
Abstract
Introduction:
Persistence in treatment is important in balancing diabetes and preventing complications. ADHD impairs quality of life and functioning in many areas of life. The aim of this study is to evaluate the possible association of ADHD and diabetes glycemic control among adults with type 2 diabetes mellitus (T2DM).
Methods:
All data were obtained from Maccabi Healthcare Services (MHS) automated databases. This retrospective cross-sectional study uses electronic medical records from the Maccabi Healthcare Services database during the years 2010 to 2020. Using a propensity score with the variables of age, gender, and duration of diabetes, we compared a group of 1,582 patients with T2DM and ADHD to 1,582 patients with T2DM and without ADHD. We used a t-test to compare continuous variables and a Mann-Whitney U test for non-parametric testing. In addition, we used multivariate logistic regression with a cutoff of several HbA1c values in T2DM patients with and without ADHD during 2019 to 2020. The proportion of patients with HbA1c values above 10%, 9%, and 8% in the group of patients with ADHD was 4.7 to 5.9 times higher than in patients without ADHD. In addition, the OR in the multivariate logistic regression was 4.2 (95% CI [2.5, 6.8]), 4.3 (95% CI [3.1, 6.1]), and 2.7 (95% CI [2.2, 3.4]) for cutoff of HbA1c of 10%, 9%, and 8%, respectively.
Conclusion:
Patients with co-morbid ADHD and T2DM have a higher incidence of poor glycemic control. The findings extend the knowledge on the relationship between ADHD and diabetes and highlight the need for further research to improve treatment.
Introduction
ADHD is one of the most common chronic psychiatric disorders in children and adolescents and often persists into adulthood (Xu et al., 2018). The diagnostic criteria include symptoms of hyperactivity, impulsivity, and inattention that occur in more than one setting and affect functioning (American Psychiatric Association, 2013). ADHD is characterized by a persistent pattern of inattention and/or hyperactivity and impulsivity that interferes with functioning in many areas of life. Notably, ADHD can impair quality of life and can lead to neglect in physical health (Barkley & Fischer, 2019; Nigg, 2013). Patients with ADHD are characterized, among other things, by managerial difficulties, which can affect the adherence to and persistence of treatment (Li et al., 2022).
Type 2 diabetes mellitus (DM) is a common metabolic disease characterized by elevated blood glucose level. It is a chronic disease and requires daily treatment to balance the blood sugar level, in order to minimize the micro and macro vascular damage and long-term complications.
Diabetes mellitus (DM) and ADHD are diagnoses whose prevalence in the population has increased in recent years (Fang et al., 2021; Polanczyk et al., 2007). In both diagnoses the treatment of the disease consists of a combination of lifestyle change and medication (Cortese, 2020).
Multifactorial risk-factor control forms the foundation of clinical care for patients with diabetes. Tight glycemic, blood-pressure, and lipid control lowers the risk of diabetes-related illness and death, especially when attained concomitantly (Cho et al., 2015; Dreiher et al., 2012). Maintaining glycemic control in T2DM requires constant attention to diet, exercise, glucose monitoring, and medications.
The co-morbidity of ADHD and T2DM may be important as the inattention and disorganization that are associated with ADHD could make it difficult for patients with co-occurrence of T2DM to adhere to treatment regimens and impact their glycemic control. Treatment persistence is essential in balancing diabetes and preventing complications. ADHD impairs quality of life and functioning in many areas of life (Landes & London, 2021). Patients with ADHD are characterized by, among other things, unrestrained eating, which can lead to overweight and managerial difficulties, which can affect the adherence to and persistence of treatment.
The association of DM and ADHD with obesity, diabetes, and hypertension has been ascertained in several studies (Chen et al., 2013; Cortese & Tessari, 2017; Landau & Pinhas-Hamiel, 2019; Vinker-Shuster et al., 2022; Xu et al., 2021). It has been shown that co-morbidity of ADHD and T1DM is associated with poor glycemic control and higher complication rates (Merzon et al., 2020; Vinker-Shuster et al., 2022).
Understanding and identifying conditions and co-morbidity that affect the quality of treatment can contribute to developing targeted interventions. This study aims to evaluate the possible association of ADHD and diabetes glycemic control among adults with type 2 diabetes in the Maccabi HMO.
