
Abstract
Objectives:
Children with ADHD commonly exhibit sleep disturbances, but there is limited knowledge about how sleep and sleep timing are associated with cognitive dysfunction in children with ADHD.
Methods:
Participants were 350 children aged 5 to 12 years diagnosed with ADHD. Three sleep-related constructs—time in bed, social jetlag (i.e., discrepancy in sleep timing pattern between school nights and weekend nights), and sleep disturbances were measured using a caregiver-report questionnaire. Linear regression models assessed the associations between sleep-related constructs and cognitive performance.
Results:
After adjustment for sociodemographic variables, there were few associations between time in bed or sleep disturbances and cognitive performance, however, greater social jetlag was negatively associated with processing speed (β = −.20, 95% CI [−0.35, −0.06]), visually-based reasoning (β = −.13, 95% CI [−0.27, 0.00]), and language-based reasoning (β = −.22, 95% CI [−0.36, −0.08]); all p < .05).
Conclusion:
Social jetlag, but not time in bed or disturbances, was associated with lower cognitive performance among children with ADHD.
Introduction
ADHD is a common neurodevelopmental disorder, characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity that results in substantive impairment (American Psychiatric Association, 2013). According to national survey data, approximately 10% of children aged 2 to 17 years in the United States have ever received an ADHD diagnosis (Danielson et al., 2018). Sleep disturbances are a common co-occurring concern for children with ADHD, with about 70% experiencing sleep problems (Sung et al., 2008; van der Heijden et al., 2018). A Canadian study reported that 42.6% of children with ADHD had excessive daytime sleepiness, 29.7% had insomnia, 26.0% had periodic limb movements, and 24.8% had sleep-related breathing disorder (Craig et al., 2020). Sleep disturbances in children with ADHD are associated with more severe ADHD symptoms, comorbid internalizing problems, and impaired daily functioning (Accardo et al., 2012; Sung et al., 2008). Unfortunately, one of the primary treatments for ADHD can result in worsening sleep. Psychostimulants, such as Ritalin, have been shown to increase sleep disturbances such as longer sleep latency, worse sleep efficiency, and shorter sleep duration (Kidwell et al., 2015; Konofal et al., 2010).
The literature on the relationship between sleep disturbances and neurocognitive dysfunction among children with ADHD is inconsistent (Fisher et al., 2014; Gruber & Sadeh, 2004; Holingue et al., 2021; Schneider et al., 2016; Um et al., 2016). Some studies have reported no association of sleep disturbances (including parent-reported sleep problems and actigraphy-assessed sleep duration) with neurocognitive outcomes, including working memory, motor function, intelligence, and executive function, among young children with ADHD (Gruber & Sadeh, 2004; Schneider et al., 2016). However, Fisher et al. (2014) found self-reported sleep problems (e.g., trouble getting to sleep, unrefreshing sleep, and frequent nightmares) among individuals with ADHD were associated with impaired neuropsychological test performance in information processing and speech-sounds perception. Moreover, higher parent-reported Children’s Sleep Habit Questionnaire (CSHQ; Owens et al., 2000) scores have been associated with poorer executive function among children with ADHD (Holingue et al., 2021). Last, a study in drug-naïve children with ADHD found that sleep architecture (i.e., proportion of stage 2 and stages 3 and 4 sleep period, rapid eye movement (REM) sleep period and latency, and limb movement index with arousals) predicted the performance on the Wechsler Intelligence Scale for Children-III (WISC-III) and the Matching Familiar Figure Test for Korean Children (MFFT-KC), for example, higher proportion of stages 3 and 4 sleep period predicted higher score in verbal intelligent quotient (Um et al., 2016). Despite inconsistent evidence in the pediatric ADHD population, evidence from the broader sleep literature supports the link between sleep disturbances and neurocognitive functioning in children (Gozal & Kheirandish-Gozal, 2007; J. Vriend et al., 2015).
The relationship between sleep problems and cognitive functioning in children with ADHD may depend on how sleep is measured or may vary across specific sleep problems. For instance, Moreau et al. (2013) found that shorter total sleep time (measured by actigraphy), but not parent-reported sleep difficulties (measured by CSHQ), was related to poorer executive function in children with ADHD. Similarly, Sciberras et al. (2015) reported that only one of six subscales (bedtime resistance) from the CSHQ was associated with poorer working memory (Sciberras et al., 2015).
In recent years, a relatively new sleep construct, social jetlag, has emerged in the literature. Social jetlag is defined as the discrepancy between biological and social rhythms. It can be quantified as the difference in sleep midpoint on working days and free days (Cespedes Feliciano et al., 2019). Human sleep/wake timing is influenced by a combination of circadian oscillations generated by the suprachiasmatic nucleus of the hypothalamus, and environmental stimuli, including bright light and mealtimes. Of course, social expectations (e.g., attending school or work on time) and behaviors (e.g., late sleep onset due to technology use) also influence sleep/wake timing. This difference between internal biological rhythms and the timing of sleep as a consequence of social factors can influence cognitive performance among adolescents and adults, yet there is little research available on the link between social jetlag and cognitive performance in children. Several studies have found that greater social jetlag is associated with poorer academic performance, learning, and cognitive ability in adolescents and adults (Díaz-Morales & Escribano, 2015; Wright et al., 2006). McGowan et al found, in a cohort of young adults without ADHD, that social jetlag was significantly associated with more ADHD symptoms and impulsivity (McGowan et al., 2020). However, Langberg et al. (2019) reported that social jetlag did not differ between adolescents with and without ADHD (Langberg et al., 2019). To the best of our knowledge, the impact of social jetlag on cognitive performance has not been examined among children with clinically diagnosed ADHD.
