
Abstract
Objective:
To identify childhood psychopathological features that predict the onset of adolescent Bipolar (BD) versus Unipolar Major Depressive Disorder (UD) during adolescence.
Method:
We analyzed clinical data from 495 juveniles diagnosed with DSM-5 UD (n = 359), and BD (n = 136), using bivariate analysis and multivariate logistic regression model.
Results:
BD subjects exhibited earlier onset of any psychiatric feature compared to UD. Antecedents associated with later BD were: oppositional defiant > specific phobias > ADHD > obsessive compulsive (OCD). Antecedents selectively associated with later UD were: social anxiety and separation anxiety. Factors significantly and independently associated with later BD diagnosis were: [a] emotional dysregulation at onset of the mood disorder; [b] first depressive episode with mixed features; [c] antecedent ADHD; [d] antecedent OCD, and [e] antecedent oppositional-defiance.
Conclusion:
Identifying developmental differences in BD and UD symptoms can aid clinicians in early identification and treatment planning for bipolar disorder in youth.
Dr. Serra was a research fellow at the Pediatric Psychopharmacology and Adult ADHD Program at Massachusetts General Hospital in 2013, receiving significant knowledge from Dr. Joseph Biederman and her collaborator Dr. Janet Wozniak. Joseph Biederman was the Chief of the Clinical and Research Programs in Pediatric Psychopharmacology and Adult ADHD at MGH, he mentored several generations of researchers and physicians, working closely with junior clinical investigators who now, themselves, mentor the next generation of clinician scientists. Dr. Biederman played a crucial role in Dr. Serra’s career development. Throughout her training, she gained valuable insights into distinguishing and treating various types of pediatric mood disorders within the context of neurodevelopmental disorders, particularly attention deficit disorders. Currently, Dr. Serra coordinates a pediatric mood disorders program in Rome, Italy, with a focus on diagnosis and treatment of pediatric bipolar disorder.
Introduction
A current concern is that the prevalence of major depressive disorder has risen sharply in young people over the past decade, especially among females (Thapar et al., 2022). The annual cross-sectional US National Survey on Drug Use and Health, published in 2019, reported that the 1-year prevalence of broadly defined depression increased from 8.3% to 12.9% in 12- to 17-year-old between 2011 and 2016. The center for Disease Control (CDC) considers pediatric MDD a major public health concern and documents that even minor symptoms of MDD dramatically increase the risk for suicidal behavior, supporting efforts aimed at the identification and treatment of pediatric MDD (Center for Disease Control and Prevention, 2018). A major problem in the diagnosis and treatment of pediatric MDD is the differentiation of children suffering from bipolar forms of depression from those suffering from unipolar forms of the disorders. Considering that literature suggests that from 20% to 45% of pediatric patients presenting symptoms of MDD may progress to a bipolar disorder (Geller et al., 1994; Uchida et al., 2015; Wozniak et al., 2004), identifying which children are at risk of developing a bipolar mood disorder is a difficult tool that require a well-rounded understanding of these disorders.
The diagnosis of major depressive disorder or bipolar disorder is clinical, according to the criteria of the DSM-5 (American Psychiatric Association 2013). These diagnoses present peculiar complexities in adolescence. DSM-5 allows irritability to be considered a symptom of depression in youth. The dimension of irritability is trans-nosographic and may lead toward different outcomes (Stringaris et al., 2009) and both episodic and severe chronic irritability characterized by violent temper outbursts has been considered a core feature of pediatric mania (Serra et al., 2017). A subthreshold (hypo)manic symptomatology that does not meet the diagnostic criteria for (hypo)manic episode was found to be a frequent childhood antecedent of adult bipolar disorder (Faedda et al., 2015). Therefore, identifying those children at greater risk to develop a bipolar disorder poses unique clinical and therapeutic challenges. The presentation of a mood disorder is frequently preceded by attenuated psychopathological phenomena with childhood onset (Faedda et al., 2014; Geoffroy et al., 2013; Salvatore et al., 2014; Skjelstad et al., 2010). Early signs and symptoms preceding the onset of bipolar disorder can be identified in childhood and adolescence in 30% to 50% of bipolar adult patients (Egeland et al., 2000; Lish et al., 1994). Mood dysregulation, behavior activation, sleep disturbance, irritability, anxiety and aggression have been identified as early symptoms of BD (Duffy et al., 2010; Faedda et al., 2014; Johnson et al., 2000; Skjelstad et al., 2010). Other factors that can be identified at an early stage of life as predictors of bipolar disorder are temperamental characteristics (Kochman et al., 2005) and family history (Strober & Carlson, 1982). A large retrospective study of adult patients with mood disorders (Serra et al., 2015) have identified childhood and adolescent antecedents in more than a half of patients with adult bipolar disorder. It has also been demonstrated a significant effect of the quantitative load of antecedents not related to mood disorders (such as anxiety, substance use, eating disorders, obsessions, and compulsions) in distinguishing trajectories leading to bipolar disorder (Serra et al., 2015). Despite the methodological limitations that require further confirmation, the study made by Serra et al. (2015) had retrospectively distinguished bipolar from unipolar adult patients with high sensitivity and specificity through the analysis of first syndromic (substance use disorder and eating disorders) and non-syndromic (symptoms related to mood swings, phobias, hyperactivity, generalized anxiety, and depressive symptoms) psychopathological phenomena occurred during childhood and adolescence. Data from longitudinal and retrospective studies, studies of high-risk offspring of parents all support that childhood clinica features of irritability, fear/anxiety (Copeland et al., 2009; Ficher et al., 2010; Lavigne et al., 2015; Pine et al., 1998; Rice et al., 2017; Stringaris et al., 2009; Vidal-Ribas et al., 2016), and social phobia (Bittner et al., 2004; Kessler et al., 1999; Stein et al., 2001) precede later mood disorder. A large prospective study of children at risk have also found that separation anxiety disorder may be a key antecedent risk factor for a range of adverse psychopathological outcomes (Biderman et al., 2007). Furthermore, early-onset panic attacks had been linked to future psychopathology, including mood disorders (Goodwin et al.,2002). Interestingly, early-onset panic attacks (Kinley et al., 2011; Vàzquez et al., 2014), and separation anxiety (Brückl et al., 2007; Faedda et al., 2014; Lewinsohn et al., 1997, 2008) had been associated with later development of bipolar disorder. In contrast, early, especially generalized anxiety disorders had been investigated as an antecedent of adult unipolar depression (Ficther et al., 2010; Pine et al., 1998). Little research had included specific phobia as an anxiety measure and future studies may also need to consider the relationships of these anxiety disorders to mood disorders (Lavigne et al., 2015; Serra et al., 2015). In addition, details of the course and temporal distribution of anxiety phenomena in BD patients require further clarification (Vàzquez et al., 2014). These findings highlight the possibility of early identification of specific development pathways to early differentiate subjects with the highest risk of developing BD with the goal of avoiding potential harmful treatment and preventing the worsening of the disorder with co-morbid substance, anxiety, or behavioral problems.
