
Abstract
Objective:
To examine the experiences of Australian parents raising primary school-aged children with ADHD and gather feedback on a proposed ADHD parenting program.
Methods:
Reflexive thematic analysis of semi-structured interviews undertaken with 11 Australian parents of 7- to 11-year-old children with ADHD. Interviews were conducted over Webex, audio recorded, transcribed verbatim, and analyzed in NVivo Ltd. software.
Results:
We identified four themes: (1) “I love my child but their ADHD traits are challenging,” (2) “Compliance, control, and completion,” (3) “It’s hard, burdensome, and exhausting and I can feel like I’m alone,” and (4) “What a welcome relief.”
Conclusion:
Parents report that although raising neurotypical children is difficult, the presence of childhood ADHD increases the emotional and support burden placed on them. Parents were also very interested in and supportive of the proposed ADHD parenting program. The program aims to enhance parents’ understanding of the neurocognitive implications of ADHD and to foster secure parent-child attachment, attuned parental responsiveness, and age-appropriate development of traits that promote well-being, adaption and recovery in people with ADHD.)
ADHD, the most common childhood neurodevelopmental condition (Francés et al., 2022), can have a far-reaching impact on the lives of children and their families (Harpin, 2005). Characterized by inattentive and/or hyperactive-impulsive symptoms (American Psychiatric Association, 2013), ADHD affects a child’s brain development (Hoogman et al., 2017), cognitive functioning (Onandia-Hinchado et al., 2021), and ability to exert age-appropriate self-control (Schel et al., 2014). The condition is frequently accompanied by emotional regulation challenges (Beheshti et al., 2020), and co-occurring conditions such as autism spectrum disorder and learning disorders (Gnanavel et al., 2019). ADHD affects a child’s everyday functioning, and accross the life course, can impact goal attainment (Barkley, 2015), social relationships (Ros & Graziano, 2018), psychological and physical health, quality of life, and life expectancy (Faraone et al., 2021).
The disruptive nature of ADHD symptoms, the high emotional and support burden ADHD places on parents (Corcoran et al., 2017; Laugesen & Groenkjaer, 2015), and the stigma parents endure (Mikami et al., 2015), can impact parental wellbeing and the parent-child attachment relationship (Wylock et al., 2023). As can the frustration that parents report arises due to behavioral management strategies being difficult to apply and limited in their effectiveness (Corcoran et al., 2017). Parents of children with ADHD report experiencing intense negative emotions (Corcoran et al., 2017) including feelings of hopelessness, inadequacy, incompetence, frustration, exhaustion, guilt, anger, helplessness, and self-blame (Laugesen et al., 2016; Laugesen & Groenkjaer, 2015). They also report higher levels of anxiety and depression (Deault, 2010); marital, family (Weyers et al., 2019), and parent-child relationship conflict (Deault, 2010); and parental stress (Cheung et al., 2018; Theule et al., 2013). These difficulties increase the likelihood that parents will respond to their children in ways that are hostile, overly critical and negative (Harold et al., 2013), and participate in parental rejection and maltreatment (Clayton et al., 2018). Adults have reported that their parent’s mismatched responses to their ADHD negatively shaped their self-esteem and self-concept, and affected their psychosocial functioning (Miller, 2017; Schrevel et al., 2016; Shattell et al., 2008), indicating these responses may contribute to children with ADHD experiencing more difficulties with attachment (Wylock et al., 2023), identity formation, self-esteem (Ringer, 2020), and self-worth (Kendall et al., 2004). They may also make living with ADHD more difficult as children with ADHD who display insecure or disorganized attachment patterns tend to display more symptoms of ADHD (Konowałek & Wolańczyk, 2020), while adults with ADHD and attachment insecurity are less likely to cope with their ADHD and less likely to use active, adaptive, and task-oriented strategies (Al-Yagon et al., 2020).
Parenting programs that are grounded in Bronfenbrenner and Morris’s (2006) Bioecological model of human development and (1) assist parents to sensitively understand or interpret their child’s behavior, (2) emphasize the creation of a good fit between their child’s inherited vulnerabilities and parental demands, and (3) facilitate competent parental responses (i.e., responses that support a child’s emotional awareness and expression and provide opportunities for choice and relational warmth), have the potential to facilitate parent-child interactions that support the attachment relationship (Shonkoff & Phillips, 2000). This is critical for facilitating adjustment and resilience in children with ADHD (Dvorsky & Langberg, 2016; Miller, 2017), and may improve parent and child wellbeing (Shonkoff & Phillips, 2000). This is especially the case while children are in the developmental stage of industry verse inferiority (E. Erikson & Erikson, 1998), as during this time a child’s self-concept and self-esteem becomes imbedded as they become more and more conscious of how they measure up to their peers (Issawi & Dauphin, 2017). Furthermore, these programs could assist parents to foster in their children traits that adolescents and adults with ADHD consider important for facilitating positive wellbeing, adaption, and recovery. These traits include: an understanding of ADHD (Ginapp et al., 2023), self-awareness (Becker et al., 2023; Miller, 2017), self-acceptance (Attoe & Climie, 2023; Beaton et al., 2022; Rasmussen et al., 2022), acceptance of disability (Botha & van der Westhuizen, 2023; Zapata & Worrell, 2023), and skills and compensatory strategies (Ginapp et al., 2023) that support self-mastery (Rasmussen et al., 2022).