The goals of this cross-sectional, observational study were to describe three sleep-related constructs (i.e., time in bed, sleep disturbances, and social jetlag) in children with ADHD and examine their association with neurocognitive performance in this population. An association between one or more of these sleep constructs and scores on objective neurocognitive testing, as hypothesized, would have important implications for sleep interventions that may improve cognitive performance. Based on the aforementioned literature, we hypothesized that less time in bed and greater sleep disturbances as well as social jetlag would be associated with poorer neurocognitive performance.
Methods
Participants
Children included in this study were referred for evaluation to an urban, outpatient neuropsychology clinic, housed within a children’s hospital in the Mid-Atlantic region of the US. Children were referred to the clinic for many reasons, including mental health, behavioral, and medical concerns. To be included in the present analysis, a child was required to have a clinical diagnosis of ADHD, be between 5 and 12 years old, and have complete data from a pre-visit history and symptom questionnaire and receive neurocognitive test. This age range was selected because of the dearth literature of for children within the age range, and parent report of sleep patterns is likely to be less accurate than self-reports among adolescents aged 13 to 17 years (Short et al., 2013).
Pre-Visit Questionnaire and Sociodemographics
Caregivers of referred children completed a clinic-specific, pre-appointment questionnaire querying basic sociodemographic, sleep, and asking them to rate their child’s behavior on specific behavioral rating scales. Demographic information, including child age, sex, and parent education level (high school, bachelors/some college, and graduate degree) was gathered from this pre-visit questionnaire. Additional sociodemographic information, including race (White, Black, and others) and insurance type (commercial, Medicaid/self-pay, or others), were collected from the electronic medical record.
Sleep Measures
Parent-reported bedtimes and wake times for children on typical school days and free days were obtained from the pre-visit questionnaire. Time in bed on school days and on free days were each defined as separate outcomes by calculating the interval between reported habitual bed and wake times in hours. Social jetlag was calculated as the absolute value of the difference in the timing of the sleep midpoint on school days and free days (midpoint on free days − midpoint on school days). For instance, if a participant typically goes to bed at 11 pm and wakes up at 7 am on school days (the midpoint of sleep is 3 am on school days), but he/she goes to bed at 12 am and wakes up at 8 am on free days (the midpoint of sleep is 4 am on free days), then the participant would have a social jetlag of 1 hour.
The pre-visit questionnaire also included five questions about sleep disturbances, which aimed to hit the main domains of sleep disturbances in children according to a literature review, including (1) sleep onset problems, (2) restlessness, (3) nighttime wakefulness, (4) snoring, and (5) difficulty waking. The verbatim questions are described in detail in Supplemental Table S1. The frequency of each type of sleep disturbance was measured by four ordinal response options in the questionnaire: 0 (Never/rarely), 1 (Sometimes), 2 (Often), and 3 (Very Often). During the analysis, a binary variable was created reflecting endorsement of each sleep disturbance: yes (combining “often” and” very often”) and no (combining “never/rarely” and “sometimes”). The total number of reported sleep disturbances for each child was based on these binary variables, which ranged from 0 to 5.
Neuropsychological Measures
Five cognitive domains were considered in the current study: (1) working memory; (2) attention; (3) processing speed; (4) visually-based reasoning; and (5) language-based reasoning. The specific neuropsychological tests administered to children in this study were determined based upon patient referral reasons and clinician discretion. As such, scores of tests assessing similar constructs (e.g., verbal ability) were combined using the age-adjusted z scores (derived from the general population mean). A detailed list of the specific neuropsychological tests for each domain is shown in Supplemental Table S2.
Statistical Analysis
Descriptive, bivariate, and multivariable statistics were used to examine the associations between sleep-related constructs and neurocognitive performance. First, time in bed, social jetlag, and sleep disturbances were summarized using visualizations and descriptive statistics. Next, Pearson’s correlations were calculated between the aforementioned sleep variables and measures of neurocognitive performance. Lastly, a series of linear regression models were performed to estimate the associations between sleep parameters (time in bed, social jetlag, and sleep disturbances) and neurocognitive performance (working memory, attention, processing speed, visually-based reasoning, and language-based reasoning). Regression models were adjusted for sociodemographic variables (child age, sex, race, parent education, and insurance type). All statistical analyses were conducted using STATA SE 18 for Windows (Stata Corp, Texas, USA), with statistical significance at p < .05.
Results
Sociodemographic, Neurocognitive, and Sleep Characteristics
We reported the basic characteristics of the sample in Table 1. A total of 350 children, aged 5 to 12 years (M = 8.7 years, SD = 1.8 years), were included in the current study. Most were boys (70.9%) and had commercial insurance (74.3%); half of children were White (56.3%). Children included in this sample had working memory, attention, and processing speed scores that were about 0.6 SD below the normative sample, while visually-based reasoning and language-based reasoning scores were 0.1 SD below the general population.
Basic Characteristics of Study Population.
