
Abstract
Objective:
Internalizing and externalizing problems predict poor academic and social outcomes. However, ADHD co-occurs with internalizing and externalizing problems and is itself a risk factor, thus preventing precise inferences. This study evaluated childhood anxiety, depression, and aggression as predictors of change in adolescent academic and social outcomes, including moderation by childhood ADHD.
Methods:
182 ethnically-diverse 5- to 11-year-old youth with (54.7%) and without (45.3%) ADHD completed a separate baseline and 6- to 7-year prospective follow-up assessment, consisting of parallel measures across youth psychopathology, academic functioning (i.e., academic achievement, school competence), and friendship quality domains.
Results:
Whereas childhood ADHD inversely predicted academic competence, depression and aggression uniquely predicted worsening friendship quality. Interestingly, anxiety was unrelated to change in academic and friendship outcomes; similarly, neither ADHD, depression, nor aggression predicted change in objectively-measured academic achievement from a standardized assessment.
Conclusion:
Implications for intervention and prevention are considered, including school-based approaches, within a developmental psychopathology framework.
Childhood internalizing (e.g., anxiety, depressed mood) and externalizing (e.g., aggression, delinquency) problems are highly prevalent and clinically significant. Nationally, 20 to 25% of youth meet diagnostic criteria for an impairing mental disorder across their lifetime (Merikangas et al., 2010) and psychopathology collectively incurs $16.3 billion in loss of economic productivity (Trautmann et al., 2016). Dimensions of psychopathology reliably predict negative outcomes spanning lower life expectancy and economic hardships (e.g., disability, unemployment) to higher physical and mental health challenges (Narusyte et al., 2017). Given that schools are a primary setting where youth socio-emotional and academic development unfolds, it is unsurprising that diverse indicators of academic functioning (e.g., school failure, school disengagement) are similarly sensitive to dimensions of psychopathology (Olivier et al., 2020). To accelerate innovations in the development of new interventions and to guide decisions about the allocation of mental health resources (Bitsko et al., 2018; Trautmann et al., 2016), there is an urgent need to identify developmentally-informed risk factors for children’s academic and socio-emotional across the lifespan.
Associations of Internalizing and Externalizing Problems With Academic Functioning
Consisting of diverse problems including anxiety (e.g., worry, fear) and depressed mood (e.g., dysphoria, irritability), youth internalizing problems reliably predict diverse indicators of youth academic achievement (e.g., standardized test scores, GPA; Grover et al., 2007; Voltas et al., 2014; Weidman et al., 2015). Whereas depression symptoms are concurrently and prospectively associated with poor academic achievement (Voltas et al., 2014; Weidman et al., 2015), anxiety is less consistently associated with academic outcomes. For example, child anxiety was positively associated with overall academic achievement (Voltas et al., 2014), negatively associated with GPA and achievement test scores (Grover et al., 2007; Weidman et al., 2015), and unrelated to standardized test scores (Riglin et al., 2013). Specific facets of anxiety (e.g., threat sensitivity) may enhance alertness/motivation to complete tasks to avoid negative evaluation whereas other anxiety facets may disrupt concentration, working memory, and potentiate intrusive/negative thoughts (Voltas et al., 2014). Similarly, shared characteristics of anxiety and depression (e.g., avoidance) may reduce help-seeking behavior (e.g., attempt to clarify instructions) or entrench lack of motivation, thus disadvantaging academic performance (Grover et al., 2007) and partially explaining more consistent linkages between depression with low academic achievement (e.g., GPA, test scores; Riglin et al., 2013; Weidman et al., 2015). A major threat to strong inferences, however, is that depression and anxiety frequently co-occur with other dimensions of psychopathology, including ADHD. Given that depression is 5.5 times more likely among youth with ADHD than non-ADHD youth (Daviss, 2008), ADHD must be carefully considered. However, previous evidence employed inconsistent timescales in predictive models ranging from short-term (e.g., same academic year) to multi-year follow-up, despite the sensitivity of these problems to age and developmental influences. For example, poor academic performance secondary to youth emotional difficulties may require longer follow-up to reveal key mediating factors (e.g., disruptions in attendance, compromised engagement with learning materials; Credé et al., 2010). The current study addresses this limitation by its use of a prospective follow-up, spanning key developmental periods, to reveal putative effects.
Externalizing behavior problems (e.g., aggression, hyperactivity) are associated with poor academic outcomes that continue to decline in subsequent grade levels (e.g., low GPA, disciplinary actions; Evans et al., 2021), although co-occurring attentional problems complicate precise inferences (D. H. Arnold, 1997), which themselves predict low academic achievement. Disciplinary actions (e.g., suspension) that remove students from the classroom may delimit normative learning and social opportunities and reinforce negative behavior by removing tasks perceived to be aversive (D. H. Arnold, 1997). Broadly, the association of externalizing problems with poor academic achievement and functioning may reflect attentional deficits that frequently co-occur with aggression and conduct problems (Daley & Birchwood, 2010; Hinshaw, 1992) or lower school competence (Langberg et al., 2011). Consequently, rigorous models testing the associations of externalizing problems with academic development must separately attend to dimensions such as ADHD and aggression (Brennan et al., 2012). Given that ADHD reliably predicts multiple dimensions of academic competence (e.g., homework completion, materials management, Langberg et al., 2011), the role of co-occurring externalizing problems must be considered.
