
Abstract
Objective:
Accumulating evidence indicates high rates of major depressive disorder (MDD) in children and adolescents with ADHD. This systematic review and meta-analysis aimed to examine the rate of depression in children and adolescents with ADHD who are without intellectual disability (ID).
Method:
A comprehensive search of six databases identified 20,745 studies. After screening based on inclusion and exclusion criteria, 24 studies were retained. A meta-analysis estimated the pooled depression rate in this population, and subgroup analyses examined differences based on sex, pubertal status, ADHD medication use, recruitment settings, depression assessment tools, informants, and risk of bias rating. Depression rates in children and adolescents with ADHD were compared with neurotypical peers in the retained case-control studies.
Results:
Depression rates in children and adolescents with ADHD across the included studies ranged from 1.7% to 60%, with the meta-analysis estimating a pooled depression rate of 11.31% (95% CI [0.07, 0.16]). Subgroup analyses indicated significant differences by sex, with females showing higher rates than males. Differences were also noted by assessment methods, with the highest rates observed when both questionnaires and interviews were used. While other factors did not significantly affect rates, notable trends were identified and reported in the current article.
Conclusion:
Depression is a common co-occurrent psychiatric condition in children and adolescents with ADHD, with rates observed in this review and meta-analysis being higher than those reported for neurotypical children and adolescents. This review underscores the importance of combining multiple assessment methods to capture a comprehensive picture of depression in this population, as well as ensuring balanced demographic representation. This review also suggests that further research should explore the depression developmental patterns in children and adolescents with ADHD and identify whether patterns are similar to the neurotypical population.
Introduction
ADHD is a neurodevelopmental disorder characterized by symptoms including excessive activities, difficulty staying still for long periods, and difficulties in cognitive function (American Psychiatric Association, 2013). ADHD affects over 5% of the pediatric population worldwide (Barkley, 2015; Polanczyk et al., 2014). Researchers, clinical practitioners, and those with lived experiences of ADHD increasingly emphasize the important influence of co-occurring mental health conditions on the health, well-being, and mortality rates of those with ADHD (Meinzer & Chronis-Tuscano, 2017; Thapar et al., 2023). It is estimated that about 55% to 65% of children and adolescents aged 4 to 15 years with ADHD are diagnosed with at least one psychiatric condition other than ADHD, and over 30% are diagnosed with two or more (Cuffe et al., 2020), markedly higher than observed in neurotypical young people (Patel et al., 2007). Among these co-occurring psychiatric conditions, depression is common in ADHD (Daviss, 2008; Meinzer et al., 2014).
Depression is a heterogeneous mood disorder, characterized by symptoms such as low mood or anhedonia, sleep disturbances, fatigue, weight loss/gain, cognitive difficulties, psychomotor changes, worthlessness, and suicidal ideation (American Psychiatric Association, 2013). In the neurotypical population, depression prevalence remains relatively low before early adolescence (Kessler et al., 2001; Maughan et al., 2013; Thapar et al., 2012); this prevalence steadily increases from early adolescence to approximately 6% during the middle to late stages of adolescence (Costello et al., 2006, 2011). The upward trend in depression prevalence accelerates significantly from middle to late adolescence in this population, with a considerable sixfold increase between 15 and 18 years old (Hankin & Abela, 2005; Hankin et al., 1998). Depression is recognized as a risk factor for maladaptive outcomes in the neurotypical population, including increased rates of substance abuse, suicide, intimate partner violence victimization, and a higher prevalence of mental health conditions (Johnson et al., 2018; McLeod et al., 2016). Co-occurring ADHD and depression can exacerbate challenges (Biederman et al., 2008; Meinzer et al., 2014). For instance, a literature review reported that adolescents with co-occurring ADHD and depression have a higher risk of long-term impairment in social functioning and suicide compared to those diagnosed with either condition alone (Daviss, 2008). Supporting this, Zahid et al. (2020) found that adolescents with co-occurring ADHD and major depressive disorder (MDD) had a 52.2% increased risk of suicide than those with MDD alone.
One systematic review has examined the prevalence of co-occurring psychiatric conditions in adults with ADHD, reporting a heterogeneity in the prevalence of depression, ranging from 8.6% to 55% (Choi et al., 2022). However, no systematic review has specifically focused on rates of depression in children and adolescents (≤18 years old) with ADHD. Co-occurring psychiatric conditions during childhood and adolescence may exacerbate ADHD symptoms, contribute to greater cognitive functioning difficulties, reduce the effectiveness of interventions and treatments, and result in a poorer overall prognosis for children and adolescents (Antshel et al., 2016; Ashwood et al., 2015). Thus, it is important to examine co-occurring depression rates in children and adolescents with ADHD (Hartman, 2023). Research has suggested that children and adolescents with ADHD may have different depressive characteristics than their neurotypical peers. Specifically, anhedonia, which refers to the loss of interest and pleasure in daily activities (American Psychiatric Association, 2013), emerges as the strongest predictor of depression in children and adolescents with ADHD (Babinski et al., 2019), whereas the most predictive symptom in neurotypical children and adolescents is low mood or irritability (Luby et al., 2009). Given these differences, understanding rates of co-occurring depression in children and adolescents with ADHD would be beneficial, especially for tailoring interventions and improving outcomes (Turgay & Ansari, 2006).
Various factors may influence depression rates in children and adolescents with ADHD. Similar to findings in the neurotypical population (e.g., Joinson et al., 2012; Stumper & Alloy, 2023), previous research has shown that adolescents with ADHD in the later stages of puberty have higher levels of depression compared to those at earlier stages (Eng et al., 2023). This suggests that variations in participants’ pubertal status may contribute to reported heterogeneity in depression rates. Another potential factor is sex. While some studies have reported no sex differences in depression among children and adolescents with ADHD (e.g., Lahey et al., 2007; Yoshimasu et al., 2012); others have shown that female adolescents and adults with ADHD have a significantly higher depression incidence compared to their male counterparts (e.g., Rucklidge, 2008; Solberg et al., 2018), consistent with findings observed in neurotypical populations (e.g., Salk et al., 2017; Shorey et al., 2022).
Empirical research findings on the impact of ADHD medications (e.g., methylphenidate [MPH]) on depression in children and adolescents with ADHD are mixed. Some research has found that the use of MPH can reduce the incidence of depression in children, adolescents, and adults with ADHD (Chang et al., 2016); while others indicate that children and adolescents with ADHD experienced increased levels of depression during MPH treatment (Oh et al., 2022). Thus, ADHD medication use is another important factor to consider when investigating depression rates in this population. Differences in recruitment pathways when investigating depression rates in ADHD may also contribute to heterogeneity reported in the literature. In comparison to those recruited through community pathways, children and adolescents with ADHD recruited through clinical pathways have been shown to experience more difficulties in interpersonal, self-actualization, and adaptive functioning (Bauermeister et al., 2007) and are more likely to present with co-occurring psychiatric conditions, including depression (Compas et al., 1997; Goodman et al., 1997).
The lack of psychometrically validated depression measurement tools specifically designed for children and adolescents with ADHD likely contributes to heterogeneity in depression rates reported in the literature. For example, the overlap between ADHD and depression symptoms (e.g., inattention and irritability) may cause children and adolescents with ADHD, as well as their parents, to inaccurately report elevated depression scores on scales originally designed and standardized for the neurotypical population (Davidsson et al., 2017; Lundervold et al., 2016). Moreover, some children and adolescents with ADHD may face working memory difficulties (Kanevski et al., 2023; Rhodes et al., 2012), which may affect their reading comprehension and interpretation of written language (Kofler et al., 2019). These challenges may introduce variability in how children and adolescents with ADHD interpret and respond to depression measures designed for the neurotypical population. Informant type for depression assessment may also influence reported depression rates, as relying solely on either children or parents may reflect differing perspectives and interpretations (De Los Reyes & Kazdin, 2005). For example, children with ADHD often report lower depression levels compared to their parents (Fraser et al., 2018). These potential differences suggest the need to consider informant type as a factor that contributes to heterogeneity in reported depression rates in the ADHD population.
It is vital to better understand rates of depression in ADHD as it can help shape healthcare policies, facilitate targeted interventions, and provide appropriate support services (Johansson et al., 2013; Williams et al., 2009); it can also contribute to advancing research on the co-occurrence of ADHD and depression (Meinzer et al., 2014). Despite this importance, there have been no systematic reviews and meta-analyses to date estimating rates of depression in children and adolescents with ADHD. This systematic review and meta-analysis aimed to identify rates of MDD in children and adolescents with ADHD, whether MDD is diagnosed clinically or identified through clinical cut-off scores on standardized questionnaires. This systematic review also aimed to examine whether rates differ by sex, pubertal status, ADHD medication use, recruitment methods, depression assessment tools, and informants for depression assessment. Based on these findings, the review made recommendations for future studies.
Methodology
Reporting
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). The protocol of this review was registered on PROSPERO (CRD42023418062).