The diagnosis of bipolar disorder can be challenging, especially in children and adolescents (Duffy et al., 2013). Early recognition of a bipolar trajectory in adolescents may allow to avoid inappropriate antidepressant treatment that may increase the risk of mania, mixed mood states, rapid cycles, aggressive, and suicidal behaviors (Baldessarini et al., 2005; Benazzi & Akiskal, 2008; Faedda et al., 2004). Moreover, an early diagnosis of bipolar disorder is crucial for timely treatment with mood stabilizers that often occur with a significant delay from the onset of the first syndromic episodes (Baldessarini et al., 1999; Post et al., 2010; Serra et al., 2015). Studies focusing on identifiable clinical factors at developmental stages that may confer a higher risk of evolution toward bipolar disorder are of clinical interest and may improve the neurobiological and psychopathological understanding of the disorder.
Given the need to pursue such fundamental question, we sought to identify early clinical factors that predict BD versus UD outcomes during adolescence. We hypothesized that symptoms and syndromes occurring during childhood before the onset of the first major depressive episode and psychopathological characteristics of the mood disorder at onset would effectively differentiate later emergence of diagnosable BD versus UD.
Materials and Methods
Populations
Historical and retrospective data obtained during clinical assessments were extracted from detailed clinical records of adolescents evaluated at the Mood Disorder Program of Bambino Gesù Children’s Hospital in Rome. This study sample was recruited from a Day hospital for the assessment and treatment of early-onset mood disorders. Subjects were firstly routinely screened in general outpatient clinics and referred to the Day hospital if presenting a severity of illness requiring assessment and treatment in a specialized psychiatric center. Possible referring sources include primary care doctors (pediatricians and general practitioners), secondary care (child psychiatrist in national healthcare centers) or the Bambino Gesù children’s Hospital emergency department. Included subjects were children and adolescents aged from 6 to 18 years with a diagnosis of a major affective disorder made clinically and confirmed by the Kiddie-Schedule for Affective Disorders and Schizophrenia for School-aged Children, Present, and Lifetime version (K-SADS-PL), as defined from the categorial diagnostic framework of the DSM5 criteria (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; American Psychiatric Association, 2013). Inclusion criteria include the following: Bipolar disorder I (BD-I), Bipolar disorder II (BD-II), Bipolar disorder unspecified (BD-NOS), Major depressive disorder (MDD), Persistent depressive disorder (PDD) with intermittent major depressive episodes. Subjects experiencing any mood episodes (major depression any specifiers, hypomania, or mania any specifiers) in the context of either a depressive and related disorder or a bipolar and related disorders were included. Exclusion criteria include diagnosis of substance-induced mood disorders and/or mood disorders due to another medical condition according to DSM-5. For our analysis, patients were grouped into unipolar-UD group (major depressive disorder or persistent) and bipolar-BD group (I, II, or NOS). Emotional dysregulation was identified clinically and retrospectively and defined as a clinical condition exhibited from an early age characterized by severe irritability with temper outbursts, mood lability and instability, low tolerance to frustration and low reactivity threshold, inappropriate expression of emotions with excessive intensity, and slow affective normalization with negative impacts on quality of life and social adjustment (Sesso et al 2021). Clinical evaluation was supported by psychological assessment with K-SADS PL including items from Disruptive Mood Dysregulation Disorder Oppositional Defiant Disorders.
The diagnosis of Oppositional Defiant Disorders (ODD) either sub-threshold or fully expressed was made following the K-SADS PL interview. Differential diagnosis of ODD versus mood disorder was based on the presence of chronic irritability plus argumentative/defiant behaviors or vindictiveness and/or impulsive aggressions observed outside a manic/mixed mood episode (Faraone et al., 2019).
Parents/legal representative of each patient proved written, informed consent at the clinic for potential research analysis and anonymous reporting of findings in aggregate form, in accordance with Italian legal and ethical requirements for clinical data. The study was conducted in accordance with the Declaration of Helsinki (1964). To maximize the reliability of study data, records for each subject were reviewed, and required data were summarized in structured research forms, independently by two investigators (MA and MT), working to consensus with a third (GS) to resolve even minor differences. Data were collected from January 2013 to April 2022.
Measures
Subjects were evaluated at the Day hospital during at least three visits providing a total of 9 to 10 hours of clinical assessment. All the assessments were based on detailed clinical evaluation and on semi-structured interviews performed by experienced child and adolescent psychiatrysts and psychologists. Data were systematically and consistently collected using semi-structured clinical assessments that investigate family history of psychiatric disorders, previous psychiatric symptoms and syndromes or behavioral abnormalities, with ages at their appearance, as well as their estimated severity. In addition, details of the history of mood disorder were recorded, including the sub-type of first-episode, hospitalizations, and information about suicidal behaviors. Information about the type of medication that subjects where taking at intake when they were assessed in our Day Hospital where also collected and analyzed. Clinical evaluation of the above-mentioned psychopathological history was routinely supported by the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K SADS-PL).
The K SADS-PL is a semi-structured, clinician-administered diagnostic interview was administered to subjects and to their parents or adult legal representatives separately to confirm the primary diagnosis of mood disorder and to assess comorbidities. Evaluations were routinely supplemented with information from family members or close friends, as well by available medical documentation.
In addition, depressive and manic or mixed symptoms were rated by the same experiences clinicians using the Children Depression Rating Scale (CDRS-R) and the K-SADS Mania Rating Scale (KMRS) respectively. Also, during the assessment visits, the following standard rating scales were scored: Child Depression inventory (CDI-2) for self-rating of depressive symptoms, investigator-rated Clinical Global Assessment Scale (CGAS) to evaluate the global function, Multidimensional Anxiety Scale for Children (MASC-2) to assess self-rated anxiety features, and Child Behavior Checklist for Ages 6 to 18 years (CBCL). Non suicidal self-injurious acts, suicidal ideation and suicidal behaviors were evaluated with the Columbia Suicide Severity Rating Scale (C-SSRS).
Data about complete and accurate medical and psychiatric clinical and family history were accurately entered in structured medical records.