Methods
The study was carried out at Maccabi Healthcare Services (MHS) in Israel, which is the nation’s second-largest health maintenance organization, covering 25% of the population in Israel. Since 1997, information on all members’ interactions (i.e., visits to outpatient clinics, hospitalizations, laboratory tests, and dispensed medications) has been downloaded daily to a central computerized database. Using this database, MHS developed and validated disease registries for major chronic diseases, including diabetes, hypertension and heart disease. The diabetes registry served as the basis for the data extracted for this study. The MHS diabetes registry has been described in detail elsewhere (Chodick et al., 2003).
Study Population
We conducted a retrospective cross-sectional study using electronic medical records from the Maccabi Health Services database. The diabetes registry at Maccabi Health Services was initiated in 1998 and includes 119,908 patients. Patients with IBD, home care, dementia, cancer, or CVA or patients without HbA1c testing in 2019 to 2020 were excluded. A total of 51,065 patients remained for research. Of these, 1,582 patients were defined as diabetics with ADHD. The definition of ADHD included patients who were diagnosed with ADHD in their medical record and in addition purchased at least twice a year during 2010 to 2020 drug for ADHD including stimulants like: methylphenidate /methylphenidate ER /Apomethylphnidate SR/focalin, ampethamine/mixed amphtamine/aderal/lisdexamphetamine XR, and non-stimulants like strattera/atomoxetine. The rest (49,483) were defined as diabetics without ADHD. The enrollment of patients to this study is shown in Figure 1.
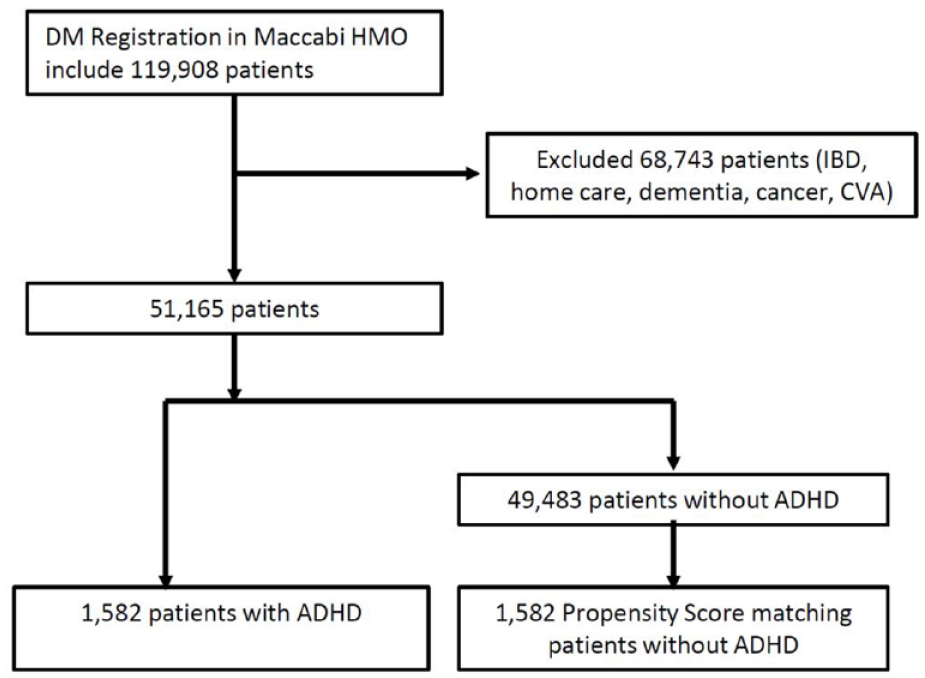
Enrollment of patients to the study.
Statistical Analysis
For the analysis, we used a propensity score matching with the variables of age, gender, and duration of diabetes. The duration of diabetes was calculated according to the age in 2020 minus the age at which diabetes was diagnosed according to the diabetes registry. We compared the clinical findings of 1,582 patients with T2DM and ADHD to 1,582 patients with T2DM and without ADHD between the years 2019 to 2020. We used a t-test for comparing continuous variables and a Mann-Whitney U test for non-parametric test. In addition, we used multivariate logistic regression with a cutoff of several HbA1c values in DM patients with and without ADHD during 2019 to 2020.