Search Strategy
Common synonyms and medical subject headings (MESH) for keywords were developed and adapted from previous systematic reviews on “depression” (Lima et al., 2013; Stewart et al., 2022), “ADHD” (Eaton et al., 2023; McDougal et al., 2022), and “children/adolescents” (Eaton et al., 2023; Stewart et al., 2022; Vacher et al., 2020). Search keywords are detailed in Table 1. Multiple keywords from different categories are combined using the Boolean operator “AND,” and multiple keywords from the same category are connected using the Boolean operator “OR” (Sayers, 2008).
Keywords and Combinations Used in the Search Strategy.
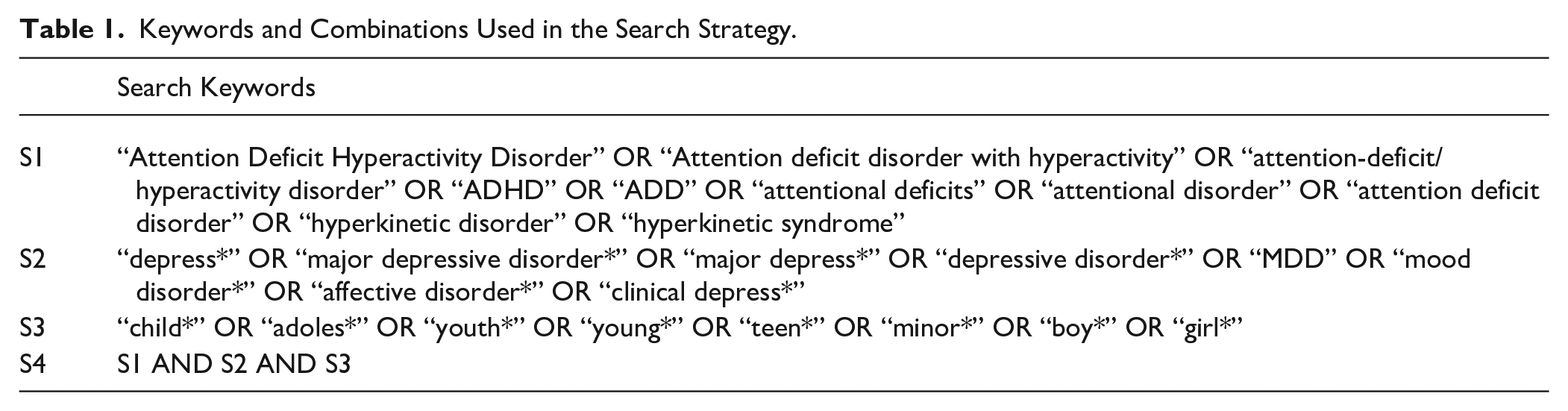
The keywords shown in Table 1 were used to search in six databases, including EMBASE, ERIC, PsycINFO, CINAHL, MEDLINE, and Web of Science. The search included research from 1992 to August 2023 based on the ADHD diagnostic criteria of the International Classification of Diseases 10th Revision (ICD-10) and later versions (e.g., ICD-11), or studies from 1994 to August 2023 based on the ADHD diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) and its subsequent versions (e.g., DSM-IV-TR and DSM-5). ICD-10, published in 1992, was the first to divide ADHD subtype diagnoses, including inattentive, hyperactive-impulsive, and combined type (World Health Organization, 1992); while DSM-IV, published in 1994, adopted nearly identical criteria to classify these ADHD subtypes (American Psychiatric Association, 1994). The search was conducted on 31st August 2023 and focused exclusively on studies involving human participants that were published in peer-reviewed journals in English. Any duplicate records found during the search were removed from the results of included studies.
Selection, Inclusion, and Exclusion
This systematic review included empirical studies involving children and adolescents ≤18 years old (i.e., studies with some participants over 18 years were retained if the mean sample age was ≤18). Inclusion criteria required that ADHD be clinically diagnosed according to the DSM-IV (or DSM-IV-TR/DSM-5) or ICD-10 (or ICD-11) criteria, or confirmed using a validated diagnostic tool (e.g., Kindle Schedule for Affective Disorders and Schizophrenia for School-Age Children [K-SADS]); Studies were eligible for inclusion if they utilized a specific depression measure, a depression subscale within a generic instrument, or assessed depression based on DSM or ICD. This review focused exclusively on children and adolescents with ADHD but without Intellectual Disability (ID) to minimize the potential confounding effects of low IQ on rates of depression. This focus was chosen because there is evidence that depression severity differs between children and adolescents who have both ADHD and ID and those with ADHD but without ID, with children and adolescents with co-occurring ADHD and ID tending to report higher levels of depression (Ahuja et al., 2013; Pearson et al., 2000). In this review, participants were defined as having no ID if they had a full-scale IQ (FSIQ) of 70 or higher (American Psychiatric Association, 2013).
Studies that did not meet the inclusion criteria were excluded. Specifically, studies were excluded if the mean age of participants exceeds 18 years, if ADHD was diagnosed using criteria predating DSM-IV/ICD-10, if only screening tools (e.g., ADHD Rating Scale [ARS] and Turgay DSM-IV Disruptive Behavior Disorders Rating Scale-Teacher and Parent Forms [T-DSM-IV-S]) were used, or if the ADHD diagnostic procedure was not reported. Additionally, studies focusing on sub-clinical depression (i.e., below the clinical threshold) or examining the lifetime rates of depression, rather than current rates, were also excluded. Theses, systematic reviews, meta-analyses, literature reviews, book chapters, or conference proceedings/abstracts were also excluded. Intervention studies were excluded, as were longitudinal studies that did not provide baseline or follow-up depression assessment data in participants. Studies were also excluded if they employed measures that did not assess depression separately. For example, if a study employed a scale that measured internalizing symptoms, that is a joint measure of depression and anxiety without reporting the two separately, it was excluded.
The first author (S.W.) searched for articles in six databases based on the keywords in Table 1. According to the inclusion and exclusion criteria, S.W. independently screened the titles and abstracts of the retrieved articles. To ensure reliability, the second and third reviewers (I.O. and A.M.) independently screened 10% of the articles (5% each). The agreement rate at this stage was 96%. Following this, S.W. independently conducted a full-text screening of articles that passed the title and abstract screening stages according to the inclusion and exclusion criteria. The second and third reviewers (I.O. and A.M.) also independently screened 10% of these articles (5% each). The agreement rate was 92.5% at this stage. These agreement rates exceed the acceptable threshold of 80% reported in the literature (Belur et al., 2018). Differences at all stages of the screening process were resolved through discussion until a 100% consensus was reached. When final decisions remained unclear, two co-authors (T.S. and S.R.) were consulted for further clarification. To capture any relevant studies that might have been missed, a backward citation search was also conducted by reviewing the reference lists of studies included after the full-text screening; however, this search yielded no additional results. Figure 1 outlines the entire selection process.
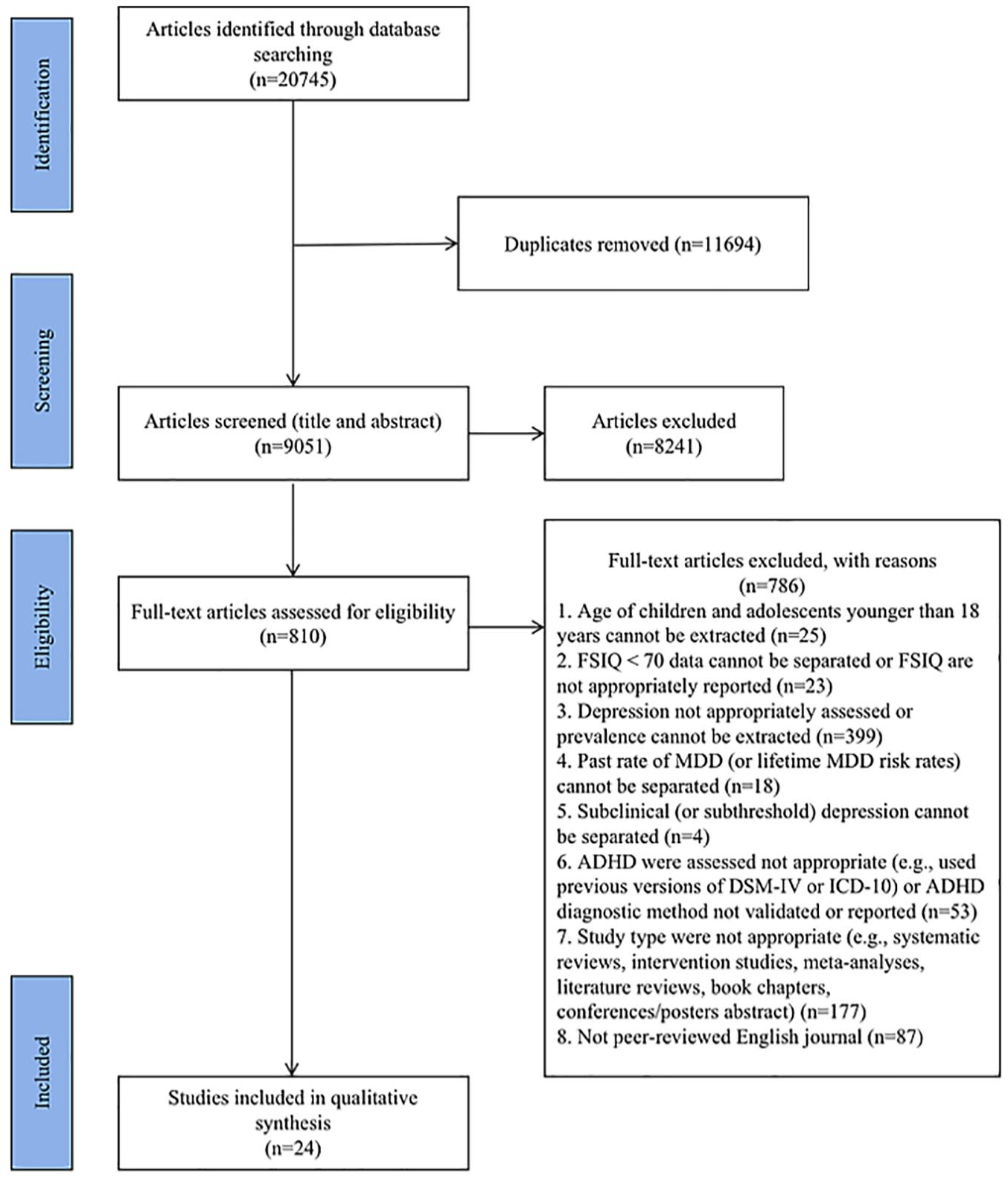
Flow chart of search strategy for this systematic review based on PRISMA.