The K-SADS-PL is a semi-structured interview that assesses current and lifetime psychopathological features and psychiatric disorders in juveniles aged 6 to 18 years according to criteria of the DSM-5. This instrument has been shown to provide reliable and valid psychiatric diagnoses in children and adolescent with a good interrater reliability (Kaufman et al., 1997). Subjects and at least one parent or legal representatives were interviewed to support the collection of all available data through the K-SADS-PL, including the onset of the first psychiatric symptoms or syndrome and the onset of the first mood episode. Psychiatric disorders were coded both as “traits” if sub-syndromal or “disorder” if meeting the criteria for the diagnosis. Diagnoses were coded by synthesizing parent and subject data.
The Children’s Depression Rating Scale-Revisited (CDRS-R) is the most widely used rating scale for assessing severity of depression in children above 6 years (Polansky). It is a 17-item semi-structured interview with a raw total score of 17 to 113 given by the sum of the scores at single items and considered positive at score of >30 (Mayes et al., 2010; Poznanski et al., 1984).
The Children’s Global Assessment Scale (C-GAS) is a scale that measures the general functioning of youths under the age of 18 years. Scores range from 1 to 100 with high scores indicating better functioning.
The Kiddie-SADS Mania Rating Scale (KMRS) is a structured interview used as a rating scale for measuring manic symptom severity in pediatric bipolar patients (Axelson et al., 2003). It has 14 items, with a raw range score of 1 to 68 (given by the sum of the scores 0–6 for single items minus 13). A total score of 12 or greater is considered indicative or clinically significant manic symptoms.
The Columbia Suicide Severity Rating scale (C-SSRS) is a suicidal ideation and behavior rating scale designed to evaluate and quantify suicide risk. It has been validated for children of ages 12 years or greater. It is used in both clinical and research settings, in adolescents as in adults. It provides definitions of suicidal ideation (SI) and suicidal attempt (SA) that are widely accepted and shared by the current research and effectively distinguishes SA from non-suicidal self-injury (NSSI). A subset of item measures inquires about suicidal ideation in the previous month and includes questions on (1) wish to be dead, (2) non-specific active suicidal thoughts, (3) suicidal thoughts with methods, (4) suicidal intent, and (5) suicidal intent with a plan. A second subset inquires about suicidal behaviors in the previous 3 months, and actual SAs, aborted or interrupted attempts are coded nominally. The timing of the suicidal behavior is recorded.
Suicidal behavior has been classified according to Posner et al. (2011) as any self-harming behavior resulting in any damage with non-zero intent to die, declared by the patient or evident from documented circumstances. For the purpose of this study, we defined the presence of “suicidal behavior” lifetime as the presence of at least one suicidal attempt.
Non-suicidal self-injury (NSSI) was systematically indagated and accurately distinguished from suicidal behavior, as defined in section III of DSM-5 (American Psychiatry Association).
The C-SSRS Screen version/recent, a brief form of the full, based on six questions is administered to all patients; if the patient presents a suicidal risk a lifetime-recent version is administered.
The Italian version of the Child Behavior Checklist for ages 6 to 18 years (CBCL-6-18) was completed by the proband and caregivers to rate behavioral and emotional problems in the study subjects. This extensively used tool provides scores with three behavior rating scales that address internalizing symptoms, externalizing symptoms, and total behavioral problems. Sub-items of these three scales include eight syndromal scales (withdrawn-depressed, somatic complaints, anxious-depression, social problems, thought problems, attention problems, rule-breaking behavior, and aggressive behavior). An overall “AAA” CBCL profile was calculated by summing scores for attention problems, aggression and anxious-depressed syndromal scales. This score is reported to be indicative of Deficient Emotional Self-Regulation (DESR), at scores of 180 to 210 (SD of 1–2), and as meeting criteria for a Dysregulation Profile (DP) at a score of >210 (>2 SD) for the sum of the three syndromal scale scores.
Children Depression Inventory 2 (CDI 2) [Kovacs 2011], one of the most used measures of self-reported depressive symptoms in infancy, was administered to patients aged 7 to 17 years and their parents. The self-report form is a 28 items assessment, while the parent report has 17 items exploring core features of depression.
Multidimensional Anxiety Scale for Children 2 (MASC 2) [March 2012] was administered to patients aged 8 to 17 years and their parents to assess for self-reported anxiety symptoms. It consists of 50-item modules that provide T-scores for six scales and four subscales considering emotional, physical, cognitive, and behavioral symptoms of anxiety. CDI2 and MASC2 were administered in 2018 after availability of the Italian version.
Analyses
Antecedent events considered were psychopathological symptoms or syndromes identified during the psychiatric anamnesis and coded with the K-SADS-PL as sub-syndromal or syndromal diagnosis other than a first mood symptom or episode, and occurring prior to the onset of the first major affective episode. Antecedents were collected and recorder during the first clinical evaluation supported with the K-SADS-PL, and prior to diagnosis with a DSM-5 BD or UD. The First mood symptoms or episode were also identified during the psychiatric anamnesis and coded with the K-SADS-PL as sub-syndromal or as first major affective episode. Medications that subjects where taking at intake were also analyzed.
Averages are means (with standard deviation [SD]) or with 95% confidence intervals (CI). We compared subjects later diagnosed as BD versus UD using contingency tables (χ2) chi square or fisher exact test if appropriate, have been used to compare prevalence rates for categorical measures, and ANOVA methods (t-test) for continuous measures.
We further evaluated factors identified preliminarily as possibly associated with BD diagnosis (at p < .05, two-tailed), using multivariate logistic regression modeling to compute odds ratios (OR) with their 95% confidence intervals. A p value of .05 or less has been considered indicative of significance. Analyses were conducted with Microsoft Office 365—Excel and IBM SPSS Statistics V26 software.
Results
Characteristics of Major Affective Disorder Study Subjects
This study sample included a total of 495 juveniles: 359 were diagnosed with unipolar depressive disorder (UD) including major depressive disorder (N = 307) or dysthymia with intermittent major depressive episodes (n = 52) and 136 diagnosed with bipolar disorder (BD) type I (27), II (16), or NAS (93) (Table 1).
Characteristics of Major Affective Disorder Study Subjects.
