
Abstract
Objective(s):
To assess the likelihood of ADHD diagnosis in children of non-US-born caregivers relative to children of US-born caregivers.
Method:
Cross-sectional analysis of a combined 2016 to 2019 National Survey of Children’s Health dataset (n = 109,881) was performed to identify associations between caregiver’s birth outside the U.S. and child’s ADHD diagnosis. Logistic regression models adjusted for potential sociodemographic confounders.
Results:
Children with one or two non-US-born caregivers were less likely to be diagnosed with ADHD (aOR = 0.58, p < .001; aOR = 0.59, p < .001, respectively). Likelihood of a diagnosis increased as non-US-born caregivers spent more time in the US. After a diagnosis, children of two non-US-born caregivers were less likely to be treated with medication.
Conclusion:
The lower likelihood of ADHD diagnosis in children with non-US-born caregivers may reflect an increasing need for public health education to raise awareness about ADHD among this population and the development of culturally sensitive ADHD identification methodologies.
Introduction
ADHD remains one of the most common neurodevelopmental disorders in children in the United States. Data from 2013-2019 estimate that approximately 9.4% to 9.8% of US children were diagnosed with the condition (Center for Disease Control and Prevention, 2022). The broad range of long-term adverse effects associated with ADHD has been well-documented in the scientific literature. Children with ADHD can be prone to future psychiatric diagnoses and socialization issues (Carpenter Rich et al., 2009; Swanson et al., 1998) and are more likely to have comorbidities such as anxiety, depression, behavior disorders, and learning problems (Chen et al., 2016; DuPaul et al., 2013; Loe & Feldman, 2007). Additionally, previous studies have shown that academic underachievement and poor educational outcomes associated with ADHD can persist well into adulthood (Loe & Feldman, 2007; Voigt et al., 2017). Early identification and treatment for the condition can thus be crucial in improving outcomes.
A unique aspect of ADHD is the difference in perspectives around whether the condition is significantly affected by sociocultural factors in American society. Description of ADHD began in the early 20th century in the US, where the majority of ADHD research has since been conducted; it was not until the 1990s that there was evidence for ADHD diagnosis and treatment in other countries (Conrad & Bergey, 2014). As a result, ADHD has been discussed by some as a “culture-bound syndrome,” one that is treated mainly in the US and some other English-speaking countries (Canino & Alegría, 2008; Timimi & Taylor, 2004). In the past few decades, more research efforts have been dedicated to determining the global prevalence of ADHD, indicating that ADHD is indeed a global condition and has been recognized in other non-Western countries. Using articles up to the year 2020, the worldwide pooled prevalence of ADHD was estimated to be 7.6% among children ages 3 to 12 and 5.6% among teenagers aged 12 to 18 (Salari et al., 2023). Among some countries with a large number of immigrants to the US, ADHD prevalence in children and adolescents was typically lower than the 9.4% to 9.8% found in the US; China had an estimated prevalence of 6.26%, while the equivalent figure was 7.1% for India (Joseph & Devu, 2019; Wang et al., 2017). While a 2020 meta-analysis estimated that the pooled prevalence of child & adolescent ADHD in Africa was 7.47%, there may be a wide range of rates within individual countries; Mhalla et al. found that the rate of ADHD among Tunisian adolescents was 18.1% (Ayano et al., 2020; Mhalla et al., 2018). There has also been a worldwide increase in ADHD diagnosis and consumption of ADHD medications that has been attributed to the rise of globalization and a shift to the Diagnostic and Statistical Manual of Mental Disorder (DSM) diagnosis criteria in many countries (Conrad & Bergey, 2014). However, challenges remain in the consistent and systematic identification of ADHD due to variations in both its definition and the perceptions of its symptoms. For instance, the World Health Organization’s International Classification of Mental and Behavioral Disorders (ICD) classifies ADHD as hyperkinetic disorder (HKD); in previous editions of the ICD, this particular definition required a higher threshold for a diagnosis than the DSM’s criteria and may have had an effect on international clinicians’ diagnosis of the condition (Conrad & Bergey, 2014; Schachar et al., 2007). One meta-analysis reported that the prevalence of hyperactivity was found to be higher among studies that used the DSM-IV criteria as opposed to ICD10 criteria (Salari et al., 2023). More importantly, ADHD deals largely with disordered behavior, which is deeply rooted in both social and developmental contexts and can be interpreted differently by cultural and ethnic groups (Conrad & Bergey, 2014). For instance, a previous study of college teachers’ perceptions of ADHD found that Chinese participants were more attentive to symptoms of hyperactivity than inattention compared to American participants (Norvilitis & Fang, 2005). One study that investigated potential explanations for lower mean ADHD scores in Norway and Sweden compared to Australia and the United States found support for over-reporting tendencies among Australian and US parents; they suggested that symptoms of hyperactivity may be more salient in these countries (MacDonald et al., 2019). Thus, when migrating to a country with significant differences in sociocultural expectations for child behavior, families may overlook symptoms of ADHD when raising children in this new environment, which could later lead to detrimental effects on their development.