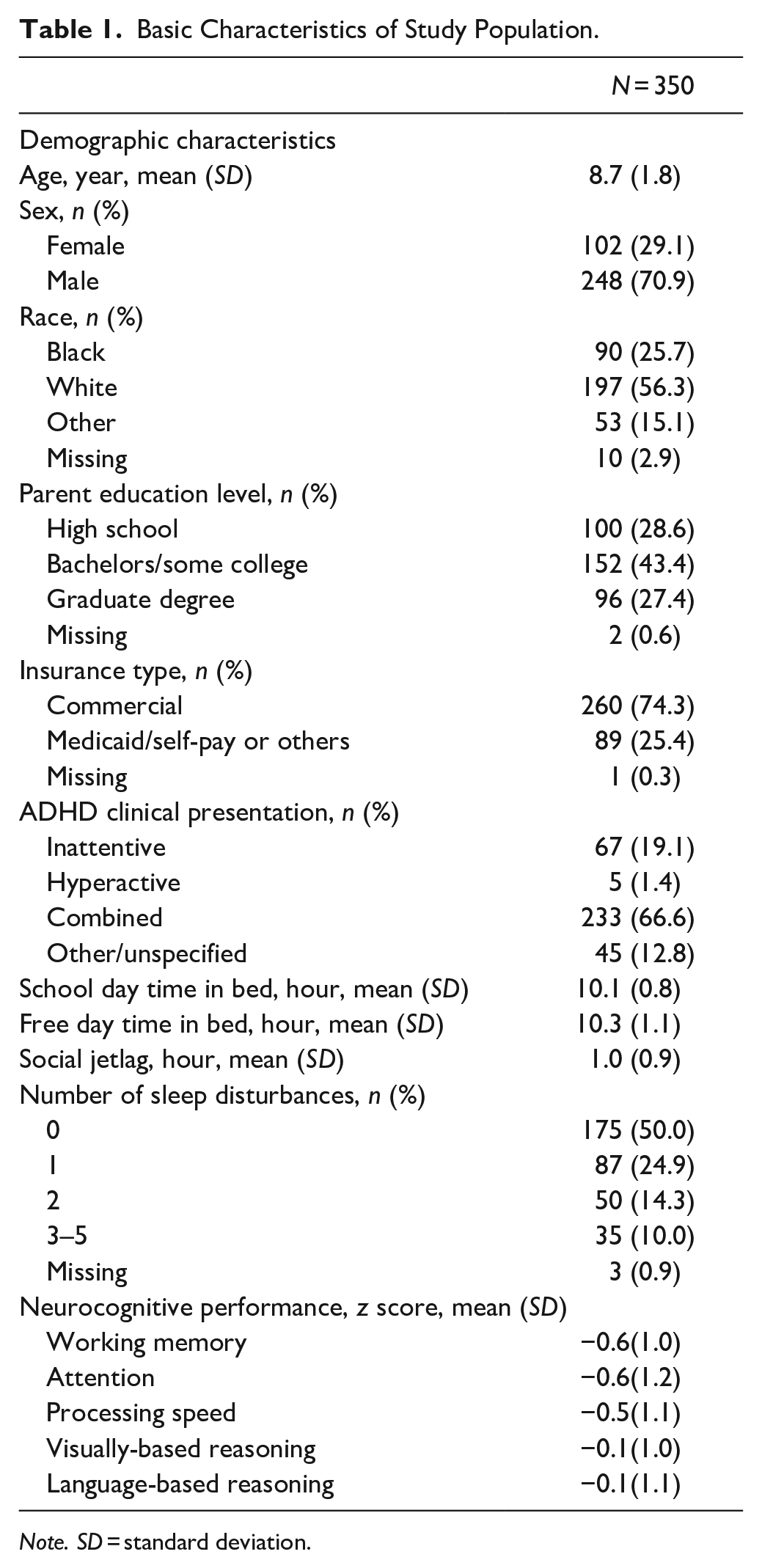
Note. SD = standard deviation.
Distributions of time in bed and social jetlag in this sample are shown in Figure 1. On average, children slept 10.1 hours (SD = 0.8, range: 6.5–12.5) on school days and slept 10.3 hours (SD = 1.1, range: 6.5–14) on free days. The mean social jetlag in this sample was 1.0 hours (SD = 0.9, range: 0–5.2). As shown in Table 2, there was a moderate correlation between time in bed on school days and free days. A weak to moderate correlation between social jetlag and time in bed on school days and free days was also observed. Sleep disturbances were very common among participants: about half of children with ADHD had at least one type of sleep disturbance and 1 in 10 children with ADHD had more than three types of co-occurring sleep disturbances. As for specific types of sleep disturbances (Figure 2), sleep onset problems (25.1%), difficulty waking in the morning (21.1%), and restlessness (17.7%) were the three most common sleep disturbances among participants.