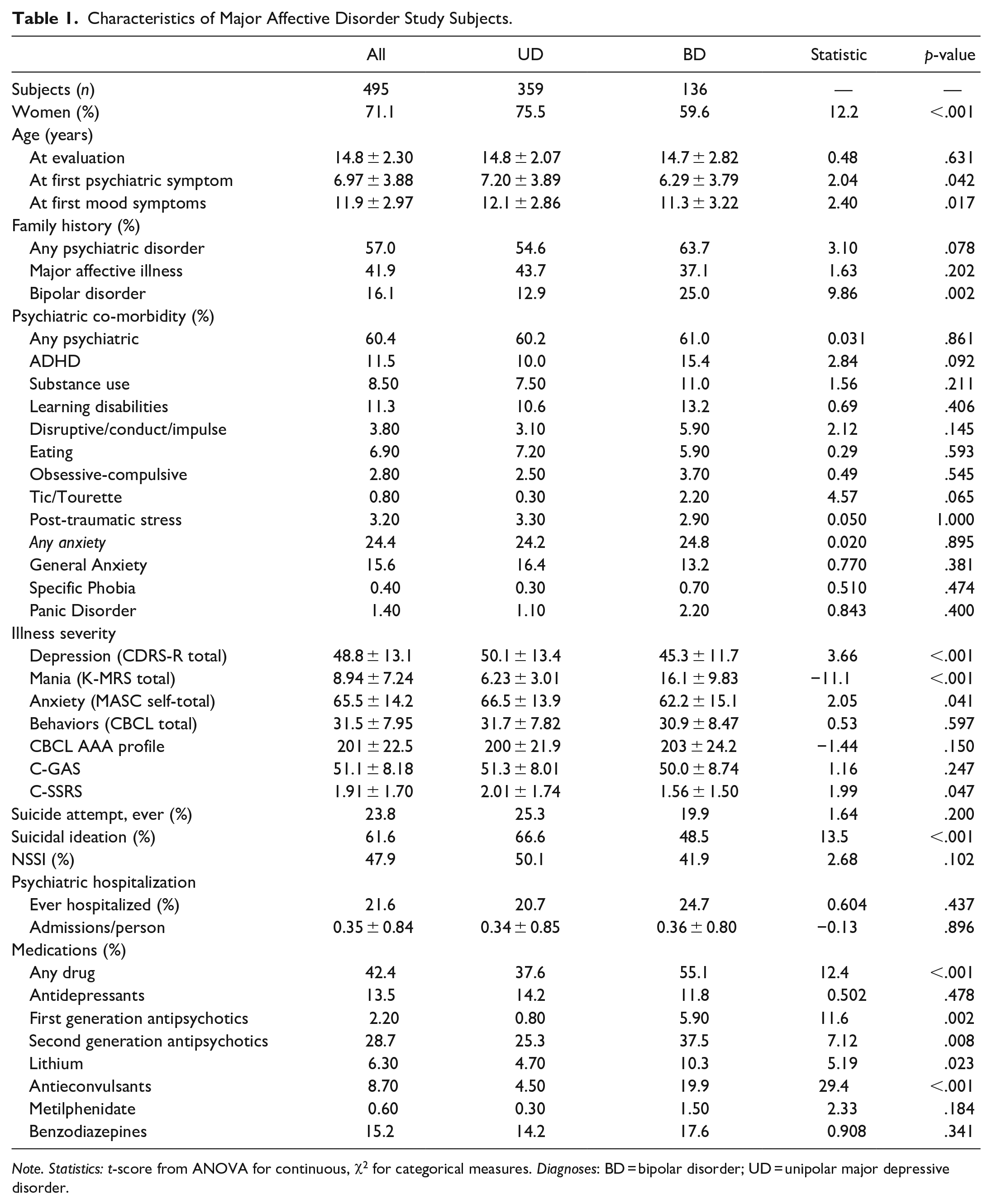
Note. Statistics: t-score from ANOVA for continuous, χ2 for categorical measures. Diagnoses: BD = bipolar disorder; UD = unipolar major depressive disorder.
The average age at assessment was 14.8 ± 2.30 years with no differences between the two groups. Among the 495 patients, 352 (71.1%) were females. There was a significant higher prevalence of females among UD (75.5%) versus BD (59.6%, p < .001, Table 1).
Psychiatric symptoms and syndromes other than mood disorders were identified as occurring for the first time at a mean age of 6.97 ± 3.88 years, and significantly earlier in BD vs. UD subjects (6.29 ± 3.79 years vs. 7.20 ± 3.89 years; p = .042). The average age at first mood symptoms or episode was 11.9 ± 2.97 years with earlier onset in BD rather than UD (BD 11.3 ± 3.22 years vs. UD 12.16 ± 2.86 years; p = .017, Table 1).
Family history of any psychiatric illness was identified in 57% of the subjects, with similar prevalence among the two groups. Family history for unipolar depression was identified in 41.9 % of subjects with no statistically significant difference between the two groups. Instead, family history of bipolar disorder was strikingly more prevalent in the BD subjects rather UD subjects (BD 25.0% vs. UD 12.9%, p = .002, Table 1).
More than half of the subjecst (60.4%) had at least one comorbid psychiatric disorder, with no differences between the two groups. The most frequent comorbidity were anxiety disorders diagnosed in a quarter of the sample (24.4%), followed by ADHD (11.5%) and learning disabilities (11.3%). Comorbidities were not significantly different among the two groups, but there was a trend toward a greater prevalence of ADHD in BD subjects (Table 1).
Severity of the index depressive episode was greater in the UD versus BD subjects (CDRS-R total score in UD 50.1 ± 13.4 vs. BD 45.3 ± 11.7; p > .001). As expected, manic symptoms rated by K-MRS scale were clinically significant greater in the BD versus UD (BD 16.1 ± 9.83 vs. UD 6.23 ± 3.01; p < .001). Anxiety symptoms, as measured by MASC self-rated scale, were greater among UD patients (UD 66.6 ± 13.9 vs. BD 62.3 ± 15.1; p = .041). CBCL total score showed similar severity among the two groups. The CBCL AAA index of the total sample was 201 ± 22.5, and indicative of Deficient Emotional Self-Regulation (DESR) both in UD and BD subjects. Subjects were considered to have significant impairment of global functioning as indicated by a mean C-GAS score of 51.8, with no significant difference between the two groups (Teble 1).
At least one lifetime suicide attempt was reported by 23.8% of subjects with no statistically significant differences between the two groups. In addition, more than half of the population (61.6%) reported suicidal ideation, which was more prevalent in UD subjects (UD 66.6% versus BD 48.5 % respectively, p < .001). Suicidal ideation was also more severe in UD versus BD as indicated by a greater C-SSRS screening version mean score (2.01 ± 1.74 vs. 1.56 ± 1.50, p = .047). Non suicidal self-injury (NSSI) was also common in about half the population (47.9%) with no significant differences between the two groups (Table 1).
More than twenty percent of the subjects (21.6%) were hospitalized in an acute psychiatric unit at least once for their psychiatric disorder, with an average of 0.35 ± 0.84 admissions per subject, similarly among UD and BD (Table 1).