Data Extraction and Quality Assessment
Data were extracted from the included studies based on a customized data collection form from the Cochrane Handbook (Higgins & Thomas, 2023), the section related to intervention studies was removed from the original form and a new section on the rate of depression was added. Three reviewers extracted all data independently, with S.W. extracting data from all included studies and I.O. and A.M. each completing 5% of the data extraction (a total of 10%). The data extracted included: (1) Key study details (e.g., first author and publication year); (2) Study country; (3) Study type or design (e.g., cross-sectional and longitudinal); (4) Recruitment pathways (e.g., clinical and community); (5) Sample size of children and adolescents with ADHD (including participants’ sex distribution); (6) Participant age (mean, standard deviation [SD], and range); (7) Full-Scale IQ (FSIQ) of participants (mean, SD, and range, and the tool used for assessment); (8) Participant medication status; (9) Other demographic information (e.g., SES and ethnicity); (10) Name and type of standard used to diagnose ADHD; (11) Name and type of measure used to assess depressive symptoms; and (12) Rates of clinical cut-off range depression or MDD. Depression rates (expressed as a percentage) were calculated by dividing the number of participants with co-occurring ADHD and depression by the total ADHD sample size. For case-control studies, data on the neurotypical group, including sample size, sex distribution, and depression rates, were also extracted. Depression rates in neurotypical children and adolescents were similarly calculated by dividing the number of neurotypical participants with depression by their total sample sizes. There was 95% to 100% agreement across both extractions. Differences were resolved through discussion until a 100% consensus was reached. Information that was missing in the included studies was noted as not reported (NR).
This review evaluated the risk of bias—defined as a systematic error or deviation from the truth in results (Higgins & Thomas, 2023)—in included studies based on the validated risk of bias assessment instrument, the Checklist for Prevalence Studies, developed by Munn et al. (2014). This instrument was developed to evaluate the risk of bias in prevalence studies across a range of disorders and evaluate the internal and external validity of prevalence data from different study designs (Munn et al., 2014). The bias rating chart utilized in this systematic review (see Table 2) was adapted from quality assessment criteria employed in similar topic-focused systematic reviews that examined depression rates in children and adolescents with Autistic Spectrum Disorders (ASD) but without ID (Stewart et al., 2022; Wigham et al., 2017) and ADHD prevalence in children and adolescents with ASD but without ID (Eaton et al., 2023). The first author (S.W.) conducted the quality assessment of the included studies independently. To ensure consistency in this stage, 10% of the studies were also evaluated by I.O. and A.M. (each assessing 5%). There was 100% agreement. No studies were excluded due to the high risk of bias ratings.
Bias Rating Chart.
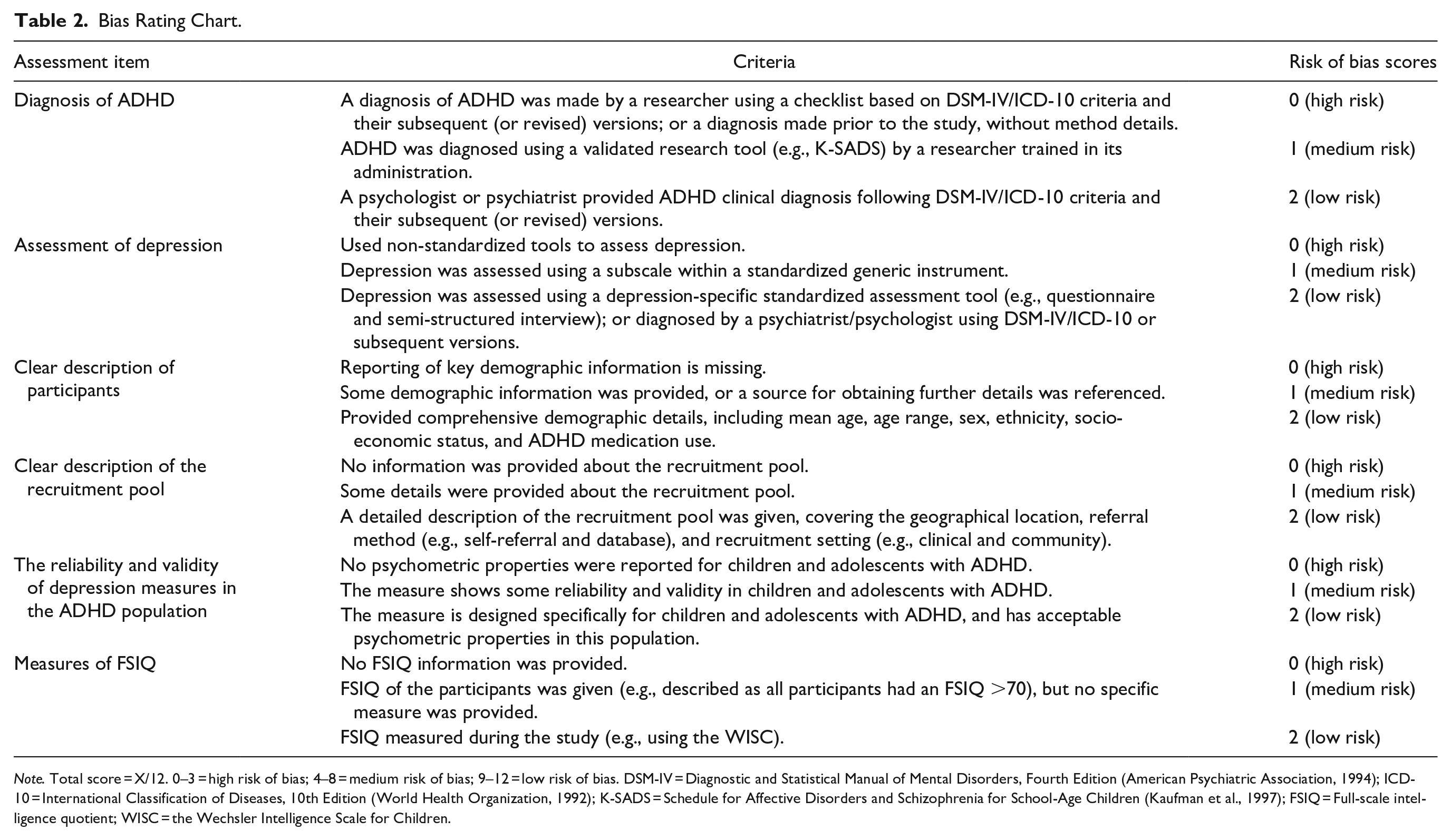
Note. Total score = X/12. 0–3 = high risk of bias; 4–8 = medium risk of bias; 9–12 = low risk of bias. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (American Psychiatric Association, 1994); ICD-10 = International Classification of Diseases, 10th Edition (World Health Organization, 1992); K-SADS = Schedule for Affective Disorders and Schizophrenia for School-Age Children (Kaufman et al., 1997); FSIQ = Full-scale intelligence quotient; WISC = the Wechsler Intelligence Scale for Children.
Data Analysis
This systematic review combined meta-analysis and narrative synthesis to comprehensively examine depression rates in children and adolescents with ADHD. The meta-analysis quantified the pooled depression rate and explored factors contributing to heterogeneity across studies (Barendregt et al., 2013; Higgins & Thomas, 2023). Studies that could not be included in the meta-analysis, such as those lacking sufficient data for statistical analysis, reporting information in incompatible formats, or using non-comparable outcome measures, were synthesized narratively to ensure their findings contributed to the broader understanding of the topic.