Association of Internalizing and Externalizing Problems With Social Outcomes
In addition to meeting important academic milestones, social functioning is crucial for healthy development. Relative to other aspects of social development (e.g., popularity, peer liking), friendship quality may be particularly meaningful (Barzeva et al., 2021; Waldrip et al., 2008). Defined as perceptions of the positive and negative characteristics of their interactions with friends, friendship quality meta-analytically predicted maladjustment (i.e., depression, loneliness) more robustly than the number of friends (Schwartz-Mette et al., 2020); friendship quality also uniquely predicted positive adjustment factors (i.e., lower risk for victimization), even with control of other peer and social factors (e.g., number of friends; Waldrip et al., 2008). Friendships are crucial sources of social support and help children meet socioemotional needs (e.g., sense of belonging; Barzeva et al., 2021); high quality friendships may also buffer against emotional and behavioral problems following other negative peer experiences (e.g., bullying; Deater-Deckard, 2001). Attesting to the clinical significance of friendship quality, depression predicted less support from close friends (Klima & Repetti, 2008), perhaps compromising the development or maintenance of friendships and sources of social support through excessive reassurance seeking and negative feedback seeking (Rose et al., 2011; Rudolph et al., 2007). Depression symptoms also predicted fewer reciprocal friendships, lower perceived friendship quality and perceived peer acceptance over time (Rudolph et al., 2007). Similarly, youth with ADHD exhibit similar peer and social problems such as lower social preference and fewer reciprocated friendships that continue to worsen over time (Y. Lee et al., 2021). Together, commensurate with predictions of academic development from anxiety and depression, improved traction in predictions of social development must consider that ADHD is also a key explanatory factor.
Similarly, the association of childhood anxiety with friendship quality is inconsistent: overall anxiety symptoms positively predicted friendship quality whereas social anxiety disorder predicted worse friendship quality (i.e., conflict), potentially through deficient social skills and lower social competence (Rose et al., 2011; Scharfstein & Beidel, 2015). Given the multidimensionality (e.g., worry, fear), which may differentially associate with outcomes, predictions of poor social functioning from anxiety may also reflect co-occurring externalizing problems rather than depression or anxiety alone (Becker et al., 2012). Surprisingly few studies have simultaneously considered ADHD and internalizing problems with respect to friendship quality: in one study, anxiety symptoms were positively associated with supportive friendship quality (over and above ADHD status) (Rokeach & Wiener, 2022) whereas co-occurring anxiety problems in youth with ADHD was unrelated to friendship quality (Normand et al., 2020). To our knowledge, no studies have examined depression × ADHD interactions in predictions of friendship quality. Youth with ADHD or internalizing problems fare worse than comparison youth with respect to social skills (Mikami, 2010; Scharfstein & Beidel 2015), which are central to developing and maintaining high quality friendships (Tipton et al., 2013). However, approximately one third of rejected youth have at least one friend (Mikami, 2010), making friendship quality a unique outcome to consider among populations experiencing other social difficulties, especially given that friendships buffered poor outcomes from other risk factors (Schmidt & Bagwell, 2007)
There is replicated naturalistic and experimental evidence that youth aggression is inversely associated with adaptive social functioning (Crick, 1996; Rose et al., 2004), including poor peer relationships (Poulin & Boivin, 1999). Interestingly, overt aggression is associated with some socially desirable characteristics (e.g., leadership), suggesting that friendship formation may be easier than friendship maintenance for aggressive youth. For example, aggressive children exhibited difficulty continuing or maintaining friendships, perhaps secondary to poor conflict resolution (Leary & Katz, 2005). Interestingly, relational aggression (e.g., social exclusion, gossip) was positively associated with friendship intimacy, despite their lower likability and vulnerability to conflictual relationships (Grotpeter et al., 1996). Given the frequent covariation of aggression and related disruptive behavior problems with ADHD (Becker et al., 2012), it is crucial to test their independent and interactive associations with peer relationships, particularly over time and across discrete developmental periods (e.g., childhood to adolescence). Youth with comorbid ADHD and externalizing problems exhibit worse social skills and lower social preference (Becker et al., 2012) relative to youth with ADHD or disruptive behavior (Hinshaw & Melnick, 1995). Hyperactive youth were more likely to be aggressive towards peers and show less prosocial behavior relative to comparison youth (Keown & Woodward, 2006), which could be explained through deficient emotion regulation implicated in ADHD and conduct problems (Steinberg & Drabick, 2015). Given the possible unique roles of specific externalizing behavior (e.g., aggressive, oppositional, hyperactive, impulsive) on children’s social development, models must consider plausible unique (i.e., independent) and interactive influences on friendship quality.
Internalizing and externalizing problems in youth reliably predict academic and social development, but this evidence consists disproportionately of cross-sectional designs and models that fail to disentangle their unique associations. Given that ADHD frequently co-occurs with internalizing and externalizing problems, and is itself associated with academic and socio-emotional development, rigorous predictive models should account for ADHD. To improve traction on predictive models, the current study tested childhood anxiety, depression, and aggressive behavior as predictors of change in academic functioning and friendship quality, including potential moderation by childhood ADHD, among 182 children with and without ADHD followed prospectively from childhood to adolescence. We hypothesized that each dimension of psychopathology (i.e., anxious-depressed, withdrawn-depressed, and aggressive behaviors) would inversely predict academic achievement and friendship quality with ADHD diagnostic status exacerbating (i.e., moderating) key predictions.
Method
Participants
At baseline, 5- to 11-year-old 232 participants were included (M = 7.90, SD = 1.189) diverse (47.8% Caucasian, 7.6% African American, 10.8% Hispanic, 3.2 Asian, 22.1% Mixed, 1.2% other, and 7.2% did not specify) youth (68.1% male) with (n = 121) and without (n = 110) ADHD (Table 1). Children were recruited from a large metropolitan city in the Western United States through local elementary schools, health service providers, and pediatric clinics. To be eligible, youth were required to live with at least one biological parent at least half the time, have a Full-Scale IQ of at least 70, and be fluent in English. Participants were ineligible to participate if diagnosed with a neurological, pervasive developmental, or seizure disorder. Families received a psychodiagnostic report and they were compensated $50 for their participation.
Participants.
