only. The interaction between internalizing and externalizing comorbidity status was significant (F1,1365 = 9.582, p < .001), such that the ADHD + DUAL group performed similarly to the ADHD + EXT group (Figure 1). Additionally, gender (though not age) was a significant covariate, such that girls had worse scores than boys (F1,1365 = 13.916, p < .001).
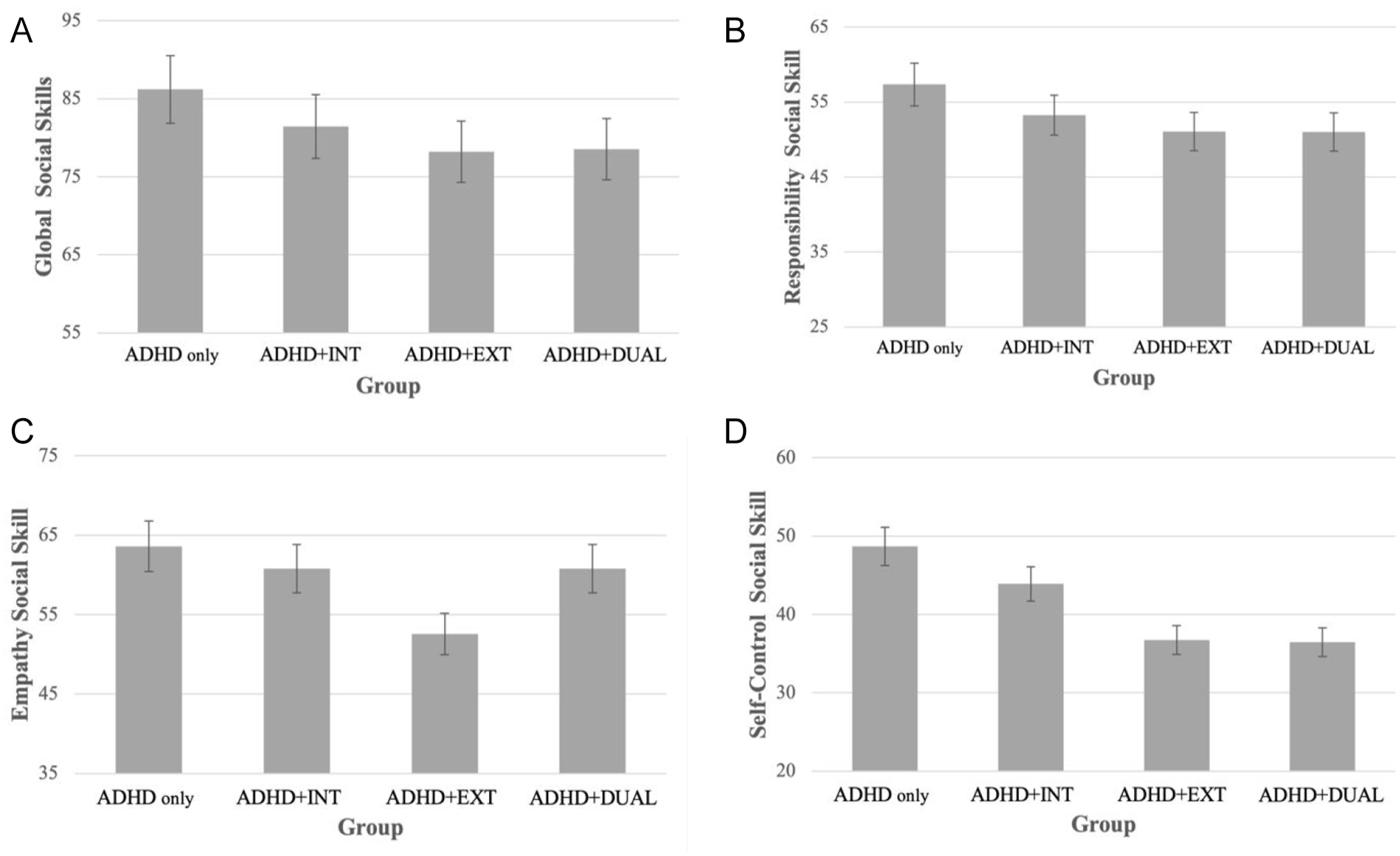
Illustration of statistical interaction effects on parent-reported social skills. (A) represents the parent-reported global social skills score, (B) represents the parent-reported responsibility subscale, (C) represents the parent-reported empathy subscale, and (D) represents the parent-reported self-control subscale. These reflect the four outcome variables for which the INT × EXT interaction term was statistically significant in the ANCOVA models. The bar graph illustrates the social skills profile for an average child in each comorbidity group based on our data.