While systematic reviews and meta-analyses suggest currently available evidence-based parent training programs reduce parent-rated ADHD symptoms and improve parent outcomes (i.e., parental stress and self-efficacy) in the short term (Coates et al., 2015; Lee et al., 2022; Leijten et al., 2018), these programs are rarely ADHD-specific. Instead, the majority were developed to treat children with conduct disorder. Although ADHD and conduct disorder appear to share some traits, the conditions are markedly different. While ADHD is a hereditable neurobiological condition associated with a neuropsychological developmental delay (Thapar & Stergiakouli, 2008) and symptoms that are outside of a child’s ability to control (Barkley, 2015), children with conduct disorder display deliberate, vindictive, threatening, and argumentative behavior (American Psychiatric Association, 2013). Furthermore, the vast majority of currently available parent training programs tend to be behavioral-based. While they teach parents to avoid yelling and other harsh parenting approaches, they aim to teach parents “how to manage their child’s non-compliance” (Lehner-Dua, 2001, p. 30) using top down parenting approaches including the provision of antecedents (i.e., routine and commands), rewards (i.e., positive attention, encouragement, praise, and tokens), and consequences (i.e., time out and other sanctions; Lehner-Dua, 2001; Lessard et al., 2016; Turan et al., 2022), which parents report have limited efficacy in the presence of ADHD (Corcoran et al., 2017).
The evidence, although very limited, suggests these programs do not improve the quality of the parent-child attachment relationship and attuned parental responsiveness when children with ADHD are aged between 6 and 11 years (Brown et al., 2024). Additionally, none appear to teach parents to listen with empathy or to use collaborative problem-solving techniques with the aim of helping parents promote age-appropriate development of self-awareness, self-acceptance, acceptance of disability, and skills and compensatory strategies that support self-mastery (Brown et al., 2024). Parents also report an unmet need for ADHD education and ADHD specific parenting advice (Bisset et al., 2023).
These findings highlighted to us the need to better understand the parenting approaches and strategies parents tend to employ, including their experiences implementing typically recommended parenting approaches. They also highlight that there may be a need for an ADHD-specific parenting training program that moves away from behavioral-based discipline toward empowering parents of children with ADHD with the knowledge and strategies required to promote attuned parental responsiveness and age-appropriate development of traits that facilitate positive long-term outcomes in people with ADHD.
Objectives
We carried out this study as per the first two non-linear stages of the UK Medical Research Council’s Framework for Developing and Evaluating Complex Interventions (Skivington et al., 2021): identification of the intervention and feasibility assessment. The aim being two-fold; (i) to better understand parent’s lived experiences and unmet support needs associated with raising their children with ADHD, and (ii) to determine if parents felt there was a need for an ADHD-specific parenting a program. One that aims to empower parents of children with ADHD to use parenting approaches and strategies that enable them to (1) scaffold the gap between their child’s innate capacity and the demands placed upon them in a manner that sets them up for success and protects them from harm, and (2) promote age-appropriate development of self-awareness, self-acceptance, and compensatory skills. The goal being to enhance the quality of the parent-child attachment relationship and help parents commence the process of fostering traits that support their child’s wellbeing, adaption, and recovery.
Methods
This qualitative study involved semi-structured interviews with 11 Australian parents of 7- to 11-year-old children with ADHD. We employed a pragmatic epistemology with the goal of making a purposeful difference to the outcomes of children with ADHD (Allemang et al., 2022).
Researcher Positionality
The researchers participating in this study are from the disciplines of nursing and psychology. Although we range in positionality and experience, we all situate ourselves in the neurodiversity paradigm. We view ADHD as a neurological difference that can cause significant disability, rather than a neurological abnormality or impairment. We consider ADHD as a condition that needs to be embraced and supported by parents, schools, and society in general so that individuals with ADHD can be empowered to live well with ADHD (den Houting, 2018; Dwyer, 2022). The first author, LEB who has ADHD and a child with ADHD, is active in the advocacy space. She feels a change in parenting approach and a focus on improving parent-child interactions within the attachment relationship may improve the outcomes of children with ADHD and their families. Before proceeding with program development however, she wanted to determine if the proposed program was something parents wanted or felt they needed, and gain insight into potential delivery mechanisms.
LEB developed this study with MT and GK. MT has an adult child with ADHD and a background in qualitative research. GK has no connection to ADHD and a background in healthcare program development. Following data collection and analysis, MB and BM were invited to join the study, their role being to independently review the data and themes prior to final confirmation. MB does not have lived experience of ADHD. He has a background in educational and developmental psychology and an interest in neurodiversity more broadly, especially the impact of neurodiversity on mental health outcomes. BM has ADHD and a child with ADHD. She has a background in translational research including psychological and health system intervention development and implementation, and participatory research practices.
Participants
Participants living in any part of Australia were recruited between November 2022 and February 2023. We used paid and unpaid Facebook advertisements to advertise the study. No compensation was offered to participants. Parents and guardians who were interested in participating were asked to contact LEB via email, who then made contact via telephone to ensure they met the study inclusion criteria, provide additional information and answer any questions. Parents who met the inclusion criteria were sent the study information and consent form. On receipt of a completed consent form, LEB arranged a suitable time for an online interview.
To be eligible to participate, parents had to have no previous or current relationship with the research team, and one or more children between 7 and 11 years of age with ADHD. Children were required to be on stimulant medication due to clinical practice guidelines recommending children with ADHD receive multimodal treatment and the impact this pharmacological intervention has on child ADHD symptoms (Cortese et al., 2012). The participant’s children could have co-occurring anxiety, depression, a learning disorder, or oppositional and defiant behavior. However, parents whose children had a diagnosis of conduct disorder, autism spectrum disorder, or bipolar disorder were excluded as these conditions significantly impact a child’s behavior and parenting requirements. The 7 to 11 years age range was chosen because, as per Erikson’s (1963) Psychosocial Theory, children move into a new developmental stage (industry vs. inferiority) at age 6 years, which ends around 11 years of age. In Australia, this coincides with the commencement of Primary School and likely necessitates a change in parenting practices, as is required when children commence high school (Kobak et al., 2017). Furthermore, clinical practice guidelines recommend not commencing children on ADHD medication until they are 6 years of age and it can take some time for the ideal medication dose to be determined (National Institute for Health and Care Excellence, 2018).