All analyses were performed using SPSS and MATLAB software.
Results
All T2DM patients were grouped according to their ADHD diagnosis; conditions under which patients were excluded from the analysis set are shown in Figure 1.
In the first box of the figure—DM registration in the Maccabi HMO includes 119,908 patients.
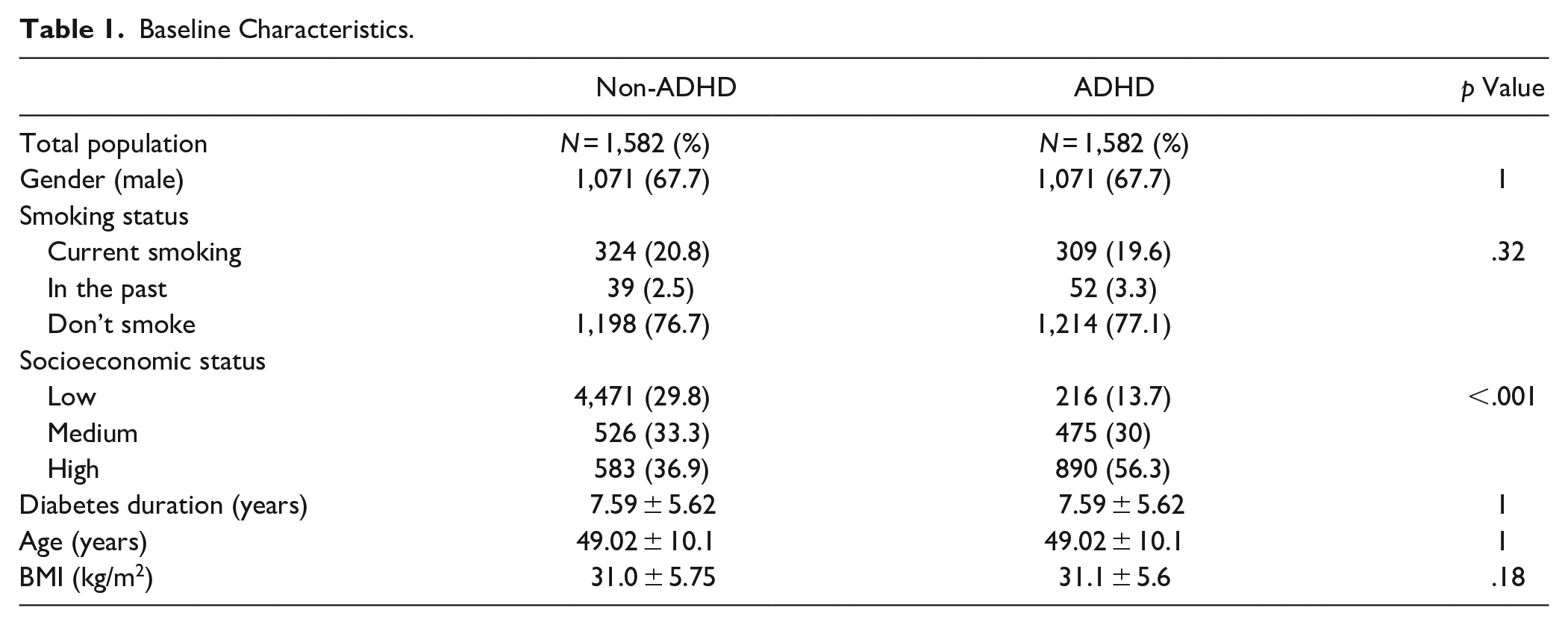
We compared the baseline characteristics of the T2DM patients with ADHD to those of T2DM patients without ADHD. The proportion of male patients was 67.7% in both groups. There was no significant difference of smoking status between the two groups, but there was a statistically significant difference in the socioeconomic status of the two groups. There was no difference in the diabetes duration. The baseline characteristics of the patients in the study are summarized in Table 1.
Baseline Characteristics.
