
Abstract
Objective:
The aim of research is to provide greater understanding of ADHD in adult females by exploring first-hand experiences of female university students with ADHD in the UK, and the impact of such experiences on social, academic, and psychological functioning.
Methods:
Semi-structured interviews were conducted with eight adult women attending university in the UK—all clinically diagnosed with ADHD during adulthood.
Results:
Participants experiences were rich and insightful, identifying that many women with ADHD experience stigmatization and social discrimination, amongst other social, academic, and psychological difficulties.
Conclusion:
Overall, the research identifies the pressing need for greater understanding and appreciation of ADHD in females, particularly amongst health professionals.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity which interferes with daily functioning (American Psychiatric Association, 2013). There are three subtypes of ADHD; predominantly inattentive, predominantly hyperactive-impulsive, and combined, which are defined by the presentation and combination of symptoms (American Psychiatric Association, 2013). In most cases, the aetiology of ADHD is an accumulation of genetic and environmental risk factors (Faraone et al., 2021). ADHD is widely recognized as a childhood disorder that is most frequently diagnosed in boys, with estimates of the male to female sex ratio in childhood and adolescence (10–18-years old) ranging from 2:1 to 10:1, depending on a community or clinically based sample (Mowlem et al., 2019). Though it is commonly perceived as a childhood disorder, research efforts have explored the persistence of ADHD into adulthood (Waite, 2010). In adulthood (over 18 years of age), prevalence of ADHD diagnosis appears to be comparable between sexes, and, although symptom onset typically occurs in childhood, a significantly greater proportion of women receive a diagnosis in adulthood (Holthe & Langvik, 2017; Quinn & Madhoo, 2014). This has led to recent reports of a lack of ADHD diagnoses in females during childhood and adolescence (Quinn & Madhoo, 2014).
A potential explanation for underdiagnosed ADHD in females is differences in core symptomatic presentation between males and females. Research suggests that females are more disposed to internalized symptoms, such as inattentiveness and disorganization, and present with fewer symptoms of hyperactivity and other disruptive external behaviours (Quinn & Madhoo, 2014). On the other hand, males with ADHD are prone to more externalized hyperactive-impulsive symptoms, such as motor hyperactivity, rule-breaking and overt aggression, which results in greater likelihood of being identified and referred for clinical assessment (Abikoff et al., 2002; Young et al., 2020). As an internalized symptom profile is less likely to be disruptive in an educational setting, females are less likely to be identified and referred for clinical evaluation or treatment of ADHD. Furthermore, internalized symptoms, such as inattentiveness, are harder for the individual and others around them to identify. Symptoms such as “daydreaming,” emotional reactivity, or hyper-talkativeness may appear stereotypical of young females with the individual accepting these traits as their personality. These symptoms may also be interpreted by others as emotional or learning difficulties, instead of five symptoms of ADHD (Lynch & Davison, 2022).
Within the UK, clinical research surrounding ADHD lays focus to males, and, as a result, current diagnostic criteria and general understanding of ADHD is biased towards a male presentation of the disorder (Holthe & Langvik, 2017) with ADHD in females often being overlooked. Lynch and Davison (2022) identified that the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-V), used by clinicians to diagnose ADHD, contains a gendered bias that does not appreciate the subtle differences in the way females experience ADHD. The DSM-V lacks guidance on gender differences in ADHD, thus likely hindering the diagnosis of ADHD in females (Waite, 2010). In general, females with ADHD present with fewer of the symptoms outlined in the DSM-V compared to males, but are equally as impaired by their symptoms, though it may not be as visible (Quinn & Madhoo, 2014). In a consensus statement of ADHD in females, Young et al. (2020) emphasized the importance of moving away from preconceptions of ADHD as a disruptive behavioural disorder, and instead focusing on internalized presentations of the disorder, which are more common in girls and women.