We applied the concept of “information power” (Malterud et al., 2016) to set an initial study sample. We determined 10 or more participants were required as (1) our study had a narrow aim and dense specificity, and we sought to (2) facilitate strong and clean communication between the researcher and participants, and (3) conduct an in-depth analysis of narratives (Malterud et al., 2016). We discontinued recruiting participants after meeting this requirement plus one. Data saturation was achieved following nine interviews, which was confirmed by two authors, this being the point at which no new information emerged from the interviews (Green & Thorogood, 2004).
Thirty-one parents expressed initial interest in participating in the study via email. The Participant Information and Consent Form was sent to 17 parents. We successfully recruited (measured by receipt of a signed consent form) and interviewed 11 participants in total: 10 biological parents and 1 foster parent, all female ranging in age between 30 and 39 years (n = 3), 40 to 49 years (n = 7), and >50 years (n = 1; See Table 1). Of the 11 participants, four had a diagnosis of ADHD or a partner diagnosed with ADHD. Their eldest child with ADHD was aged between 7 and 11 years (mean age = 9.8 years). They received their ADHD diagnose between the ages of 6 to 10 years (mean age = 7.3 years). The participants lived in Western Australia (n = 5), Queensland (n = 3), and New South Wales (n = 3). Seventy-two percent of participants had completed an Undergraduate Bachelor’s degree in comparison to 20.3% of the Australia population, and 36.4%, a post graduate degree (i.e., Masters or PhD) in comparison to 8.1% of the Australia population (Australian Bureau of Statistics, 2023). Four participants had previously participated in a parent training program, these included Circle of Security (n = 3; Powell et al., 2009), 1-2-3 Magic (n = 3; Phelan, 2004), Triple P (n = 2; Sanders & Turner, 2011), and Incredible Years (n = 1; Webster-Stratton, 1998). Three had previously worked with a Parent Coach (n = 1), Social Worker (n = 1), or Organizational Psychologist (n = 1).
Participant Demographic Details.
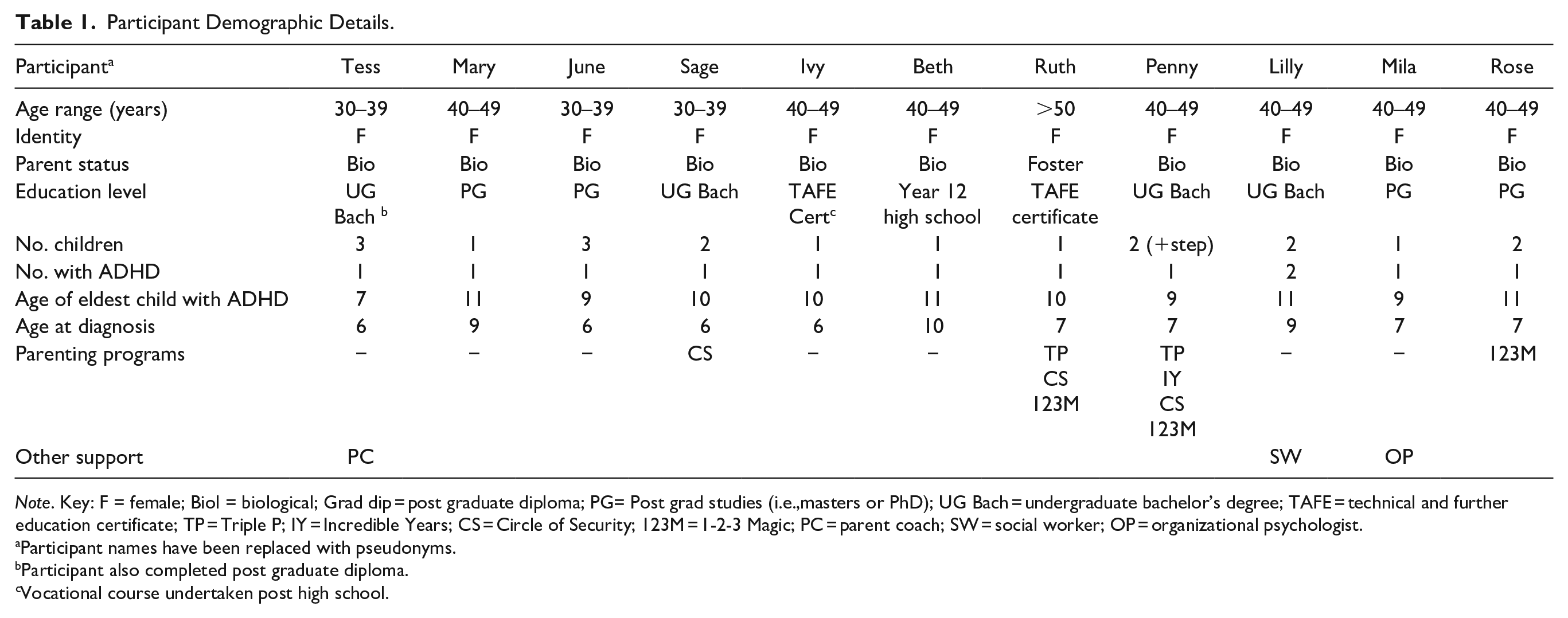
Note. Key: F = female; Biol = biological; Grad dip = post graduate diploma; PG= Post grad studies (i.e.,masters or PhD); UG Bach = undergraduate bachelor’s degree; TAFE = technical and further education certificate; TP = Triple P; IY = Incredible Years; CS = Circle of Security; 123M = 1-2-3 Magic; PC = parent coach; SW = social worker; OP = organizational psychologist.