Forty-two percent of the total sample (N = 210) was taking psychotropic medications at intake, significantly more frequently among BD than UD (55.1% vs. 37.6%, p < .001). Fifty-one subjects were taking antidepressants, with no differences between BD versus US subjects; 153 subjects (30% of the total sample) were taking antipsychotics, significantly more frequently among BD versus UD (respectively 5.90% vs. 0.80%, p = .002 were taking first generation antipsychotics, and 37.5% vs. 25.3%, p = .008 were taking second generation antipsychotics); 33 subjects (15% of the total sample) were taking lithium or anticonvulsant, significantly more frequently among BD versus UD (respectively 10.3% vs. 4.70%, p = .023 was taking lithium, and 19.9% vs. 4.50%, p < .001 was taking anticonvulsants). Only few subjects were taking metilphenidate at intake (three subjects, 0.6% of the total sample, Table 1).
Antecedent Psychiatric Symptoms and Syndromes in BD Versus UD, Bivariate Analysis
Clinical antecedents significantly more prevalent among subjects later diagnosed with BD than UD, ranked by BD/UD risk-ratio as: oppositional-defiant ( >2.92-times more with BD; p < .001) > specific phobias (>2.66-times more with BD, p = .021) > ADHD (>2.63-times more with BD, p < .001) > obsessive compulsive (<1.80-times more with BD, p = .015). On the contrary, factors significantly more prevalent among subjects later diagnosed with UD than BD, ranked by UD/BD risk-ratio as: social anxiety (>4.08-times more with UD, p = .002) > separation anxiety (>1.81-times more with UD, p = .029, Table 2).
Prevalence of Antecedents of Mood Disorders.
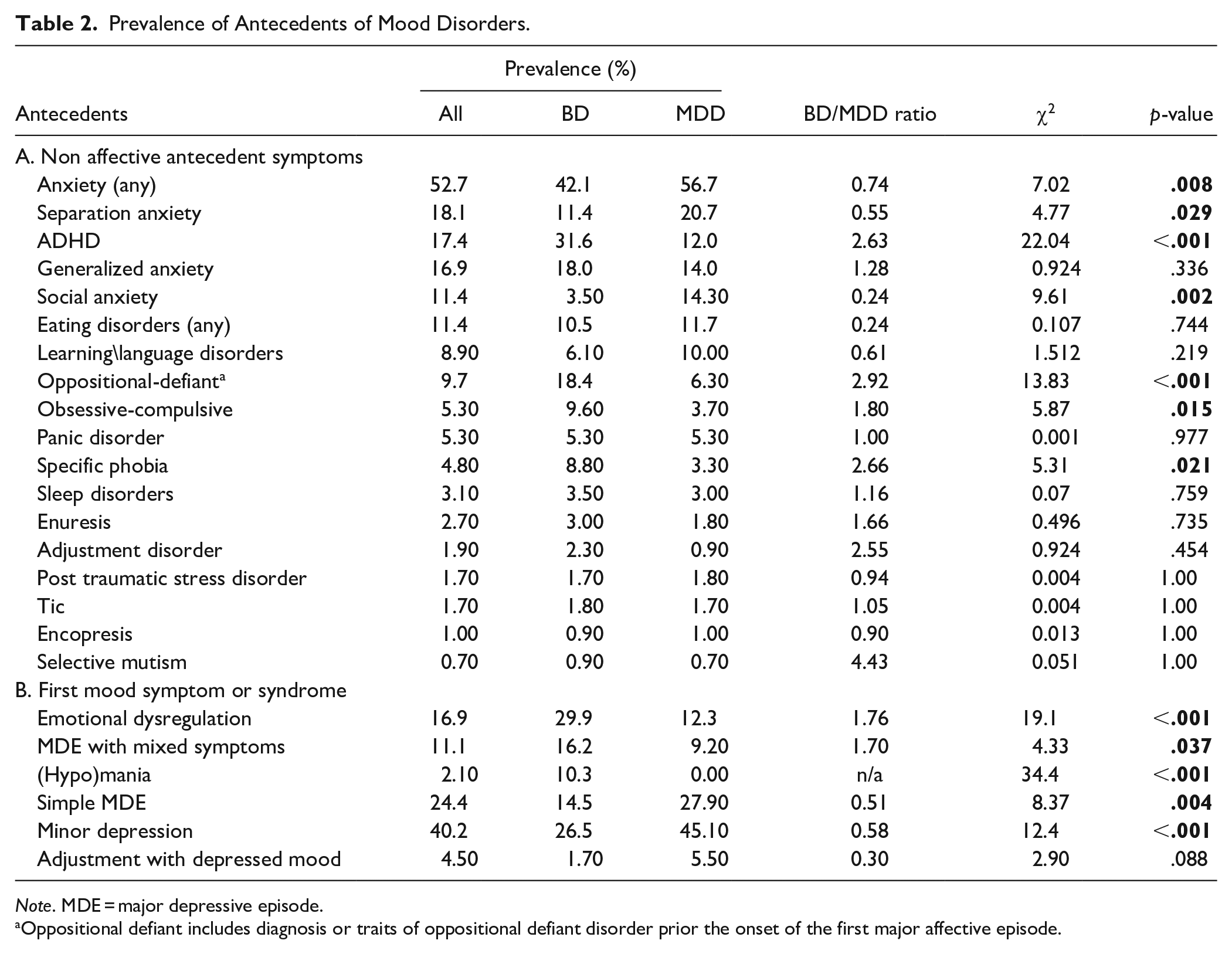
Note. MDE = major depressive episode.
Oppositional defiant includes diagnosis or traits of oppositional defiant disorder prior the onset of the first major affective episode.
Clinical Features of First Mood Episode in BD versus UD, Bivariate Analysis
First affective symptoms or episodes significantly more prevalent among subjects later diagnosed with BD than UD, ranked by BD/UD risk-ratio were emotional dysregulation (>1.76-times more with BD, p < .001) and first major depressive episode with mixed symptoms (<1.70-times more with BD, p = .037).
In contrast, subthreshold depressive symptoms and a simple major depressive episode at onset were significantly more associated with later development of UD than of BD (respectively UD/BD risk ratio 1.70, p < .001 and UD/BD risk ratio 1.92, p = .004; Tabe 2).
As expected, symptoms of (hypo)mania at onset were identified only in BD subjects. Adjustment disorder with depressed mood was identified at MDD onset in a minority of youth (4.5%), with no statistical difference among the two groups; (see Table 2).