The HbA1c was 7.26% ± 0.78 and 7.13% ± 1.5 in the non-ADHD and the ADHD group, respectively (p < .0001). Although the mean HbA1c value was less in the ADHD group, the variance was much higher. The proportion of patients with HbA1c value higher than 8% (9% or 10%) was higher in the ADHD group than in the non-ADHD group (Figure 2).
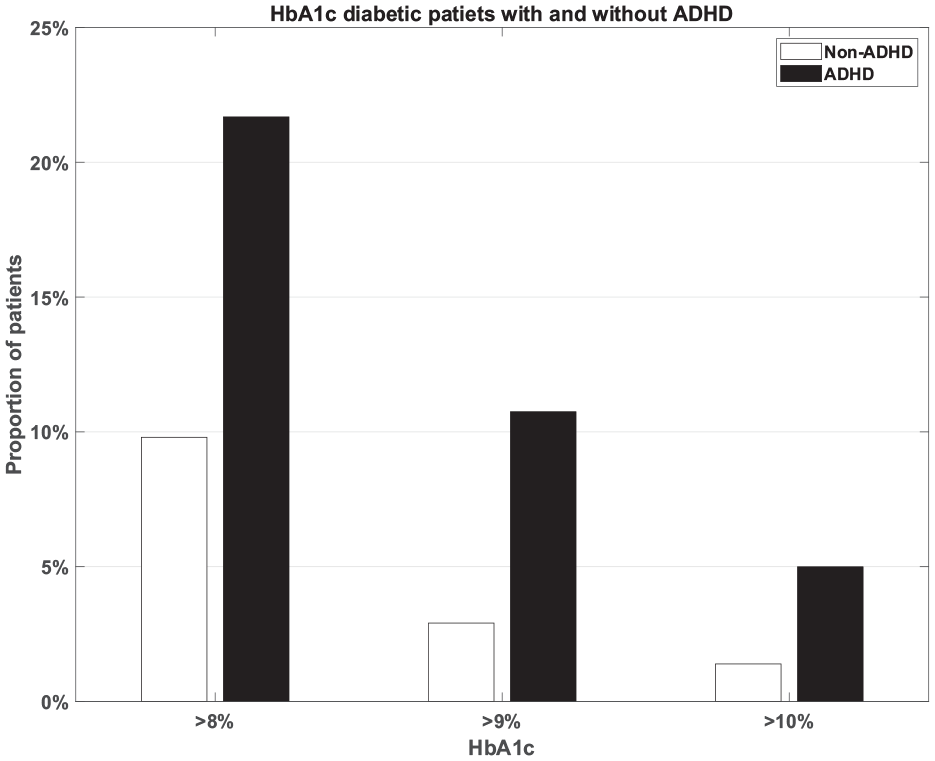
Proportion of patients with HbA1c level higher that 8%, 9%, and 10%.
The proportion of patients with HbA1c values above 10%, 9%, and 8% in the group of patients with ADHD was 4.7 to 5.9 times higher than in patients without ADHD. In order to account for the difference in socioeconomic status we conducted a multivariate logistic regression including the socioeconomic status and BMI as confounders. The OR was 4.2 (95% CI [2.5, 6.8]), 4.3 (95% CI [3.1, 6.1]), and 2.7 (95% CI [2.2, 3.4]) for cutoff of HbA1c of 10%, 9%, and 8%, respectively. Table 2 summarizes the results of the multivariate logistic regression.
The Results of Multivariate Logistic Regression.