The meta-analysis was conducted using R (version 4.4.2 with the meta package; Balduzzi et al., 2019; Schwarzer et al., 2015). A generic inverse-variance method with a random effect model was used (DerSimonian & Laird, 1986), as it accounts for variability between studies due to differences in populations, settings, assessment methods, and methodological quality. This approach also provides a high conservation null hypothesis (Han & Eskin, 2011; Higgins & Thomas, 2023). Freeman-Tukey double arcsine transformation of rate to stabilize the variance was used, which is a reliable and robust option to deal with the instability of variance of a proportion in the meta-analysis, especially for studies with extreme rate estimates (Doi & Xu, 2021; Freeman & Tukey, 1950). The pooled rate estimate with 95% confidence intervals (CI) was presented in a forest plot. Heterogeneity was assessed using Cochran’s Q test (χ2, statistic significant: p < .05) and I2 statistic (substantial heterogeneity: I2 > 50%; Higgins & Thomas, 2023
The narrative synthesis was conducted following the guidance from the Economic and Social Research Council (ESRC) Methods Program, ensuring the results’ robustness and transparency. According to this narrative synthesis guidance, this systematic narrative synthesis was based on the framework of Figure 2 (Popay et al., 2006).
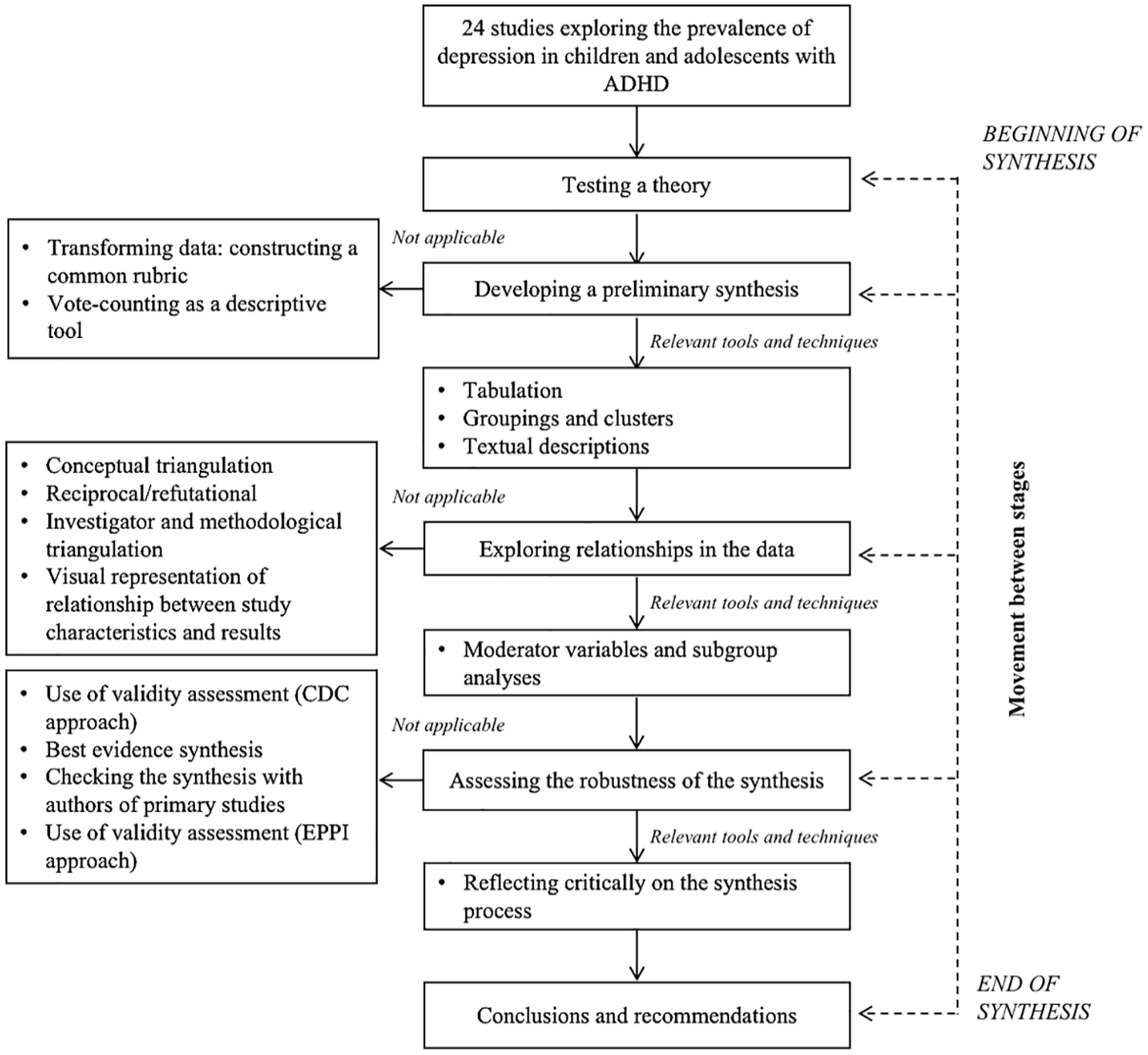
Systematic narrative synthesis framework.
Results
Description of Included Studies
A total of 24 studies were included in this review, and their detailed characteristics are summarized in Table 3. Altogether, 6,815 participants were included in this review, consisting of 4,991 (73.24%) males and 1,824 (26.76%) females (excluding data from Sumiła & Cieślukowska, 2008, which did not provide subsample details—see Table 3). Among these participants, 5,047 were children and adolescents with ADHD, of whom 3,862 (76.52%) were male and 1,185 (23.48%) were female, with the distribution of male participants with ADHD ranging from 56.7% (Zerón-Rugerio et al., 2021) to 90.5% (Byun et al., 2006). ADHD sample sizes varied from 18 (Breaux et al., 2022) to 1000 (Inci et al., 2019), with participants’ ages spanning from 5 to 19 years old (Sumiła & Cieślukowska, 2008). Although this upper age limit exceeds the review’s criteria of 18 years or younger, Sumiła and Cieślukowska (2008) reported a mean sample age of 12.57 years, which is ≤18 years and therefore, they were retained. Three studies were also retained because they reported an average age of ≤18 years, despite not reporting a range of ages (Cleminshaw et al., 2020; Di Trani et al., 2014; S. Park et al., 2013).
Demographic and Recruitment Pool Details, ADHD and Depression Assessment Methods, and Rates of Depression in the Studies Reviewed (n = 24).
Note. ID = intellectual disability; M = mean; SD = standard deviation; FSIQ = full-scale intelligence quotient; MDD = major depressive disorder; NR = not reported; ARS-IV = ADHD Rating Scale, Fourth Edition (DuPaul et al., 1998; Italian Version: Marzocchi & Cornoldi, 2000; Korean Version: So et al., 2002); ARS-5 = ADHD Rating Scale 5 Home Version (DuPaul et al., 2016); CBCL = Child Behavior Checklist (Achenbach & Rescorla, 2001); CDI = Children’s Depression Inventory (Kovacs, 1985; Turkey version: Öy, 1991; Korean version: Cho & Lee, 1990); ChIPS/P-ChIPS = Children’s Interview for Psychiatric Syndromes (Weller et al., 2000)/Children’s Interview for Psychiatric Syndromes-Parent Version (Weller et al., 1999); CPRS/CTRS-RS/CPRS-R:S = Conners Parent Rating Scale (Kao & Thomas, 2010)/Conners’ Teacher Rating Scale-Revised Short Version (C. K. Conners et al., 1998; Turkish Version: Kaner et al., 2013)/Conners’ Parent Rating Scale–Revised: Short Form (C. K. Conners, 1997); DISC-IV = Diagnostic Interview Schedule for Children, Version IV (Shaffer et al., 2000); DSM-IV/DSM-IV-TR/DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (American Psychiatric Association, 1994)/Fourth Edition, Text Revision (American Psychiatric Association, 2000)/Fifth Edition (American Psychiatric Association, 2013); DSRSC = Depression Self-Rating Scale for Children (Birleson, 1981); ICD-10 = International Classification of Diseases, 10th Edition (World Health Organization, 1992); KEDI-WISC = Korean Educational Developmental Institute’s Wechsler Intelligence Scale for Children (K. S. Park et al., 1996); K-SADS = Schedule for Affective Disorders and Schizophrenia for School-Age Children (Kaufman et al., 1997; Farsi version: Ghanizadeh et al., 2006); Chinese K-SADS-E = Schedule for Affective Disorders and Schizophrenia for School-Age Children Epidemiologic version Chinese Version (S.-F. Gau & Suen Soong, 1999); K-SADS-P-IVR = Schedule for Affective Disorders and Schizophrenia for School-Age Children Present State version IV-Revised; K-SADS-PL = Schedule for Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime version (Kaufman et al., 1997; Turkish version: Gökler et al., 2004; Korean Version: Kim et al., 2004; Spanish version: Ulloa et al., 2006); RADS-2 = Reynolds Adolescent Depression Scale, Second Edition (Reynolds, 2004); RCADS = Revised Child’s Anxiety and Depression Scale (Chorpita et al., 2000); SNAP-IV = Swanson, Nolan, and Pelham Teacher and Parent Rating Scale (J. M. Swanson, 1992); SWAN = Strengths and Weaknesses of ADHD Symptoms and Normal Behaviors (J. Swanson et al., 2001); T-DSM-IV-S = Turgay DSM-IV Disruptive Behavior Disorders Rating Scale—Teacher and Parent Form (Turgay, 1994); VADPRS/VADTRS = Vanderbilt ADHD Diagnostic Parent/Teacher Rating Scale (Wolraich et al., 1998, 2003); VADRS-P/C = Vanderbilt ADHD Diagnostic Rating Scale—Parent/Child (Wolraich et al., 2003);WAIS-III = The Wechsler Adult Intelligence Scale, Third Edition (Wechsler, 1997); WASI-II = Wechsler Abbreviated Scale of Intelligence Second Edition (Wechsler, 2011); WISC-III/IV/R = The Wechsler Intelligence Scale for Children, third Edition (Wechsler, 1991; Turkey version: Orsini & Picone, 2006)/fourth Edition /Revised Turkish Version (Savaşır & Sahin, 1995).