Multivariate Logistic Regression Model
We tested for independent and significant association of antecedent psychpathological conditions, overall, before diagnosis of BD versus US. Factors significanlty and selectively associated with later BD diagnosis were: [a] emotional dysregulation at onset of the mood disorder (OR = 2.70; 95% CI [1.45, 5.02]); [b] first major depressive episode with mixed features (OR = 2.63; 95% CI [1.31, 5.28]); [c] antecedent ADHD (OR = 2.21; 95% CI [1.15, 4.27]); [d] antecedent obsessive-compulsive symptoms (OR = 2.93; 95% CI [1.06, 8.06]); and [e] antecedent oppositional-defiance symptoms or diagnosis before the onset of the first major affective episode (OR = 2.30; 95% CI [1.04, 5.11]; Table 3).
Logistic Regression Model.
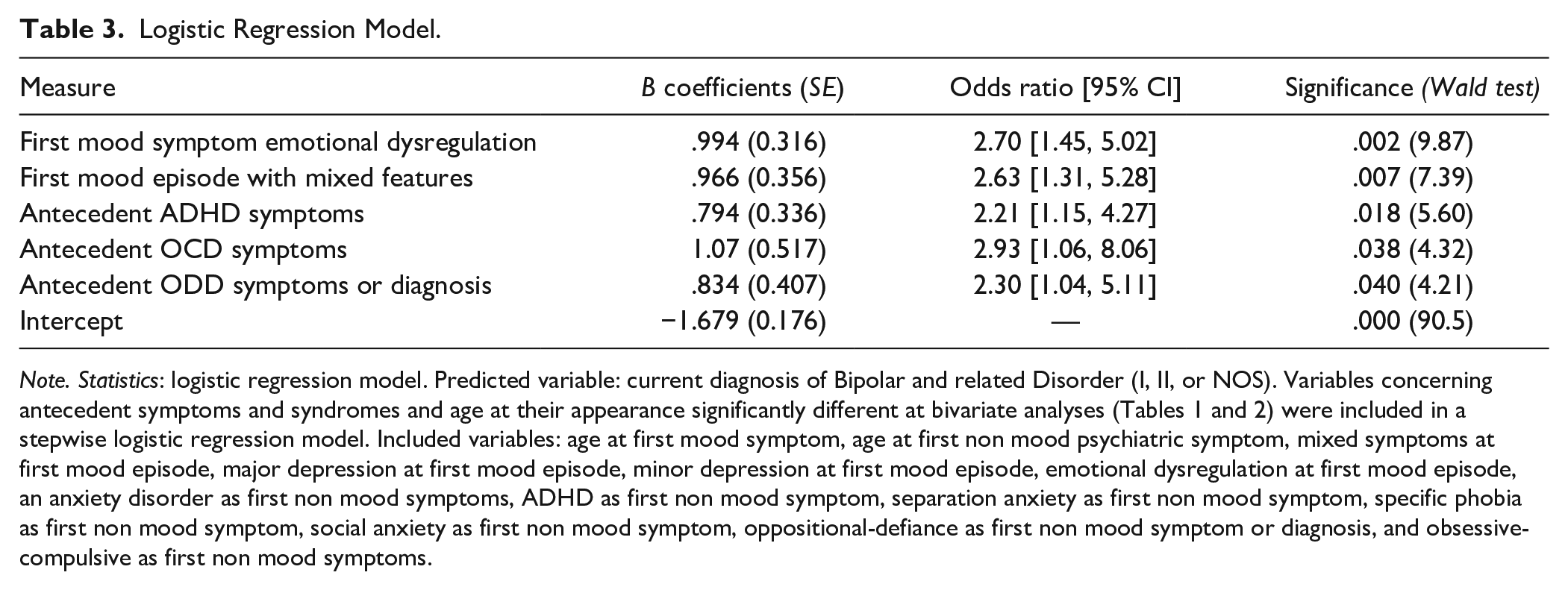
Note. Statistics: logistic regression model. Predicted variable: current diagnosis of Bipolar and related Disorder (I, II, or NOS). Variables concerning antecedent symptoms and syndromes and age at their appearance significantly different at bivariate analyses (Tables 1 and 2) were included in a stepwise logistic regression model. Included variables: age at first mood symptom, age at first non mood psychiatric symptom, mixed symptoms at first mood episode, major depression at first mood episode, minor depression at first mood episode, emotional dysregulation at first mood episode, an anxiety disorder as first non mood symptoms, ADHD as first non mood symptom, separation anxiety as first non mood symptom, specific phobia as first non mood symptom, social anxiety as first non mood symptom, oppositional-defiance as first non mood symptom or diagnosis, and obsessive-compulsive as first non mood symptoms.
Discussion
In the present study, we identified demographic and clinical differences between BD and UD adolescent subjects, and retrospectively identified childhhood psychopathological features as predictors for later development of BD versus UD during adolescence.
Subjects diagnosed with UD were more likely to be women compared to BD subjects (UD 75.5% vs. BD 59.6%, p < .001, Table 1), more likely to have a more severe current depressive episode (CDRS total score UD 50.1 ± 13.4 vs. BD 45.3 ± 11.7, p < .001, Table 1), with a greater comorbid self-rated anxiety score (respectively MASC total score UD 66.5 ± 13.9 vs. BD 62.2 ± 15.1, p < .041, Table 1). UD subjects were also more likely to have suicidal ideation (UD 66.6% vs. BD 48.5%, p < .001, Table 1) with an average greater score at the C-SSRS screening version (C-SSRS screening version score UD 2.01 ± 1.74 vs. BD 1.56 ± 1.50, p < .001, Table 1).
Subjects diagnosed with a BD were more likely to be male, younger at onset of the first psychopathological manifestations and of the first appearance of mood symptoms or episode (respectively 6.29 ± 3.79 years vs. 7.20 ± 3.89 years; p = .042, and BD 11.3 ± 3.22 years vs. UD 12.16 ± 2.86 years; p = .017). Also, BD subjects were more likely to have a family history of BD (BD 25% vs. UD 12.9%, p = .002, Table 1), and tautologically to have a greater K-MRS total score and to be treated with antipsychotis and mood stabilizers (see Table 1).
Comorbidity rates was 60.4% for the whole sample, with no differences between the two groups. The most frequent comorbidity were anxiety disorders diagnosed in a quarter of the sample (24.4%), followed by ADHD (11.5%) and learning disabilities (11.3%).