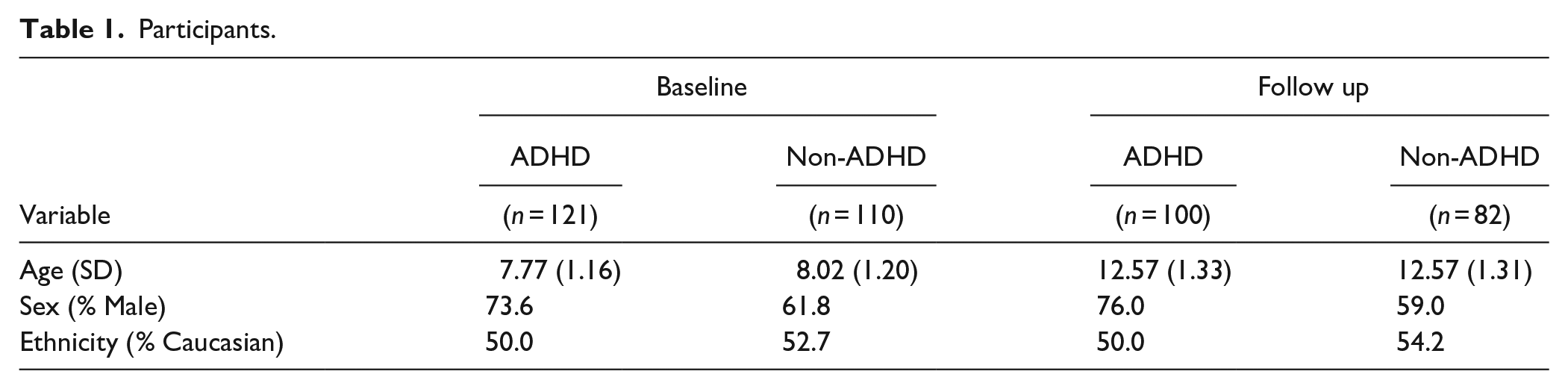
Of the original 232 baseline participants, 182 participants (78%) completed a follow-up visit approximately 5 years following their baseline visit when youth were 10 to 16 years old (M = 12.58, SD = 1.319) (see Table 1 for additional demographic information). Compared to non-participants, families who returned for the follow-up visit did not differ significantly with respect to key clinical and demographic measures at baseline. Of note, participants completed an additional follow-up visit approximately two years after the initial baseline timepoint, but those data were not used in the current study. All families who participate at baseline were invited to participate in all follow up visits, regardless of their participation in previous assessments.
Procedures
At baseline, families were initially phone screened and those eligible were invited to the laboratory to be further assessed to gather baseline data. After obtaining parent consent and youth assent, parents completed a structured diagnostic interview and rating scales of child psychopathology. Approximately 6 to 7 years after their baseline assessment, participants returned for a laboratory-based follow-up assessment (N = 182) which consisted of a standardized evaluation of academic achievement as well as a semi-structured interview with you about their friendships. Overall, assessment procedures were highly similar at baseline and follow-up with all procedures were approved by the Institutional Review Board (IRB).
Measures
Baseline Child Psychopathology
Child Behavior Checklist (CBCL)
Parents completed the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001), a 113-item parent rating scale of child psychopathology rated from 0 to 2 (0 = not true to 2 = very true or often true) at baseline and follow-up. At baseline, internalizing and externalizing behaviors were estimated using the Withdrawn/Depressed, Anxious/Depressed, and Aggressive Behavior subscales. Because the child’s age, biological sex, and race-ethnicity were adjusted for in all models, we used raw scores. All CBCL predictor variables were centered (i.e., z-scores) to aid in interpretation of interaction terms.
Covariates
Diagnostic Interview Schedule for Children, 4th edition (DISC-IV)
Youth DSM-IV ADHD diagnostic status was determined using the Diagnostic Interview Schedule for Children, fourth edition (DISC-IV; Shaffer et al., 2000), a fully structured interview conducted with participants’ parents. Participants who met diagnostic criteria for other disorders besides ADHD were placed into the non-ADHD group, as exclusion of such participants could result in an unrealistically high functioning comparison sample. The DISC-IV is considered a gold standard diagnostic measure with a rich history of strong psychometric properties.
Dishion Social Preference Scale
At baseline, parents completed the Dishion Social Preference Scale (Dishion, 1990), a three-item measure that assesses the proportion of peers who accept/like, reject/dislike, and ignore the child according to parents’ ratings on a 5-point scale (1 = “None or 0% of peers” to 5 = “Almost all or 100% of peers”). Item 1 (What proportion of his/her peers like and accept him or her?) was reversed scored and combined with Item 2 (What proportion of his/her peers dislike or reject him/her?) to create a composite negative social preference variable. As detailed further below, baseline social preference score was controlled for in models predicting adolescent friendship quality (see “Data Analytic Procedures”).
Adolescent outcomes
Academic achievement
The Wechsler Individual-Achievement Test–Second Edition WIAT-II (Wechsler, 2002) is a standardized test of academic achievement that was administered at baseline and at follow-up. Given the lack of strong theory to hypothesize that math and reading achievement outcomes would be differentially sensitive to childhood psychopathology dimensions, as well as to reduce Type I error, Math Reasoning and Word Reading scores were combined. The Math Reasoning and Word Reading scores were correlated at .68, which further justified the creation of a composite score (i.e., z-score sum of Math Reasoning and Word Reading raw scores).
Academic competence
The CBCL (Achenbach & Rescorla, 2001) School Competence subscale was administered at baseline and follow-up. This subscale was used to estimate overall academic functioning, which consisted of four items related to performance in core school subjects, repetition of grades, whether child received special education services, and academic or other problems administered at baseline and follow-up.
Friendship quality
The Friendship Quality Scale (FQS; Lansford et al., 2003) is a semi-structured interview with youth about their friendship quality (i.e., companionship, closeness, and conflict). The companionship subscale consisted of four items (e.g., “My friend and I go to each other’s houses after school and on weekends” and “Sometimes my friend and I just sit around and talk about things like school, sports, and other things we like”). The closeness subscale consisted of five items (e.g., “if my friend had to move away, I would miss him”). The conflict subscale consisted of four items (e.g., “My friend and I disagree about many things” and “I can get into fights with my friend”). All items were rated on a 3-point scale (0 = not true, 1 = somewhat or sometimes true, 2 = very or often true) with each subscale consisting of its mean.
