
Abstract
Background:
ADHD and ASD are associated with dermatologic manifestations, yet little research investigates co-occurring ADHD/ASD and common dermatologic conditions.
Objective:
To investigate associations between ADHD, ASD, acne vulgaris, and atopic dermatitis.
Methods:
Using de-identified patient records from the TriNetX database, we created four cohorts on ADHD diagnosis, ASD diagnosis, both, neither. Cohorts were separated into males and females. We balanced each cohort based on age, sex, race, and ethnicity to the baseline cohort with neither ASD or ADHD. Finally, we examined prevalence of acne and eczema.
Results:
The cohort sizes varied from 19,764 to 345,626. Compared to matched peers, males with ADHD or ADHD/ASD had increased prevalence of acne, and all neurodivergent males had increased prevalence of eczema. Females with ADHD had an increase in both. Females with ADHD/ASD had no significant differences, and females with ASD had a decreased risk of eczema.
Limitations:
Due to database limitations, we are unable to: analyze symptom severity, skincare routine, or treatment adherence.
Conclusions:
The decreased risk of eczema in females with ASD and lack of significant difference in incidence of acne or eczema in females with ADHD/ASD compared to matched peers suggests research into approaches to skincare in males versus females with ASD may provide clinically relevant insights.
Take Aways
ADHD/ASD patients may struggle with organizational skills required to follow recommended dermatologic care, potentially contributing to an increase in eczema or acne.
Decreased risk for both conditions in ASD indicates research into skincare routines for neurodivergent individuals may provide valuable insights for providers treating these patients in their practice.
Introduction
Attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) are neurodevelopmental conditions with some overlap concerning the impacts on interpersonal relationships, executive functioning, associated comorbidities, and more. ADHD is characterized by inattention, hyperactivity, and impulsivity, whereas communication difficulties, fixed interests, and repetitive activities/behaviors mark ASD. Both conditions present differently across individuals and, in some, lead to functional impairment (Hours et al., 2022). Though the pathophysiology of ADHD and ASD present with different neurofunctional deficits, there appears to be an association between both conditions and dermatologic manifestations, specifically with acne vulgaris and atopic dermatitis. The goal of this paper is to characterize the associations between either ADHD or ASD to acne vulgaris and atopic dermatitis.
Acne and atopic dermatitis, also known as eczema, are two common cutaneous conditions. The healthcare expenditure for treatment and lost productivity due to acne and eczema in the United States were $1.2 billion and $442 million in 2013, respectively (Burden of Skin Disease, n.d.). Acne is a chronic inflammatory disease involving sebaceous glands, with lesions typically classified as papules and pustules (Bhate & Williams, 2013). Acne predominantly occurs in adolescents around puberty, notably affecting 85% of those aged 12 to 24, but it can also present later in adulthood (Bhate & Williams, 2013). A retrospective cross-sectional study found that acne was 2 times more likely to be associated with ADHD compared to other dermatological conditions, even when controlling for potential confounders such as stimulant medication use, mood disorders, age, sex, and a prior diagnosis of atopic dermatitis (Gupta et al., 2014). Regarding ASD, a study using regression analysis found that in male and female patients with ASD, higher levels of androstenedione were detected compared to both control groups (Mann-Whitney W = 2677, p = .002). Androstenedione is a precursor for testosterone, dihydrotestosterone, and estrogen in hormone-sensitive organs such as the skin. Higher androgen levels can lead to increased sebum production and inflamed pilosebaceous glands, the hallmark of acne.
Eczema is an inflammatory cutaneous condition with a 20% lifetime prevalence, whereby 80% of affected individuals develop it before age 6 (Nemet et al., 2022; Weidinger et al., 2018). Concerning ADHD, a study using population-based surveys of 354,416 children in the United States found that eczema was associated with an approximately 50% increased risk of later acquiring ADHD compared to those without eczema (Strom et al., 2016). Adverse sleep could partly explain the increased association of ADHD in those with eczema. However, there may be more mechanisms influencing the association between eczema and ADHD that are unknown. ASD is also associated with skin manifestations like eczema (Jameson et al., 2022). A study examining the association between symptom severity of ASD and atopic conditions (eczema, allergies, asthma, and hay fever) found that children with atopic conditions were 2.4 times more likely to have increased disease severity of ASD compared to the non-atopic cohort based on the ADOS-2 assessment tool. Furthermore, one-tailed statistical analysis revealed that children with comorbid eczema presented with increased ASD symptom severity compared to both the non-atopic cohort and those with other atopies, not including eczema (Jameson et al., 2022). Analyzing the combined findings of such studies may elucidate the relationships between acne, eczema, ADHD, and ASD in males and females and serve as a starting point for further research.