The presence of co-morbidities in females also appears to cloud ADHD diagnosis. The overall prevalence of a comorbid psychiatric disorder for those with ADHD ranges from 40% to 80% (Shi et al., 2021). The most common psychiatric disorders that co-occur with ADHD include depression, anxiety disorders, substance use disorders, bipolar disorder, and personality disorders (Katzman et al., 2017). Specifically, females with ADHD are at a much greater risk of psychiatric comorbidities in comparison to males with ADHD and non-ADHD females (Solberg et al., 2018). Co-existing internalized symptoms of depression and/or anxiety have the potential to overshadow ADHD symptoms, resulting in missed diagnoses and therefore inappropriate treatment (Quinn, 2008). It is unclear whether psychiatric comorbidities, such as anxiety and depression, occur independent of ADHD or develop due to undiagnosed and untreated ADHD. Yet, these comorbidities have the potential to complicate identification and treatment of the disorder. Furthermore, in comparison to males, females with ADHD are more likely to develop effective masking strategies which hide the impact of their ADHD symptoms, resulting in problems being underestimated and their needs less likely to be met (Quinn & Madhoo, 2014).
Overall, ADHD is associated with significant likelihood of developing psychological, social, and emotional difficulties, which can be amplified when left undiagnosed and untreated. In general, ADHD is significantly associated with poor academic functioning across the lifespan, from school readiness to going to university (Daley & Birchwood, 2010). Problems at school are often the primary reason for a child’s clinical referral for diagnosis of ADHD, attributed to hyperactivity, inattentiveness, organizational difficulties, and lack of motivation (Arnold et al., 2020; Sedgwick, 2018). Poor educational outcomes can be a key predictor of long-term functional impairments, including anti-social behaviour, obesity, and social function outcomes, amongst others (M. Shaw et al., 2012). Among university students, poor academic attainment has shown to have a negative impact on students’ mental health and wellbeing (Sedgwick-Müller et al., 2022). There is evidence to suggest that females with ADHD do not present with academic difficulties until they reach higher education (Quinn, 2005). Quinn (2005) identified that girls with ADHD may work harder at school to mask their symptoms and meet parent/teacher expectations. However, in higher educational settings, such as university, it becomes increasingly difficult to cope with the struggles of ADHD amongst other lifestyle changes, such as moving away from home and taking on greater personal responsibilities (Quinn, 2005).
The potential absence of academic difficulties at school age may present greater challenges in recognizing ADHD in young females, providing further explanation for why many females do not receive a diagnosis of ADHD during their childhood. Individuals with ADHD commonly experience impaired social behaviours and interpersonal relationships (Sedgwick, 2018). University students with ADHD often face challenges making and maintaining academic and social relationships, and may struggle with participating in group work, team activities, and societies at university (Sedgwick-Müller et al., 2022). Impaired social functioning has a negative impact on self-esteem (Quinn & Madhoo, 2014). It is widely documented in the literature that girls and women with ADHD are more likely to experience low self-esteem in comparison to males with ADHD and non-ADHD females (Quinn & Madhoo, 2014). Rucklidge and Kaplan (1997) concluded that women who do not receive a diagnosis of ADHD until adulthood are at greater risk of suffering with low self-esteem. Low self-esteem predicts negative real-world consequences, such as unemployment, low socioeconomic status, and poor mental and 7 physical health (Trzesniewski et al., 2006). In a qualitative study exploring adult females’ experiences with ADHD, Holthe and Langvik (2017) identified that females with ADHD are more likely to experience psychological distress in comparison to males and non-ADHD females, due the profound social and personal impact of the disorder. Together, this highlights the severity of the impairments experienced by females with ADHD, exacerbated by a missed or late diagnosis of the disorder.