Teacher ratings
Teachers rated the ADHD + EXT group as having poorer global social skills (F1,1327 = 60.828, p < .001) relative to children with ADHD only. Both age (F1,1327 = 10.779, p < .001) and gender (F1,1327 = 14.113, p < .001) were significant covariates, where younger children and girls had worse scores. The comparison between the ADHD + INT and ADHD only groups was nonsignificant; nor was there an interaction effect between internalizing and externalizing comorbidity status in the teacher report model.
Subscale Specific Social Skill Performance
These ANCOVA results and effect sizes are also in Table 4. All but one analysis survived the Benjamini-Hochberg procedure (teacher-reported assertion and ADHD + EXT). The subscale scores represent proportion scores (see above), derived from raw data and not gender-normed.
Parent ratings
Communication
Parents rated communication as more impaired in the ADHD + EXT group (F1,650 = 17.871, p < .0001) compared to children with ADHD only, while all other associations and interactions for this outcome were nonsignificant.
Cooperation
Similarly, there was a main effect where the ADHD + EXT group was rated as having poorer cooperation skills (F1,1377 = 75.922, p < .001) relative to children with ADHD only. Neither the main effect of ADHD + INT, nor the interaction effect between externalizing and internalizing comorbidity, was significant. Age (but not gender) was a significant covariate (F1, 1377 = 13.122, p < .001) such that older children demonstrated better cooperation.
Assertion
Conversely, there was a main effect such that the ADHD + INT group had poorer parent-rated assertion (F1,1377 = 7.183, p = .007) compared to children with ADHD only. No other variables or covariates were significant for the outcome of assertion.
Responsibility
There were main effects of ADHD + INT (F1,1376 = 5.340, p = .021), as well as ADHD + EXT (F1,1376 = 27.543, p < .001), associated with poorer responsibility, compared to ADHD only. The interaction effect between internalizing and externalizing comorbidity was significant (F1,1376 = 4.215, p = .040), such that the ADHD+DUAL group performed similarly to the ADHD + EXT group (Figure 1). Neither age nor gender was associated with responsibility.
Empathy
Parents rated empathy as poorer in the ADHD + EXT group (F1,650 = 17.867, p < .001) relative to ADHD only. The interaction effect between internalizing and externalizing comorbidity was also significant (F1,650 = 5.052, p = .025), such that the ADHD + EXT group performed worse than the ADHD + DUAL group (Figure 1). That is, the negative association between externalizing comorbidity and the social skill of empathy was buffered by the addition of an internalizing comorbidity. Neither age nor gender was significant.
Engagement
No significant covariates, main effects of ADHD + INT or ADHD + EXT relative to ADHD only, or the interaction effect between the two comorbidities, were present.
Self-control
The parent model demonstrated main effects of both ADHD + INT (F1,1376 = 7.528, p = .006) and ADHD + EXT (F1,1376 = 117.353, p < .001) as associated with poorer self-control, compared to ADHD only. The interaction effect between internalizing and externalizing comorbidity was also significant (F1,1376 = 5.148, p = .023), such that the ADHD + DUAL group performed similarly to the ADHD + EXT group (Figure 1). Age (but not gender) was a significant covariate (F1, 1376 = 3.898, p = 0.490); older children had poorer self-control.
Teacher ratings
Communication
Children with ADHD + EXT were rated by teachers as having poorer communication skills (F1,648 = 23.182, p < .001), relative to children with ADHD only. The comparison between the ADHD + INT and ADHD only groups, and the interaction effect between internalizing and externalizing comorbidity, were nonsignificant. Gender (F1, 648 = 11.573, p < .001) and age (F1,648 = 17.688, p <.001) were both significant covariates, such that girls and older children were rated as having better communication.
Cooperation
Similarly, cooperation was rated poorer in the ADHD + EXT group (F1,1375 = 16.871, p < .001) compared to in the ADHD only group. No main effects for ADHD + INT or the interaction between internalizing and externalizing comorbidity were significant. Gender (F1,1375 = 52.837, p < .001) and age (F1,1375 = 21.950, p < .001) were both significant covariates, with girls and older children displaying better cooperation.