Previous studies on the association between parental immigration and ADHD diagnosis have yielded conflicting results. A population-based case-control study in Finland showed that the likelihood of being diagnosed with ADHD was significantly increased among children of two immigrant parents and children of an immigrant father (Lehti et al., 2016). Another study from Denmark investigating differential parent and teacher reports of ADHD symptoms found that while teachers reported similar amounts of symptoms regardless of migration status, immigrant parents reported fewer symptoms relative to non-immigrant parents (Sahuric et al., 2021). A similar pattern applies to ADHD medication and behavioral treatment. One Swedish study reported that immigrant parents, particularly those from countries of origin with lower income levels, were less likely to receive ADHD medication for their children (Arat et al., 2018). While the use of stimulants for ADHD has increased worldwide, the use of behavioral therapy in combination with pharmacologic therapy has been shown to be superior to medication alone, especially in cases with comorbid conditions (Drechsler et al., 2020; Rajaprakash & Leppert, 2022). Past studies have shown considerable variability in different countries’ usage of psychosocial or behavioral interventions even within an all-European cohort (Hodgkins et al., 2013). However, differences in the use of behavioral treatment for ADHD in immigrant families have not been studied in depth. A parent’s willingness to obtain care for their child may remain dependent on the predominant ideological theories of their country of origin, their personal acceptance of ADHD as a medical condition, and the structural and cultural influences on the perception of ADHD (Hinshaw et al., 2011). Despite the aforementioned international studies on this topic, to date, there has been no similar large-scale effort in the US to identify the differential likelihoods of ADHD diagnosis between children of US-born caregivers and children of non-US-born caregivers.
The National Survey of Children’s Health (NSCH), a cross-sectional and nationally representative annual survey of various health indicators of US children between the ages of 0 and 17 years old, presents a unique opportunity to compare the differences in ADHD diagnosis between children of US-born caregivers and children of non-US-born caregivers. In this study, we assess the association between parental nativity and ADHD diagnosis, with controls for potential confounders, and compare that with other common developmental, behavioral, and mental health conditions. Additionally, we investigate whether the amount of time that non-US-born caregivers have spent in the US is related to ADHD diagnosis and whether there are differences in children taking ADHD medications and receiving behavioral treatments post-diagnosis. We hypothesize that children with non-US-born caregivers are less likely to be diagnosed with ADHD. Additionally, our secondary hypothesis is that the likelihood of diagnosis increases with the longer amount of time that the caregivers spent in the US.
Methods
Sample
The U.S. Health Resources & Services Administration administers the NSCH, an annual survey that examines physical and emotional health of the US population of non-institutionalized children ages 0 to 17. The NSCH uses a two-phase multimodal survey process, and the data is subsequently weighted to be nationally representative (US Census Bureau, 2020a). The results of the surveys are publicly available through the United States Census Bureau website. The NSCH datasets from 2016, 2017, 2018, and 2019 were combined for cross-sectional analysis according to the 2019 NSCH Guide to Multi-Year Analysis (US Census Bureau, 2020b). The 2020 and 2021 datasets were not included due to overlap with the COVID-19 pandemic. Since the NSCH did not ask questions about ADHD diagnosis and treatment for children younger than 3 years old, the sample was restricted to children ages 3 to 17. Data collection instruments were available in English and Spanish, and telephone questionnaire assistance was available in multiple languages for all years. The questionnaire was completed by an adult in the household who was one of the child’s primary caregivers (and could then subset their relationship as biological or adoptive parent, step-parent, grandparent, foster parent, other: relative, or other: non-relative).
Parental Nativity Designation
Caregivers were asked to provide information on whether the person filling out the survey and the second caregiver in the household were born in the US. Subsequently, the sample was categorized into three separate groups:
Group 1 (Reference group): Children with two US-born caregivers/Children with one US-born caregiver in a single-caregiver household
Group 2: Children with one non-US-born caregiver, not in a single-caregiver household
Group 3: Children with two non-US-born caregivers/Children with one non-US-born caregiver in a single-caregiver household
Additionally, the duration of time since the caregiver’s move to the US was also taken into account. For children with only one caregiver born in the US, only the caregiver who had been born outside the US was considered. For children with two non-US-born caregivers, only the caregiver who had spent more time in the US was considered. For the purpose of this analysis, all different types of primary caregivers as noted by the aforementioned NSCH response options, without consideration of their current marital status, were included. This also included single-caregiver households. This designation was conducted via the response “There is only one primary adult caregiver in the household for this child” when asked about the second adult caregiver in the household.
Single-Item Outcome Measures
For the developmental, behavioral, and mental health conditions assessed by the NSCH, caregivers responded to two survey items on whether a doctor or other healthcare provider ever told them that the child had the condition and whether the child currently had the condition. If the caregiver responded “Yes” to both items, the child was considered to be currently having the condition. While we refer to the ADHD diagnosis according to the official DSM-5 terminology for the purposes of this manuscript, the questions regarding ADHD asked whether the child had “Attention Deficit Disorder or Attention Deficit/Hyperactivity Disorder, that is, ADD or ADHD?.” In addition to ADHD, nine other developmental, behavioral, and mental health conditions were included in this analysis to provide a comparison of the likelihood of diagnosis: autism spectrum disorder (ASD), Tourette syndrome, behavior or conduct problems, developmental delay, intellectual disability, speech or other language disorder, learning disability, anxiety, and depression. All conditions included in this analysis were only assessed for children ages 3 to 17. Finally, caregivers gave a binary response (“Yes” or “No”) to whether the child was taking ADHD medications or receiving behavioral treatments.