The treatments for acne and eczema warrant engagement with healthcare providers and adherence to prescribed regimens. Regarding acne, healthcare providers will carefully assess the type and severity of lesions, the presence of acne-related complications, and other contributing factors to customize acne treatments for each patient. Topical retinoids stand as the primary treatment option for mild-to-moderate acne vulgaris, both for initial therapy and long-term maintenance. Depending on acne severity, retinoids may be administered alone or in conjunction with benzoyl peroxide and topical or oral antibiotics. Inflammatory acne unresponsive to topical treatments may necessitate oral antibiotics, but it is crucial not to rely on topical or oral antibiotics as singular therapy. Furthermore, providers may incorporate oral contraceptives and/or spironolactone into the treatment regimens of females with acne. In severe cases characterized by extensive nodules, oral isotretinoin is preferred. At the same time, oral isotretinoin is frequently employed for moderate cases with visible scarring, significant psychological distress, or failed prior treatment attempts (Ingram et al., 2010; UpToDate, n.d).
Improvement in acne may take time as it involves resolving existing lesions and preventing new ones. Some regimens may take several months, and initial results may show a reduction in lesions rather than complete clearance. Adjustments to the treatment plan are typical due to varying responses. Long-term maintenance with topical retinoids is often necessary for sustained results (Leung et al., 2021). In addition to medically treating acne, it is essential to consider general skincare alterations. This includes using gentle skin cleansers, avoiding aggressive scrubbing, and choosing non-comedogenic products. Refraining from picking acne lesions is crucial to prevent scarring (Ingram et al., 2010a; Leung et al., 2021; UpToDate, n.d.)
The primary therapy for managing atopic dermatitis flare-ups and maintenance involves using emollients. For flare-ups, topical corticosteroids serve as the first-line treatment. In moderate to severe atopic dermatitis cases, topical calcineurin inhibitors can be considered first-line treatment combined with topical steroids. Second-line treatment options include Ultraviolet B phototherapy for moderate to severe atopic dermatitis. Furthermore, current guidance suggests that patients with atopic dermatitis have a once-daily bath with lukewarm water, limited to 5 to 10 minutes. Following these recommendations can help effectively manage atopic dermatitis symptoms (Frazier & Bhardwaj, 2020; Weidinger et al., 2018; Yim et al., 2021).
The skincare interventions for acne and eczema are intended for long-term maintenance, and patients with ADHD and ASD may struggle with the organizational skills required to establish appointments or comply with recommended care, thus potentially further contributing to lost productivity and an increase in the psychological burden of these skin conditions.
Our study is the first to examine the association between ASD, ADHD, and two of the most common skin disorders. As the prevalence of those with either ADHD or ASD has increased, so too have many cutaneous disorders, with several studies finding significant associations between allergic disorders (“asthma, rhinitis, conjunctivitis, skin, food, or drug allergy”) and ADHD or ASD (Nemet et al., 2022). Awareness of the symptoms that characterize ADHD and ASD can grant insight into how patients with these neurodevelopmental disorders interface with the healthcare system and adhere to recommended treatments. In understanding how these conditions may impact the patients’ ability to execute a dermatologic treatment regimen as advised, providers may find that changing certain aspects of the treatment regimen for acne and/or eczema in individuals with ADHD and/or ASD result in improved patient outcomes. For example, changing the texture of a topical treatment, adjustments in dosing and frequency, and discussing what small changes in their daily lives could increase adherence to the prescribed regimen could contribute to improved patient-provider relationships in patients with ADHD and/or ASD, thus encouraging equity.
Methods
This study was a retrospective examination of de-identified data from the TriNetX research database. TriNetX contains electronic medical records from nearly 60 large healthcare organizations and contains more than 90 million individual patient records. This proprietary database is available to institutions who contribute to the dataset and can be accessed by researchers at those institutions who adhere to their university policies; thus, it has been well-established for medical research, including but not limited to ADHD comorbidities, (Walsh et al., 2022) cardiovascular illness (Singer et al., 2022), and surgical outcomes (Yoon et al., 2022), to name a few. TriNetX, LLC is compliant with the Health Insurance Portability and Accountability Act (HIPAA), the US federal law which protects the privacy and security of healthcare data, and any additional data privacy regulations applicable to the contributing HCO (TriNetX, n.d.). TriNetX is certified to the ISO 27001:2013 standard and maintains an Information Security Management System (ISMS) to ensure the protection of the healthcare data it has access to and to meet the requirements of the HIPAA Security Rule. Any data displayed on the TriNetX Platform in aggregate form, or any patient level data provided in a data set generated by the TriNetX Platform only contains de-identified data as per the de-identification standard defined in Section §164.514(a) of the HIPAA Privacy Rule (TriNetX, n.d.).
