
Abstract
Introduction:
Prescription stimulants are an effective FDA approved treatment for attention deficit hyperactivity disorder (ADHD) however their safety has come under scrutiny. Multiple studies demonstrate safe use in pediatric populations, but prescriptions are increasing to adults and it is not evident which comorbidities might place people at risk of adverse outcomes. The aim of this study is to identify risk factors of adverse cardiovascular events for individuals exposed to stimulants across the lifespan.
Methods:
We conducted a case control study utilizing the TriNetX research network database. Individuals were included for study if they were younger than 90 years old and prescribed stimulants between January 1, 2010 and December 31, 2020. We utilized summary statistics, chi2, and multivariate logistic regression to identify risk factors for cardiovascular events.
Results:
Of the 987,762 individuals prescribed stimulants, 49,902 experienced an adverse cardiovascular event. Individuals with atherosclerotic heart disease had the highest odds of adverse events (aOR = 36.7, p < .001). Hypertension (aOR = 2.78 p < .001), cocaine use (aOR = 1.64 p < .001), and anxiety (aOR = 1.46 p < .001) were also strongly predictive of adverse outcomes, but risk varied by age.
Conclusions:
Atherosclerotic heart disease and its antecedents pose the greatest risk for cardiovascular events for people prescribed stimulants. Mental health diagnoses are also independent predictors and age may be an effect modifier of these relationships. ADHD was not an independent risk factor for major adverse cardiovascular events when controlling for other biopsychosocial variables in adult populations. Additional research focused on predictive models and prospective studies may be warranted to better inform clinical decisions regarding stimulant prescriptions for the broad demographic of patients that may benefit from these medications.
Introduction
There are 3.3 million children and 16 million adults prescribed stimulants such as amphetamine, lisdexamfetamine, and methylphenidate in the United States (Danielson et al., 2018; Piper et al., 2018; Safer, 2016). Stimulants exert their effects via neurotransmitters such as dopamine, serotonin, and norepinephrine to increase alertness, reduce appetite, elevate heart rate, blood pressure, and enhance mood (Olfson et al., 2013). They are broadly utilized in treatment of attention deficit hyperactivity disorder (ADHD) as well as narcolepsy, but may also be utilized for other conditions (Hardy, 2009; Lim et al., 2023; Smith et al., 2021).
While stimulants are effective across a broad phenotype of symptoms, concerns have been raised regarding their safety (Arnsten, 2006; Hechtman et al., 2004; Rajeh et al., 2017). Multiple studies demonstrate stimulant safety in pediatric populations, but studies also consistently show elevations in heart rate as well as blood pressure, and episodes of sudden cardiac death involving stimulant medications have been documented and warned by the FDA (Charatan, 2006; Hennissen et al., 2017). Just as concerning, recent studies demonstrated a six- to nine-fold elevated risk of major adverse cardiovascular events (arrhythmia, heart attack, and stroke) when stimulants are prescribed to older adults, and stimulants are increasingly prescribed to nonpediatric populations, where safety data are lacking (Brumbaugh et al., 2022; Latronica et al., 2021, 2022).
There are many factors that may contribute to this elevated risk in older populations including atrophy of pacemaker cells, myocardial fibrosis, and atherosclerosis (Choi et al., 2022). However, the aging process is not uniform, so it is possible that safety may vary across the lifespan, and within age demographics. Given the cases of sudden cardiac death, continual increase in stimulant prescriptions, and the increasingly broad demographics that are receiving these prescriptions, it is important to identify potential risk factors for cardiac events so that patients and providers can make informed decisions when considering risks and benefits of stimulant medications (Brumbaugh et al., 2022). The aim of this study is to determine which patient level factors are associated with adverse cardiovascular events for people prescribed stimulants across the lifespan.
Methods
Data Source
We conducted a case control study utilizing a national database (TriNetX). TriNetX is a federated health research network consisting of de-identified, aggregated electronic health records (EHRs) (demographics, diagnoses, procedures, medications, laboratory tests, and genomics) of more than 70 million patients from participating healthcare organizations.