Data Analytic Procedures
To review, we tested the independent association of Anxious/Depressed problems with respect to six to seven year change in separate academic (i.e., combined math and reading knowledge, academic competence) and social (i.e., companionship, closeness, and conflict with friends) outcomes, with inclusion of baseline childhood ADHD diagnostic status (i.e., ADHD vs non-ADHD) as well as adjusting the child’s age, biological sex, and race-ethnicity. The model was then reproduced where Anxious/Depressed problems was replaced with CBCL Withdrawn/Depressed; the third model consisted of CBCL Aggressive Behavior problems. In all cases, to improve specificity of inferences, we conservatively controlled for the child’s age, biological sex, and race-ethnicity in each model. In most cases, baseline levels of the outcome being predicted (e.g., baseline WIAT academic achievement in predictions of adolescent WIAT academic achievement) were included in predictive models. Thus, collectively, these models capitalize on temporally ordered variables – predictors preceding adolescent outcomes – such that we tested predictors of 6- to 7-year change in outcomes. However, given that friendship quality data were not collected at baseline, we employed baseline social preference as a proxy for friendship quality. Thus, social preference was controlled in in predictions of adolescent friendship quality.
Following expert recommendations for regression, all predictors were centered to avoid scaling artifacts (Kraemer & Blasey, 2004). We employed SPSS version 27 to fit hierarchical multiple regression models to discern associations of childhood anxiety, depression, and aggression with key outcomes, including their moderation by childhood ADHD diagnostic status. This strategy allowed for inferences with and without the interaction term: if the interaction term was not significant, models with main effects only were interpreted.
Results
To review, we tested the associations of childhood internalizing and externalizing problems with respect to five-year change in separate academic (i.e., combined math and reading knowledge, academic competence) and social (i.e., companionship, closeness, and conflict with friends) outcomes, adjusting for baseline ADHD diagnostic status (i.e., ADHD vs non-ADHD) and controlling for the child’s age, biological sex, and race-ethnicity. We also tested plausible baseline ADHD × externalizing and ADHD × internalizing problems interactions as predictors of change in these same academic and social outcomes.
Childhood Predictors of Change in Academic Achievement and Academic Competence
Controlling for age, sex, race-ethnicity, and baseline academic achievement, each model regressed adolescent academic achievement on to each predictor (i.e., withdrawn depressed problems, anxious depressed problems, or aggressive behavior). Neither Anxious/Depressed problems nor ADHD status predicted prospective change in academic achievement (b = 0.06, SE = 0.05, p = .26 and b = −0.04 SE = 0.10, p = .50, respectively). Similarly, the Anxious/Depressed × ADHD diagnostic status interaction was unrelated to adolescent academic achievement (b = −0.04, SE = 0.11, p = .65). In a separate model predicting the same outcome, neither Withdrawn/Depressed problems nor ADHD status significantly predicted change in academic achievement (b = 0.06, SE = 0.05, p = .25 and b = −0.03, SE = 0.10, p = .53, respectively). The baseline Withdrawn/Depressed problems × ADHD diagnostic status was similarly unrelated to change in adolescent academic achievement (b = 0.04, SE = 0.13, p = .75). A highly similar model tested predictions of change in adolescent academic achievement, but featured baseline Aggressive Behavior and ADHD status. Neither Aggressive Behavior nor ADHD status significantly predicted change in academic achievement (b = 0.08, SE = 0.05, p = .16 and b = −0.05, SE = 0.10, p = .34, respectively). The Aggressive Behavior × ADHD status was also unrelated to change in adolescent WIAT scores (b = −0.03, SE = 0.14, p = .80).
Next, with respect to predictions of academic competence, we constructed parallel models to those above wherein age, sex, and race-ethnicity were entered as covariates; with additional control of baseline academic competence. Neither Anxious/Depressed problems nor ADHD status significantly predicted change in CBCL school competence (b = 0.00, SE = 0.07, p = 1.0 and b = −0.12, SE = 0.14, p = .07, respectively). Similarly, the Anxious/Depressed × ADHD diagnostic status interaction was unrelated to change in adolescent CBCL school competence (b = −0.03 SE = 0.15, p = .83). In a similar model, Withdrawn/Depressed problems was unrelated to change in CBCL school competence (b = 0.09, SE = 0.07, p = .18). However, youth with ADHD had worsening school competence relative to non-ADHD youth (b = −0.15, SE = 0.14, p = .03). ADHD diagnostic status did not moderate predictions of change in academic competence from baseline Withdrawn/Depressed behavior (b = −0.15, SE = 0.17, p = .30). Finally, a highly similar model tested predictions of change in school competence, but featured baseline Aggressive Behavior and ADHD status. Baseline Aggressive Behavior remained unrelated to prospective change in CBCL school competence (b = 0.08, SE = 0.07, p = .26) whereas youth with ADHD had worsening school competence relative to youth without ADHD (b = −0.16 SE = 0.15, p = .03, respectively). The Aggressive Behavior × ADHD status was unrelated to change in adolescent CBCL school competence (b = −0.19, SE = 0.20, p = .22).
Childhood Predictors of Adolescent Friendship Quality
Next, similar models consisted of separately regressing adolescent companionship, closeness, and conflict on to separate baseline Anxious/Depressed, Withdrawn/Depressed, and Aggressive Behavior predictors. Each model consisted of a single predictor of an adolescent peer outcome (e.g., closeness), controlling for age, sex, race-ethnicity, and baseline peer status (e.g., closeness). First, neither Anxious/Depressed symptoms nor ADHD status significantly predicted change in adolescent companionship (b = −0.13, SE = 0.03, p = .12 and b = −0.09, SE = 0.07, p = .36, respectively). The baseline Anxious/Depressed problems × ADHD diagnostic status also did not predict change in adolescent companionship (b = 0.03, SE = 0.07, p = .84). Second, neither main effect for Anxious/Depressed problems nor ADHD diagnostic status was significantly predictive of change in adolescent closeness (b = 0.00, SE = 0.03, p = .98 and b = −0.10, SE = 0.06, p = .29, respectively). Similarly, the baseline Anxious/Depressed problems × ADHD diagnostic status was unrelated to change in adolescent closeness (b = 0.06, SE = 0.06, p = .69). Next, neither Anxious/Depressed problems nor ADHD status significantly predicted change in conflict (b = −0.03, SE = 0.03, p = .75 and b = 0.08, SE = 0.08, p = .43, respectively). The baseline Anxious/Depressed problems × ADHD diagnostic status interaction also did not significantly predict change in adolescent conflict (b = −0.15, SE = 0.08, p = .33).