Assertion
There was a main effect for ADHD + EXT being associated with poorer assertion (F1,1375 = 3.995, p = .046) compared to ADHD only. Similar to other subscales, there was no significant main effect of ADHD + INT, nor a significant interaction effect between internalizing and externalizing comorbidity. Gender (but not age) was a significant covariate (F1,1375 = 12.047, p < .001) with girls displaying better assertion than boys.
Responsibility
Responsibility was rated as poorer in children with ADHD + EXT (F1,648 = 52.321, p < .001) relative to children ADHD only. The main effect of ADHD + INT relative to ADHD only, and the interaction between internalizing and externalizing comorbidity, were nonsignificant. Gender (F1,648 = 21.162, p < .001) and age (F1,648 = 5.347, p = .021) were significant covariates, such that girls and older children were rated as having better responsibility.
Empathy
Teachers rated the ADHD + EXT group as having poorer empathy (F1,648 = 23.447, p < .001) compared to the ADHD only group. The ADHD + INT group did not differ from the ADHD only group in teacher-rated empathy, nor was there an interaction between internalizing and externalizing comorbidity. Gender (but not age) was a significant covariate (F1,648 = 30.087, p < .001); girls were rated as having better empathy than boys.
Engagement
There were no significant main effects or interactions in the teacher model for engagement. However, gender (but not age) was a significant covariate in the model (F1,647 = 5.370, p = .021), with girls rated as displaying better engagement than boys.
Self-control
Children with ADHD + EXT received teacher ratings of poorer self-control (F1,1373 = 139.909, p < .001) compared to children with ADHD only. The main effect of ADHD + INT, and the interaction between internalizing and externalizing comorbidity, were nonsignificant. Gender (F1,1373 = 29.126, p < .001) and age (F1,1373 = 5.515, p = .019) were significant covariates, such that girls and older children were rated as having better self-control.
Exploratory Analyses
Identical models were conducted for global social skills and each subscale, considering only anxiety disorders (excluding depression) as an internalizing comorbidity. As shown in Table 1, the majority of children with an internalizing comorbidity had anxiety disorders, and there are theoretical distinctions between anxiety and depression. Subsequently, we repeated these models for global social skills and each subscale, considering only ODD (excluding CD) as an externalizing comorbidity, given that most children with an externalizing comorbidity had ODD (Table 1). As shown in Supplementary Tables 3 and 4, the overall results remained largely consistent with the original models. However, the interaction effects between internalizing and externalizing comorbidities on parent-reported communication and cooperation became statistically significant. Specifically, for children with an externalizing comorbidity, the presence of an additional internalizing comorbidity was associated with better social skills. That is, the ADHD + EXT group demonstrated the greatest social skill impairments, followed by ADHD + DUAL, ADHD + INT, and ADHD only, in that order.
Finally, identical models were conducted for global social skills and each subscale while adding ADHD presentation as a covariate alongside age and gender. ADHD presentation was not included in the main analysis owing to indications that it may not be stable over time (Lahey et al., 2005). Supplementary Table 5 shows that children with ADHD inattentive presentation generally tended to be rated as having better social skills than the other presentations. Results for the main and interaction effects of comorbidity were largely unchanged.
Discussion
The current study leveraged a well-characterized, aggregated sample of 1,400 children with ADHD to examine the contribution of internalizing (i.e., anxiety or depression) and externalizing (i.e., ODD or CD) comorbidities, as well as age and gender, to their social skill profiles. Results suggested that children with ADHD and these comorbidities had poorer social skills relative to children with ADHD only, as perceived by parents and teachers, but also that there may be different social skill profiles depending on the comorbid condition and informant.