This review included a diverse range of study designs: cross-sectional designs (Ambrosini et al., 2013; Breaux et al., 2022; Byun et al., 2006; Cleminshaw et al., 2020; Di Trani et al., 2014; Elia et al., 2009; Ghanizadeh, 2008; Inci et al., 2019; Ipci et al., 2020; Işık et al., 2018; Mitchison & Njardvik, 2019; Nadeau et al., 2015; Sumiła & Cieślukowska, 2008; Suthar et al., 2018; Yüce et al., 2013), longitudinal designs (S. S.-F. Gau, Lin, et al., 2010), and case-control studies (Ahmed et al., 2021; S. S.-F. Gau, Ni, et al., 2010; Hurtig et al., 2007; Joseph et al., 2019; Palacio-Ortiz et al., 2018; S. Park et al., 2013; Xia et al., 2015; Zerón-Rugerio et al., 2021).
Six studies reported participants’ ethnicity (Ambrosini et al., 2013; Breaux et al., 2022; Cleminshaw et al., 2020; Di Trani et al., 2014; Elia et al., 2009; Nadeau et al., 2015). The ADHD medication use of participants was reported by 10 studies (Ahmed et al., 2021; Breaux et al., 2022; Cleminshaw et al., 2020; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Işık et al., 2018; Joseph et al., 2019; Nadeau et al., 2015; Palacio-Ortiz et al., 2018; Zerón-Rugerio et al., 2021).
All studies reported participants’ FSIQ≥70, although 13 studies did not report the IQ measure used (Ambrosini et al., 2013; Byun et al., 2006; S. S.-F. Gau, Lin, et al., 2010; Ghanizadeh, 2008; Inci et al., 2019; Ipci et al., 2020; Joseph et al., 2019; Nadeau et al., 2015; Sumiła & Cieślukowska, 2008; Suthar et al., 2018; Yüce et al., 2013; Xia et al., 2015; Zerón-Rugerio et al., 2021). Two studies reported a higher threshold, with an FSIQ of 80 or above (S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010). Fourteen studies reported socioeconomic status (SES); eight provided data on parental income (Breaux et al., 2022; Cleminshaw et al., 2020; Di Trani et al., 2014; Elia et al., 2009; Hurtig et al., 2007; Nadeau et al., 2015; Palacio-Ortiz et al., 2018; Suthar et al., 2018), three reported parents’ education or occupation (S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Ghanizadeh, 2008), and three included both parents’ education or occupation and income (Ipci et al., 2020; Joseph et al., 2019; Xia et al., 2015).
In this review, included studies were conducted across various regions, with most published in Asia (n = 6), including three studies in China (including Taiwan; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Xia et al., 2015), two in South Korea (Byun et al., 2006; S. Park et al., 2013), and one in India (Suthar et al., 2018). The Middle East had five studies, including four conducted in Turkey (Inci et al., 2019; Ipci et al., 2020; Işık et al., 2018; Yüce et al., 2013) and one in Iran (Ghanizadeh, 2008). North America was represented by five studies from the United States (Ambrosini et al., 2013; Breaux et al., 2022; Cleminshaw et al., 2020; Elia et al., 2009; Nadeau et al., 2015). Europe contributed five studies, with one each from Italy (Di Trani et al., 2014), Finland (Hurtig et al., 2007), Iceland (Mitchison & Njardvik, 2019), Poland (Sumiła & Cieślukowska, 2008), and Spain (Zerón-Rugerio et al., 2021). Other regions included Australia in Oceania (Joseph et al., 2019), Colombia in South America (Palacio-Ortiz et al., 2018), and Egypt in Africa (Ahmed et al., 2021), each represented by a single study.
Measures of Depression
In this review, the included studies assessed depression in children and adolescents with ADHD using various methods (see Table 3), mainly interviews and questionnaires. Some included studies combined both methods: Suthar et al. (2018) employed senior psychiatrists to conduct interviews with children based on DSM-IV-TR, while depression ratings were also collected from parents and teachers using the Vanderbilt ADHD Diagnostic Parent/Teacher Rating Scale (VADPRS/VADTRS); Xia et al. (2015) involved senior psychiatrists interviewing children and their parents using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) while children self-reported depression scores via the Depression Self Rating Scale for Children (DSRSC).
Thirteen studies assessed depression through interviews, predominantly using the K-SADS and its different adaptations. The K-SADS is a semi-structured interview developed to evaluate present and past symptoms of affective and psychotic disorders (e.g., MDD, anxiety, ADHD, conduct disorder, and schizophrenia) in children and adolescents aged 6 to 18 years, and diagnoses are typically determined according to a combination of interview data obtained from the child and their parents (Kaufman et al., 1997). Among these 13 studies using the K-SADS, 9 explicitly reported interviewing both parents and children (Byun et al., 2006; Di Trani et al., 2014; Elia et al., 2009; S. S.-F. Gau, Lin, et al., 2010; S.S.-F. Gau, Ni, et al., 2010; Ghanizadeh, 2008; Hurtig et al., 2007; Xia et al., 2015; Yüce et al., 2013); one seemed to indicate that only children and adolescents were interviewed (i.e., “. . .The children and adolescents were first interviewed using the K-SADS-PL,” Inci et al., 2019, p. 1358); and three studies did not specify whether the interview was conducted with the child, the parent/guardian, or both (Ambrosini et al., 2013; Ipci et al., 2020; Zerón-Rugerio et al., 2021). For these three studies, this review assumes interviews included both the child and parent/guardian, which followed the interpretation of K-SADS in line with Kaufman et al. (1997), but caution should be given here. Of the 13 studies using the K-SADS, 10 employed interviews conducted by clinicians or psychiatrists (Ambrosini et al., 2013; Byun et al., 2006; Di Trani et al., 2014; Elia et al., 2009; Ghanizadeh, 2008; Inci et al., 2019; Ipci et al., 2020; Xia et al., 2015; Yüce et al., 2013; Zerón-Rugerio et al., 2021), while three used researcher or trained student research assistants (S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Hurtig et al., 2007). Two additional studies conducted interviews with both children/adolescents and parents, administered by psychiatrists and clinicians, but did not specify the tools used, only mentioning that they followed DSM-5 or ICD-10 criteria (Palacio-Ortiz et al., 2018; Sumiła & Cieślukowska, 2008). Another study conducted interviews with children, administered by senior psychiatrists, but only reported that these were based on DSM-IV-TR without specifying the tool used (Suthar et al., 2018). One study interviewed parents and children using the Children’s Interview for Psychiatric Syndromes (ChIPS), administered by researchers (Breaux et al., 2022). Another study interviewed parents using the Diagnostic Interview Schedule for Children, Version IV (DISC-IV), conducted by trained research assistants (Joseph et al., 2019).
Six studies used clinical cut-off scores from questionnaires to assess children and adolescents’ depression: one study reported by parents using the Child Behavior Checklist (CBCL; Ahmed et al., 2021); while the other five studies relied on child/adolescent self-report questionnaires, including the Reynolds Adolescent Depression Scale, Second Edition (RADS-2; Cleminshaw et al., 2020), the Children’s Depression Inventory (CDI; Işık et al., 2018; Mitchison & Njardvik, 2019; S. Park et al., 2013), and the Revised Child’s Anxiety and Depression Scale (RCADS; Nadeau et al., 2015).
Measures of ADHD
The included studies utilized a range of approaches to assess ADHD (see Table 3), including prior diagnoses without further confirmation, prior diagnoses with confirmation in the study, ADHD diagnoses made in the study based on the DSM/ICD, and ADHD diagnoses in the study further validated by multiple sources.