We identified all patients under the age of 26 between Jan 18, 2003 and Jan 18, 2023, as the data were extracted on Jan 18, 2023. From this patient population, we separated initially into four cohorts based on presence of an ADHD diagnosis (ICD: F90), an ASD diagnosis (ICD: F84), both, and neither. The group with only ADHD is the “ADHD” cohort, the group with only ASD is the “ASD” cohort, the group with both diagnoses is the “both” cohort, and the group with neither is the “neurotypical” or “NT” cohort. We then separated each group into males and females based on data from the corresponding record. Demographic information has been provided in Supplemental Table S1. The events of interest in this study were identified as follows: “acne” (ICD-10: L70); “atopic dermatitis,” also called “eczema” (ICD-10: L20).
We performed two sets of analysis using the TriNetX statistical software. First, we established the overall prevalence of our events by comparing the base rate of acne and eczema within each group. The results of this set of analysis are presented in Tables 1 and 2 and Figure 1. For this analysis, we did not control for any variables within the cohorts. Following this analysis, we sought to isolate the effect of neurodivergent diagnoses on the skin disorders. We established the “NT” group as the baseline. We then balanced each subgroup to this baseline cohort based on age, sex, race, and ethnicity using nearest-neighbor matching to a difference between propensity scores <0.1 (TriNetX, n.d.). The identified characteristics utilized in nearest-neighbor matching, as well as pre- and post- matching t-test values for these characteristics, are presented for each sub-group in Supplemental Table S1. The outcome of this methodology was that each patient within a sub-group had a peer in the “NT” cohort who had no significant difference based on age, sex, race, or ethnicity.
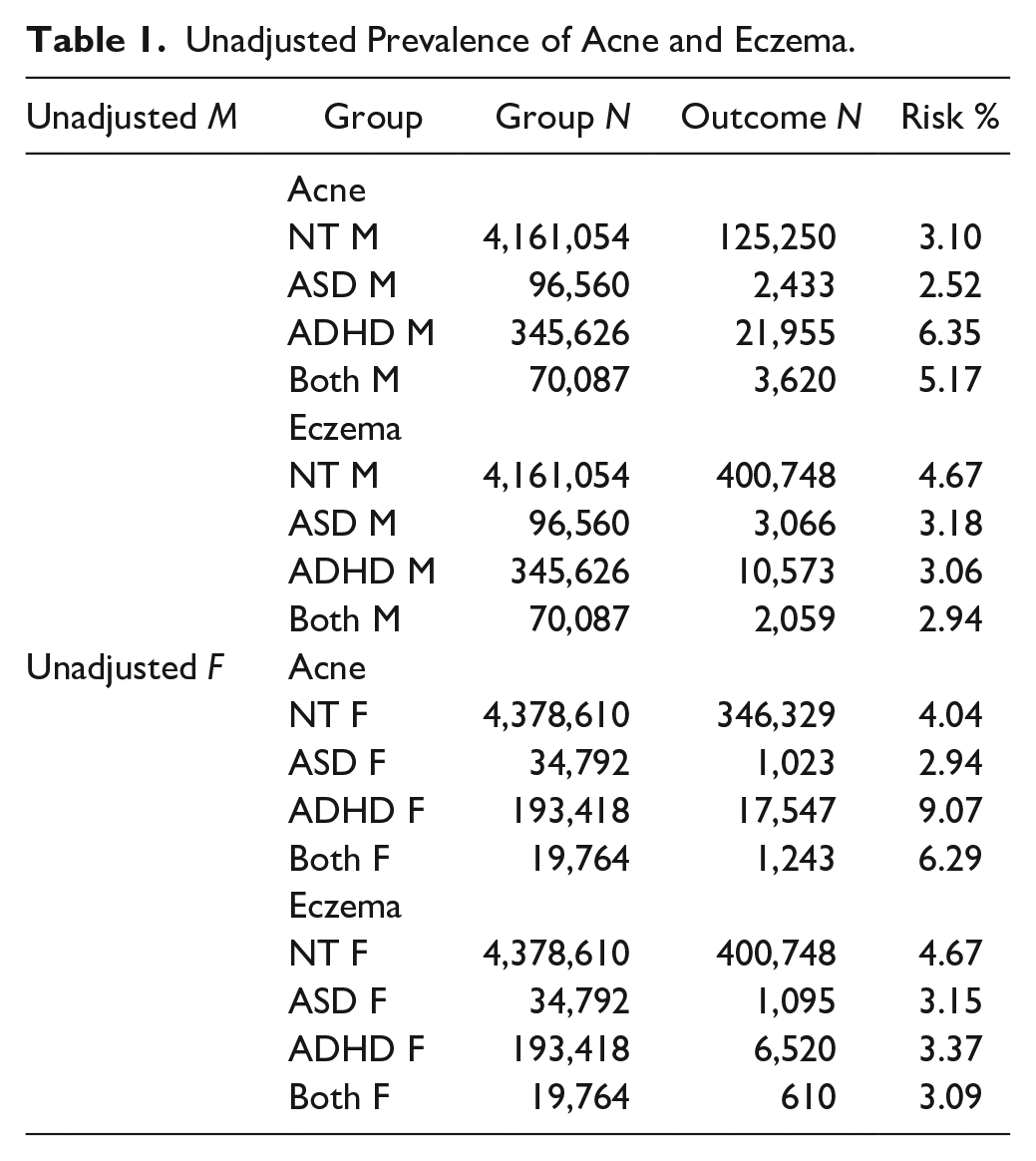
Unadjusted Prevalence of Acne and Eczema.