Statistical Analysis
Sociodemographic factors between children of two US-born caregivers and children of at least one non-US-born caregiver were compared using second-order Rao-Scott χ2 test, which accounted for the survey’s complex sampling design. Logistic regression models were used to model outcomes of interest as a function of the caregivers’ nativity designation (i.e., Group 1 vs. Group 2 and Group 1 vs. Group 3). Odds ratios (OR), adjusted odds ratios (aOR), and 95% confidence intervals (95% CI) were derived with adjustments for child’s age, sex, race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, or non-Hispanic other/multi-racial), household income (0%–99%, 100%–199%, 200%–399%, or 400%+ of federal poverty line), highest level of adult education in the household (less than high school, high school/GED, some college/technical school, or college degree or higher), health insurance coverage (currently insured/consistently insured/adequate insurance or not currently insured/coverage gap/inadequate insurance), primary household language (English or other than English), whether the child was born in the US (yes vs. no), and whether the child had received any type of medical care in the past 12 months (yes vs. no). Although some of these factors have previously been linked to ADHD, this study specifically aimed to investigate the association between ADHD diagnoses and parental nativity designation; thus, other sociodemographic factors were controlled for (Morgan et al., 2014; Russell et al., 2016).
For all analyses, p-values were derived from two-sided tests, and the statistically significant threshold was at p = .05. All analyses were conducted on the R statistical programing platform (version 4.1.1) using the survey package (version 4.1.1), which accounted for the complex sampling design of the NSCH. The study was exempt from review by the institutional review board because it used publicly available, de-identified data.
Results
Demographics
In total, 109,881 children met the criteria of inclusion for this analysis. Of these children, 90,520 were in Group 1, 8,269 were in Group 2, and 11,092 were in Group 3, which accounted for 71.94%, 9.07%, and 18.99% of the eligible sample, respectively (weighted). Children with at least one non-US-born caregiver were less likely to be White (F = 1,637.6, p < .001), more likely to have lower household income (F = 114.1, p < .001), and their caregivers tended to have lower levels of education (F = 299.9, p < .001) (Table 1). Additionally, there was an association between children with foreign-born caregivers and (1) not receiving any type of medical care in the past 12 months (F = 110.7, p < .001) and (2) not having adequate insurance (F = 10.0, p = .002). These factors were controlled for in the subsequent analyses along with demographic factors.
Sample Characteristics, 2016 to 2019 National Survey of Children’s Health (n = 109,881).
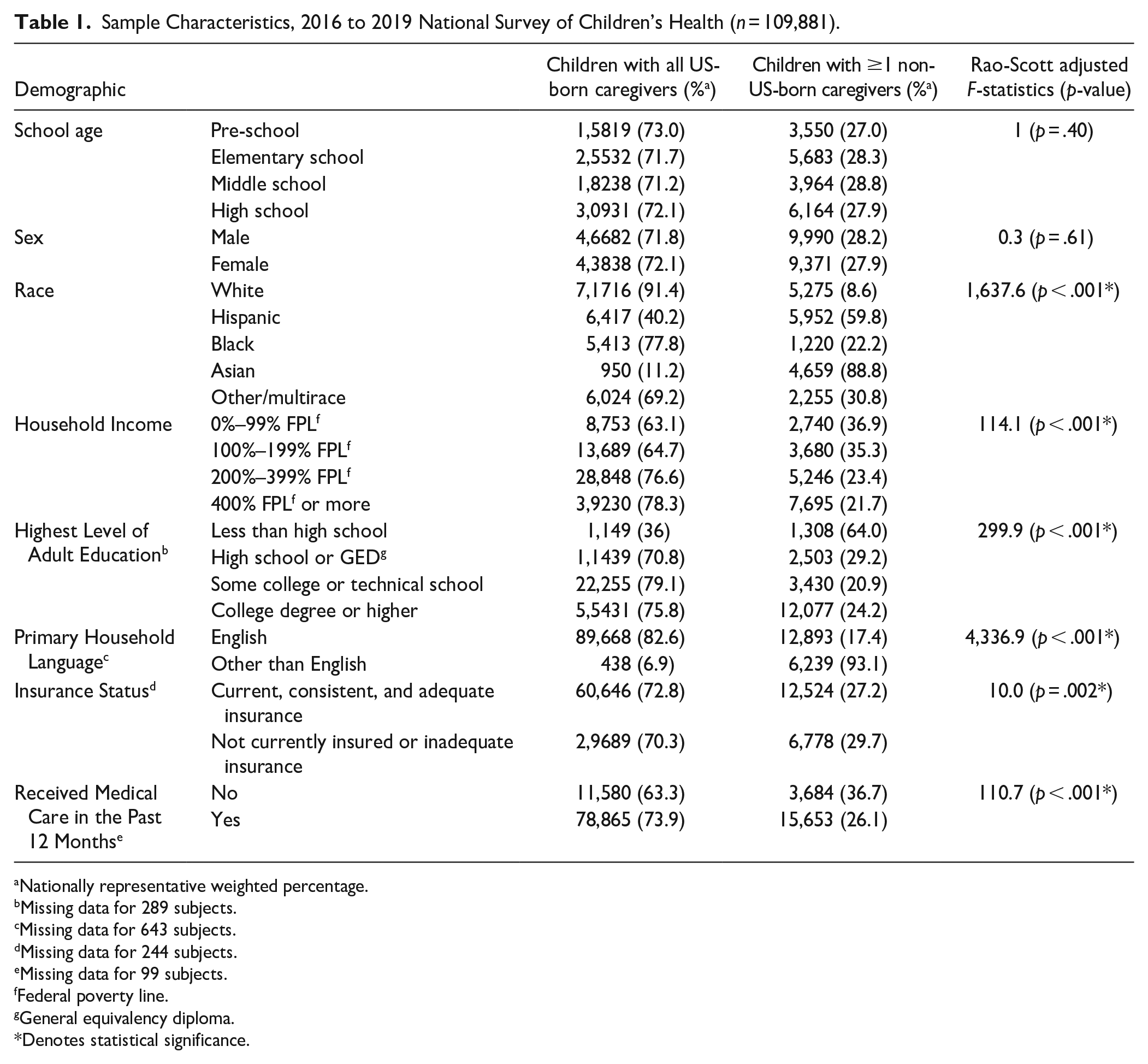
Nationally representative weighted percentage.