Two studies relied solely on prior ADHD diagnoses; Ambrosini et al. (2013) did not report specific details, while Sumiła and Cieślukowska (2008) reported that ADHD was diagnosed based on ICD-10. Six studies confirmed prior clinical diagnoses using the K-SADS to interview both children and their parents (Byun et al., 2006; Elia et al., 2009; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Ghanizadeh, 2008; Yüce et al., 2013). Four studies used parent- and/or teacher-reported questionnaires to confirm prior ADHD diagnoses: Ahmed et al. (2021) employed the Conners Parent Rating Scale (CPRS); Di Trani et al. (2014) used the ARS-IV reported by both parents and teachers; Nadeau et al. (2015) used the Vanderbilt ADHD Diagnostic Rating Scale-Parent/Child (VADRS-P/C) reported by children and parents; and S. Park et al. (2013) utilized the ARS-IV reported by parents. Five studies confirmed prior diagnoses with a combination of parent and/or teacher reported questionnaires (i.e., ARS, Conners’ Teacher Rating Scale-Revised Short [CTRS-RS], and T-DSM-IV-S) and interviews using the K-SADS (Inci et al., 2019; Ipci et al., 2020; Işık et al., 2018; Mitchison & Njardvik, 2019; Zerón-Rugerio et al., 2021).
One study, Palacio-Ortiz et al. (2018), diagnosed ADHD during the study using DSM-5 criteria by child psychiatrists. Six studies involved ADHD diagnoses made during the study using multiple sources: Breaux et al. (2022) diagnosed ADHD through clinicians and confirmed it using ChIPS interviews with parents alongside parent and teacher reports on the VADPRS/VADTRS; Cleminshaw et al. (2020) assessed ADHD with parent-reported ARS-5 scores, confirmed through ChIPS interviews with parents conducted by trained research assistants; Hurtig et al. (2007) collected parent-reported Strengths and Weakness of ADHD symptoms and Normal Behaviors (SWAN) ratings and confirmed ADHD through K-SADS-PL interviews with parents and children/adolescents administered by psychiatrists; Joseph et al. (2019) gathered ADHD symptoms using the 10-item Conner 3 ADHD Index from parents and teachers, confirmed through DISC-IV interviews with parents conducted by trained psychologists; Suthar et al. (2018) collected ADHD data via parent and teacher VADPRS/VADTRS reports and confirmed diagnoses using DSM-IV-TR-based interviews conducted by senior psychiatrists; and Xia et al. (2015) collected ADHD symptom ratings from parents using Swanson, Nolan, and Pelham Teacher and Parent Rating Scale (SNAP-IV) and a psychiatrist conducted K-SADS-PL interviews with children and parents to confirm ADHD.
Quality Appraisal
Of these 24 included studies, 8 demonstrated a low overall risk of bias (Breaux et al., 2022; Cleminshaw et al., 2020; Işık et al., 2018; Mitchison & Njardvik, 2019; Nadeau et al., 2015; Palacio-Ortiz et al., 2018; S. Park et al., 2013; Suthar et al., 2018), while the remaining 16 had a medium overall risk of bias. None of the studies had a high overall risk of bias. Table 4 presents a detailed summary of the quality assessment results, including the risk of bias ratings for each item and the overall rating of the included studies.
Results of the Quality Assessment.
Note. FSIQ = full-scale IQ.
In terms of ADHD diagnosis, 20 were considered to have a low risk of bias. In these studies, ADHD was diagnosed by clinicians following DSM/ICD criteria, with further confirmation provided by a validated standardized research tool (e.g., ChIPS and K-SADS). Three studies were considered to be at medium risk in this item as they solely relied on validated tools (e.g., DISC-IV, K-SADS, and PChIPS) to diagnose ADHD without clinicians’ involvement (Cleminshaw et al., 2020; Hurtig et al., 2007; Joseph et al., 2019). One study was assessed as high risk as participants’ ADHD were diagnosed before the study but did not provide detailed information about the methodology (Ambrosini et al., 2013).
Regarding the assessment of depression, 16 studies were classified as having a medium risk due to the use of depression subscales from standardized universal measures; the remaining 8 were considered as low-risk as they used standardized assessment tools (or clinical interviews) specifically designed to assess depression, or a diagnosis made by clinicians or researchers based on DSM/ICD (Cleminshaw et al., 2020; Işık et al., 2018; Mitchison & Njardvik, 2019; Palacio-Ortiz et al., 2018; S. Park et al., 2013; Sumiła & Cieślukowska, 2008; Suthar et al., 2018; Xia et al., 2015).
Regarding the clear description of participants, three studies were considered to have a low risk of bias because they provided detailed information on key demographic characteristics, including mage age and age range, sex distribution, medication use, SES, and ethnicity (Breaux et al., 2022; Cleminshaw et al., 2020; Nadeau et al., 2015); the other 21 studies were assessed as medium risk due to incomplete or missing demographic information.
In the item “Clear description of the recruitment pool,” 18 studies adequately reported referral methods and study settings and were therefore rated low risk. Transparency in recruitment methods is an important aspect of methodological quality, as it enables researchers to better evaluate the potential generalizability of the findings (Munn et al., 2014). In contrast, the remaining six provided only partial details on these aspects and were thus rated medium risk of bias (Di Trani et al., 2014; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Hurtig et al., 2007; Ipci et al., 2020; Sumiła & Cieślukowska, 2008).
Regarding the item “The reliability and validity of depression measures in the ADHD population,” 20 were assessed as having a high risk of bias as depression measures in these studies did not show any psychometric properties evidence in the ADHD population. Four were classified as medium risk of bias in this item: two studies used depression assessment questionnaires that showed acceptable reliability and validity in children and adolescents with ADHD (Nadeau et al., 2015; Suthar et al., 2018); the other two involved direct depression diagnoses by psychiatrists according to DSM-5/ICD-10 (Palacio-Ortiz et al., 2018; Sumiła & Cieślukowska, 2008).
Eleven of the 24 studies were considered to be at low risk in measures of full-scale IQ (FSIQ) because they provided FSIQ data and reported on the validated FSIQ assessment tools they used (Ahmed et al., 2021; Breaux et al., 2022; Cleminshaw et al., 2020; Di Trani et al., 2014; Elia et al., 2009; S. S.-F. Gau, Ni, et al., 2010; Hurtig et al., 2007; Işık et al., 2018; Mitchison & Njardvik, 2019; Palacio-Ortiz et al., 2018; S. Park et al., 2013). The other 13 studies were classified as having a medium risk of bias in this item because they did not report the specific tools used to measure FSIQ.
Rates of Depression in ADHD
The reported rates of depression among children and adolescents with ADHD in the included studies varied widely, ranging from 1.7% to 60%. Using a random-effects model, the pooled estimated rate of depression was 11.31% (95% CI [0.07, 0.16]; I2 = 91%, τ2 = .03), as illustrated in the forest plot in Figure 3. To examine the robustness of this pooled estimate, a sensitivity analysis was conducted by using the leave-one-out approach, whereby excluding each study one-by-one from the analysis (Suvorov et al., 2023). The pooled rate remained stable, which varied between 10% (95% CI [0.07, 0.13]), with Ahmed et al. (2021) excluded, to 12% (95% CI [0.07, 0.17]), with Zerón-Rugerio et al. (2021) excluded. This indicated that no single study disproportionately influenced the pooled rate.
Forest plot of rates of depression of depression in children and adolescents with ADHD.
Rates by Measure Used to Assess Depression
The included studies employed various methods to assess depression in children and adolescents with ADHD, including interviews, questionnaires, or a combination of both. A subgroup analysis indicated significant differences in rates based on depression assessment methods (χ²(2) = 8.89, p < .05). Due to some depression measures having been used only in a single study (e.g., CBCL, ChIPS, RCADS, and DISC-IV), a subgroup analysis for specific measures was not conducted.
Studies employing mixed methods (combining questionnaires and interviews conducted by clinicians) reported the highest pooled rate of 20.87% (95% CI [0, 0.82]). Specifically, Suthar et al. (2018) employed VADPRS/VADTRS alongside DSM-IV-TR-based interview, reporting a rate of 26.30% (95% CI [0.16, 0.40]); and Xia et al. (2015) combined the DSRSC with the K-SADS-PL, reporting a rate of 17.8% (95% CI [0.12, 0.25]).
Studies using questionnaires reported a pooled depression rate of 16.13% (95% CI [0.02, 0.39]). Studies using versions of the CDI (n = 3) reported a total rate of 9.8% (95% CI [0, 0.41]; Işık et al., 2018; Mitchison & Njardvik, 2019; S. Park et al., 2013). Other tools included the CBCL, which reported a rate of 60% (95% CI [0.47, 0.72]; Ahmed et al., 2021); the RADS-2, with a rate of 12% (95% CI [0.23, 0.68]; Cleminshaw et al., 2020); and the RCADS, with a rate of 9% (95% CI [0.04, 0.16]; Nadeau et al., 2015).