Participant names have been replaced with pseudonyms.
Participant also completed post graduate diploma.
Vocational course undertaken post high school.
Procedures
Following informed consent, participants were invited to take part in a semi-structured interview at a date and time convenient to them. Participant demographic details were collected verbally at commencement of the semi-structured interviews. Semi-structured interviews were conducted by LEB using the WebEx video conferencing service. A semi-structured interview guide (see Appendix 1, Supplemental File 1) comprising open-ended questions and follow up probes was used to guide the interview process. The interview consisted of two parts. Part 1 explored topics related to the parent-child attachment relationship and participant’s experiences of raising their children with ADHD. In part 2, the proposed ADHD parenting program (Appendix 2, Supplemental File 1) was described before enquiring about participant’s views regarding acceptability and preferences for structure and delivery format. Interview length ranged between 43.11 and 61.05 min (mean = 51.04 min). The interviews were audio recorded before being transcribed verbatim. Personal identifying information was removed from the transcripts. Pseudonyms were used to refer to participants and the name/s of the participant’s child/ren were replaced by generic descriptors (i.e., son and daughter). LEB took field notes to document contextual aspects (setting) and participant behaviors (physical responses and mannerisms, nonverbal behavior) that could not be captured via WebEx audio recording. The study was approved by the Curtin University Ethics Committee (HE2021-0090).
Data Analysis
We used the six-phase reflexive thematic analysis process proposed by Braun and Clarke (2006, 2012). These steps involved: (a) data familiarization, (b) generation of initial codes, (c) identification of initial themes, (d) reviewing themes, (e) defining and naming themes, and (f) report writing (Braun & Clarke, 2006, 2012, 2021). NVivo Ltd. (Lumivero, 2023) version 14 software was used to manage the data and facilitate the systematic development of semantic and latent codes and themes. We used a hybrid inductive-deductive approach to coding and theme identification. For Part 1, the approach was primarily inductive, allowing codes and themes to be constructed from the data. For Part 2, the approach was primarily deductive as we were interested in participants responses to particular aspects of the proposed ADHD parenting program.
To assist with data familiarization, transcripts were read several times, and initial annotations were made to record LEB’s reflections on the text. This helped identify initial codes that demonstrated the meaning participants made from their experiences. Personal reflections on the interview experience and data were recorded in LEB’s reflexive notes and discussed in weekly meetings with MT to support reflexivity. Several rounds of coding occurred in discussion with MT, whereafter codes were collated and developed into initial themes using a thematic tree. The thematic tree underwent several iterations to assist with theme construction and refinement. To enhance clarity and distinctness, the thematic tree was reviewed by GK, discussed and further refined, and assessed against the dataset to confirm the themes before being considered ready for independent review. MB and BM then examined the data and themes, engaged in further conversation with LEB, and provided theme confirmation (see Supplemental File 2 for thematic tree). Relevant quotations were chosen from the data to illustrate each theme.
Results
Objective/Aim 1: Experiences of Parenting a Child With ADHD
Three themes related to the experience of parenting children with ADHD were generated. The first theme, “I love my child but their ADHD traits are challenging,” provides insight into expressed parental warmth, dedication and attunement; parent-child attachment relationship quality; and factors that threaten a parent’s perception of their child/ren with ADHD. The second theme, “Compliance, control, and completion,” describes the dominant parenting goals described by participants. The third theme, “It’s hard, burdensome, and exhausting and I can feel like I’m alone,” provides insight into the personal impact of raising a child/children with ADHD and parent’s unmet need for ADHD-focused parenting support.
Theme 1: I Love My Child, But Their ADHD Traits Are Challenging
All participants provided responses that gave insight into the love they feel toward their child/ren with ADHD via expressions of warmth, positive regard, and dedication. For instance, participants commented: “He has a beautiful big heart. He is incredibly creative and intuitive. . . and smart and kind. . . Yeah, he is a beautiful child.” (Penny).
I mean it costs me yeah, the financial side of things has always been really, really, really hard, but I’ll keep doing it. I don’t care what debt I get into, given. . . this is the only time I’m going to have in [my son’s] life in terms of intervention and. . . getting him to develop the best skills he can. It’s this period of his life. . . not later on. It’s now, so I wanna put in that work to scaffold him so he can go on and thrive. . . (Ivy).
A few participants expressed their love for their child/ren with ADHD when describing the enjoyment they experience when they spend time with them. For example, Mary remarked her son brings her “joy”: “We just laugh and just enjoy each other’s company. . . . We’ll play a board game or something like that. We’re doing the Christmas tree together. So, we do things that are fun.” For June, this enjoyment was relatively new: “She’s hard work, but. . . as we have gone along this journey, I am starting to really enjoy my child more.”
A couple of participants described how their understanding of ADHD enabled them to respond to their child/ren’s struggles with empathy, support, and unconditional positive regard. For instance, Mila voiced that when her daughter becomes emotionally dysregulated, “I just try to stay with her so that she knows that her feelings aren’t too big for us.” Mary recalled that when her son loses things at school, “[I] don’t really see the point of punishing him. . . it’s really hard [for him] not to lose stuff. . . unless you have helped him work out exactly where and how.” All but one participant, however, admitted they found it difficult to always maintain unconditional positive regard toward their child/ren with ADHD. For instance, Sage stated, “Me and my son are really close. . . . I can get frustrated and then sometimes we yell at, at him to hurry up. . . or ‘Stop doing that,’ or ‘I’ve reminded you five times.’” June disclosed, “There’s been a lot of fighting between us.”