Missing data for 289 subjects.
Missing data for 643 subjects.
Missing data for 244 subjects.
Missing data for 99 subjects.
Federal poverty line.
General equivalency diploma.
Denotes statistical significance.
ADHD Diagnosis and Comparison With Other Conditions
Relative to children with all US-born caregivers (Group 1), children of Group 2 and Group 3 had a lower likelihood of receiving an ADHD diagnosis (aOR = 0.58, 95% CI [0.48, 0.71]; aOR = 0.59, 95% CI [0.52, 0.67], respectively) (Table 2). In comparison to other developmental, behavioral, and mental health conditions included in the NSCH, ADHD was among the conditions with the lowest likelihood of diagnosis for children of one or two non-US-born caregivers. More specifically, for children in Group 2, ADHD was the condition with the second lowest likelihood for a diagnosis, only after Tourette Syndrome (aOR = 0.34, 95% CI [0.15, 0.76]). For children in Group 3, ADHD and depression shared the lowest odds for a diagnosis.
Likelihood of ADHD Diagnosis in Comparison With Other Developmental, Behavioral, and Mental Health Conditions, 2016 to 2019 National Survey of Children’s Health (n = 109,881).
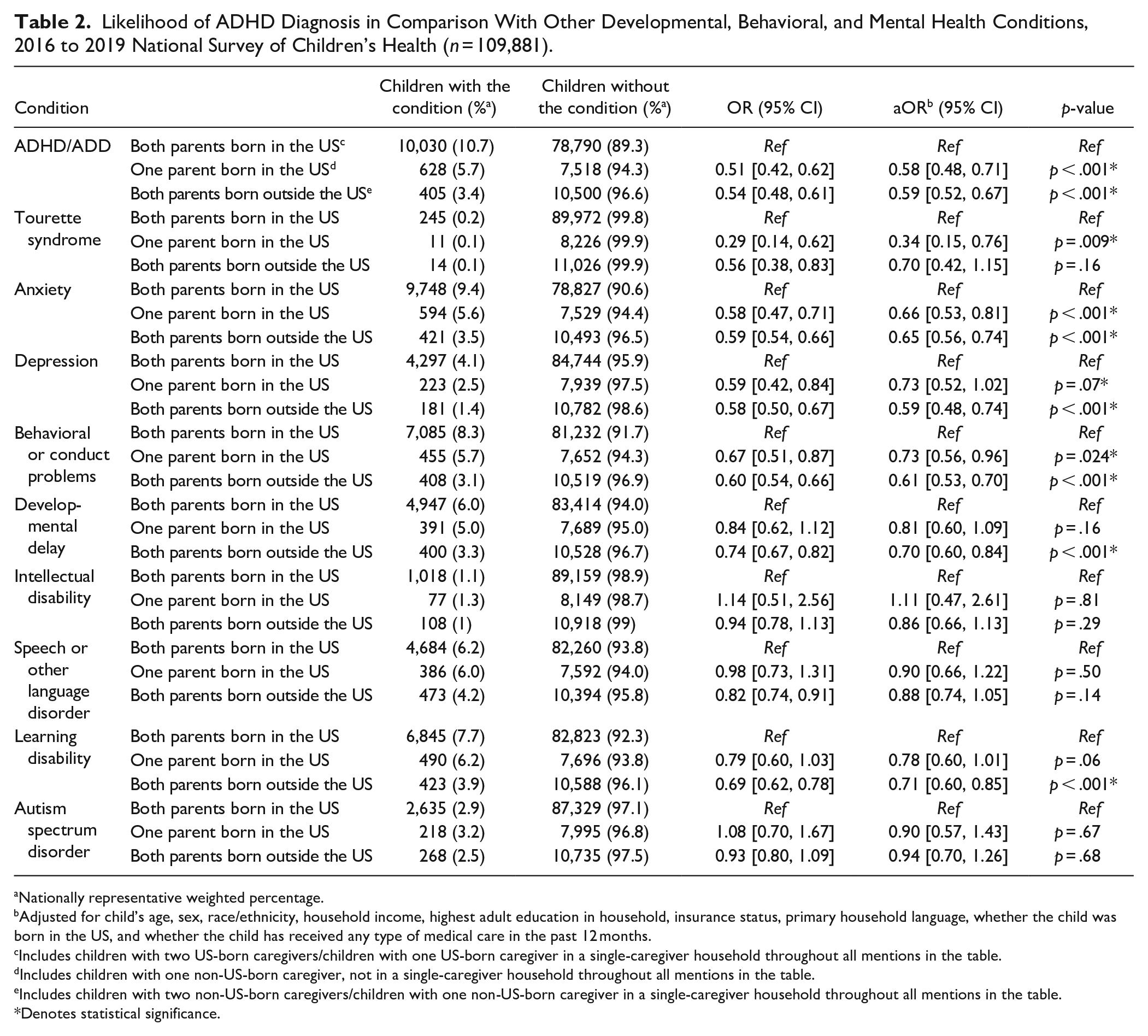
Nationally representative weighted percentage.