Studies using interviews (n = 16) reported the lowest pooled rate (8.43%, 95% CI [0.05, 0.13]). Twelve studies using the K-SADS and its adaptations reported a total rate of 7.39% (95% CI [0.05, 0.10]; Ambrosini et al., 2013; Byun et al., 2006; Di Trani et al., 2014; Elia et al., 2009; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Ghanizadeh, 2008; Hurtig et al., 2007; Inci et al., 2019; Ipci et al., 2020; Yüce et al., 2013; Zerón-Rugerio et al., 2021). Other interviews included the ChIPS (44.4%, 95% CI [0.23, 0.68]; Breaux et al., 2022); the DISC-IV (2%, 95% CI [0, 0.05]; Joseph et al., 2019); the DSM-5-based interview (15.4%, 95% CI [0.11, 0.21]; Palacio-Ortiz et al., 2018); and the ICD-10-based interview (27.4%, 95% CI [0.17, 0.40]; Sumiła & Cieślukowska, 2008). A subgroup analysis of these studies using interviews, categorized by administrators (clinicians vs. researchers), found no significant difference in depression rates (χ²(1) = 0.28, p = .60). The pooled rate was 8.01% (95% CI [0.04, 0.13]) for interviews conducted by clinicians/psychiatrists and 10.63% (95% CI [0.002, 0.31]) for those administered by trained researchers/research assistants.
Rates by Type of Informant
The included studies utilized various informants to assess depression in ADHD, including parent, child/adolescent, both parent and child/adolescent, and a combination of parent, child/adolescent, and teacher. Subgroup analysis indicated no significant differences in depression rates based on informant type (χ²(2) = 0.31, p = .86). The pooled depression rate was lowest in studies relying solely on children/adolescents as informants, at 9.52% (95% CI [0.04, 0.17]). Studies in which both parent and child/adolescent as informants reported a pooled rate of 9.73% (95% CI [0.06, 0.15]). The highest pooled rate of 24.37% (95% CI [0, 1]) was observed in studies using the parent as the sole informant. No comparison was conducted for the study incorporating teacher reports, as only one study (i.e., Suthar et al., 2018) met this criterion, reported a rate of 26.3% (95% CI [0.16, 0.39]).
Rates by Risk of Bias Rating
Subgroup analysis based on overall risk of bias ratings found no significant differences in depression rates between studies (χ²(1) = 1.06, p = 0.30). Studies with a medium overall risk of bias reported a pooled rate of depression of 9.85% (95% CI [0.05, 0.16]); while those with a low overall risk of bias had a slightly higher rate of 14.5% (95% CI [0.06, 0.25]).
Among other risk of bias items, most studies were rated as low or medium risk. However, the item assessing “the reliability and validity of depression measures specific to the ADHD population” showed a different rating pattern as no study was rated as low risk, and 20 studies were rated as high risk. To explore the potential impact of this imbalance, a subgroup analysis was conducted based on the rating of this item and indicated no significant differences between groups (χ²(1) = 2.75, p = .09). Studies rated as medium risk of this item had a higher pooled depression rate (18.22%, 95% CI [0.06, 0.35]) compared to those rated as high risk (10.1%, 95% CI [0.06, 0.16]).
Rates by Pubertal Status
According to the National Health Service (NHS), the typical onset of puberty occurs at around age 11 for girls and age 12 for boys (NHS, 2022). Based on this guidance, included studies were categorized into those focusing on estimated pre-pubertal children (mean age ≤12) and estimated post-pubertal adolescents (mean age >12). Subgroup analysis showed a higher estimated depression rate in the post-pubertal group (15.06%, 95% CI [0.05, 0.29]) compared to the pre-pubertal group (9.91%, 95% CI [0.05, 0.16]), although the difference was not significant (χ²(1) = 1.07, p = .30). Palacio-Ortiz et al. (2018) was not included in the subgroup analysis because they did not report the mean age (SD) of participants.
Rates by Sex
Four studies provided sex-specific depression rates (Inci et al., 2019; Ipci et al., 2020; Mitchison & Njardvik, 2019; Yüce et al., 2013). Subgroup analysis showed a significant difference in rate between sexes (χ²(1) = 5.09, p = .02), with females showing a higher rate (20.93%, 95% CI [0.07, 0.39]) than males (8.97%, 95% CI [0.02, 0.19]).
Rates by ADHD Medicine Use
Ten studies reported on ADHD medication use among participants (Ahmed et al., 2021; Breaux et al., 2022; Cleminshaw et al., 2020; S. S.-F. Gau, Lin, et al., 2010; S. S.-F. Gau, Ni, et al., 2010; Işık et al., 2018; Joseph et al., 2019; Nadeau et al., 2015; Palacio-Ortiz et al., 2018; Zerón-Rugerio et al., 2021). Subgroup analysis found no significant difference in depression rate between studies with and without participants receiving ADHD medication (χ²(1) = 0.17, p = .68). The pooled depression rate was 10.93% (95% CI [0.03, 0.22]) for studies reporting participants using ADHD medication and 17.78% (95% CI [0, 0.98]) for studies reporting participants not using ADHD medication.
Rates by Recruitment Pathways (Clinical or Community)
Subgroup analysis by recruitment settings showed no significant difference between groups (χ²(1) = 0.79, p = .50). Studies recruiting participants from community settings reported a pooled rate of 14.95% (95% CI [0.01, 0.38]), whereas those recruiting from clinical settings reported a lower pooled rate of 10.61% (95% CI [0.06, 0.16]).
Comparison of Depression Rates Between ADHD and Neurotypical Participants
A subgroup analysis of seven case-control studies compared depression rates between children and adolescents with ADHD and their neurotypical peers, where a neurotypical group was included in the current studies. The analysis indicated that the pooled depression rate was significantly higher in the ADHD group (12%, 95% CI [0.01, 0.31]) compared to the neurotypical group (2%, 95% CI [0.01, 0.04]; χ²(1) = 4.88, p = .03). Figure 4 presents a forest plot summarizing the pooled rate estimates and 95% CI for both groups.
Forest plot comparing rates of depression in children and adolescents with ADHD to neurotypical children and adolescents in case-control studies.
Discussion
This systematic review and meta-analysis examined depression rates in children and adolescents (≤18 years old) with ADHD but without ID, with reported rates varying from 1.7% to 60%. The meta-analysis estimated a pooled rate of 11.31% across 24 studies. The substantial heterogeneity (I2 = 91%) highlights the potential influence of various factors, including demographic characteristics (e.g., pubertal status, sex, and ADHD medication use), recruitment pathways (i.e., clinical and community), assessment tools (i.e., questionnaire and interviews), and informants (i.e., self and parent reports). Subgroup analyses were conducted to explore the sources of heterogeneity, indicating significant differences in depression rates in ADHD for sex and assessment tools, while no significant differences were found in others. Subgroup analyses for key factors such as SES, ethnicity, and geographical regions were not feasible due to inconsistent or absent reporting across studies. Nevertheless, depression frequently co-occurs in children and adolescents with ADHD, and rates in this population are significantly higher than for their neurotypical peers.
This review indicated sex and depression assessment tools as key factors significantly influencing the estimated rates of depression in children and adolescents with ADHD. Subgroup analysis suggested significant sex differences, with girls with ADHD having a higher pooled depression rate (20.93%) compared to boys (8.97%), approximately twice as high. A similar disparity is observed in their neurotypical peers, where depression rates in girls are two to three times higher than in boys (e.g., Frey et al., 2020; Salk et al., 2017). This pattern extends into adulthood; Hartman et al. (2023) demonstrating that while women with ADHD have higher depression rates than men with ADHD, the proportional sex differences remain consistent across those with and without ADHD. These findings suggest that ADHD may not alter the sex differences in depression rates. However, the underrepresentation of females in ADHD research may influence the accurate estimation of the depression rate in this population. This underrepresentation may stem from sex differences in ADHD symptoms, as females are more likely to show less hyperactivity/impulsive and disruptive behaviors, and more internalizing symptoms or eating disorders, which can lead to missed or delayed ADHD diagnosis in women and girls (Attoe & Climie, 2023; Quinn, 2008). Thus, some females with undiagnosed ADHD may be excluded from the ADHD group, leading to an underestimation of both the prevalence of ADHD and the associated rate of co-occurring depression. The predominance of male participants (over 70%) in most included studies highlights a longstanding sex imbalance in ADHD diagnosis. Further studies should strive for more sex-balanced samples, with a particular focus on females, given the recent increase in ADHD diagnoses among this group (Nussbaum, 2012; Young et al., 2020).
The methods used to assess depression also significantly influence rate estimates for children and adolescents with ADHD, with rates varying widely depending on the assessment method. The highest rates were reported in studies using both interviews and questionnaires (20.87%), followed by questionnaires alone (16.13%) and interviews alone (8.43%). This finding is consistent with previous research showing that prevalence estimates based on depression screening tools or rating scales tend to be higher than those based on interviews (Levis et al., 2019; Parsons et al., 2024). This review conducted a subgroup analysis that further indicated that depression rates reported through interviews were consistently low, regardless of whether clinicians (8%) or trained researchers (11%) administered the interviews. Compared to questionnaires or rating scales, interviews typically elicit more accuracy for diagnosing depression and estimating prevalence rates due to interviewer expertise and the supportive environment they provide for clarification (Phellas et al., 2012; Vassilopoulos et al., 2020). However, accurately assessing depression in children and adolescents with ADHD remains challenging due to the phenotypic overlap between the two conditions.