Study Design
We included all individuals younger than 90 years of age who were prescribed a stimulant (amphetamine, dextroamphetamine, lisdexamfetamin, methylphenidate, methamphetamine, or dexmethylphenidate) between January 1, 2010 and December 31, 2020. We excluded all individuals prescribed a stimulant before 2010 and those 90 and older. Individuals were classified as a case if they experienced a cardiovascular event after starting stimulant medications and a control if they did not experience a cardiovascular event during the study period. Cardiovascular events were captured using the following ICD-10 diagnosis codes: ischemic heart diseases (I20-I25), cardiac arrest (I46.9), atrial fibrillation (I48), cardiac arrhythmias (I49), heart failure (I50), and cerebral infarction (I63). We utilized the biopsychosocial model, literature review, and clinical expertise to determine variables of interest and controlled for known risk factors of cardiovascular events including patient demographics and relevant comorbidities. Our final model included age, gender, race atherosclerotic heart disease, hypertension, diabetes, obesity, depression, anxiety, schizophrenia, bipolar disorder, nicotine use, alcohol use, cocaine use, and opioid use. We also conducted an age stratified analysis to explore age as an effect modifier in the relationship between biopsychosocial variables and cardiovascular events.
Data Analysis
We addressed our aims with descriptive statistics (t-test for continuous variables, Chi-square test for categorical variables) and logistic regression analyses. The adjusted odds ratio (aOR) and p-value were computed to indicate the effect and the significance level of prescription stimulants. We conducted all analyses with R statistical software package and all data in TriNetX are de-identified so this study was exempt from Institutional Review Board oversight.
Results