Participants perception of their child/ren appeared to be impacted by their child/ren’s ADHD symptoms, with the vast majority describing their child/ren’s ADHD traits in a manner that inferred that they found them upsetting. For June, this appeared to be especially the case when “they’re doing all this stuff and they’re just so dysregulated.” Over half of parents also provided information that indicated that they found their child “hard work” and their ADHD traits inconvenient, irritating and/or embarrassing. For example, Lilly shared that when her daughter is bored, “She really can’t handle it. She can’t handle going to the supermarket, she can’t handle going in the car. . . She can’t handle waiting two minutes when she’s picked up from school.” Rose called her daughter “a little tornado. You clean the house and within a blink of an eye, it’s back to being, like you can’t see the floor.” Beth shared, “I do get upset and embarrassed sometimes about how he behaves.”
Along with these sentiments, many parents expressed feeling resentment toward their child/ren accompanied with a sense of loss, sadness, or disappointment. To illustrate, Ivy confessed, “I don’t feel I’ve got. . . that parenting kind of joy and moments that I see a lot of others, of my friends get with. . . their children.” Furthermore,
[To connect with my son] . . .it has to be outside, basketball court, football, rugby. So, that’s what I’m constantly doing with him and that really pisses me off sometimes. I don’t want to do that, I really don’t. I just want him to sit the hell down and read a book.
Theme 2: Compliance, Control, and Completion
All participants described using parenting strategies with their children with ADHD aimed at ensuring task completion. All but one also described using parenting strategies aimed at gaining compliance and control. While the vast majority of participants described using a top-down parenting approach, a couple of participants indicated they employed collaborative problem-solving techniques and involved their child/ren in decision-making and strategy development. As described by Sage, “With the collaborative problem solving, it’s like trying to work out together . . . what kind of things you can do to help him and what kind of things he can do to help himself.” Just under half of the participants also described attempting to teach their child/ren skills and strategies to cope with their ADHD using a top-down approach.
The most frequently used parenting strategy, described by three quarters of parents, was the provision of frequent or persistent instructions and follow-up reminders (i.e., proactively and reactively telling child/ren what to do). As an example, Ruth described herself as a:
Bit of a micro-manager. . . . It’s the same thing every single day, but you have to constantly. . . give them a heads-up about. . . what the routine is. . . . Time to keep moving, go brush your teeth, go wash your hands. . . put your school uniform on, pack your bag. . . pack your lunchbox.
The second most common strategy, described by over half of participants, was the use of visual prompts (i.e., lists, whiteboards, timers, and clocks). For instance, Rose shared that they have a lot of “signage around the house. . . Her timetable, I created and color coded. She’s got 5 or 6 copies around the house that help her get ready.”
Over half of participants disclosed that they yell at their child/ren with ADHD, while a few disclosed that they use negative consequences to gain compliance. Descriptions of the use of negative consequences were often accompanied by information indicating their use evoked unfavorable parent-child interactions. For instance, Rose shared:
We have a blanket rule in the house, so the worst punishment she gets is loss of digital devices and sent to her room. She had lost the digital devices. She was then sent to her room. You then have to sit guard outside her room or she just doesn’t care and comes out. . . She spent the hour either hocking up as much phlegm as she could to spit on me. . . or ‘snot on me.’ And so, I was covered from the tip of my head down in whatever she could fling out of her sinuses at me.
Over half of parents also described physically assisting their child/ren with ADHD. For Mila that “sometimes involves me. . . physically dressing him.” For Mary, it involves keeping her son company while completing tasks he finds difficult:
We did do some work this morning cleaning his room together. . . which he wasn’t keen on, but I. . . [break] it down and do it in chunks. . . and engaged him in how we are going to do it. In which order. . . and then helped him. I always offer to help, to get things started. I think that’s really important having a child with ADHD. You don’t just send them off into the great unknown. . . and expect them to be able to do it.
Along with implementing strict routines and structure, participants often used reward systems as a means of promoting task completion or desired behaviors but with limited success. For example, Sage explained that when her son was younger they had:
. . . routines and charts. . . rewards systems and things like that, but he would generally. . . lose interest in getting the reward or following the routines and structure, so I’d have to try and think of a new one every [sigh] sought of month.
A few participants indicated that they try to talk to their child/ren about their emotions and what happened after an incident and a couple of participants provided insight into how they role model rupture and repair. One participant provided insight into the communication strategies she uses, and has taught her son to use, in order to protect their relationship:
We talk a lot. . . . We’ve spoken quite clearly. . . about. . . using emotional language. . . If I’m getting to the end of my tether, he will know that . . . I’m comfortable to say. . . “I’m getting really frustrated now because I asked you to do this a number of times and I just need a few moments to myself.” So, I’ll remove myself from the situation. . . He might say the same thing. . . . He [also] likes to discuss any kind of ruptures I s’pose and so there’s that opportunity for repair. (Mary)
Many participants were concerned about the impact their parenting behavior had on their child/ren; that they had received and internalized negative messages and felt frustrated, hard done by, and defensive. For example, Lilly shared she worried her son “is not getting enough positive affirmation. . . because we’re always telling him off for things.” And that her daughter “has periods where it just like escalates. . . she regularly said she wants to kill herself and hurt herself.” Over half of the participants also disclosed that their child/ren with ADHD often get upset with them. For instance, Tess shared her biggest concern was her relationship with her son: “Knowing even right now, you’re the worst parents ever.” Ivy remarked, “He does have bouts of yelling and. . . getting very frustrated with me.” Rose stated her daughter once “pulled a knife on me. She’s gone and got a hammer and come back at me.”