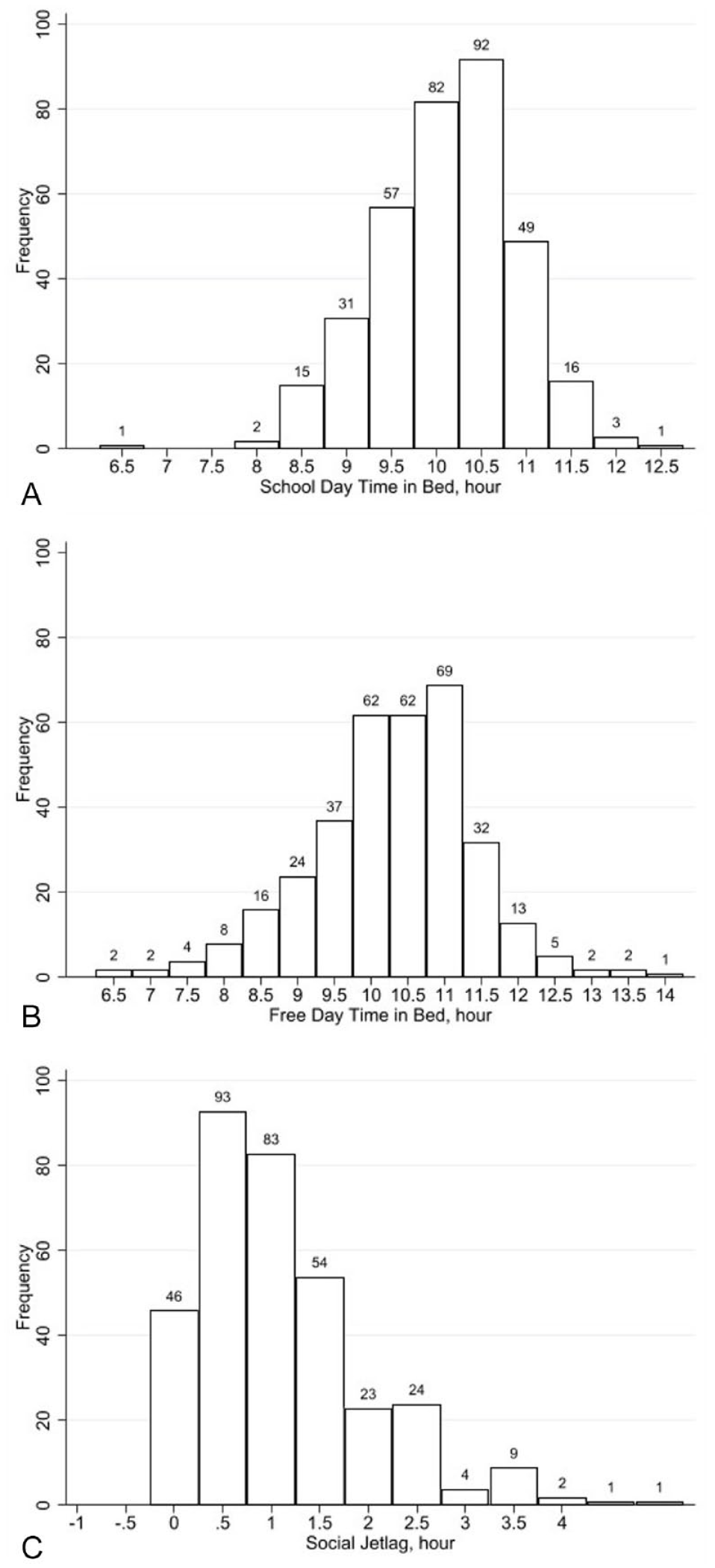
Distribution of school day time in bed, free day time in bed, and social jetlag.
Correlation Matrix for Continuous Sleep Variables and Neurocognitive Performance.
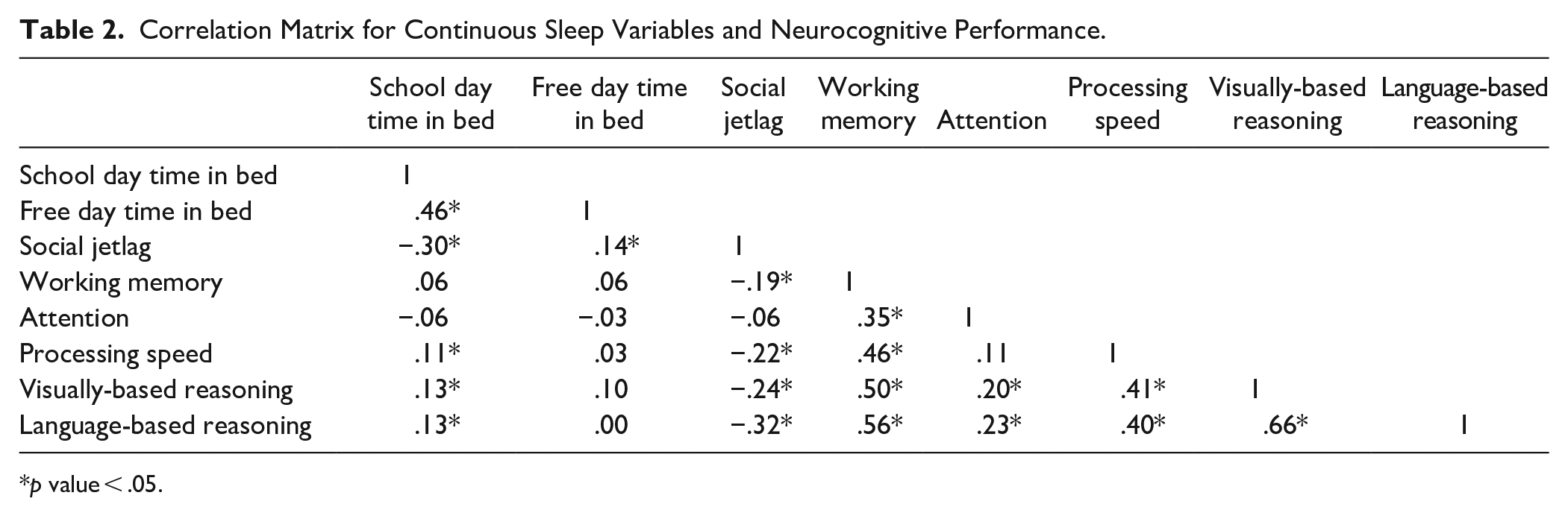
p value < .05.