Overall, the literature highlights that there is insufficient understanding of ADHD in females, resulting in many females not being diagnosed with ADHD until they reach adulthood, and suffering with many of the consequences of a late diagnosis. Further research studies of females with ADHD are needed to improve understanding of the disorder and draw attention to the subtle differences in symptom presentation between males and females. Lynch and Davison (2022) highlighted that there is a lack of qualitative research exploring female experiences of ADHD from those directly affected by the condition. Sedgwick-Müller et al. (2022) also underlined that there is a deficit in research exploring the impact of ADHD on university students.
The aim of this qualitative research is to approach these gaps in the literature by exploring the personal experiences of adult, female university students with ADHD in the UK, and the impact of such experiences on their social, academic, and psychological functioning. This is an exploratory piece of research; therefore, the research does not address any specific research questions or hypotheses.
Methodology
Research Design
A qualitative approach was use, utilizing semi-structured interviews to gain an in-depth understanding of the personal experiences of adult female students with a clinical diagnosis of ADHD attending university in the UK. Semi-structured, in-depth interviews were identified as the optimal method for collecting qualitative data about participants’ experiences of ADHD (Creswell, 2007; Hammarberg et al., 2016). The General Health Questionnaire-28 (GHQ-28; Goldberg & Hillier, 1979), a self-report instrument widely used in assessing mental symptoms and psychological wellbeing, was implemented alongside the semi-structured interviews (Hjelle et al., 2019). The GHQ-28 was implemented to gain additional quantitative information about participant’s psychological wellbeing, and to explore potentially significant confounding variables, such as symptoms of depression and anxiety, which might have affected the experiences being explored.
Participant Recruitment
A purposeful sampling method was used, recruiting participants based on a set of pre-determined criteria. The inclusion criteria comprised of being an adult female (18-years +), a student at any university within the UK with a clinical diagnosis of ADHD—no formal confirmation of participant’s diagnosis of ADHD was required. Exclusion criteria included participants who had a co-morbid diagnoses of another serious mental health disorder, such as a depressive disorder or a personality disorder. These exclusion criteria were selected as acknowledgement that diagnosis of another serious mental health disorder may present greater influence on the experiences being investigated in comparison to ADHD autonomously.
Participants were recruited via advertisements in several UK-based ADHD support groups for women on Facebook and Instagram. Twenty-five women registered their interest in taking part in the study, eight of which fully completed the consent forms, GHQ-9 questionnaire and attended their allocated interview time. Thirteen individuals did not provide full consent, three individuals did not return the questionnaire and one participant did not attend their interview. Eight interviews were conducted with intention of further interviews if data did not reach saturation. Following analysis of the data, it was agreed between the researchers that no further theoretical insights or themes would emerge from further interviews and that data had reached saturation (Charmaz, 2006).
The eight participants were adult women, aged between 22 and 53 years old (mean age of 31 years old). All participants were formally diagnosed with ADHD in adulthood, and either part-time or full-time students at a university in the UK. Further participant demographics, such as ethnicity or sexual orientation, were not collected, as this information was not relevant to the outcomes of the research.