Study Population
A total of 987,762 individuals were prescribed stimulants between January 1, 2010 to December 31, 2020. The average age of all participants was 28.7 years old, and 48.7% of the study sample was female. There were 49,902 cases (cardiovascular events) and 937,860 controls. The most common diagnoses were ADHD (43.2%), anxiety (26.9%), and depression (21.4%). Of note, the majority of those prescribed a stimulant did not have a diagnosis of ADHD (56.8%). The most common diagnoses among cases were hypertension (55.5%), depression (48.9%), anxiety (47.9%), ADHD (33.9%), and atherosclerotic heart disease (31.1%) (Table 1).
Characteristics of the Study Population.
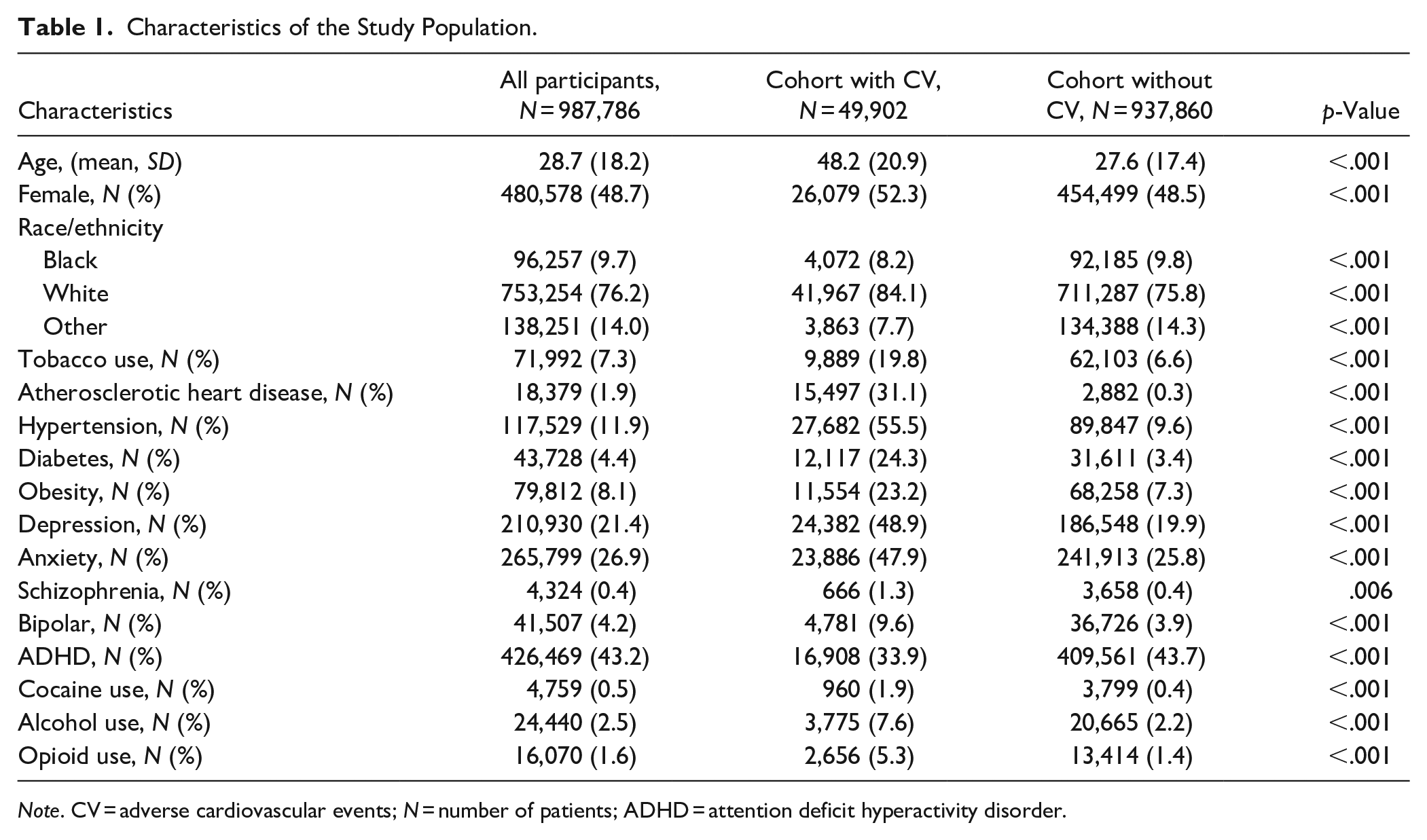
Note. CV = adverse cardiovascular events; N = number of patients; ADHD = attention deficit hyperactivity disorder.
Risk Factors for Cardiovascular Events
People with a cardiovascular event had a higher average age (48.2 years old) than those without a cardiovascular event (27.6 years old, p < .001). The strongest risk factor for cardiovascular events was diagnosed atherosclerotic heart disease (aOR = 36.7, p < .001). Other notable biological variables associated with cardiovascular events included hypertension (aOR = 2.78, p < .001), diabetes (aOR = 1.56, p < .001), and obesity (aOR = 1.45, p < .001). Additionally, depression (aOR = 1.55, p < .001) and anxiety (aOR = 1.46, p < .001) were both strongly correlated with cardiovascular events (Table 2). Substance use disorders (SUDs) such as cocaine alcohol, and opioid use were also associated with increased odds of adverse cardiovascular events. Of note, a stimulant prescription for people with a diagnosis of ADHD was associated with reduced risk of a cardiovascular event (aOR = 0.95, p < 0.01) when controlling for other risk factors.
Assessment of Risk Factors for Cardiovascular Events Among Patients With Stimulant Prescriptions.