Internalizing Comorbidity
Existing literature is inconsistent regarding whether comorbid internalizing disorders are associated with poorer social skills in children with ADHD. Existing literature presents inconsistent findings regarding whether comorbid internalizing disorders are associated with poorer social skills in children with ADHD. The current study supports this association, as ADHD + INT was linked to poorer parent-rated but not teacher-rated global social skills relative to ADHD only. This finding is consistent with Becker et al. (2015), who reported that internalizing comorbidity was specifically related to poorer social skills based on parent-report. Additionally, our results suggest that, rather than mitigating ADHD-related impulsivity in a way that benefits social skills (see Jarrett & Ollendick, 2008), internalizing comorbidity may be associated with poorer social skills, at least from the perspective of parents. Given that previous research on this topic has often combined parent and teacher ratings into a composite score or relied on only one informant, such approaches may have obscured informant-specific patterns (see Becker, Langberg, et al., 2012, for a discussion of this issue).
In addition to global performance, parents rated specific social skills as poorer for ADHD + INT relative to children with ADHD only: namely assertion, responsibility, and self-control. This demonstrates how social impairment in children with ADHD+INT may be represented by a nuanced pattern of deficits, possibly diluted to the point of becoming indetectable in some small samples if only global scores are considered. The particular impaired subdomains of social skills associated with ADHD + INT in this study have been found to relate to depression in children (Feldman et al., 2017). The assertion and responsibility subscales include behaviors like introducing oneself to others and asking for help and communicating effectively with adults; these outward-facing behaviors require confidence and social initiative, which might be difficult for children who worry about making mistakes, fear being judged, or experience low mood. Items in the self-control subscale reflect response to conflict, which on the surface might seem associated with externalizing disorders. However, items such as “responds appropriately to teasing” do not indicate what the child does when being teased. That is, a child who lashes out and a child who cries may both be responding inappropriately, in different ways.
Externalizing Comorbidity
Both parents and teachers reported global social skills as more impaired in ADHD + EXT relative to children with ADHD only, as expected based on previous literature (Booster et al., 2012). However, the current study went beyond this to examine subdomain specific social skills. Although parents and teachers mostly agreed that ADHD + EXT related impairments are visible across most individual social skills, interestingly, not every subscale was associated with poorer performance. In the current sample, teachers rated assertion, communication, cooperation, responsibility, empathy, and self-control lower in children with ADHD + EXT compared to ADHD only; this is consistent with previous research (Factor et al., 2016; Rosen et al., 2014). Parents, like teachers, reported similar impaired subdomains, rating communication, cooperation, self-control, responsibility, and empathy lower for ADHD + EXT relative to ADHD only.
However, engagement was not rated by either parents or teachers as worse in children with ADHD + EXT compared to ADHD only. The engagement subscale assesses the ability to approach peers and join activities, such as by asking peers to play, introducing self, and starting conversations. These children may appropriately express interest in peers’ activities, as indicated by the absence of significant impairment in engagement; however, the quality of their interactions may be lower, as reflected in deficits in cooperation and communication (C. A. Lee et al., 2018; Ronk et al., 2011). The majority of the children in the sample with ADHD + EXT had ODD (characterized by defiance toward adult instructions) as opposed to CD (containing antisocial behavior that could be directed at peers). Because the engagement subscale focuses more on peer interactions instead of adult-directed behaviors, ODD may not confer additional risk for problems in engagement.
Externalizing + Internalizing Comorbidity
The pattern of social skills associated with ADHD + DUAL (comorbid internalizing and externalizing disorders) is the least well-researched, yet this characterization describes up to one fourth of children with ADHD. A novel aspect of this study was its examination of whether there were statistical interaction effects between internalizing and externalizing comorbidity, and if so, were social difficulties compounded, overshadowed, or exponentially impairing?
Interaction effects were found for the outcome measures of parent-reported global social skills, and in the specific parent-reported subdomains of responsibility, self-control, and empathy. For the global score, and the subdomain scores for responsibility and self-control, ADHD + DUAL performed similarly to those with ADHD + EXT. In other words, any effects of internalizing were overshadowed by externalizing-related impairments. While there is very limited research explicitly investigating interaction effects between internalizing and externalizing comorbidity in children with ADHD, and existing studies report inconsistent results, these findings align with Booster et al. (2012) who found that children with both internalizing and externalizing comorbidities performed similarly on social skills relative to children with externalizing comorbidities only. Notably, global social skills, and the subdomains of self-control and responsibility, were each found to be significantly associated with ADHD + INT as a main effect. The interaction effects for these outcomes, however, imply that internalizing comorbidities do not incrementally add to poorer performance in these subdomains when an externalizing comorbidity is already present.