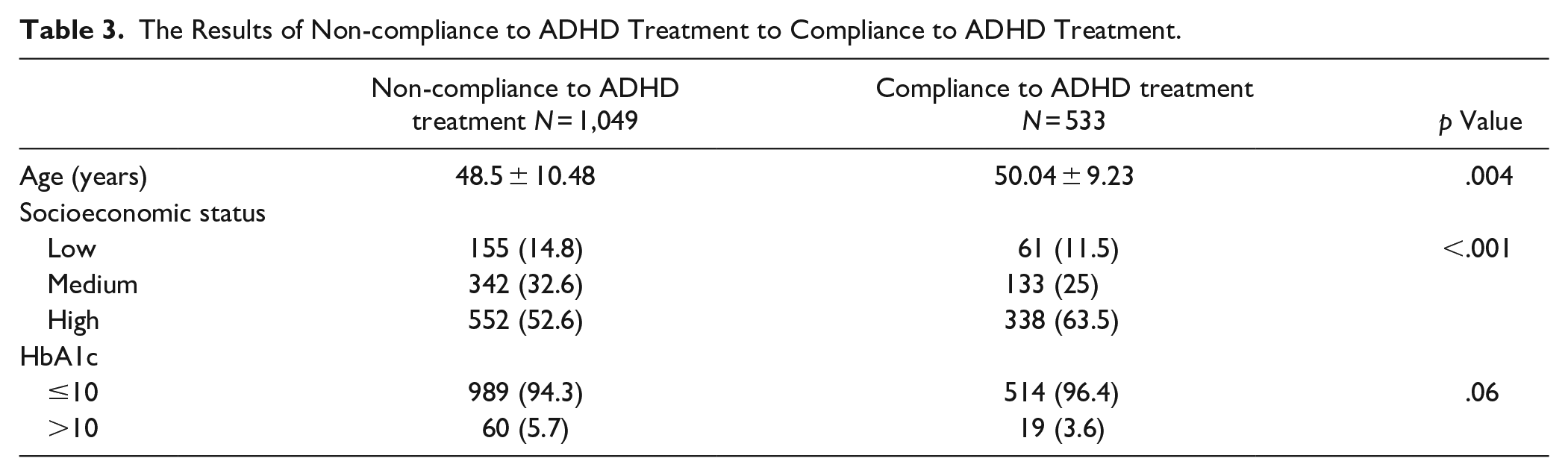
During 2020 the adherence with ADHD treatment rate was 33%. More specifically, out of 1582 patients with ADHD 1049 (66.3%) did not use any ADHD medication during 2020 and 533 patients used ADHD treatment. Comparing the ADHD patients with adherence to ADHD treatment to ADHD patients without adherence to ADHD treatment revealed that the age of patients that used ADH treatment was higher than patients that did not use ADHD medication (48.8 ± 10.48 vs. 50.04 ± 9.23, p = .04). The socioeconomic status of patients who used ADHD treatment was higher than patient that did use ADHD treatment and the rate of patients with HbA1c > 10% is higher in ADHD patients without adherence than in ADHD patients with adherence (5.7% vs. 3.5%, p = .06). Table 3 summarizes the results of the difference between patients with ADHD that used ADHD treatment to patients with ADHD that did not used ADHD treatment.
The Results of Non-compliance to ADHD Treatment to Compliance to ADHD Treatment.
Discussion and Conclusions
In this study we used Maccabi HMO medical records data to show that patients with T2DM and ADHD have a higher incidence of poor glycemic control than patients with T2DM without ADHD. The rate of uncontrolled diabetic patients with ADHD (HbA1C >8%, >9%, and >10%) was three to four times higher than in patients without ADHD. Similar results were found in patients with T1DM and ADHD (Merzon et al., 2020; Vinker-Shuster et al., 2019, 2022). In addition, we found that medication use may attenuate the negative outcome experienced by patients with DM who also have ADHD. We may speculate that the reasons that patients with ADHD have worse diabetic control relates to fact that patients with ADHD and DM have difficulties in planning and difficulties in coordinating daily tasks which make it harder for them to remember to take the medication on time and to follow the instructions regarding lab tests, doctors’ visits, and dietary guidelines. Our results indicate that patients with T2DM and ADHD may warrant special attention to their needs.
There are several limitations to this study. Although we adjusted for many potential confounding factors, we could not rule out the possibility of residual confounding from unmeasured factors. Namely, we do not have data whether in a low SES group patients with DM there was underdiagnosed ADHD.