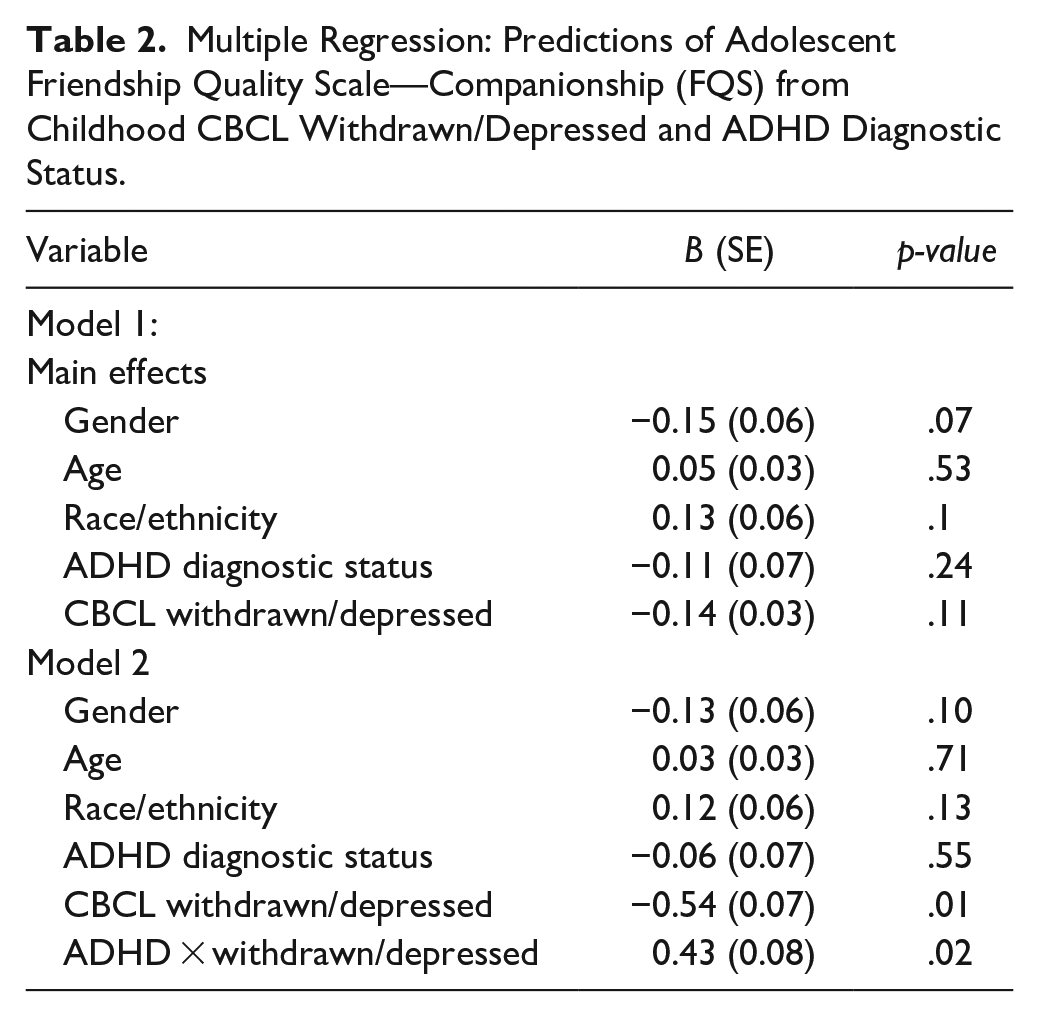
The second set of models tested predictions of relative change in adolescent friendship quality from baseline Withdrawn/Depressed problems. Neither Withdrawn/Depressed problems nor ADHD status significantly predicted change in companionship (b = −0.14, SE = 0.03, p = .11 and b = −0.12, SE = 0.07, p = .24, respectively). However, the baseline Withdrawn/Depressed problems × ADHD status significantly predicted change in adolescent companionship (b = 0.43, SE = 0.08, p = .02) (see Table 2). To explore the interaction, we tested the association of Withdrawn/Depressed problems with adolescent companionship separately among youth with versus without ADHD. Among youth without ADHD, baseline Withdrawn/Depressed problems predicted worsening companionship (b = −0.54, SE = 0.07, p < .01); among youth with ADHD, however, Withdrawn/Depressed problems were unrelated to change in adolescent companionship (b = −0.04, SE = 0.04, p = .65), further depicted in Figure 1. Next, in a highly similar model, neither Withdrawn/Depressed problems nor ADHD status significantly predicted change in closeness (b = 0.05, SE = 0.03, p = .55 and b = −0.10, SE = 0.06, p = .23, respectively). The baseline Withdrawn/Depressed problems × ADHD diagnostic status predicted change in adolescent closeness (b = 0.35, SE = 0.07, p = .047). However, baseline Withdrawn/Depressed problems did not significantly predict adolescent closeness separately among youth with and without ADHD (b = 0.13, SE = 0.03, p = .16 and b = −0.28, SE = 0.06, p = .13, respectively) (see Figure 2). This pattern suggests that the simple slopes differed significantly between youth with and without ADHD, but neither slope differed from zero. In a separate model, neither Withdrawn/Depressed symptoms nor ADHD status predicted change in adolescent peer conflict (b = 0.10, SE = 0.04, p = .24 and b = 0.05, SE = 0.07, p = .59, respectively). Additionally, baseline Withdrawn/Depressed problems × ADHD status did not significantly predict change in adolescent peer conflict (b = 0.12, SE = 0.09, p = .52).