Adjusted for child’s age, sex, race/ethnicity, household income, highest adult education in household, insurance status, primary household language, whether the child was born in the US, and whether the child has received any type of medical care in the past 12 months.
Includes children with two US-born caregivers/children with one US-born caregiver in a single-caregiver household throughout all mentions in the table.
Includes children with one non-US-born caregiver, not in a single-caregiver household throughout all mentions in the table.
Includes children with two non-US-born caregivers/children with one non-US-born caregiver in a single-caregiver household throughout all mentions in the table.
Denotes statistical significance.
ADHD Diagnosis and Non-US-born Caregiver’s Length of Time in the US
For children in Group 3, the likelihood of ADHD diagnosis increased as caregivers spent more time in the US (Table 3). Relative to children in Group 1, children whose caregivers moved to the US within the past 0 to 10 years had the lowest likelihood for an ADHD diagnosis (aOR = 0.32, 95% CI [0.17, 0.62]), while children whose caregivers had been in the US for 30 + years were the most likely to receive such a diagnosis (aOR = 0.86, 95% CI [0.78, 0.95]). For children in Group 2, this association was only significant for the non-US-born caregiver who had lived in the US for 21 to 30 years and 30 + years (aOR = 0.73, 95% CI [0.65, 0.82] and aOR = 0.89, 95% CI [0.84, 0.95], respectively).
Association Between ADHD Diagnosis in Children and Years That Non-US-Born Parents Spent in the United States, 2016 to 2019 National Survey of Children’s Health (n = 109,881).
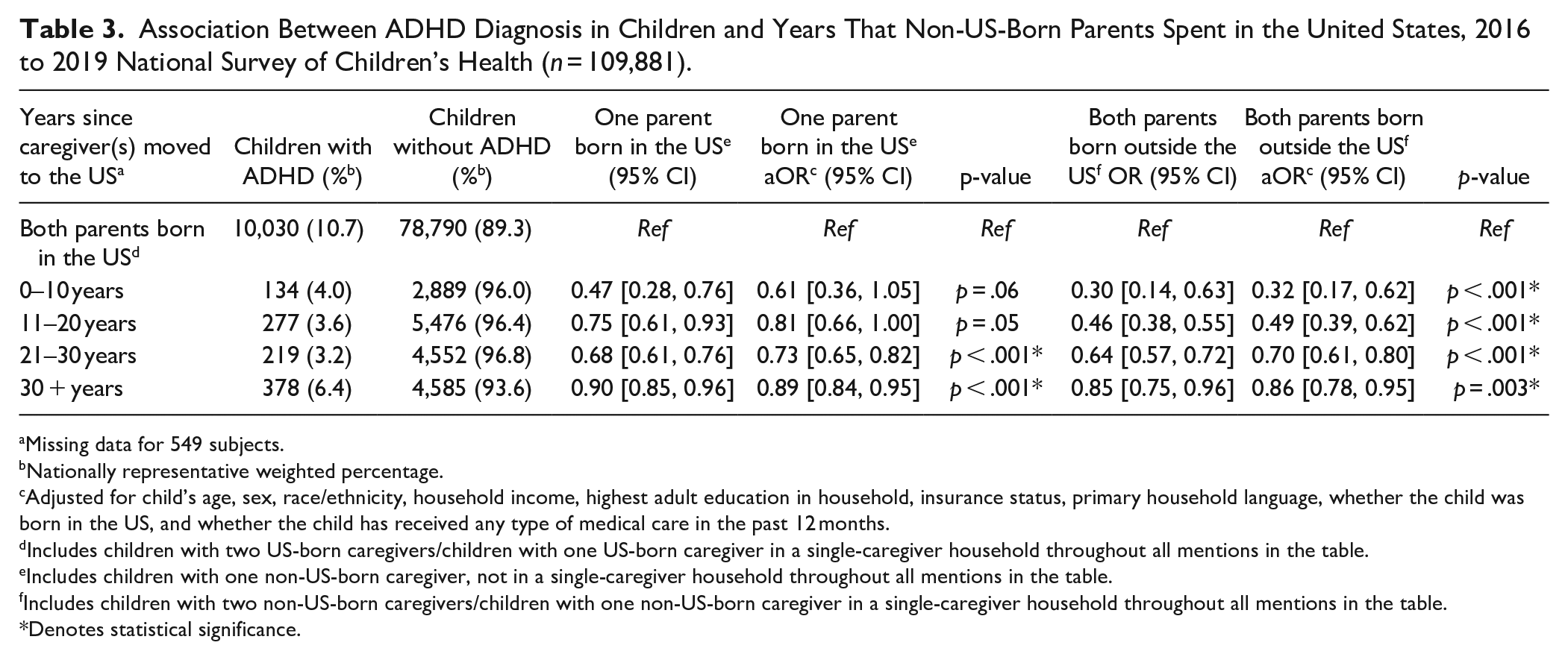
Missing data for 549 subjects.
Nationally representative weighted percentage.
Adjusted for child’s age, sex, race/ethnicity, household income, highest adult education in household, insurance status, primary household language, whether the child was born in the US, and whether the child has received any type of medical care in the past 12 months.
Includes children with two US-born caregivers/children with one US-born caregiver in a single-caregiver household throughout all mentions in the table.
Includes children with one non-US-born caregiver, not in a single-caregiver household throughout all mentions in the table.