Interestingly, the interaction for parent-reported empathy indicated that ADHD + DUAL performed better than those with ADHD + EXT. This suggests that the impairments in empathy experienced by children with ADHD + EXT may potentially be buffered by the addition of an internalizing diagnosis. Researchers have argued that externalizing behaviors exhibited by children with ADHD might be inhibited by comorbid anxiety disorders (see Jarrett & Ollendick, 2008). If that is the case, it is interesting that this relationship was only observed in the subscale of empathy. Evidence from a non-ADHD sample has suggested that empathy may be involved in the development and/or maintenance of anxiety symptoms in adolescents (Gambin & Sharp, 2018). Future work should consider these associations in an ADHD sample, considering a more nuanced understanding of internalizing comorbidities and empathy.
Gender and Age
Girls were reported as having poorer global social skills by both parents and teachers, while teachers noted higher raw scores for girls on every specific subscale. Because the global score is gender normed, this suggests parents and teachers perceive girls with ADHD to have more deficient social skills relative to their female peers, than they perceive boys with ADHD to be deficient relative to their male peers. Meanwhile, at least teachers perceived girls with ADHD to have objectively more skilled behavior (as indicated by the raw scores on the subscales) relative to boys with ADHD. This might suggest that the social impairment of girls with ADHD is greater than that of their male counterparts, perhaps because the core symptoms of ADHD interfere more with the expected social behaviors for girls (e.g., taking turns in conversations, listening to others, following directions) relative to for boys. Said another way, the gap between the social behaviors of girls with ADHD and their female peers is greater than the gap between the social behaviors of boys with ADHD and their male peers, even if objectively, girls with ADHD may be performing more socially skilled behaviors compared to boys with ADHD. It is important to remember that, although each research group attempted to recruit broadly and via community sources, it is possible that only the most severely affected girls enrolled in the studies; thus, results may not generalize to the population of girls with ADHD.
When age was a significant covariate, it was nearly always that older children displayed better social skills. As children mature, they have more opportunities to learn and practice social skills, so the logical progression may be that these skills improve over time. Our results suggest that this maturation process may occur in children with ADHD a well as in neurotypical children. One exception to the overall pattern in our data was that parent-reported self-control was rated as better for younger children (though teachers rated self-control as better for older children).
Parent Versus Teacher Report
Nuanced relationships between internalizing and externalizing comorbidities were found exclusively for parent-reported social skills. Instead, teacher report only implicated ADHD + EXT as associated with poorer social skills compared to ADHD only, across both the global score and subdomains. The informant discrepancies between parent and teacher report are consistent with some previous studies (Becker et al., 2015; Becker, Langberg, et al., 2012; Jensen et al., 2001), and may reflect differences in the expression of social impairment associated with each comorbidity, even when in the same social skills subdomain. While deficits in responsibility may manifest as back-talk to adults by a child with ADHD + EXT, it may present as avoidance of interaction by a child with ADHD + INT. Similarly, communication deficits may appear as rule-breaking for children with ADHD + EXT versus an inability to join others at play for those with ADHD + INT.
Informant discrepancies are common in child psychopathology research (De Los Reyes & Kazdin, 2005). In this particular case, the way that internalizing-related social skills deficits are expressed may help explain why parents are more likely than teachers to report associations between social difficulty and internalizing disorders. At home, parents may have more bandwidth to notice such internalizing-related behaviors and identify them as social difficulties, whereas at school, externalizing-related social difficulties might be so disruptive that they overshadow any internalizing-related behaviors.
It may also be the case that children display different behaviors at home versus at school, or that each environment requires somewhat different social skills. Additionally, in our sample, interview data about children’s internalizing disorders were provided by parents, whose own internalizing psychopathology may influence their perceptions of their child’s internalizing psychopathology and social skills (De Los Reyes & Kazdin, 2005). An avenue for clarification could involve including child self-report, observation, or peer report. Future research should continue to probe why informant discrepancies are so prevalent, and what they might suggest about both measurement and social skill performance in children with ADHD.