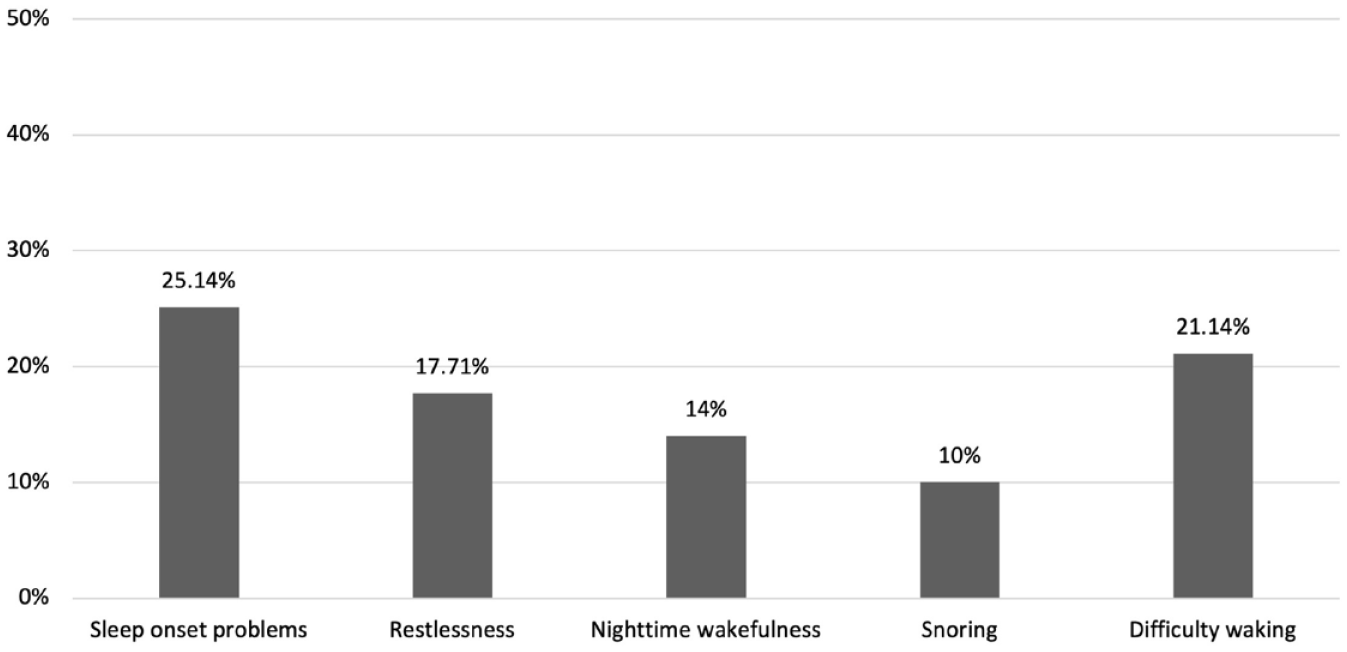
Distribution of sleep disturbances.
Relationship Between Time in Bed and Cognitive Performance
Shown in Table 3, in the unadjusted model, time in bed on school days was positively and significantly associated with processing speed, visually-based reasoning, and language-based reasoning. That is, a 1-hour increase in time in bed on school days was associated with .14 (95% CI [0.00, 0.29]) SD increase in the processing speed score, .16 (95%CI [0.03, 0.30]) SD increase in the visually-based reasoning score, and .19 (95% CI [0.04, 0.33]) SD increase in language-based reasoning. However, the above associations did not remain significant after adjusting for other covariates. Longer time in bed on free days was not associated with cognitive performance in any domain.
Linear Regression Model Estimating Association Between Time in Bed and Neurocognitive Performance.