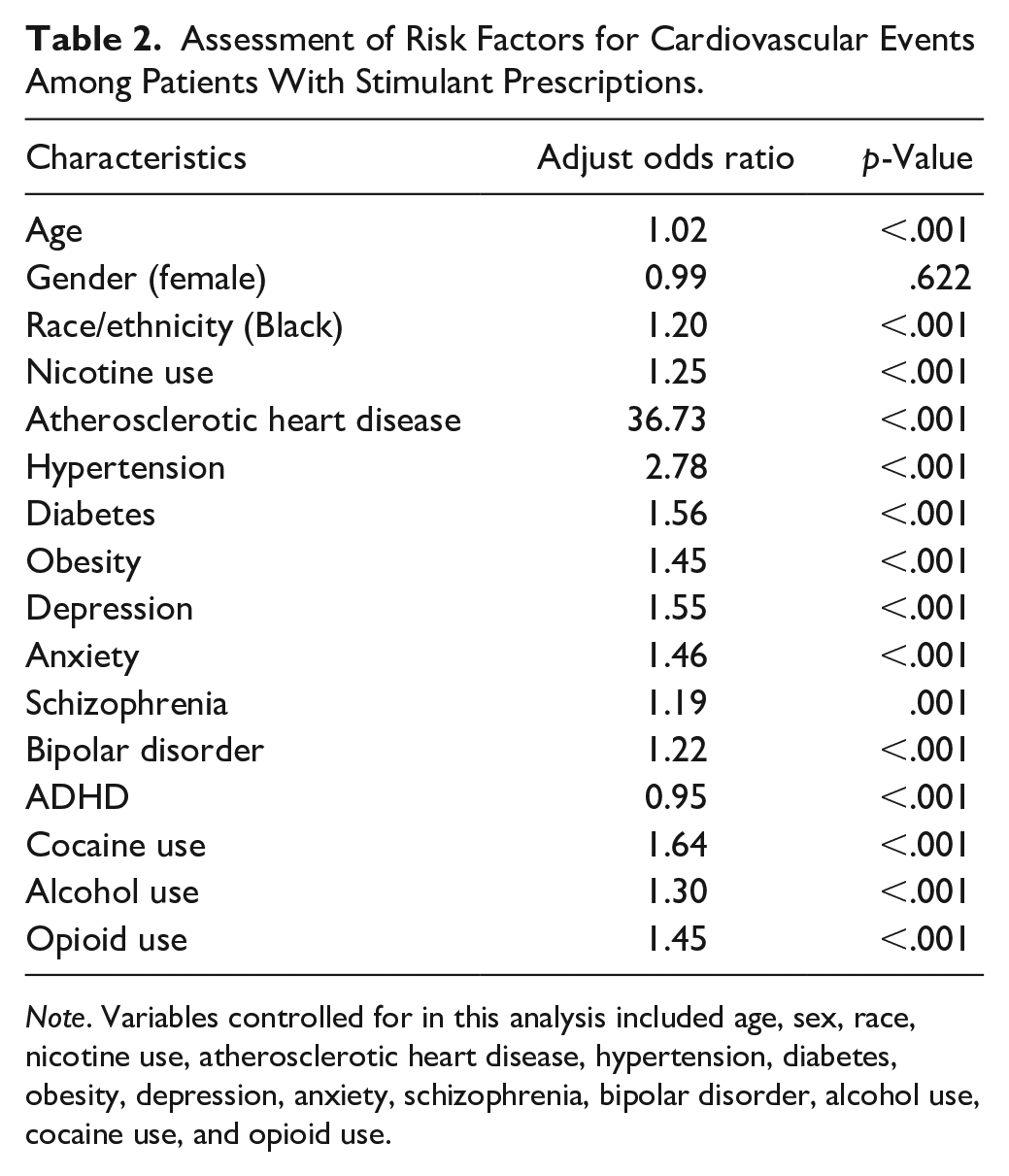
Note. Variables controlled for in this analysis included age, sex, race, nicotine use, atherosclerotic heart disease, hypertension, diabetes, obesity, depression, anxiety, schizophrenia, bipolar disorder, alcohol use, cocaine use, and opioid use.
Multivariable Age Stratified Analysis
Multiple variables demonstrate differences in risk across the lifespan. The strongest risk factor for adverse events in all age groups was a diagnosis of atherosclerotic heart disease (aOR = 13.32–316.0, p < .01) (Figure 1a). Known risk factors for atherosclerotic heart disease were also consistently associated with elevated risk across the lifespan: hypertension (aOR = 2.43–4.72, p < .01), diabetes (aOR = 1.44–1.75, p < .01), obesity (aOR = 1.29–1.58, p < .01) (Figure 1a). Race was not a strong independent risk factor for adverse events in younger age groups, but was associated with increased risk of cardiovascular events among those aged 36 and older (aOR = 1.24–1.33, p < .01) (Figure 1b).