Limitations
Several study limitations should be considered. First, some datasets contained ratings on the SSIS, whereas others used its predecessor, the SSRS, but these measures are not exactly comparable. Similarly, internal consistency statistics for the SSIS/SSRS could not be calculated in the current sample owing to the unavailability of item-level data. Additionally, the present study considered children who had either anxiety and/or depression as having internalizing comorbidity, and children who had either ODD or CD as having externalizing comorbidity (though see Supplementary Tables 3 and 4). In this sample, anxiety and ODD were far more common than depression and CD, perhaps due to the age of the children or study inclusion/exclusion criteria. Future studies that encompass a larger age range might determine if a more precise comorbidity group yields distinct patterns of social skill impairment. Some datasets also included children with a specific phobia under the anxiety umbrella. This may have increased the rates of internalizing comorbidity in the current study, and future work could parse apart types of anxiety disorders. Additional work might also consider how ADHD presentation relates to the relationship between social skills and comorbidity (see Supplementary Table 5), or compare these results to a neurotypical control group. Other child characteristics like ethnicity and IQ could be investigated as they relate to comorbidity and social skill performance as well. The present study considered gender as a binary variable owing to the structure of the pooled datasets. However, the social skills profiles of children with diverse gender identities represent a critical and understudied area of research and should be considered as a future direction. In addition, while the current study focused on social skills, future work should investigate patterns of impairment on other social variables like friendship, social cognition, or peer rejection. Lastly, future research should incorporate more advanced analytic methods for large pooled datasets, such as latent class analysis or individual participant data meta-analysis.
Clinical Implications and Conclusion
Given the challenges in improving social skills in children with ADHD (Morris et al., 2021), perhaps interventions could be tailored to reflect unique patterns of strengths and weaknesses to improve treatment response. Our results also lend credence to the concept that individual social skills can be learned independent of one another. Thus, children with different comorbidity patterns may need different social skills to be targeted in treatment (e.g., assertion for those with internalizing comorbidities). Our findings also suggest the utility of measuring specific social skills as treatment outcomes, so that potential treatment effects are not masked by a global social skills score. Future research could further delineate these specific skill differences further by developing standardized, normed subscale scores. Such benchmarks would facilitate comparisons across youth and help identify targeted areas for intervention. However, given the high level of agreement between parents and teachers regarding both global and subscale social skill ratings for ADHD + EXT, once the influence of other individual differences has been adequately examined, it may be cost- and time-efficient, particularly in research contexts, to rely on global scores as a representative measure of social skills.
Finally, if girls with ADHD, compared to boys with ADHD, objectively perform more skilled behaviors but deviate more from their same-gender peers, understanding this could help parents and teachers build empathy for these children. From a psychoeducational perspective, these findings could be used to enhance awareness of how social skill deficits manifest in different contexts. For example, psychoeducation efforts might highlight that when girls with ADHD interact with same-gender peers, their social norm violations may be perceived as more pronounced compared to when they interact with boys.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251344711 – Supplemental material for Social Skill Profiles in ADHD and Comorbid Disorders
Supplemental material, sj-docx-1-jad-10.1177_10870547251344711 for Social Skill Profiles in ADHD and Comorbid Disorders by Caroline E. Miller, L. Eugene Arnold, Andrea Chronis-Tuscano, Lily Hechtman, Stephen P. Hinshaw, Michael J. Kofler, Brooke S.G. Molina, Sébastien Normand, Linda J. Pfiffner and Amori Yee Mikami in Journal of Attention Disorders
Footnotes
Author Note
Other than the first author and the last (senior) author, all other authors are listed in alphabetical order.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Arnold has received research funding from Supernus Pharmaceuticals, Roche/Genentech Pharmaceuticals, Otsuka Pharmaceuticals, Axial, Yamo, and YoungLiving Essential Oils and National Institute of Health (USA, R01 MH 100144), has consulted with Pfizer Pharmaceuticals, Yamo, and CHADD, and been on advisory boards for Otsuka and Roche/Genentech.
Dr. Chronis-Tuscano receives research funding from NIH and book royalties from Oxford University Press.
Dr. Hechtman has a CIHR Grant and books which earn small royalties from Oxford U. Press, Guildford Press, and APA Press.
Dr. Hinshaw receives research funding from NIH and book royalties from Oxford U. Press, Guilford Press, Wiley, and St. Martin’s Press.
Dr. Molina receives NIH funding.
Dr. Normand receives research funding from CIHR and book royalties from Routledge.
Dr. Pfiffner receives research funding from NIH and IES.
Dr. Mikami receives research funding from CIHR and SSHRC and book royalties from Routledge.
Funding
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.