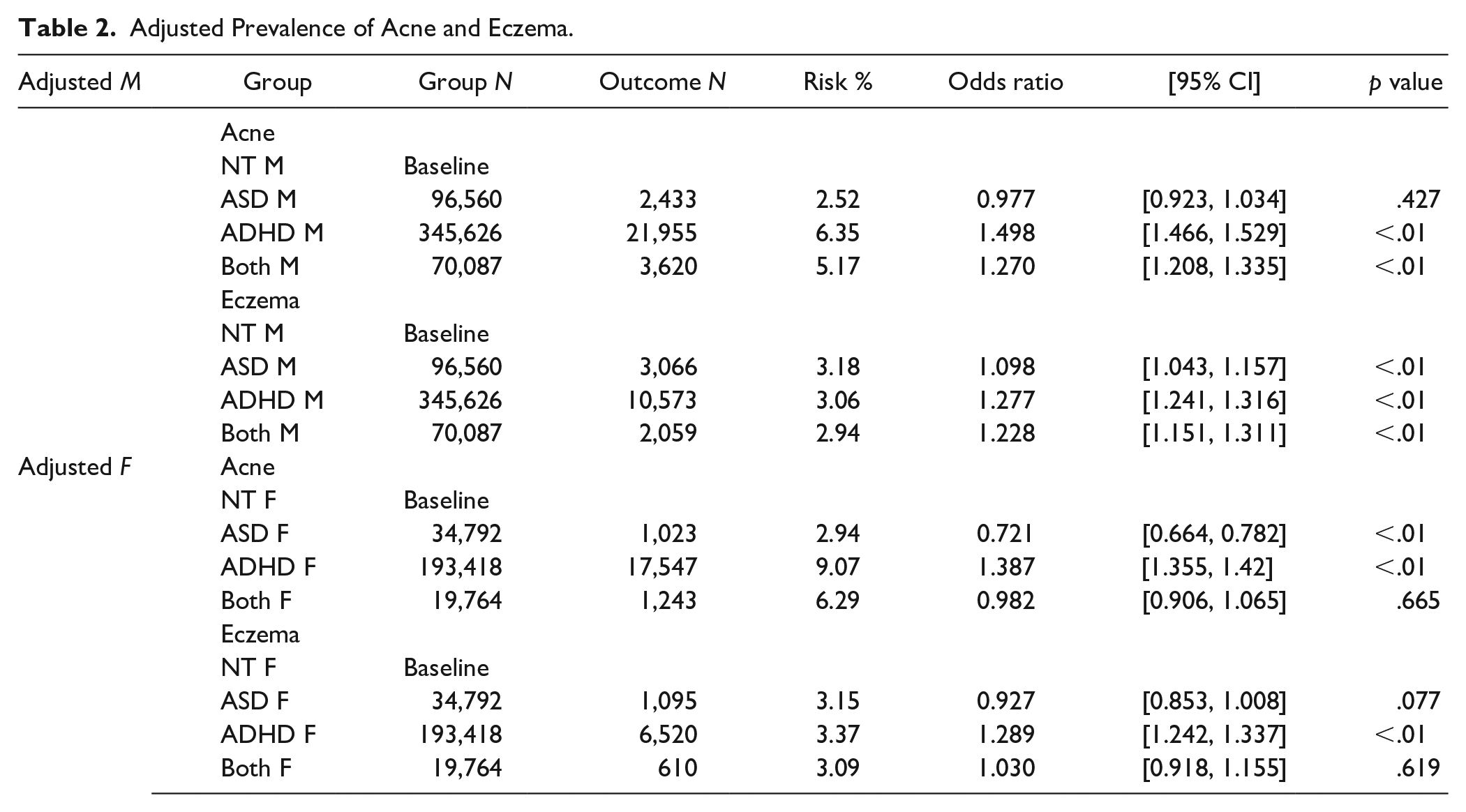
Adjusted Prevalence of Acne and Eczema.