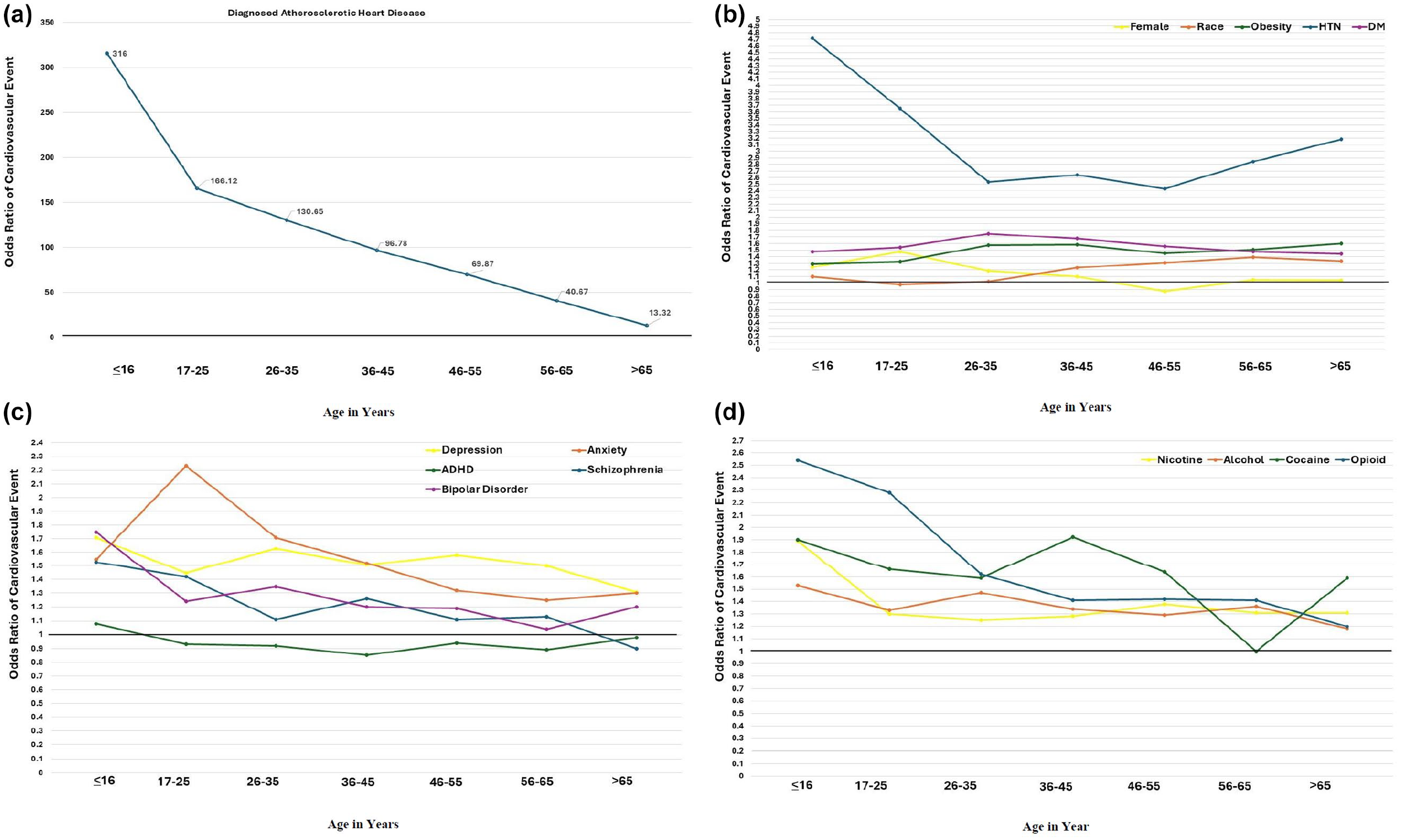
Age stratified assessment of cardiovascular events based on biopsychosocial risk factors.