Our finding that the mean HbA1c in patients with DM and ADHD was slightly but significantly lower than in DM patients without ADHD was initially surprising. However, the ADHD group exhibits a higher proportion of patients with HbA1c levels above 8%, 9%, or even 10% (Table 2), prompting a need for further investigation. In the non-ADHD group, HbA1c follows a normal distribution with a mean of 7.26% and a standard deviation of 0.78. Conversely, in the ADHD group, the distribution of HbA1c is not normal but rather follows a Skew Normal Distribution (positive skewness), with an average of 7.13% and a standard deviation of 1.5. Figure 3 presents the HbA1c distributions of the ADHD and non-ADHD groups. While there is a statistically significant difference between the two means, this difference is relatively small, likely influenced by the large sample size (n = 1,582). It is noteworthy that the ADHD group not only shows a higher proportion of patients with HbA1c levels above 8%, 9%, or even 10% compared to the non-ADHD group (Table 2), but also a higher proportion with HbA1c levels below 6% or even 7%. Specifically, in the ADHD group, 16% of patients have HbA1c levels below 5.7%, whereas in the non-ADHD group, this percentage is less than 1.5%.
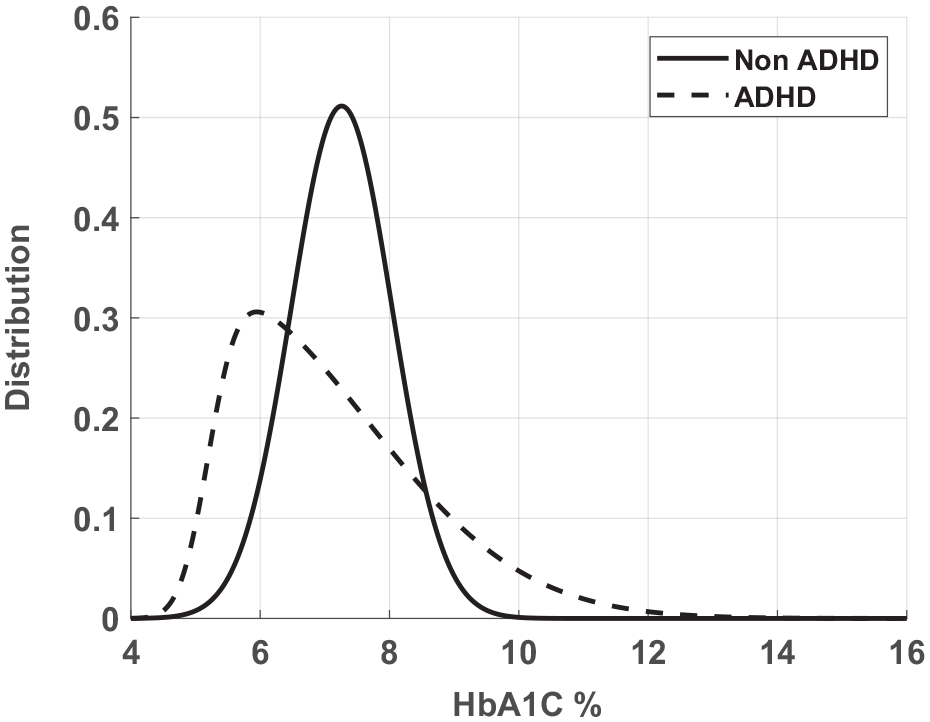
The distribution of HbA1c in the ADHD and non-ADHD groups. The non-ADHD group is normally distributed, while the non-ADHD is positively skewed.
The increased proportion of patients with HbA1c levels greater than 8% in the ADHD group is likely attributable to less effective treatment among those individuals and is the focus of this study. However, the relatively high proportion of ADHD patients with HbA1c levels less than 6% is less clear.
One possible explanation is that, despite the high specificity (99.9%) of the DM Registry used in Maccabi HMO, the specificity might be lower in individuals with ADHD, leading to a higher rate of false DM diagnoses. Another possibility is that some patients with ADHD receive intensive treatment for DM, leading to lower HbA1c levels, while others are undertreated, resulting in higher HbA1c levels. It is also possible that the ADHD group is heterogeneous, with a wide spectrum of symptoms contributing to variability in HbA1c outcomes.
Personalized treatment strategies may be key to overcoming barriers for patients with ADHD, helping them navigate the complexities of their care and providing the necessary reminders to improve adherence to treatment.
These findings extend the knowledge on the relationship between ADHD and DM and highlight the need for further research to improve treatment. Further research is needed for targeted interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Marom, Maccabi Healthcare Services Research Program, and Kahn-Sagol-Maccabi Research and Innovation Institute, Israel.
Ethical Approval
The study was approved by the institutional review board of MHS.