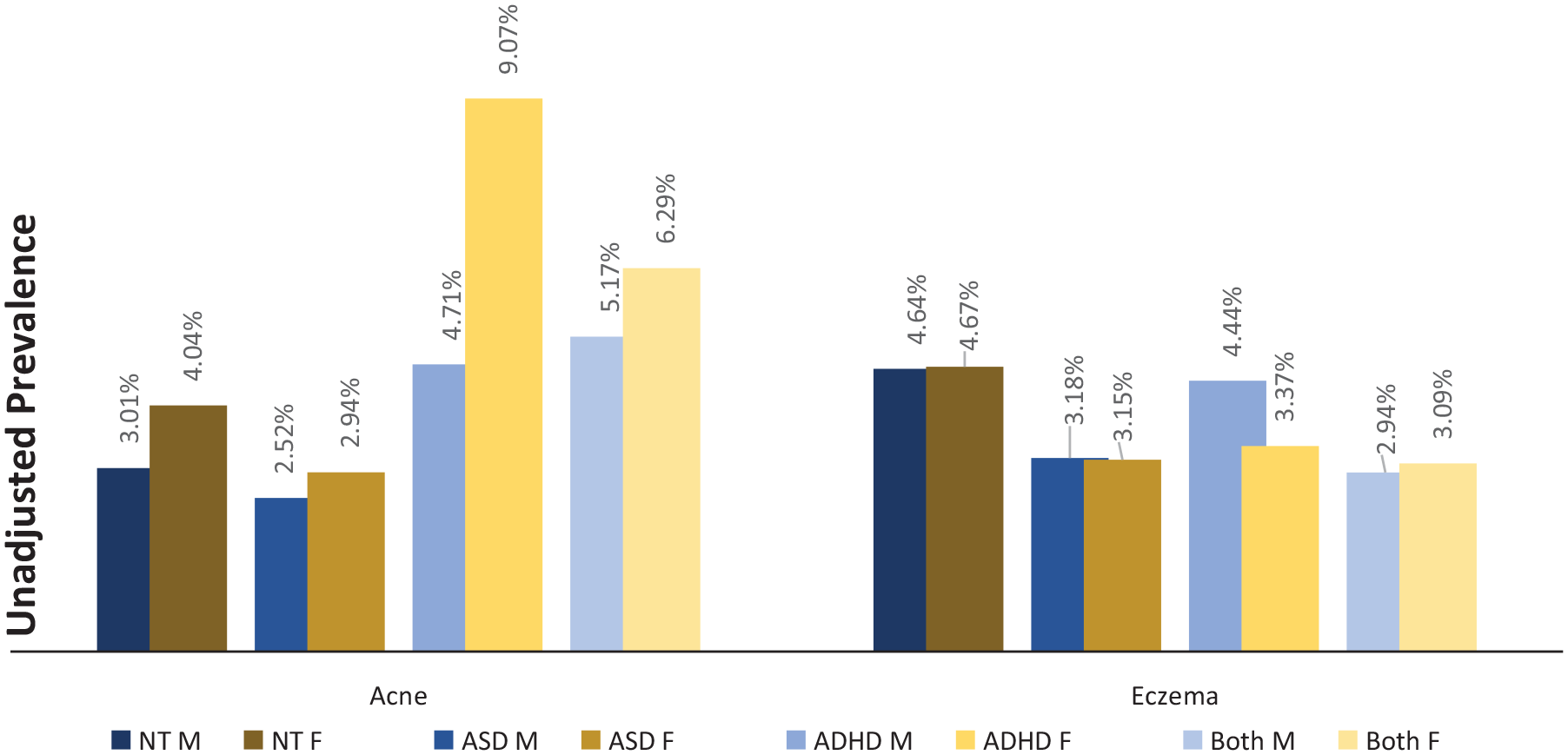
Unadjusted prevalence of acne and eczema in NT males and females and males and females with ASD, ADHD, or both.
Once the cohorts were balanced, event rates were extracted from the relevant patient records, and odds ratios with 95% confidence intervals were calculated from the given incidence of each event. The baseline event rate for the “NT” cohort is not provided, as the individuals analyzed varied based on matching to the relevant sub-group. For example, when analyzing the “ASD M” group which had 96,560 individuals, another 96,560 individuals were extracted from the overall “NT” cohort based on nearest-neighbor matching as above. The results of this set of analysis are presented in both table and graph form in Table 2 and Figures 1 to 3. Significance for this study was set at a two-tailed p-value <.05. As this study contained only deidentified aggregate data, the Colorado Multiple Institutional Review Board (COMIRB) designated it as non-human research not in need of approval.