Rates of comorbid ADHD was remarkably lower than reported in several studies (Angold et al 1999; Biederman et al., 1996). This finding mith be related to the clinical profile of patients enrolled in our mood disorder program, as they are predominantly referred when exhibiting a severe mood disorder, frequently with critical suicidal ideation. For this reason, the primary clinical outcome of our program is stabilization of mood and recuction of suicidal risk, postponing a more detailed evaluation of the indications for a stimulant treatment for ADHD to a period of mood stability. Furthermore, individuals with a diagnosis of ADHD and a comorbid mood disorder of mild to moderate severity, are routinely referred to a specific diagnostic and treatment program for ADHD in our hospital. Also, in line with previous studies, ADHD might be underdiagnosed and undertreated in Italy, especially compared to north European countries and US (Donfrancesco & Loprieno, 2015). However, despite these considerations, the rationale behind the lower prevalence of ADHD in our dataset remains uncertain, and further exploration are warranted to better understand the factors contributing to this observation.
The findings of more severe depressive symptomatology and more suicidal ideation among UD versus BD subjects, and no differences in the number of suicide attempts between the two groups call for comments as not fully supported by the extant literature on adolescent mood disorders (De Crescenzo et al., 2017; Patel et al., 2020; Serra et al., 2022; Uchida et al., 2015).
Findings on suicidal ideation more prevalent among UD versus BD are consistent with the results from a recent meta-analysis reporting that a primary diagnosis of UD increases the likelihood of suicidal ideations by 18% compared to BD (Patel et al., 2020). In contrast, several previous research reported a significantly greater risk of suicide and suicide attempts in BD compared to MDD during both adult and adolescent ages (Brent et al., 1998; De Crescenzo et al., 2017; Lewinsohn et al., 2003), and some reviews reported that very severe depressive episodes and suicidal ideation are more prevalent among BD and are considered important clinical factors to early differentiate bipolar versus unipolar depression and for prediction of manic switches from MDD to BD (Uchida et al., 2015).
This discrepancy observed in the current literature and reported in the present clinical sample might be explained by uncertainty about the future course of illnesses presenting as “depression” in children and adolescents. Indeed, there is a high rate (20%–45%) of change of diagnosis from MDD to BD among of juveniles initially meeting diagnostic criteria for MDD, based on emergence of hypomanic, manic, or mixed states, sometimes during treatment with an antidepressant or other mood-elevating medicine (Baldessarini et al., 2013; Faedda et al., 2015). Also, severe major depressive episodes during juvenile ages are frequently characterized by the presence of subthreshold manic or mixed symptoms such as mood lability, severe irritability, and racing thoughts both in subjects nominally diagnosed with either BD or MDD (Serra et al., 2021). Indeed, most cases of juvenile mood disorders, including those in our sample, appear to be distributed on a spectrum and longitudinal observation sufficient to allow differential diagnosis between single episode or recurrent depression versus fully expressed bipolar disorder at the moment is not available. It follows that the present results may underestimate the ratio of suicide attempt rates among adolescents with BD versus UD by overestimating the rate among subjects diagnosed with UD. Higher risk of suicide attempts in both juveniles and adults diagnosed with BD than with UD might in part arise from manic-depressive mixed states, nominally diagnosed as major depressive disorder with mixed symptoms in this sample, as characterized by depressed mood marked by irritability, agitation, racing thoughts, greater tendency to act, especially impulsively, but not meeting neither DSM-5 criteria for a Bipolar Disorder.
Overall, there were notable differences in the developmental pattern of symptoms between the two groups. Generally, our findings indicate that the first signs and symptoms of mood disorders can begin in early childhood, manifesting itself in children at the beginning of life and may have an insidious onset. Consistent with previous studies (Serra et al., 2015; Tondo et al., 2010; Uchida et al., 2015; Wozniak et al., 2004), we found an earlier age-at-onset of both antecedent symptoms and of first-lifetime major depressive episodes among BD compared to UD cases (see Table 1). Of note, on average BD patients exhibit initial psychiatric symptoms and first major depressive episode at a younger age, approximately one year earlier than UD patients (Table 1). To date, some researchers have identified several potential contributors to the earlier onset of bipolar disorder. First, numerous studies have demonstrated that genetic factors might play a more pronounced role in BD that in UD, contributing to the onset and course of illness. Interestingly, accumulating body of evidence indicates that genetic variations linked with dysfunctional neurodevelopmental pathways may be implicated in the underlying pathophysiology of at least a subset of individuals with BD, particularly those with an early onset of illness (Kloiber et al., 2020). Some authors also proposed that early-onset BD may comprise a neurodevelopmental subtype of the disorder with a more pernicious illness course than those with later-onset BD (Baldessarini et al., 2012; Holtzman et al., 2015; Zhang et al., 2016).
Consistently with previous studies (Geller et al., 1994; Wozniak et al., 2004), our data also confirmed that family history of bipolar disorder is significantly more prevalent among BD subjects compared with UD. On the contrary, the prevalence of family history for major depressive disorder and other psychiatric illness did not differ between the two groups. Our results confirm previous hypothesis suggesting that early onset BD may represents a specific phenotype of BD associated with higher familial loading and more severity course of illness (Birmaher et al.,2014).
More than half of the total sample (52.7%) had symptoms of anxiety emerging before the onset of the first affective episode, with greater prevalence among UD versus BD (56.7% vs. 42.1%, p = .008; Table 2). Anxiety was the most common initial psychopathological phenomena in the overall population, supporting the hypothesis that anxiety disorders are particularly likely to precede mood disorders with early onset age. A longitudinal study carried out by Fichter et al. (2010) showed that the transition from anxiety to depressive syndromes was more likely than the reverse (Fichter et al., 2010).
Focusing on the different subtypes of anxiety, we found that social anxiety was four-times more likely to precede the onset of unipolar versus bipolar disorder (UD/BD ratio = 4.08, p = .002; Table 2). This is consistent with previous literature suggesting that social phobia is a significant risk factor for subsequent depression (Alpert et al., 1994; Bittner et al., 2004; Stein et al., 2001). Social anxiety disorder is reported to be the most common comorbid anxiety disorder among patients with depressive disorders (Kessler et al., 1999; Stein et al., 1998), occurring many years prior to the onset of depression. Indeed, patients with social anxiety disorder often have negative self-perceptions, low self-esteem, and others negative beliefs that are often identified in patients with major depression as well. Given the distinct nature of symptoms bipolar disorder, although social anxiety disorder may co-occur with bipolar depression, the predictive pattern might not be the same as those observed with unipolar depression.
Also separation anxiety was found to precede the development of unipolar disorder twice as commonly than bipolar disorder (UD/BD ratio = 1.81, p = .029; Table 2). Consistently to our findings, longitudinal studies have found associations between childhood separation anxiety disorder and the subsequent development of major depressive disorder in life (Brückl et al., 2007; Lewinsohn et al., 2008). Biederman et al. (2007) suggested that separation anxiety disorder may also help identifying a group of children at very high risk for a range of psychiatric disorders and with a less favorable outcomes.