Theme 3: It’s Hard, Burdensome, and Exhausting, and I Can Feel Like I’m Alone
Although ADHD medication, as per Tess, “takes parenting into the realm of manageable,” all participants perceived parenting a child with ADHD to be more difficult than parenting neurotypical child/ren: “You know, parenting is already really hard, this just is like another level” (Penny). Nearly all participants described parenting their child/ren with ADHD as challenging, physically and mentally exhausting, and often stressful. For instance, Lilly reported mornings with her son with ADHD are “a nightmare in general.” Beth shared:
Sometimes he’s just so frustrating and sometimes you’re just so exhausted. . . You feel like you’re managing a lot of his stuff for him. . . It’s very tiring because he’s never off, ever. . . . Sometimes you can just get into some big power struggles. . . because you’re not understanding each other. You’re frustrated, they’re frustrated.
Over three quarters of participants described raising their child/ren with ADHD as time consuming; requiring monitoring, supervision, prompting, hands on assistance, flexibility, hypervigilance, and patience. To illustrate, Tess disclosed:
Looking back, as a toddler, even as a baby. . . I did so much with him. . . for one child that I would never, now having my other two. . . I just don’t need to do that stuff. . . . [Even now, I put his] uniforms in the box, so he doesn’t have to at least source the items, because it just adds six more things to find. . . . Sometimes he gets changed in his room. Sometimes if he is just too engrossed in something I bring the box to him. And it’s like, ‘get dressed, like right where you are, just get dressed.’ . . . I shouldn’t. . . have to do this. And I don’t want to be doing that all the time.
Furthermore, over three quarters of participants provided information that indicated parenting a child/ren with ADHD can be a constant battle. For example, Sage shared, “He’ll ask me if he can do something. . . and if my answer is, ‘No,’ he wants to know, ‘Why?’ . . . [Its exhausting] constantly debating the merits of every little decision.”
Our analysis also provided insight into the significant emotional burden that tends to accompany the task of raising children with ADHD. Along with experiencing a sense of loss or sadness, and feelings of disappointment and resentfulness (see Theme 1), all but one participant shared concerns about their child’s future. For Penny this concern was:
Because everybody else around him is neurotypical generally speaking. . . they don’t understand that his behaviour is not just being naughty. . . . I don’t feel like other people. . . treat him fairly, and I think that most people are very uncompassionate. . . . There’s still not the level of understanding that there needs to be.
When it comes to factors that increase parental burden, nearly all participants spoke about how hard it was for them to access information on ADHD following diagnosis. Penny, who had completed four manualized parenting programs, shared:
My husband and I’ve both had to. . . educate ourselves massively on [ADHD]. There isn’t a huge amount that’s formally available. . . I found it very challenging to find those resources and that support. . . . I feel like it’s a constant. . . growth piece for us and. . . on a day-to-day basis, we send each other clips from Instagram, from people that we follow that have ADHD, because we then learn. You know, they’ll release this content. . . and we’ll watch it and be like, ‘Oh my god, mind blown!’. . . I had no idea that. . . brushing your teeth was so difficult. . . So, it’s incredibly important that we’re constantly on it because as neurotypicals we cannot possibly imagine what that is like and why it happens.
Most participants discussed feeling conflicted when making parenting decisions as they were unsure what the expectations and rules should be or how much support they should provide their child/ren with ADHD. As an example, Lilly shared it is:
. . .very hard to know how much do you let your child do certain things because. . . they physically can’t help what they’re doing, and how much am I supposed to be training and trying to teach them that this is the world that they’re going to be growing up in. . . That would be my biggest challenge. . . finding a balance. . . Not trying [to] put them into. . . a neurotypical world but also understanding that they are in that world and they will need these skills, and I just need to know what the right balance is.
Most participants, including those that had previously completed one or more parenting program, also reported that traditional behavior management strategies do not work, with some parents sharing that such strategies tended to make things worse. Tess recalled:
I remember asking our friends, ‘Like what do you do with?’ And they’re like, ‘Oh, have you tried taking away his toy?’ And I was like, ‘That just makes him more angry.’ Or. . . ‘Have you tried giving him a time out?’ or ‘Have you tried. . .’ And it’s like, yes, we’ve tried but it doesn’t produce a change in behaviour whatsoever. If anything, it would exacerbate the behaviours and make him more angry and more dysregulated.
Although a very small number of parents did express confidence in their ‘behavior management’ style parenting approach, these same parents disclosed that their children struggle greatly with anxiety. In regards to typically recommended strategies, many participants reported they have limited utility; “. . . using charts and stuff [is] useless because they’ve got to remember to look at the wall or the chart in the first place” (Penny).
Nearly all participants spoke about experiencing stigma and judgement that contributed to them feeling misunderstood and isolated. June shared that although discipline issues are seen as very important, “I’ve just let go of that. Just let go of the traditional parenting things. . . . But you have outside family that doesn’t understand and just tells you you’re, you’re not disciplining them properly.” Mila spoke of the difficulty “dealing with judgment from other people or even perceived judgement. You know, there is still this really strong perception in society that ADHD is pretend and it’s just an excuse for bad behavior.”
Objective/Aim 2: Feedback on Proposed ADHD Parenting Program
Our analysis of the data collected when discussing the proposed ADHD parenting program identified one superordinate theme: “What a welcome relief.” Tess described the proposed ADHD parenting program as “really practical,” and stated, “We want them all to develop into an independent, healthy, functioning adult.” Ruth who had previously completed three parenting program felt the information contained in these programs was “generic” and stated, ”I really do think that we need sort of a bit more specific and tailored information.” Mary affirmed, “It’s a wonderful idea. Can’t wait ‘til it’s available. . . . [I] really think we need fresh, sort of compassionate and. . . neuro scientifically-based parenting support for. . . parents of kids with ADHD.” Almost half the participants also expressed thankfulness that such a program was being proposed. No negative feedback was received.