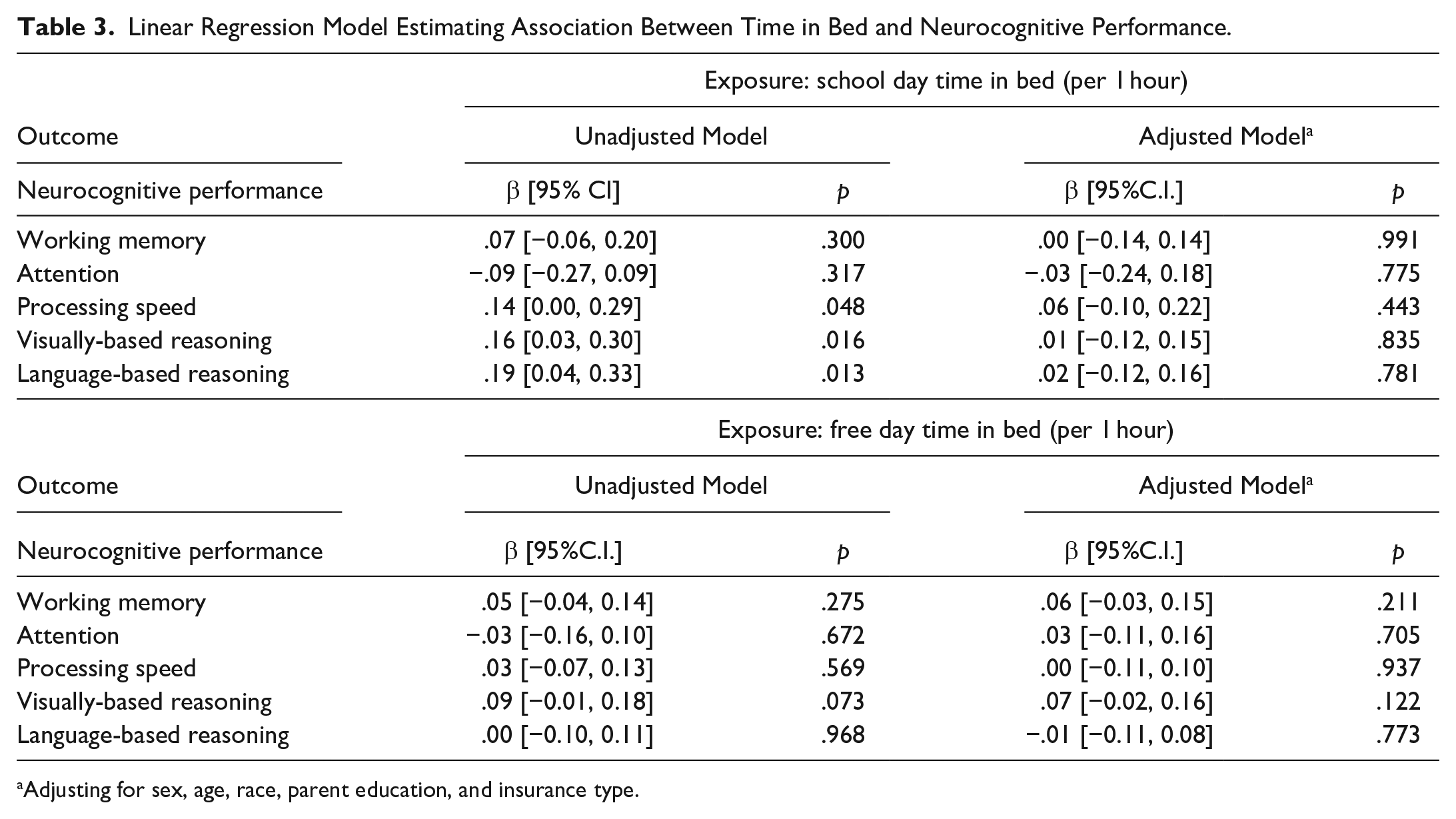
Adjusting for sex, age, race, parent education, and insurance type.
Relationship Between Social Jetlag and Cognitive Performance
Shown in Table 4, the unadjusted associations between greater social jetlag and poorer neurocognitive performance were significant for all domains, except attention. However, after adjustment for sociodemographic characteristics, the association between social jetlag and working memory was no longer significant. The associations of social jetlag with processing speed, visually-based reasoning, and language-based reasoning remained significant, however, after adjustment, with a slight decrease in effect size. Every 1-hour increase in social jetlag was associated with a 0.20 SD decrease (95% CI [−0.35, −0.06]) in processing speed scores, a 0.13 SD decrease (95% CI [−0.27, 0.00]) in visually-based reasoning scores, and a 0.22 SD decrease (95% CI [−0.36, −0.08]) in language-based reasoning scores.
Linear Regression Models Estimating Association Between Social Jetlag and Neurocognitive Performance.
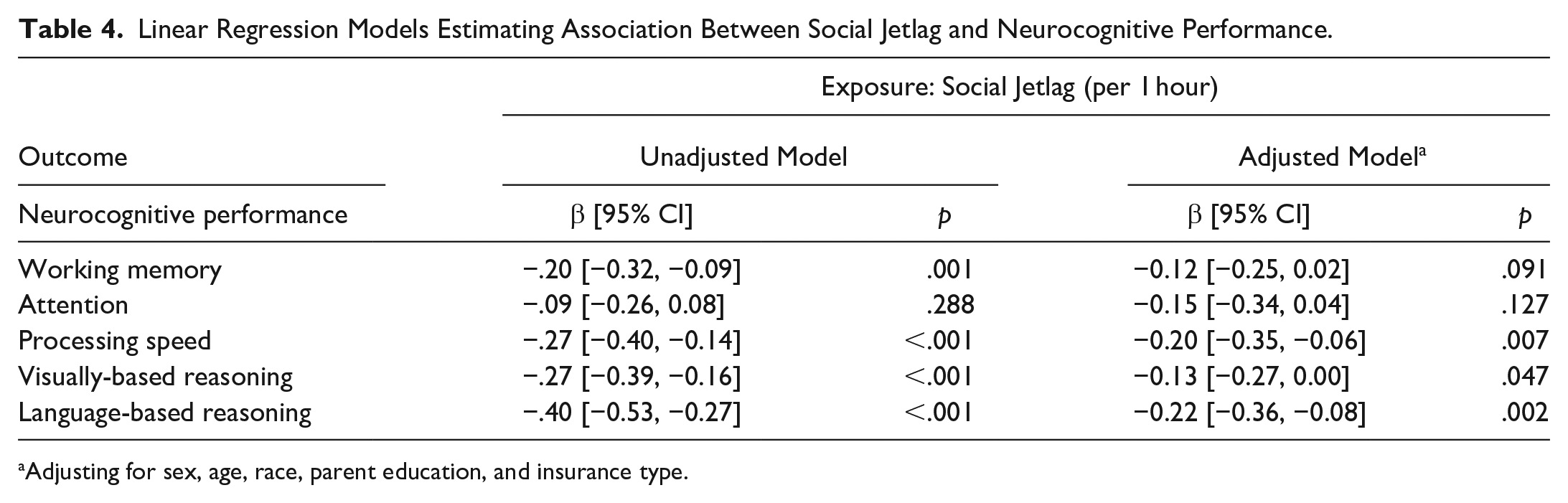
Adjusting for sex, age, race, parent education, and insurance type.