When we evaluated psychological variables, we noticed that ADHD was associated with slightly increased risk of adverse events in people younger than 16 but was the only variable consistently associated with reduced risk or no difference in adverse events in all other age groups (aOR = 0.85–0.98) (Figure 1c). Anxiety was most strongly associated with adverse events among people ages 17–25 (aOR = 2.23, p < .01) and consistently associated with increased risk through adulthood. We observed a similar trend for depression. Bipolar disorder and schizophrenia did not evidence statistically significant between group differences for those 56–65 and those 26 and older, respectively (Figure 1c).
Similar to psychiatric illness, substance use was a significant risk factor for cardiovascular events across the lifespan, but most strongly predictive of adverse events in younger populations. All associations for nicotine use, alcohol use, opioid use, and cocaine use were statistically significant with the exception of the following substances by age group: nicotine use age 56–65, cocaine use ages 56 and older, opioid use ages 65 and older (Figure 1d).
Discussion
Prescription stimulants have increased dramatically over the past 20 years and their safety has been questioned, particularly in older populations. The strongest risk factor for cardiovascular events at all ages was a diagnosis of atherosclerotic heart disease, and the majority of people that experienced adverse events had a diagnosis of hypertension (55%), a known risk factor of atherosclerotic heart disease. Psychosocial variables such as depression, anxiety, and substance use, were more prominent risk factors in younger adults than older adults. ADHD was not an independent risk factor for adverse events in people older than 16 when adjusting for other biopsychosocial risk factors. Although atherosclerosis is consistently the strongest predictor of negative events, our data suggest variable risk of cardiovascular events across the lifespan.
A recently published case control study that thoroughly evaluated the relationship between ADHD medications and cardiovascular outcomes found increased duration of medication exposure was associated with increased risk of cardiovascular events (Zhang et al., 2024). They observed similar patterns in the relationship between stimulant exposure and cardiovascular events in youth and adults (Zhang et al., 2024). While this suggests conflict with our results, differences in study design may explain differing conclusions. First, their study controlled for similar risk factors (diabetes, hypertension, gender, substance use disorders, depression, and schizophrenia) and assessed similar outcomes of interest (incident adverse cardiovascular events), but their study took place in Sweden, where there is lower prevalence of substance use disorders than the United States (Vetter et al., 2008). Prevalence of substance use disorders varies across the lifespan, which may have contributed to some of the variance we detected in our US sample (Wu & Blazer, 2014). Second, they excluded individuals that received a stimulant prescription for a non-ADHD diagnosis prior to the study index date (Zhang et al., 2024). We included all individuals that received stimulants, which may have also contributed to the age related variability in our data. Finally, they only assessed two age groups 1) those <25 and 2) those
The American Heart Association (AHA) currently recommends clinicians assess for history of fainting, dizziness with exertion, chest pain with exercise, or change in exercise tolerance before prescribing stimulants (Vetter et al., 2008). They also recommend assessing for heart murmur, family history of sudden cardiac death, long QT syndrome, Wolff-Parkinson-White syndrome, and Marfan’s syndrome (Vetter et al., 2008). These recommendations align with our data, however we suggest providers remain mindful that many do not manifest overt symptoms of conditions such as atherosclerosis. Other prominent risk factors for cardiovascular events such as obesity, diabetes, anxiety, and depression are not mentioned in their guidelines. Still, these more insidious conditions may contribute to adverse events, such as the unexpected deaths that resulted in a black box warning by the FDA. This is most evident in the trends witnessed between atherosclerosis and cardiovascular events in various age groups. Atherosclerosis is a prominent risk factor across the lifespan but in our study, the magnitude of the association decreases with increased age. This is unlikely due to a reduced absolute risk associated with stimulant use in older adults with atherosclerosis and most likely explained by increased prevalence of undiagnosed atherosclerosis as well as increased general risk of cardiovascular events in non-pediatric populations. Obesity and hypertension are both examples of conditions that can slowly yield elevated cardiac vulnerabilities over time. This may explain why our study shows they are more prominent independent risk factors among people older than 65 than people in their 20s. Given potential for silent disease, these risk factors of atherosclerosis may be particularly important when considering stimulant prescriptions for older adults.