Nearly three quarters of the parents expressed the proposed program’s focus on (1) the parent-child attachment relationship, and (2) education that would facilitate understanding of the neurobiology underlying ADHD and how it affects a child from a child’s perspective, stood out to them. As per Rose, “That attachment relationship is really at the core of. . . the child’s ability to grow up into a functioning adult.’ As highlighted by Mila, “If the relationship has started to deteriorate, how can you recover from that and what sort of language can you use, and how can you sort of re-establish that core relationship?” In regard to education on ADHD, Ruth shared:
That would be helpful, absolutely. . . a general better understanding of ADHD and obviously what it actually sort of means for their child. . . because at the moment. . . any perspective I’ve got is basically. . . [from] having to like reactively. . . deal with [my son’s] issues. If I had that understanding about. . . I guess why he does what he does. . . that would be extremely helpful.
The other thing that stood out to parents was the ADHD parenting programs focus on helping them foster in their child/ren traits that adolescents and adults with ADHD have reported to be important for facilitating wellbeing, adaption and recovery. As per Sage, “The journey [from] childhood to adulthood, that probably doesn’t get as much airtime, or like. . . how are you going to move from here into the future?” Sage also shared that it is “really good” that the proposed ADHD parenting program acknowledges children with ADHD “should be involved in their own diagnosis and their own strategies. . . and then moving forward how that’s going to look for them,” while Mary highlighted the need to promote “self-advocating” and Rose highlighted the importance of providing scaffolding: “So, understanding how to do that as parent and then being able to teach that to your child so that that’s something that they can continue. . . into their adulthood is really important.”
When asked specific questions about preferences for the program delivery, all participants stated that they would prefer to attend face-to-face. As per Tess, “Face-to-face is always ideal.” Mary: “I think there’s a great benefit in parents meeting each other because they, they get it. . . and it’s often quite isolating I think. . . when there is. . . no other parent.” A couple of parents, like Lilly, however, shared it “would be very hard for us to make [a face-to-face course], but obviously we would probably prioritise it.” As per Tess, a few parents also disclosed, “Four hours for both parents to attend [face-to-face]. . . can sometimes be a bit of a challenge. . . if there was a good childcare thing then yes, I would.”
When it comes to the possibility of the program being offered online, Ivy shared, “For someone with ADHD. . . I’ve got the whole world around me that I’m taking in as well as trying to focus. . . so I know that wouldn’t benefit me.” However, several parents expressed the need for an online or at least hybrid format parenting program so that parents living in remote areas could attend. For example, June questioned, “I wonder how accessible face-to-face is, if you want to roll this program out. . .? You can definitely reach a lot more people. . . online.”
Discussion
This study aimed to understand the parenting experiences of parents of children aged 7 to 11 years with ADHD, and garner feedback on a proposed ADHD parenting program. It builds upon the qualitative data examining the impact childhood ADHD has on parents, children, and the parent-child attachment relationship. All study participants were motivated to take part in this study as they wanted to make a difference in the lives of their child/ren and other children with ADHD. While their views may not represent those of all parents who have children with ADHD, our analysis identified three inter-related, and at times contradictory, themes. The first being, “I love my child, but their ADHD traits are challenging.” This theme is consistent with previous research reporting parents love their children with ADHD, display dedication (Firmin & Phillips, 2009), and are sensitive to their needs (Mofokeng & van der Wath, 2017). However, they don’t always like their children with ADHD (Leitch et al., 2019) or experience the “joy” that tends to accompany being a parent (Peters & Jackson, 2009). This is likely because childhood ADHD traits elicit feelings of anger, frustration, and irritation (Mofokeng & van der Wath, 2017), resentment (Sikirica et al., 2015), embarrassment, incompetence, and hopelessness (Laugesen & Groenkjaer, 2015), and make it difficult for parents to maintain unconditional positive regard (Moen et al., 2014).
Our second theme, “Compliance, control, and completion,” highlights how childhood ADHD traits tend to elicit a parenting approach that is top-down and more authoritarian in nature, and aimed at task completion and gaining compliance and control. This is in keeping with prior literature (Chang & Gau, 2017) that shows parents tend to proactively and reactively use commanding and directive instructions to manage their children’s ADHD (Wirth et al., 2017), and implement structure and routine, visual prompts and rewards, often with limited success (Davis et al., 2011; Moen et al., 2014). Our study extends this understanding by highlighting that parents of children with ADHD spend the majority of their time focused on meeting the demands of daily living (i.e., task completion), and when compliance is not achieved using these top-down strategies, tend to become frustrated and yell at their children, or resort to negative consequences. This is unsurprising as compliance-focused parenting has been shown to evoke elevated parental emotional expressions, a high degree of criticism and over-involvement (Harold et al., 2013), and maladaptive, negative, angry or coercive parenting responses and tactics (Deault, 2010), while lack of compliance when children have ADHD can lead to parents using more punitive parenting approaches (Brinkman et al., 2009; Wirth et al., 2017). Furthermore, this study provides insight into how such parenting approaches may damage the parent-child attachment relationship and negatively impact child wellbeing. It also informs us that despite the evidence against yelling or harsh verbal discipline (Wang & Kenny, 2014) and maternal overcontrol (Affrunti & Ginsburg, 2012), and in support of practicing collaborative problem-solving (Heath et al., 2020), parents of children with ADHD rarely engage in this practice and instead tend to rely on a top-down authoritarian approach even when attempting to foster in their children skills and strategies.
Our third theme, “It’s hard, burdensome, and exhausting and I can feel like I’m alone,” aligns with previous parental reports that raising children with ADHD is hard work, challenging, physically and mentally exhausting (Ghosh et al., 2016; Peters & Jackson, 2009), and time consuming. Participants described how parenting children with ADHD requires a lot more effort, vigilance (monitoring), prompting, hands on assistance, flexibility, and patience, and provided insight into how childhood ADHD challenges parental self-regulatory capacity and increases parental stress. This has been noted in other studies (Brinkman & Epstein, 2011; Firmin & Phillips, 2009), and highlights the burden parents of children with ADHD often experience (Cheung et al., 2018; Leitch et al., 2019; Theule et al., 2013). In our study, participants also identified factors that increased this burden including the lack of education they received on ADHD, traditional behavior management strategies not working or making things worse (Davis et al., 2011), and the stigma surrounding ADHD (Mikami et al., 2015).