On the opposite, consistently with restrospective studies differentiating juvenile antecedents of adult bipolar versus major depressive disorder (Serra et al., 2015), antecedent specific phobias was more than two-times more prevalent among BD than UD subjects.
Other antecedent non affective symptoms or syndromes found two-to-three-times more prevalent in subjects later developing BD versus UD were ADHD, oppositional defiant symptoms or diagnosis, and obsessive compulsive symptoms (Table 2).
Examnining the initial mood symptoms or syndrome subtypes, we found that a first major depressive episode with mixed symptoms was more prevalent in youth with BD compared to UD. This findings is in line with previous research (Wozniak et al., 2004). So far, many studies have suggested that illness onset in pediatric bipolar patients have a less common presentation with “the classical” euphoria-like symptoms and is more often characterized by irritability, polarity shifts, and mixed symptoms (Goldstein & Birmaher, 2012; Janiri et al., 2021). In our population, BD patients were 1.7 times more likely to exhibit a first major depressive episode with mixed features than UD patients (BD/UD ratio = 1.70, p = .037, Table 2). Our results also indicate that bipolar patients were 1.8-times more likely to have an onset of the mood disorder with emotional dysregulation compared to unipolar subjects (BD/UD ratio = 1.76, p < .001, Table 2). Consistently with our findings, retrospective studies have found that irritability and mood lability may be the predominant psychopathological features of pediatric bipolar disorder at onset (Serra et al., 2017). The significant higher prevalence of mixed features and emotional dysregulation at the mood disorder onset in bipolar patients may suggest a role of these clinical features as potentially meaningful predictors on the future development of a fully expressed bipolar disorder. On the contrary, UD patients were more likely to present a simple MDE (UD/BD ratio = 1.92, p = .004, Table 2) or to present mild depressive symptoms (the so called “minor depression”; UD/BD ratio = 1.70, p < .001, Table 2) at onset of the mood disorders, showing a general less variability of clinical manifestations compared to BD. Previous studies (Hill et al., 2014; Klein et al., 2009; Uchida et al., 2018) have suggested that subsyndromal forms of depression, including isolated negative or irritable mood, loss of interest, and negative selftalk, may predict the future development of a fully expressed major depressive disorder.
In the logistic regression model, some clinical features arising before the onset of the mood disorder or characteristics of the first mood episode were found to be significantly and independently associated with later BD diagnosis, including: [a] emotional dysregulation at onset of the mood disorder; [b] first mood episode with mixed features; [c] antecedent ADHD; [d] antecedent obsessive-compulsive symptoms; and [e] antecedent oppositional-defiance symptoms or diagnosis before the onset of the first major affective episode (Table 3).
There is a broad literature from pediatric and adult studies documenting a high and bidirectional overlap between bipolar disorder and ADHD (Biederman et al., 2003, 2004; Biederman, Faraone, et al., 2000; Biederman, Mick, et al., 2000; Sachs et al., 2000). A study conducted by Biederman et al. (2009) also found that the presence of ADHD represents a substantial risk factor for children and adolescents with unipolar depression to switch to bipolar disorder over time.
Also, while previous research (Amerio et al., 2016; Angst et al., 2005; Krüger et al., 1995) has well documented the comorbidity between obsessive compulsive disorder and bipolar disorder, the long-term relationship between these disorders has rarely been investigated. Notably, Cederlöf et al. (2015) conducted a study revealing that subjects with obsessive-compulsive disorder had a 13-fold increased risk of developing BD. This finding suggests that the presence of obsessive-compulsive disorder may be an indipendendet risk factor for the later development of BD. Additionally, another study (Masi et al., 2001) demonstrated that OCD symptoms often precede the onset of BD. Oppositional defiant disorder symptoms or diagnosis at onset were also strongly associated with later development of BD. This is consistent with previous findings showing that conduct/oppositional defiant disorder in childhood preceded adult bipolar disorder (Kim-Cohen et al., 2003). Interestingly, another study found that the coexistence of conduct disorder and/or oppositional defiant disorder as comorbidities of ADHD increased the risk of later bipolar disorder compared to ADHD alone (Biederman et al., 2008).
The present findings suggest that the evaluation of a major mood disorder during juvenile age should always include a detailed collection of the previous psychopatological history. Factors like neurodevelopmental disorders, early antecedent non affective symptoms and syndromes, toghether with their age at onset, family history of psychiatric disorders and characteristics of the first major affective episode should be always carefully collected during the assessment of an adolescent presenting to a psychiatric clinical service for a major mood disorder. Antecedents factors should be taken into account when formulating the diagnosis and might drive pharmatherapeutic decisions in kids at high risk for developing biplar disorder.
Limitations
The average age at evaluation and diagnosis with bipolar or major depressive disorder was 14.8 years and this study lacks information about the longitudinal follow-up of subjects after the initial diagnosis of a major mood disorder. Given that from 20% to 45% of adolescents diagnosed with a major depressive disorder might progress to a bipolar disorder during late adolescence or young adulthood, our findings might potentially underestimate the difference between antecedents of BD versus UD. Some differences identified in this report may be more significant than what the study has reported. Antecedent events and clinical factors associated with the outcome diagnoses of BD or UD were investigate retrospectively based on medical records. However, all symptoms were assessed through the K-SADS interviews with both parents and adolescent and supported by medical records of previous evaluations/diagnosis.
Finally, this sample was selected from patients referred to a third-level center for severe diseases. As a result, the characteristic of our study population may not be fully representative of the general population, especially regarding the ADHD comorbid rates.
Conclusions
The findings from this study may be useful to clinicians in the early recognition of patients at high risk for treatment emergent mania when treated with antidepressants. Despite the emerging studies focusing on clinical predictors, questions remain as to which clinical characteristics of depression should alert clinicians to the likelihood of bipolar depression. Family history of bipolar disorder, earlier onset of any type of psychopatological symptoms, antecented ADHD, OCD, specific phobias, and ODD are all clinical features arising before the onset of the first major affective episode that can help distinguishing youths with bipolar versus major depressive disorder.
Future Purposes
Despite the numerous studies focusing on the identification of psychiatric, sociodemographic, and psychosocial factors related to suicide risk, there are still significant gaps in our knowledge of reliable risk factors for suicide in adolescents (Glenn et al., 2014). There is little research focusing on the role of antecedent psychopathological trajectories related to suicide risk. Future studies should investigate psychopathological antecedents in childhood also in relation to the risk of suicidal behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (grant GR-2018-12367476) from Italian Ministry of Health (to GS), which had no involvement with the design, analysis, or reporting of the study. This work was supported also by the Italian Ministry of Health with Current Research funds.