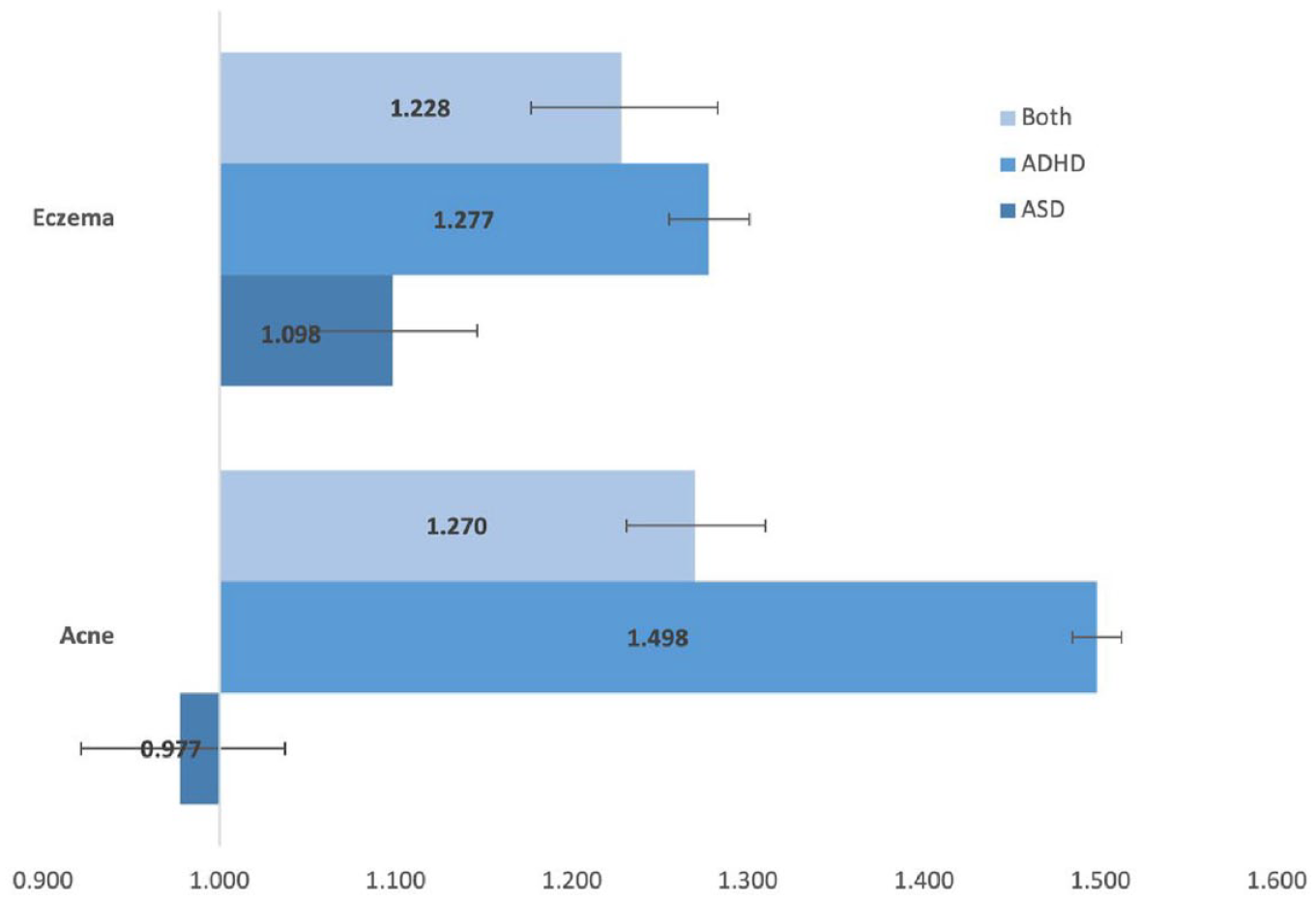
Adjusted odds ratio for males.
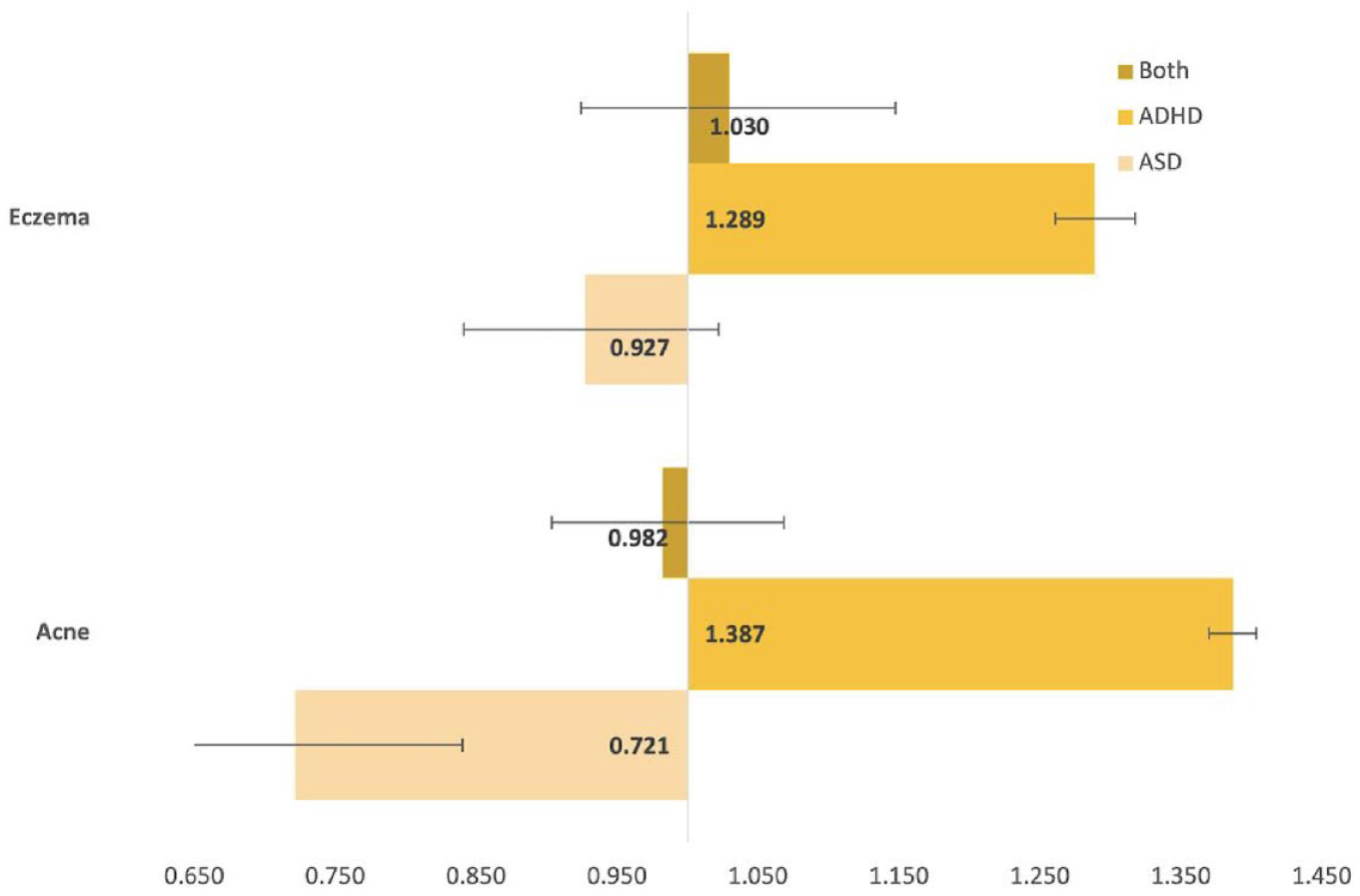
Adjusted odds ratio for females.
Results
The original size of each cohort is included in Tables 1 and 2. The unmatched, unadjusted analysis revealed a range of prevalence for acne from 2.52% in males with ASD, to 9.07% in females with ADHD. The same analysis revealed a range for eczema from 2.94% in males with both ADHD and ASD, to 4.67% for neurotypical females.
After matching, the cohort sizes varied from 19,764 to 345,626. Compared to neurotypical peers with no differences in age, sex, race, or ethnicity: males with ASD had an insignificant difference in likelihood of acne, and an increased risk of eczema (OR: 1.098, p < .001); males with ADHD had an increased risk of both acne (OR: 1.498, p < .001) and eczema (OR: 1.277, p < .001); males with both ASD and ADHD had an increased risk of both acne (OR: 1.270, p < .001) and eczema (OR: 1.228, p < .001); females with ASD had an insignificant difference in likelihood of eczema, and a decreased risk of eczema (OR: 0.721, p < .001); females with ADHD had an increased risk of both acne (OR: 1.387, p < .001) and eczema (OR: 1.289, p < .001); females with both ASD and ADHD had insignificant differences for both acne and eczema; detailed results are in Table 2. Figures 2 and 3 present visual depictions of odds ratios and confidence intervals between the relevant neurodivergent cohort and the corresponding neurotypical cohort.
Discussion
In this matched peer retrospective cohort study, acne and eczema had significant associations with neurodiversity. Our controlled analyses showed neurodivergent males were more likely to be diagnosed with eczema and acne than neurotypical males, except for males with ASD only, in which there was no significant difference. Interestingly, our analyses also showed females with ADHD only were more likely to experience eczema and acne. At the same time, females with ASD or both ASD/ADHD had insignificant differences for most diagnoses.