Includes children with two non-US-born caregivers/children with one non-US-born caregiver in a single-caregiver household throughout all mentions in the table.
Denotes statistical significance.
ADHD Treatment and Medication
When the sample was further restricted to only children with an ADHD diagnosis, those in Group 3 were less likely to take medication for the condition relative to children in Group 1 (aOR = 0.76, 95% CI [0.58, 0.98]) while those in Group 2 showed no significant difference (Table 4). There was no significant difference in terms of receiving ADHD behavioral treatment.
Association Between Parental Nativity and ADHD Medication and Behavioral Treatment Among Children Diagnosed With ADHD, 2016 to 2019 National Survey of Children’s Health (n = 11,063).
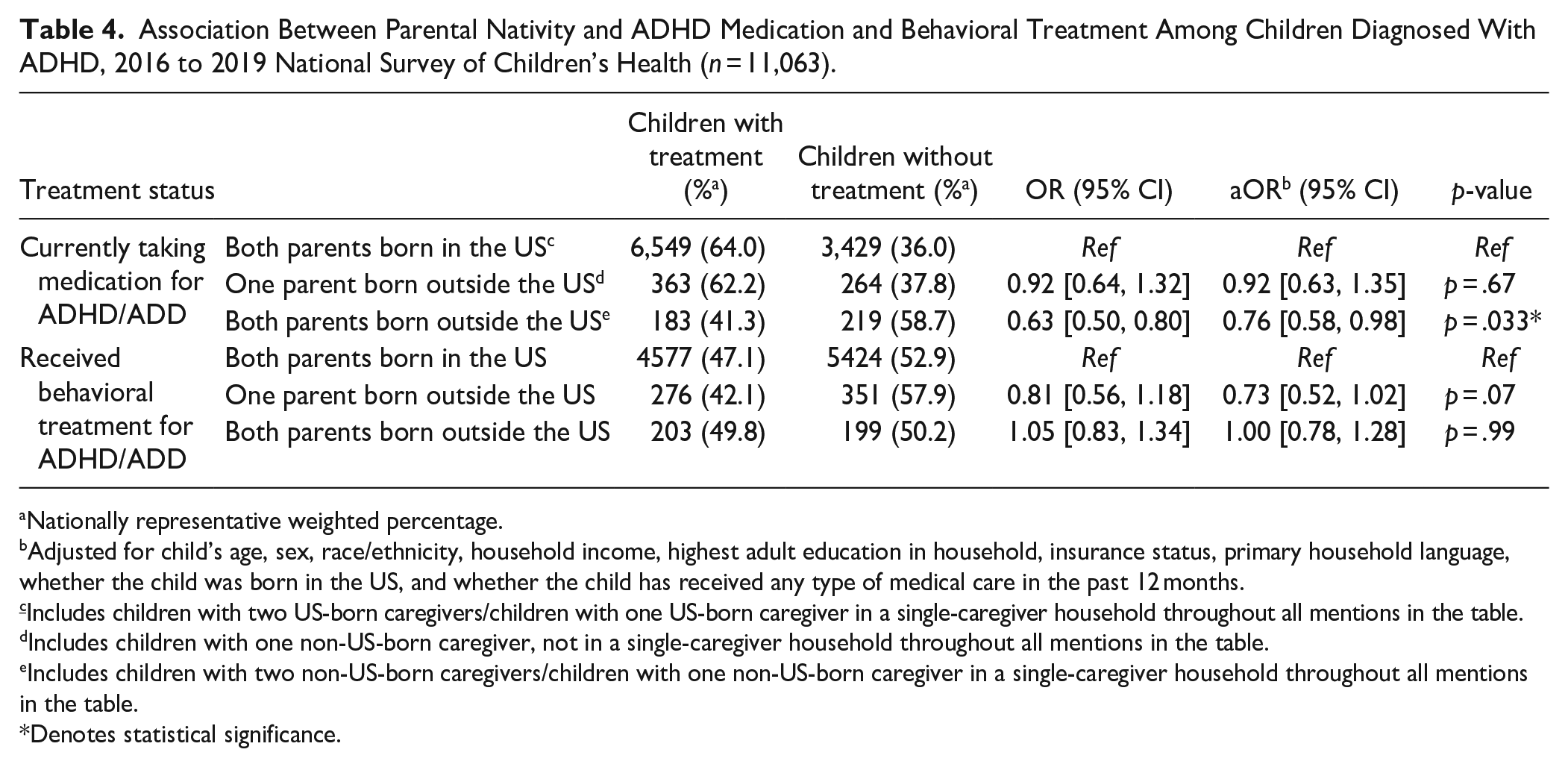
Nationally representative weighted percentage.
Adjusted for child’s age, sex, race/ethnicity, household income, highest adult education in household, insurance status, primary household language, whether the child was born in the US, and whether the child has received any type of medical care in the past 12 months.
Includes children with two US-born caregivers/children with one US-born caregiver in a single-caregiver household throughout all mentions in the table.
Includes children with one non-US-born caregiver, not in a single-caregiver household throughout all mentions in the table.
Includes children with two non-US-born caregivers/children with one non-US-born caregiver in a single-caregiver household throughout all mentions in the table.
Denotes statistical significance.