Relationship Between Sleep Disturbances and Cognitive Performance
The number of sleep disturbances was not associated with cognitive performance in any domain (Table 5). We further assessed if the relationship differed for different types of sleep disturbances (Supplemental Table S3). The children who had sleep onset problems often or almost always were more likely to have poor performance in attention: they had 0.38 (95% CI [−0.72, −0.05]) lower attention z scores than the children who never or sometimes had such disturbances.
Linear Regression Models Estimating Association Between Number of Sleep Disturbances and Neurocognitive Performance.
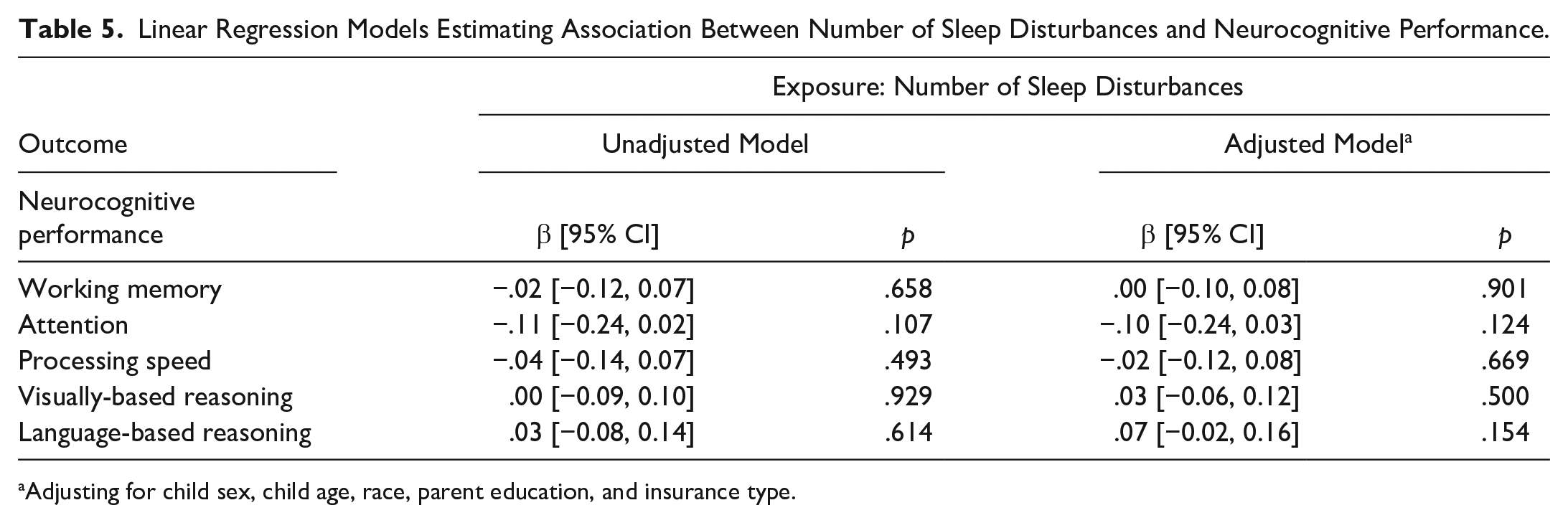
Adjusting for child sex, child age, race, parent education, and insurance type.
Discussion
Cognitive development is associated with a multitude of biological and environmental factors, such as genetics, family experiences (e.g., maternal education), environmental conditions (e.g., lack of access to clean water and sanitation), and health conditions (e.g., anemia in infancy), much of which are difficult to change (Mason et al., 2021; Mollon et al., 2021; Sania et al., 2019). However, sleep is relatively easy to modify in comparison to these other factors (e.g., genetic and structural environment), making it an attractive target for intervention. To the best of our knowledge, this is the first paper to report the distribution of social jetlag and its relationship with neurocognitive performance in pediatric ADHD. Although the majority of studies about social jetlag in the general population have focused on adolescents, social jetlag begins to present at 5 years of age and increases with age until its peak at the end of adolescence (Randler et al., 2019). Examining this construct in children with ADHD is particularly valuable given the common occurrence of this condition in the general population, the known association between attention problems/hyperactivity and sleep, and the early onset of both sleep problems and ADHD in childhood.
The average social jetlag among children in our study was 1 hour, which is substantially larger than that of the general pediatric population (43 minutes; Stoner, Castro, et al., 2018). This is likely due to the inclusion of a clinical population. Our results indicated a consistently negative association between social jetlag and cognitive performance, outside of attention, in the unadjusted models. In the adjusted models, language-based reasoning and processing speed demonstrated a moderately negative association, visually-based reasoning a weak negative association, and attention as well as working memory showed a null association with social jet lag.