Together these three themes and the corresponding findings closely align with those reported in previous qualitative studies examining parent’s experiences of raising a child with ADHD (Corcoran et al., 2017; Theule et al., 2013; Wylock et al., 2023). They also (1) extend our current understanding by providing insight into the parenting approaches parents tend to employ, including their experiences implementing typically recommended parenting approaches, and (2) accentuate the unmet need for parental support and an ADHD-specific parenting program. One that empowers parents to understand their child’s diagnosis and respond to them effectively in an ADHD-informed manner. Lastly, they highlight the need for the parenting program to include information that equips parents to educate relatives and other community members about ADHD. Addressing this service gap is critical for the wellbeing of parents and children with ADHD.
With regards to the proposed ADHD parent education program, we identified one superordinate theme: “What a welcome relief.” Despite their struggles, all participants expressed the desire to improve their parent-child attachment relationship and raise healthy independent functioning adults with ADHD. Furthermore, in line with other studies, most expressed dissatisfaction with the education on ADHD they received (Ahmed et al., 2014; Davis et al., 2011), and felt conflicted about what the expectations and rules should be, how much discipline or support they should provide, and where the balance between offering support and fostering independence lies. They also expressed (1) a need for ADHD-specific parent training that includes an explanation of the neurobiology of ADHD and how these neurological differences affect cognition, behavior and development, (2) a willingness to engage in programs that could help them better support healthy development of their children and achieve these goals, and (3) a preference for face-to-face delivery, although the benefits of online or hybrid delivery also were discussed. These findings, along with the positive feedback received, provide evidence that supports the development of the proposed ADHD parenting program. Future research will be needed to explore how the proposed program may fit within the ecosystem of ADHD care in Australia, and the possible enablers and barriers to dissemination and implementation.
Limitations of our study include we only advertised the study on Facebook and interviewed 11 mothers, all white, from three Australian states. Four mothers had previously participated in a parent training program, while three had received parenting guidance and support from a healthcare professional. No fathers or remotely located parents participated in the study, and participation was limited to parents who could access and use the online communication system. Furthermore, most parents had sons with ADHD and we did not interview children themselves, explore the influence parental ADHD had on participant experiences, or examine whether parents used the same parenting approach with their neurotypical children. Nor did we ask parents about their background (i.e., marital status, racial/ethnic or socio-economic factors, and full mental health status), or elicit details related to the severity of children’s ADHD symptoms, diagnostic specifiers, and medication usage. Together these factors may limit our understanding of the parenting experience of fathers and other cohorts of parents, and the experience of parenting girls with ADHD. Further research is required to understand the experiences, perspectives, and unmet needs of all ADHD community members, and to determine if parents parent their children with ADHD differently to their neurotypical siblings.
As with all thematic analysis studies, as researchers we may have influenced the study findings. However, to maintain credibility and enhance the trustworthiness of the study, strategies known to promote reflexivity were employed throughout the data collection and analysis process, and two researchers joined the study to independently review the data and finalize the themes. Future research should aim to involve fathers, people from diverse cultures and backgrounds, parents living in remote areas, and parents with daughters who have ADHD, to ensure their experience of raising children with ADHD are also captured. Consideration should also be given to the impact parental ADHD has on the experiences of parents raising children with ADHD.
Conclusion
Our analysis highlighted parents of children with ADHD aged 7 to 11 years love their children and display warmth and dedication. However, due to their challenging ADHD traits, often find it difficult to maintain unconditional positive regard toward their children at all times. Our analysis also identified that parents of children with ADHD aged 7 to 11 years tend to focus on gaining compliance or control and on task completion; describe parenting their child with ADHD as being hard, challenging, and exhausting; and are dissatisfied with the education on ADHD they received. Consequently, parents overwhelmingly expressed their support for a new ADHD-focused parenting program that could provide parents with accurate information on the neurobiology underpinning ADHD, how this influences children’s cognitive and emotional development, as well as strategies that parents can use to promote secure parent-child attachment, attuned parental responsiveness, and age-appropriate development of traits that can support long-term well-being, independence, and functioning throughout life. The development and evaluation of such a program should be the focus of future research.
Supplemental Material
sj-docx-1-jad-10.1177_10870547241309526 – Supplemental material for Parents’ Experiences of Raising 7- to 11-Year-Old Children With ADHD and Perception of a Proposed Parenting Program: A Qualitative Study
Supplemental material, sj-docx-1-jad-10.1177_10870547241309526 for Parents’ Experiences of Raising 7- to 11-Year-Old Children With ADHD and Perception of a Proposed Parenting Program: A Qualitative Study by Louise E. Brown, Mary Tallon, Garth Kendall, Mark Boyes and Bronwyn Myers in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547241309526 – Supplemental material for Parents’ Experiences of Raising 7- to 11-Year-Old Children With ADHD and Perception of a Proposed Parenting Program: A Qualitative Study
Supplemental material, sj-docx-2-jad-10.1177_10870547241309526 for Parents’ Experiences of Raising 7- to 11-Year-Old Children With ADHD and Perception of a Proposed Parenting Program: A Qualitative Study by Louise E. Brown, Mary Tallon, Garth Kendall, Mark Boyes and Bronwyn Myers in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LEB was funded by a Curtin University RTP scholarship. MB is supported by the National Health and Medical Research Council, Australia (Investigator Grant 1173043).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.