Discussion
In this analysis of a large, nationally representative dataset of children ages 3 to 17, ADHD was less likely to be diagnosed if the child had one or two non-US-born caregivers. Additionally, ADHD had one of the lowest likelihoods for a diagnosis in comparison with nine other common developmental, behavioral, and mental health conditions. However, relative to the children with two US-born caregivers, the likelihood of an ADHD diagnosis increased as the non-US-born caregivers spent more time in the US. Lastly, we found that children with all non-US-born caregivers were less likely to be taking ADHD medications following a diagnosis, but we did not find significant differences in receiving behavioral treatments.
The findings of this study indicate a pressing need for more medical attention from the pediatric community toward the population of children with non-US-born caregivers. Compared to children of US-born caregivers, these children were less likely to receive an ADHD diagnosis, regardless of whether they had one or two non-US-born caregivers. These results concur with two similar studies on the association between ADHD and immigration from Sweden and Denmark (Osooli et al., 2021; Sahuric et al., 2021). Using a nationwide retrospective cohort, Osooli et al. (2021) reported lower risk of ADHD among immigrant groups, although there was variation depending on the parents’ countries of origin. Similarly, Sahuric et al. (2021) found that immigrant parents were less likely to report symptoms of ADHD, while teachers observed equal amounts of ADHD between native and non-native students. Notably, Sahuric et al. relied on ADHD symptoms rating rather than clinical diagnoses. However, there was a discrepancy between our findings and a nested, case-control study from Finland, which reported increased likelihood of ADHD diagnoses in children of two immigrant parents and of one immigrant father (Lehti et al., 2016). These contradictory results might be explained by the barriers to healthcare access for immigrants in the US as well as significant differences in terms of the make-up and size of the immigrant populations when comparing the US, Sweden, Norway, and Finland (Derose et al., 2007; Gelatt, 2016; OECD, 2017; Wafula & Snipes, 2014). Although our study controlled for whether the child had received medical care in the last year in an effort to adjust for differences in healthcare access, more research is needed in order to illuminate the underlying causes for such disparate results.
The differences between diagnosis rates for children of US-born versus non-US-born caregivers could potentially be attributed in part to the significant challenges in the identification of ADHD. Previous research efforts have demonstrated that geographic regions around the world had a different prevalence and understanding of ADHD as a medical condition (Amaral, 2007; Polanczyk et al., 2007; Slobodin & Masalha, 2020). Specifically, Polanczyk et al. (2007) showed in their worldwide meta-analysis that regions such as Asia, the Middle East, and Europe had lower estimated prevalence of ADHD. It has also been suggested that tolerance for certain behaviors associated with ADHD might vary cross-culturally, which can potentially lead to different perceptions of the condition (Gómez-Benito et al., 2019). Thus, caregivers who moved and raised their child in the US may face substantial difficulties in interpreting their child’s behavior according to new social and cultural norms; parents of different cultures typically have different perceptions of what is considered to be typical or developmentally appropriate behavior (Slobodin & Masalha, 2020). In the US, an ADHD diagnosis requires clinical symptoms in at least two settings, such as at school, home, or interactions with friends or relatives (CDC, 2020). Consequently, non-US-born caregivers may overlook or fail to identify the typical clinical symptoms of ADHD in their children in settings where physicians do not have a complete understanding of the children’s behaviors, potentially leading to inconsistent information for a diagnosis. Moreover, a large portion of immigrants are considered to be ethnic minorities in the US (Budiman, 2020). Previous research has shown that American parents of an ethnic minority have different perceptions of ADHD than Caucasian American parents (Slobodin & Masalha, 2020). Additionally, the current ADHD identification methodology, which is heavily reliant upon White middle-class reference groups, standard questionnaires, and clinical observations, might not account for the process of acculturation, placing children of minority groups at a disadvantage (Serra-Pinheiro et al., 2008; Slobodin & Masalha, 2020). Lastly, these results reflect wide variations in parental explanatory models of the source of ADHD as well as the general lack of receptivity to mental health conditions, treatments, and services that exists in some cultural backgrounds (Bussing et al., 2003).
The likelihood of an ADHD diagnosis was also among the lowest in comparison to that of other conditions included in the NSCH. Although our study focuses specifically on ADHD, it is noteworthy that for almost all other developmental, behavioral, and mental health conditions that were used as comparison points, the likelihoods of diagnosis for children of non-US-born caregivers were lower than that of children of US-born caregivers. As the share of US immigrants in the population is projected to continue growing, these findings potentially reaffirm a structural lack of medical and behavioral health access in immigrant communities and the difficulties they face in obtaining adequate medical services (Budiman, 2020; Derose et al., 2009; Goldman et al., 2006). Without an official diagnosis from a medical provider, children with ADHD or other developmental conditions are met with significant barriers in receiving educational accommodations under a 504 plan, potentially leading to even greater educational deficits (U.S. Department of Education, 2011; NYC Department of Education, n.d.).
Interestingly, our study results showed that the length of time that non-US-born caregivers spent in the US could modify the relationship between ADHD diagnosis and migration status. For the timeframes examined in this analysis, the likelihood of an ADHD diagnosis was lowest if the caregivers had spent less than a decade in the US and highest if the caregivers had spent over 30 years in the US. The same trend was observed for children with one caregiver born outside the US, with ADHD diagnosis likelihood increasing when they spent more time in the country. These results add another dimension to our understanding of how immigrants assimilate in the US. It has been well established that after arriving in the US, immigrants converge to the same level of health as the American population across decades and generations (Markides & Rote, 2019). Substantial cultural assimilation also occurs for immigrants to the US, with language, attitudes, and cultural practices shifting toward the US norm (Abramitzky et al., 2020; Lalami, 2017). Our results suggest that in addition to these aspects of assimilation, attitudes toward certain culture-bound syndromes or toward utilization of healthcare and educational resources to treat mental/behavioral conditions may also shift over time for immigrant populations. Immigrants who have spent more time being exposed to American people, healthcare systems, school systems, language, and culture may be more likely to identify or interpret their child’s symptoms as concordant with the US cultural understanding of conditions like ADHD.