Multiple Regression: Predictions of Adolescent Friendship Quality Scale—Companionship (FQS) from Childhood CBCL Withdrawn/Depressed and ADHD Diagnostic Status.
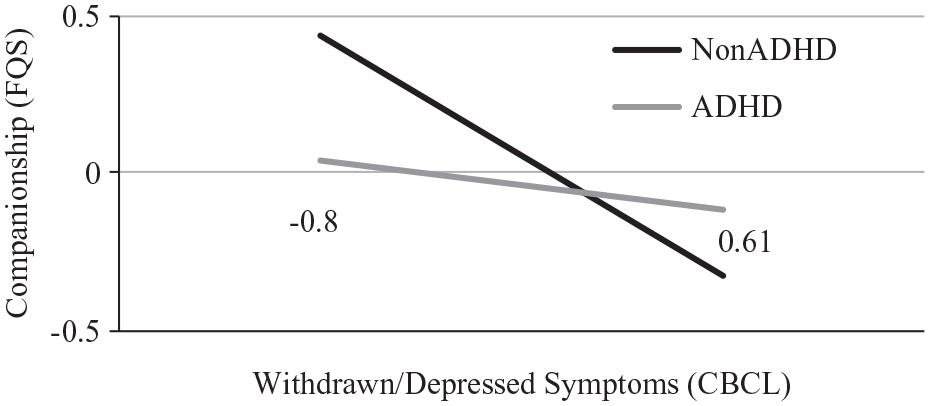
Predictions of adolescent friendship quality (FQS) companionship from childhood CBCL withdrawn/depressed problems: Moderation by ADHD diagnostic status.
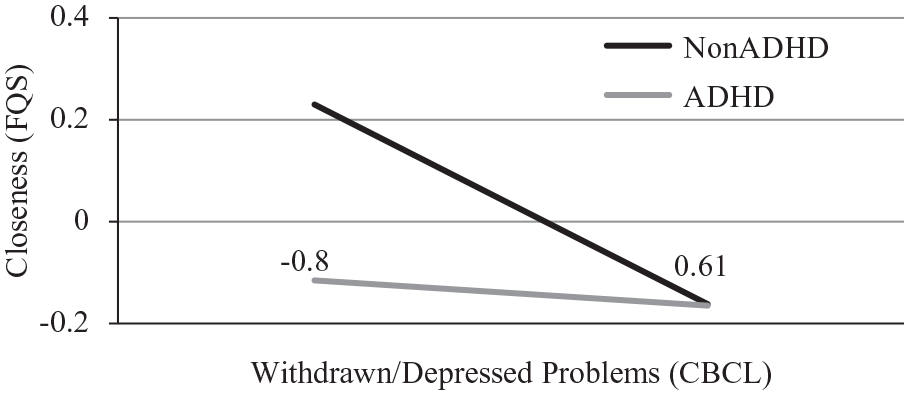
Predictions of adolescent friendship quality (FQS) closeness from childhood CBCL withdrawn/depressed problems: Moderation by ADHD diagnostic status.
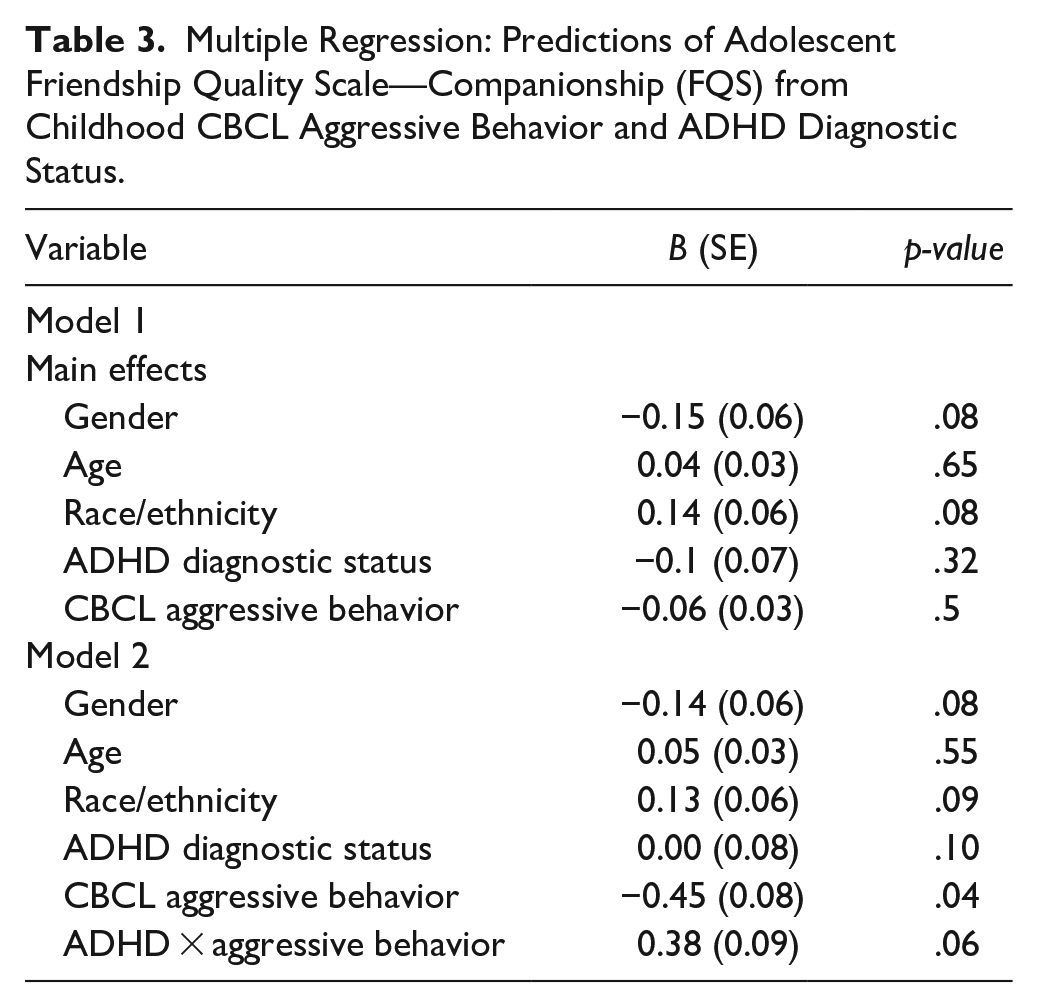
The third set of models tested predictions of adolescent friendship quality from Aggressive Behavior. Neither Aggressive Behavior nor ADHD status significantly predicted change in companionship (b = −0.06, SE = 0.03, p = .50 and b = −0.10, SE = 0.07, p = .32, respectively). However, the baseline Aggressive Behavior × ADHD diagnostic status interaction marginally predicted change in adolescent companionship (b = 0.38, SE = 0.09, p = .06), as shown in table 3, such that among non-ADHD youth, Aggressive Behavior predicted worsening companionship (b = −0.45, SE = 0.08, p = .04) whereas Aggressive Behavior did not predict change in companionship among with ADHD (b = 0.02, SE = 0.04, p = .84). In a highly similar model, the baseline Aggressive Behavior × ADHD diagnostic status did not significantly predict change in adolescent closeness (b = 0.04, SE = 0.08, p = .81). Finally, neither Aggressive Behavior nor ADHD diagnostic status significantly predicted change in adolescent conflict (b = −0.01, SE = 0.04, p = .93 and b = 0.07, SE = 0.08, p = .49, respectively). Similarly, the Aggressive Behavior × ADHD diagnostic status interaction did not predict change in conflict (b = 0.16, SE = 0.10, p = .42).