The elevated risk for adverse cardiac events in young people prescribed stimulants with a diagnosis of anxiety, depression, or substance use in our study population also aligns with existing literature. It is possible that cardiovascular events among individuals with mental illness are mediated by subclinical QT prolongation, the risk factor identified by the AHA. However, studies show that young adults with depression or anxiety are more likely to engage in prescription stimulant misuse or non-oral use (inhalation or injection) of stimulants; this can strongly influence the risk of cardiovascular events and may explain the increased risk of cardiovascular events in patients with depression, anxiety, bipolar disorder, and schizophrenia across the lifespan in our study (Chang et al., 2014). It is also worth noting that substance use and misuse decrease with age, which we observe in the reduced strength of the association between psychosocial variables and cardiovascular events in our older age groups (Wu & Blazer, 2014). The reduced magnitude of these independent effects may also be attributed to increased relevance of other cardiovascular variables (diabetes, hypertension, obesity, atherosclerosis) in older adults.
Importantly, treatment of ADHD with stimulants may reduce risk of substance use and related disorders (Chang et al., 2014). ADHD is associated with reduced risk of adverse events in nearly all age groups of our study. These reduced cardiovascular risks align with a recent study that demonstrated reduced all-cause mortality among a cohort of individuals who were treated with stimulants for ADHD (Li et al., 2024). These associations are important to consider as prescription stimulant requests grow across the United States and providers are forced to make decisions with patients regarding risks compared to benefits in both pediatric and non-pediatric populations.
Limitations
While these data offer value to clinical and scientific communities, there are a number of limitations that should be considered. First, the study relied on electronic health records which has known susceptibility to inaccuracy and misclassification bias. There is no ability to review charts to validate data or evaluate the extent of bias. However, there is no reason to suspect unbalanced misclassification. Additionally, this study explores the risk of cardiovascular events with stimulant use, however the analyses are based on a proxy for stimulant use, stimulant prescriptions. Our research data did not indicate whether a diagnosis was a primary diagnosis nor specify the diagnosis associated the stimulant prescription. Furthermore, this study explores the risk of cardiovascular events with prescription stimulant use, however it does not detail variability in risk based on specific dose, duration, or the type of stimulant prescribed. Nevertheless, this study offers providers initial information regarding cardiovascular risks when they consider prescribing stimulants irrespective of their justification, when the patient has co-morbid anxiety, depression, substance use disorders, and other underlying cardiovascular risks at various life stages.
We hope this study serves as a foundation for future inquiry as well as clinically relevant information that providers may consider when discussing potential risks and benefits of stimulant prescriptions with their patients. Further study is needed to establish dose response relationships and the degree of risk among individuals with multiple risk factors as well as those exposed to various formulations of stimulants. Feasibility and acceptability of more nuanced risk stratification prior to initiation of prescription stimulants, time to event studies, and prospective trials to further evaluate safe use of prescription stimulants in non-pediatric populations are warranted.
Conclusion
These data suggest that risk associated with stimulants varies across the lifespan and the majority that do have adverse outcomes have known risk factors for atherosclerosis or diagnosis of atherosclerosis. Attention deficit and hyperactivity disorder was not an independent risk factor for major adverse cardiovascular events when controlling for other biopsychosocial variables in adult populations. Additional research focused on predictive models and prospective studies may enhance conversations regarding risks and benefits of stimulant prescriptions for the broad demographic of patients that receive these prescriptions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.