In terms of utilizing available treatments for ADHD, only children in Group 3 were less likely to take medication after being diagnosed with ADHD, but there were no differences in likelihood of receiving behavioral treatment. The results regarding behavioral treatment concur with previous research on ethnic differences in ADHD treatment, which showed that ethnic minority parents rated behavioral treatments higher than Caucasian American parents (Pham et al., 2010). A previous study utilizing data from the 2016 NSCH survey also found that children with at least one foreign-born parent were less likely to receive mental/behavioral health treatment, including medication or counseling (Rosenberg et al., 2020). It has been shown that fewer children diagnosed with ADHD received behavioral therapy compared to other treatment modalities, which might potentially impact the validity of this finding (Visser et al., 2015). However, the significant difference in ADHD medication use for children in Group 3 is concerning. Even after receiving an ADHD diagnosis, children of two non-US-born parents had a lower likelihood of taking ADHD medication. Similarly, a previous study of children in Germany found a significantly lower prevalence of ADHD medication use among children of immigrant families compared to children with non-immigrant parents (Knopf et al., 2012). Our study expands on this finding by examining medication use among children with ADHD who have non-US-born parents. This finding is perhaps due to a lack of healthcare services for this population or differing cultural attitudes toward ADHD medication use among non-US-born caregivers. Further research may investigate the reasons for differences in ADHD medication use among this population.
Our study is the first to use a nationally representative dataset of 109,881 children to examine the likelihood of an ADHD diagnosis in the US. Our combined 2016 to 2019 NSCH dataset is one of the largest and most comprehensive datasets on pediatric well-being and health outcomes to date, which improves the generalizability of our findings to the general population. The information about health conditions gathered by the NSCH also utilizes diagnoses from physicians or other professional healthcare providers, which reduces the potential for any reporting bias from parents. Additionally, the broad range of health conditions and demographic information gathered allows for reliable comparison between diagnosis rates for different conditions and enables us to control for potential sociodemographic confounders in our analytic models.
However, our study is still subject to limitations. The NSCH is inherently limited by the reliance on caregiver reports for all questions. However, because the query asks for a medical provider’s diagnosis, the responses are less likely to be influenced by bias on the caregiver’s part. As with all retrospective cross-sectional analyses, there may have been residual confounders that were not readily available through the NSCH or not included in our analysis. Despite our efforts to control for sociodemographic characteristics and use of medical care, these may not completely encompass structural barriers to care or underlying caregiver characteristics that may have affected the results. For instance, family history of ADHD (or other mental/behavioral health conditions) and the amount of time that the caregiver has spent with the child are potential confounders that were not evaluated. The grouping “non-US-born caregivers” also encompasses a heterogenous population that may not reflect the challenges that specific groups face. Most notably, the NSCH does not ask questions about important immigration-related family characteristics (such as the caregivers and child’s legal immigration status) or the caregivers’ race and country of origin, which may have impacted our findings. For instance, a caregiver could be born outside of but raised in the US; thus, the “non-US-born” label would not accurately reflect the cultural and geographical concordance between the parent and the child’s upbringing. The lack of this information in the NSCH also prevents us from correlating these results to the ADHD diagnosis rate in the parents’ country of origin or making more granular conclusions about culturally specific attitudes toward ADHD. Additionally, immigration status can be a substantial barrier to help seeking; for instance, green card or visa holders whose status is unclear, or those whose legal immigration status has not been established, may be less likely to seek medical care. Between 2016 and 2019, the US government’s particularly stringent immigration policies may have been a particular deterrent to care-seeking, especially among Spanish-speaking families and immigrants of color.
Future research may investigate public health education measures, social support groups, and classroom accommodations specifically targeting immigrant communities to raise awareness about the identification and treatment of ADHD. Researchers may also study differences in ADHD diagnoses among specific immigrant communities and differences in cultural interpretations of ADHD symptoms. Because current methods of diagnosing ADHD rely heavily on parent and teacher reports, future work can aim to develop a more reliable and culturally sensitive ADHD identification methodology that involves simultaneous assessments from parents, teachers, physicians, and other healthcare providers in order to build confidence in non-US-born caregivers to seek out necessary and timely interventions. Lastly, healthcare professionals and policymakers should strive to decrease the overall barriers of care that face immigrant communities.
Conclusion
In this study, we find that children of non-US-born caregivers were less likely to be diagnosed with ADHD, even after controlling for potential confounders. The likelihood of an ADHD diagnosis for children in this population was also one of the lowest compared to nine other common developmental, behavioral, and mental health conditions. However, ADHD diagnosis rates increased as caregivers spent more time in the US. While there was no significant difference in receiving behavioral treatments following a diagnosis, children with two non-US-born caregivers or a single non-US-born caregiver were less likely to be taking medication after an ADHD diagnosis. These findings emphasize the need for increased effort toward ADHD identification, education, and medical and social services for children of non-US-born caregivers to ensure that they receive the necessary support and care to thrive.
Footnotes
Acknowledgements
We would like to thank Dr. Andrew Adesman and Dr. Charles Schleien for their continued support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.