Multiple Regression: Predictions of Adolescent Friendship Quality Scale—Companionship (FQS) from Childhood CBCL Aggressive Behavior and ADHD Diagnostic Status.
Discussion
Although youth externalizing and internalizing problems (e.g., anxiety, depression) predict poor outcomes, these associations may reflect co-occurring ADHD, including potential interactive influences. We leveraged a large (N = 182) and ethnically diverse (47.8% non-White) sample of school-age children with and without ADHD followed prospectively for five to six years into early adolescence to address the following aims: to separately test childhood internalizing and externalizing problems as predictors of five to six year change in academic functioning and friendship quality, including their potential moderation by baseline ADHD diagnostic status. Several key findings emerged: (1) early withdrawn/depressed problems and aggressive behavior each predicted worsening peer companionship, but this was specific to non-ADHD youth; (2) anxious/depressed problems were unrelated to change in adolescent friendship quality; (3) relative to non-ADHD youth, youth with ADHD exhibited worsening school competence in adolescence; and (4) contrary to expectations, neither anxious/depressed, withdrawn/depressed, nor aggressive behavior problems predicted six to seven year change in academic functioning from childhood to adolescence.
Predictions of Friendship Quality From Internalizing and Externalizing Problems
Contrary to hypotheses, early depression predicted worsening adolescent companionship specifically in non-ADHD youth, which may reflect deficient self-perceptions in ADHD. ADHD is associated with positive illusory bias, a deficit characterized by a discrepancy between self-reported competence and actual competence (Owens et al., 2007). For example, peers of youth with ADHD reported more conflict and fewer positive relationship qualities than friends of non-ADHD youth, but youth with ADHD did not report peer and friendship difficulties (Normand et al., 2013). Also, early depression predicted negative expectations with respect to social interactions as well as broader negative self-biases (Rudolph et al., 2007). Given that ADHD predicts poor social adjustment (Blachman & Hinshaw, 2002), withdrawn and depressed behaviors may not predict prospective change in social functioning relative to the primacy of ADHD and replicated correlates of social functioning (e.g., social skills deficits); thus, withdrawn and depressed behaviors may not constitute frontline intervention targets (Gardner & Gerdes, 2015).
Despite poor social functioning constituting a cardinal feature of youth with ADHD, especially with co-occurring disruptive behavior problems, aggressive behavior predicted worsening adolescent peer companionship specifically among non-ADHD youth. Youth with ADHD are more likely to befriend high-risk peers by virtue of ADHD, behavior problems, or other socially marginalized youth (Marton et al., 2015; Mikami, 2010). Dyadic relationships embedded in multiple behavior problems may alter perceptions around normative social interactions and peer relationship factors. Aggressive and other disruptive behaviors may be particularly atypical within friendships between children without ADHD, potentially making these behaviors especially detrimental for non-ADHD youth. Relatedly, youth with and without ADHD may exhibit different types of aggressive behaviors that differentially affect peer relationship factors, including companionship. For example, ADHD symptoms are meta-analytically associated with reactive aggression, but not proactive aggression (Card & Little, 2006); there is evidence that proactive aggression is more harmful to friendships relative to reactive aggression, including predicting more dissatisfaction and conflict (Poulin & Boivin, 1999). While youth with ADHD are at risk for multiple negative social outcomes extending into adulthood (Barkley et al., 2006; Poulin & Boivin, 1999), aggressive behavior (particularly if reactive in nature) may not significantly increment predictions of poor friendship quality beyond ADHD itself. For example, baseline observed overt aggression did not predict lower social preference in adolescence among youth with ADHD (S. S. Lee & Hinshaw, 2006). We conclude by cautioning inferences about better-than-expected peer functioning secondary to early ADHD given the potential for iatrogenic effects of associating with peers at risk for externalizing problems (Grotpeter et al., 1996).