These findings suggests a negative association between social jetlag and neurocognitive performance in school-age children with ADHD, particularly as it relates to processing speed and language-based reasoning. This provides a potential target for intervention. Social jetlag among children occurs due to the changes in rules and routines within households between school/weekdays and weekends. Parents naturally provide more freedom over the weekends when these demands are absent, opposed to during the week (Stoner, Beets, et al., 2018). When time in bed is increasingly different between weekends and weekdays, this can perturb the natural circadian rhythms, leading to poorer cognition and mental acuity. Our findings suggest keeping consistent routines for children with ADHD could improve learning and attention. From the perspective of school, delaying the school start times by up to an hour has been proven to be an effective approach to reduce social jetlag (Minges & Redeker, 2016).
It’s important to recognize our findings are not completely in line with prior work. Previous research reported that social jetlag was negatively associated with attention/inhibition in healthy adults (McGowan et al., 2020) and with performance on spatial, reasoning, and numerical tests, but not with vocabulary and verbal fluency in adolescents (Díaz-Morales & Escribano, 2015). The contradictory findings between our study and that of Díaz-Morales and Escribano (2015) might be explained by the differences in the sample characteristics. For example, the participants included in Díaz-Morales and Escribano’s (2015) study were 12 to 16 years old, while the children in our study were much younger.
Our results indicated a weak relationship between time in bed and neurocognitive outcomes among children with ADHD. Several studies conducted in general pediatric populations indicated that short sleep duration is related to impaired memory (Steenari et al., 2003; J. L. Vriend et al., 2013), as well as poor academic performance (Dewald et al., 2010). Clinical trials among children and adolescents with ADHD reported that experimental manipulation of sleep restriction contributes to impaired neurocognitive functioning (Becker et al., 2019; Gruber et al., 2011). As for evidence from observational studies, Moreau et al. reported that short sleep duration was associated with impaired executive function in children with ADHD, even controlling for gender, age, and use of medication (Moreau et al., 2013). Thus, our results are inconsistent with the findings from previous studies. There potentially many reasons for this discrepancy, including measurement, study design, and sampling. For instance, the questionnaire used in our study only asked bed and wake times, but we were unable to know if the child actually slept or not during the time period. Additionally, the association between sleep duration and cognition might be different in observational research settings and clinical trial settings. Also, we did not find strong evidence to support the potential link between sleep disturbances and neurocognitive performance. It is important to state that our measurement of sleep disturbances was limited. Further study using clinical sleep diagnoses to measure such disturbances is needed to understand this association better.
These findings should be interpreted in the context of the study’s limitations. First, we leveraged clinically collected data for the purposes of analysis, which means the results are not generalizable to the general population. Second, there are some weaknesses in the measurement of sleep-related constructs in our study. On the one hand, it is difficult to measure sleep disturbances through only five items. A more comprehensive instrument should be used in future studies, for example, the Children’s Sleep Habits Questionnaire (CSHQ). However, it is important to state that the five items in our study reflect the key sleep domains within the CSHQ briefly, including sleep onset, night waking, and sleep-disordered breathing. On the other hand, measures of time in bed and social jetlag were based on caregivers’ retrospective reports, which are imprecise, rather than actual sleep duration measured by sleep diary or actigraphy. For example, a child might be awake during part of the night, which could not be captured by current measurements in our study. Additionally, the current measurement did not provide estimates of time that are precise to the minute. Third, there are multiple cognitive measures used in our study and the method of collapsing results from different subtests across cognitive tests into z-scores for each domain still requires validation. However, combining scores from similar subtests together as measures of a target construct has been applied in previous studies (Patrick et al., 2013; Ris et al., 2008), which is a feasible approach to deal with real-world data. Last, the cross-sectional nature of our data cannot be used causally, as sleep problems and neurocognition may have a bidirectional relationship.
Despite these limitations, this study has several strengths. Our sample was relatively large compared with previous studies in this area, constructed using a clinically determined diagnosis, and our outcome was measured using comprehensive objective measures. In summary, our study indicated that social jetlag is an important sleep construct in ADHD population and is related to several domains of cognition. The results of our study suggest that sleep-related issues, particularly social jetlag, could affect the performance of children with ADHD in the neurocognitive assessment and might influence their school performance and life functioning in long term. Thus, it is important for healthcare providers to understand the potential link, pay attention to how to interpret neurocognitive evaluation in the presence of sleep jetlag, and consider how to support children with ADHD in need regarding their sleep issues.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231204010 – Supplemental material for Association of Time in Bed, Social Jetlag, and Sleep Disturbances With Cognitive Performance in Children With ADHD
Supplemental material, sj-docx-1-jad-10.1177_10870547231204010 for Association of Time in Bed, Social Jetlag, and Sleep Disturbances With Cognitive Performance in Children With ADHD by Xueqi Qu, Luther G. Kalb, Calliope Holingue, Darlynn M. Rojo-Wissar, Alison E. Pritchard, Adam P. Spira, Heather E. Volk and Lisa A. Jacobson in Journal of Attention Disorders
Footnotes
Author’s Note
Calliope Holingue is also affiliated to Kennedy Krieger Institute, Baltimore, MD, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.