Our findings align with prior research, which has found that ADHD bares a substantial impact on hygiene and self-care routines (du Rietz et al., 2020). The prevailing hypothesis is that the consistency inherent in self-care and hygiene is at odds with the impulsivity and time management difficulties found in ADHD (Schoenfelder & Kollins, 2016). Consequently, some individuals with ADHD experience a higher rate of preventable health events (Ehlers et al., 2019; Libutzki et al., 2019). Based on our findings, the ADHD-only cohort was most likely to be diagnosed with eczema and acne, regardless of gender. Compared to males without ASD or ADHD, males with ADHD were approximately 1.3 times and 1.5 times more likely to experience eczema and acne, respectively. Similarly, females with ADHD were about 1.3 times and 1.5 times more likely to experience eczema and acne than neurotypical females. Given that skincare routines can often involve a multi-step, daily process, it is conceivable that those with ADHD may find it more challenging to adhere to a recommended preventive treatment (Ingram et al., 2010). Furthermore, drastic shifts in diet, environment, and activity level may worsen eczema and acne (Vickery, 2007; Webster, 2007). ADHD frequently drives individuals to seek out novel experiences and engage in impulsive behaviors, which may relate to inciting events for periods of intense acne or eczema (Hale et al., 2022; Langan & Williams, 2006; Magin et al., 2005; Soldati et al., 2020). ADHD is also strongly associated with increased sexual behaviors, including masturbation, which has been demonstrated to increase acne in males and may explain some of the gender-based differences in our data (Hale et al., 2022). While it is unknowable from our current data, our increased rates of skin disorders in this population may correspond to decreased preventive habits and increased predisposing behaviors.
While those with ADHD had higher rates of both skin disorders, ASD seemed to have a mitigating effect. The male cohort with co-morbid ASD and ADHD had increased rates of eczema and acne compared to neurotypical males; however, the analogous female group did not significantly differ in either cutaneous disorder. Additionally, males with ASD alone were more likely to have eczema but no significant difference in acne. In contrast, females with ASD had no difference in eczema and had decreased rates of acne compared to neurotypical females. While the literature speaks less to skincare and routine health maintenance in those with ASD, the most plausible explanation for our findings relates to the behaviors found in ASD. In contrast to the resistance to routines found in ADHD, the DSM-5 criteria for ASD include “excessive adherence to routines”(American Psychiatric Association, n.d.). These routines frequently apply to non-hygiene tasks; however, previous research has suggested that individuals with ASD may exhibit high adherence rates to prescribed treatment regimens (Kloosterboer et al., 2021). Consistent adherence to preventive regimens can be curative for acne and significantly reduce the severity of eczema episodes, although some may still occur (Magin et al., 2005; Yim et al., 2020). Our findings support ASD as a mitigating factor in eczema and acne, revealing that individuals with both ASD and ADHD were consistently less likely than individuals with only ADHD and more likely than individuals with only ASD to experience eczema or acne.
The data presented in our study have implications for many healthcare providers and individuals with ADHD or ASD. The association with acne and eczema found in those with ADHD may indicate an opportunity for providers to aid this unique patient population further. Patients with ADHD struggle with routine tasks, particularly those that do not have an immediate benefit (Mücke et al., 2021). Unfortunately, skincare may have a direct cost of time and effort with delayed benefits; however, dermatologists, psychiatrists, and primary care providers may overcome this uneven cost-benefit analysis perceived by patients through suitable communication. Visual aids, narrative stories, and clear statistical information on risks have all shown usefulness in mitigating risk-benefit alterations in ADHD and similar disorders (Aljubour et al., 2022; Bellani et al., 2011; Sleath et al., 2014). While we do not advocate graphic exaggeration, providers may find it helpful to describe and display a vivid case of acne scarring or lichen simplex chronicus, complications of acne, and eczema, respectively, to emphasize the importance of adhering to a patient-centered skin care regimen (UpToDate, n.d.; Yim et al., 2021).
As with all studies, our study does have limitations. Namely, the nature of database studies on deidentified data posits restrictions. Without identifying individuals, we are unable to analyze the severity of ADHD or ASD symptoms or to analyze the corresponding burden of acne or eczema. Similarly, we were unable to adjust for specific geographical data for patients, so it may be that certain patients lived in areas with significantly higher humidity, UV index, or average temperature, all of which impact skin disorders (Bhate & Williams, 2013; Langan & Williams, 2006). Finally, most individuals in our sample were white, which limits the generalizability to patients of other races. However, the statistical strength supplied by our large cohort size mitigates the impact of these limitations.
Our study is the first to examine the association between ASD, ADHD, and two of the most common skin disorders. The overall increased risk of acne and eczema in patients with ADHD has utility for a wide variety of providers, including dermatologists, psychiatrists, and primary care providers, as well as the patients themselves. The decreased risk in those with ASD suggests that further research into skin care in this population may provide valuable insights. As the number of individuals with ADHD and ASD grows and providers become more likely to encounter these patients in their practices, awareness of associated dermatologic conditions is critically important as it may ultimately lead to improved communication and collaboration between physician and patient.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231197236 – Supplemental material for Co-occurring ASD Mediates Impact of ADHD on Atopic Dermatitis and Acne: A Retrospective Cohort Study
Supplemental material, sj-docx-1-jad-10.1177_10870547231197236 for Co-occurring ASD Mediates Impact of ADHD on Atopic Dermatitis and Acne: A Retrospective Cohort Study by Karima M. Osman, Pauline Gerard and Elijah W. Hale in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Status
Designated not in need of review by COMIRB.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.