While we hypothesized that childhood anxious and depressed problems would predict worsening trajectories of academic functioning and friendship quality, they were in fact unrelated to prospective change in academic functioning or friendship quality with inclusion of baseline academic functioning and ADHD diagnostic status. This approach was particularly conservative, but defensible given the frequent co-occurrence of ADHD and the need to strengthen temporally-ordered inferences that anxious/depressed problems are a risk factor for poor academic achievement (rather than simply being a correlate; see Kraemer et al., 2001). Another contributing factor to these associations may be heterogeneity within anxiety. Whereas depression has been consistently associated with negative peer and academic outcomes (e.g., low social support, low GPA; Klima & Repetti, 2008; Weidman et al., 2015), predictions from anxiety are inconsistent (Voltas et al., 2014). For example, there is longstanding theoretical and empirical work suggesting that anxiety consists of separable fear- vs. worry-based dimensions (Sylvers et al., 2011), including divergent patterns of association (e.g., treatment response). Previous evidence inconsistently implicating anxiety as a risk factor for poor academic and social outcomes may inadvertently reflect these separable dimensions. For example, worry-based anxiety dimensions (e.g., generalized anxiety) positively predicted social (e.g., number of friends, friendship quality; Rose et al., 2011) and academic outcomes (e.g., GPA; Sarason, 1957), whereas fear-based anxiety dimensions (e.g., social phobia) negatively predicted social (e.g., friendship quality (Rodebaugh, 2009), and academic outcomes (e.g., lower grades); Baptista et al., 2012). We strongly suggest that specific internalizing dimensions, including anxious avoidance versus withdrawn behaviors, may improve specificity with respect to predictions of individual differences in social and academic functioning.
Predictions of Academic Functioning From Internalizing and Externalizing Problems in Children With and Without ADHD
Consistent with replicated evidence that ADHD is a risk factor for poor academic outcomes (Langberg et al., 2011; Loe & Feldman, 2007), these preliminary data suggested that childhood ADHD predicted declining school derived from a standardized assessment instrument in adolescence was not sensitive to early ADHD. Although related, school competence is a broader construct consisting of academic knowledge as well as key academic readiness skills such as appropriate peer interactions, attention to teachers’ instructions, and adherence to classroom norms. Given that ADHD diversely compromises multiple academic readiness skills relevant to classroom functioning (e.g., trouble focusing on teachers, interrupting or appearing not to listen during interactions with peers and authority figures, difficulty working independently; Daley & Birchwood, 2010), broader measures of academic functioning are likely more sensitive to ADHD and related risk processes. Additionally, a previous meta-analysis revealed that whereas childhood ADHD is broadly associated with substandard academic functioning (e.g., achievement testing, parent or teacher ratings, GPA, repeating a grade), effect sizes varied according to the type of measure employed (e.g., subject of the achievement test, respondent on rating form; Frazier et al., 2007). In the present study, youth school competence was estimated from parent report across indicators such as academic performance in several subjects, receipt of special services, repetition of a grade, and other school problems. Consistent with our formulation here, ADHD diagnostic status predicted larger effects in school competence relative to academic achievement (results available upon request), further underscoring the separability of academic achievement (derived from standardized assessments) from school competence (McConaughy et al., 2011).
As predictors and with potential moderation by ADHD diagnostic status, neither children’s anxious/depressed, withdrawn/depressed, nor aggressive behavior problems significantly predicted change in children’s academic functioning. Although contrary to hypotheses, these models specifically tested prospective change, across five to six years, in key constructs (i.e., controlling for baseline level of the adolescent outcome being predicted). Furthermore, measures of academic achievement (e.g., test scores) are generally stable throughout childhood and adolescence (Rimfeld et al., 2018), including considerable rank-order stability. In the current study, we observed a similar pattern given that baseline achievement was the only significant predictor of adolescent achievement; similarly, baseline school competence was one of the only significant predictors of adolescent school competence. While evidence on how comorbid symptoms relate to academic functioning among ADHD youth is underdeveloped (L. E. Arnold et al., 2020; Loe & Feldman, 2007), preliminary cross-sectional evidence suggested that co-occurring internalizing (Blackman et al., 2005) or externalizing (Cuffe et al., 2020) problems did not increment predictions of poor academic outcomes beyond the risk of ADHD alone. However, when defined more particularly in ways that increase the severity of clinical presentation for ADHD (i.e., accompanied by three or more comorbid conditions), co-occurring problems may increment predictions (beyond ADHD) of academic functioning (Larson et al., 2011). Results from the current study underscore the potency of childhood ADHD as a unique risk factor on academic functioning across development separable from co-occurring internalizing or externalizing problems.
Limitations and Future Directions
This study included several important limitations. First, although key constructs were assessed using multiple methods (e.g., structured interviews, normed rating scales, and standardized tests), additional reports from teachers, peers, and children themselves may have improved traction on predictive models. For example, given that much of children’s interactions with peers happen at school, teacher reports of children’s social functioning may provide additional perspectives on social development and peer functioning. Furthermore, because they interact with a large body of children to which they can compare a child’s behavior, social functioning, and academics to, their reports may be less biased than that of parents (Webster-Stratton & Lindsay, 1999). Indeed, parents’ perceptions may be biased by their own characteristics and experiences (e.g., psychopathology, parenting stress; Najman et al., 2000). Second, this study used broad measures of emotional and behavioral problems rather than specific dimensions that may reveal more specific patterns of association. Anxiety consists of separable dimensions (e.g., fear vs. worry) that show divergently predict functional outcomes (Voltas et al., 2014). Finally, academic assessments were based solely on a standardized achievement test and parent reports of competence at school. Although change in school competence, from childhood to adolescence, was sensitive to early ADHD, this scale includes the receipt of special education services. Given that early ADHD problems are associated with educational accommodations and services (Barkley et al., 2006), associations may be artificially inflated. Future research should evaluate more diverse measures of school competence that perhaps are not as correlated with ADHD. Additionally, achievement tests are a specific indicator of academic knowledge and functioning, and, as previously noted, parent reports are susceptible to bias. Additional academic indicators, spanning GPA, attendance, and homework completion may provide a more complete understanding of individual differences in academic functioning.
The present study provided key evidence on predictions of adolescent academic and social outcomes from separable dimensions of childhood psychopathology. We contend that future research must continue to employ diverse, developmentally-sensitive designs that adequately attend to risk processes underlying psychopathology and its predictions of future functional outcomes. Replicated risk factors and the key explanatory processes underlying outcomes (including resilience) constitute important targets for intervention and prevention with respect to academic and social milestones across development. Given schools are a key source of academic and socio-emotional development, mental health screening and increased prevention and intervention efforts in school are critical to enhance youth outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.