ADHD symptoms such as inattention, restlessness, and irritability also manifest in depressive symptomatology (Fraser et al., 2018; Powell et al., 2021), potentially leading children and their parents to overreport depressive symptoms on standardized questionnaires designed for neurotypical populations (Thapar et al., 2023). While interviews are generally more accurate for symptom evaluation, the lack of ADHD-specific validated measures may cause interviewers to interpret overlapping symptoms as part of ADHD, potentially masking and underestimating co-occurring depression (Garcia-Argibay et al., 2024). These contrasting biases highlight the importance of developing and/or adapting assessment tools tailored to ADHD populations. Furthermore, combining questionnaires and interviews may provide a more accurate assessment of depression, as questionnaires are effective for identifying specific depressive symptoms (e.g., low mood, concentration disturbance, sleep disturbances, and suicidal ideation), while interviews offer advantages in exploring contextual factors, clarifying symptoms, and evaluating their impact on functioning (Vassilopoulos et al., 2020).
In this review, only four employed tools were found to have acceptable psychometric properties for children and adolescents with ADHD. Nadeau et al. (2015) used the RCADS (Chorpita et al., 2000), a questionnaire that has demonstrated acceptable reliability, convergent validity, and discriminant validity in this population, particularly for the anxiety and depression subscales (Becker et al., 2019). Suthar et al. (2018) employed the VADPRS/VADTRS, a standardized questionnaire developed to assess ADHD and its co-occurring externalization (ODD/CD) and/or internalization (anxiety/depression) conditions in research and clinical settings (Wolraich et al., 1998, 2003). Additionally, two studies used diagnoses based on DSM-5 or ICD-10 interviews by experienced child psychiatrists (Palacio-Ortiz et al., 2018; Sumiła & Cieślukowska, 2008). These criteria, commonly used by psychiatrists, are the foundation of most depression measures and are considered acceptable for diagnosing depression in the ADHD population (Saito et al., 2010; Zimmerman et al., 2010). Most of the included studies used measures designed for the neurotypical population, given the overlapping symptoms of ADHD and depression, using specialized instruments designed or adapted for the ADHD population may help improve diagnostic accuracy (Thapar et al., 2023). The differences in reported depression rates between studies using measures with demonstrated reliability and validity for ADHD populations (18%) and those without such evidence (10%) suggest a need for further exploration of how assessment tools impact rate estimates. Further studies would benefit from exploring if developing or adapting existing measures to better account for the nuances of ADHD populations could enhance the accuracy of depression assessment. Future studies could also consider the combined use of questionnaires and interviews to provide a more comprehensive and accurate evaluation of depression in this population.
Other factors, including pubertal status, informant type, recruitment settings, and ADHD medication use, did not show statistically significant effects but may still influence depression rates in children and adolescents with ADHD. Puberty is a crucial developmental stage marked by physical changes, hormonal fluctuations, and social relationship challenges that can increase the risk of developing depression (Jiang et al., 2021; McGuire et al., 2019). This review found slightly higher depression rates in post-pubertal participants (15.1%) compared to pre-pubertal participants (9.9%), though the difference was not significant. The lack of significance may be due to the broad age ranges in some studies (e.g., 5–19 years) but classified them as pre-pubertal based solely on a mean age below 12 years (e.g., Ambrosini et al., 2013; Inci et al., 2019; Ipci et al., 2020; Nadeau et al., 2015; Zerón-Rugerio et al., 2021). Such classification may obscure developmental differences related to pubertal onset and introduce bias in depression rate estimates. Future research would benefit from focusing more selectively on different age stages or accurately assessing pubertal status to better understand the developmental trajectory of depression in this population.
This review found no significant differences in depression rates based on informants. However, trends indicated that studies only using parent reports had the highest pooled rates (24.37%), followed by combined parent and child reports (9.73%) and child/adolescent-only reports (9.52%). The lack of significance may be due to the limited number of studies exclusively using parent reports (n = 2), reducing the statistical power. These trends align with prior research suggesting that children and adolescents with ADHD tend to underestimate their depressive symptoms, while their parents may overreport them (Fraser et al., 2018). This underscores the importance of incorporating multiple informants in depression assessments to reduce bias in depression assessment (De Los Reyes & Kazdin, 2005; Tepper et al., 2008). Although teachers’ reports can offer valuable insights into depressive symptoms in social and academic contexts (Mesman & Koot, 2000; Thapar et al., 2023), only one study in this review included teachers as informants. Similarly, while clinicians’ observations provide a nuanced and multidimensional understanding of depression (Baik et al., 2008; Vares et al., 2015), none of the included studies used them as a primary source, suggesting a gap in the literature. Future research would benefit from integrating multiple informants—teachers, parents, children/adolescents, and clinicians—to enhance the validity and reliability of depression assessments in the ADHD population.
This review found no significant differences in depression rates based on recruitment settings. However, recruiting participants from both clinical and community settings remains important, as clinical samples often capture more severe ADHD and/or depressive symptoms due to stricter referral thresholds (Bauermeister et al., 2007; Orchard et al., 2017), while community samples reflect a broader range of symptom severities (e.g., subthreshold symptoms; Cuijpers et al., 2010; Seymour et al., 2014). Similarly, no significant differences were observed between studies with and without ADHD medication use. This may be attributed to inconsistencies or lack of the type of ADHD medication reported across included studies and variability in the proportion of participants receiving medication (ranging from 14% to 87.5%). Different medications, such as stimulants (e.g., methylphenidate) and non-stimulants (e.g., atomoxetine), can affect depressive symptoms through different mechanisms (Chang et al., 2016; Oh et al., 2022). Furthermore, a tendency for lower rates of ADHD medication use may also lead to under-treatment of co-occurring depression (Chang et al., 2016). These issues within the included studies likely introduced bias and reduced the reliability of the findings. To better understand the co-occurrence of ADHD and depression, future research would benefit from incorporating diverse recruitment sources and ensuring detailed reporting of ADHD medication use.
Limitations and Future Directions
There are some limitations in this systematic review and meta-analysis. First, studies that used cut-off questionnaires to assess depression were included. While interviews may provide a more comprehensive evaluation of depressive symptoms (Craddock & Mynors-Wallis, 2014; Pettersson et al., 2018), questionnaires remain widely used in clinical practice, research, and screening. The Children’s Depression Inventory (CDI), for instance, is a well-researched and clinically valuable tool commonly applied to assess depression in pediatric psychiatric inpatients (Friedberg & Sinderman, 2011). Thus, including studies that employed these questionnaires was necessary for capturing the breadth of available research. Secondly, this review excluded studies not published in English, potentially limiting the inclusion of broader, regionally diverse studies.
This review was not able to examine the impact of SES, ethnicity, and geographical regions on depression rates in children and adolescents with ADHD due to inconsistent or absent reporting, and limited country representation in the included studies. Considering these factors is important, as clinical practices, diagnostic criteria, and cultural attitudes toward mental health can vary significantly across regions and populations (Krendl & Pescosolido, 2020; Rodríguez-Donate et al., 2024; Simon et al., 2002). Moreover, this review included some studies with small sample sizes (e.g., Breaux et al., 2022; sample size = 18). Small sample sizes are common in ADHD research due to the challenges of recruitment and the specificity of the population (Kanevski et al., 2023). However, studies with small sample sizes are more susceptible to variability and introduce “small-study effects,” where studies with small sample sizes tend to report larger prevalence rates or treatment effects due to factors such as publication bias, methodological differences, or greater sampling variability (Lin, 2018; Sterne et al., 2000). While these studies were retained due to their relevance to the aims of this review, the results should be interpreted with caution given the potential for bias.
It was beyond the scope of the current review to systematically examine factors and mechanisms contributing to differences in depression rates between children and adolescents with ADHD and their neurotypical peers. While a subgroup meta-analysis was conducted on the included case-control studies, moderate-to-high heterogeneity was observed in both groups, suggesting that methodological and sampling variability may have introduced bias. For example, most included studies (except Zerón-Rugerio et al., 2021) did not consistently report exclusion criteria for neurotypical participants, making it unclear whether these control groups recruited individuals who did not have any psychiatric conditions (i.e., “super-control” group; Tiego et al., 2023). Future studies would benefit from incorporating well-matched neurotypical control groups and applying consistent recruitment strategies (e.g., matching on age, recruitment settings, FSIQ, and co-occurring conditions apart from the ADHD diagnosis) to better examine the specificity of observed patterns.
Notwithstanding these limitations, this is the first systematic review and meta-analysis to identify depression rates in children and adolescents with ADHD. It underscores that depression is a common co-occurring condition in this population, with significantly higher rates than their neurotypical peers. This review highlights methodology diversity across studies in this field, including variations in recruitment pathways, depression assessment tools, and informants. It also points to the inconsistent reporting of crucial characteristics, including SES, ethnicity, pubertal status, and ADHD medication use, as well as the lack of safe and effective depression assessment tools tailored to children and adolescents with ADHD. To achieve more reliable and accurate rate estimates in further research, there should be a focus on recruiting large samples from community settings, using standardized depression assessment tools designed for the ADHD population, and collecting data from multiple informants, including children, parents, and teachers. This systematic review also highlights the need for further studies to explore if the developmental trajectory of depression in children and adolescents with ADHD follows patterns similar to those in neurotypical populations across different pubertal statuses and sex.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.