Procedure
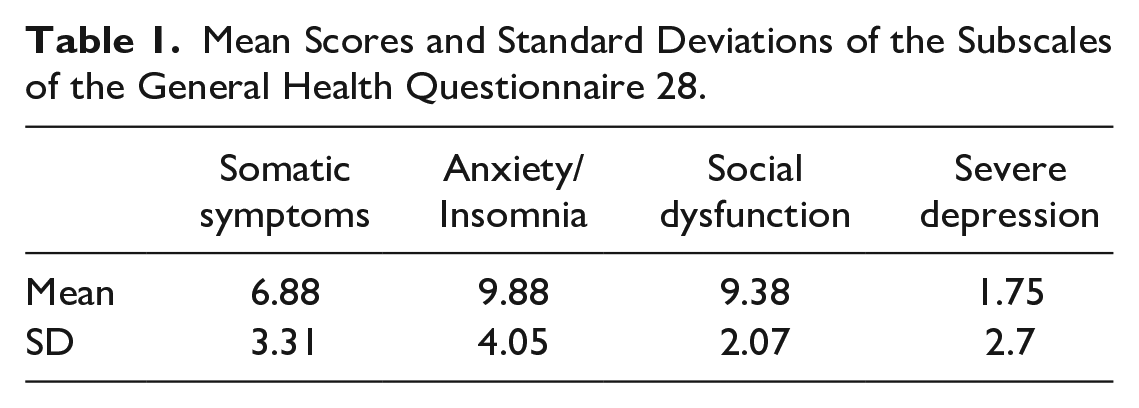
Following obtainment of informed consent, participants were asked to complete the GHQ 28, which consisted of 28 short questions asking participants how their general health had been over the weeks prior to the study (Goldberg & Hillier, 1979). Participants responded to the questions based on four criteria: better than usual, same as usual, worse than usual, and much worse than usual. Goldberg and Hillier (1979) outlined four subscales of the GHQ-28 using factor analysis: somatic symptoms, anxiety/insomnia, social dysfunction, and severe depression. Each subscale contained seven questions. The validity and stability of this factor structure has been confirmed across several different contexts (Hjelle et al., 2019). Semi-structured interviews were conducted and recorded online via Microsoft Teams, a web-based video platform. All interviews were performed by AT. The interviews ranged in duration from 21 to 32 min, with a mean duration of 26 min.
Topics of discussion included: reasons for seeking a diagnosis, personal feelings after receiving a diagnosis, and the impact of ADHD on participants’ social, academic, and psychological functioning. Questions asked within the interviews were developed and agreed among the researchers to ensure the primary research question was approached and allow an easier triangulation process. A full outline of the interview questions used can be found in Appendix A. Participants were encouraged to elaborate on topics which they found relevant. Following completion of the study, participants received a £5 Amazon e-voucher as reasonable compensation for their time.
Data Analysis
Participants were scored on their responses to the GHQ-28 using a Likert scale scoring system of 0 to 3 (0 = better than usual, 1 = same as usual, 2 = worse than usual, 3 = much worse than usual). Mean scores and standard deviations were calculated for each of the four subscales of the GHQ-28. The lowest possible total subscale score is 0 and the highest subscale score is 21. Lower scores indicated lower levels of psychological distress, and higher scores indicated higher levels of psychological distress amongst participants. All interviews were transcribed and analysed by one author and checked by the other. A full transcript of the interviews can be found in Appendix B. Content of the interviews was analysed in accordance with thematic analysis, chosen as an accessible and flexible method for identifying and interpreting themes and patterns of meaning within qualitative data (Braun & Clarke, 2006; Clarke & Braun, 2017). The six steps of thematic analysis include familiarizing yourself with the data, generating initial codes, searching for themes, reviewing themes, defining, and naming themes, and producing the report (Braun & Clarke, 2006). An inductive approach was used to analyse the data and generate codes and themes.
Data Triangulation
Both authors independently analysed the raw data and developed initial codes and themes. These codes and themes were then compared between the researchers referring to the raw data to ensure validity. Any discrepancies of themes and codes developed were discussed with agreement that a third researcher would be involved if an agreement could not be made. There were no discrepancies between the codes and themes made.
Ethical Considerations
Ethical Approval was obtained from the University of Nottingham Research Ethics Committee (Ref: S1439R). The ethical considerations reviewed for this study centred around confidentiality, and implications of the discussion of personal memories surrounding a problem which had received clinical psychological attention. Informed 10 consent was required from all research participants. Participants were informed that the researcher was not a clinical professional, therefore could not provide any form of diagnosis or psychological care. At the end of the online interviews, participants were fully debriefed and provided links to professional support services, both within the University of Nottingham and outside the University of Nottingham, should participants have felt affected by the nature of the interview and/or discussion of sensitive topics. To maintain confidentiality, all identifiable information was removed from the data following transcription and names were replaced with pseudonyms.
Results
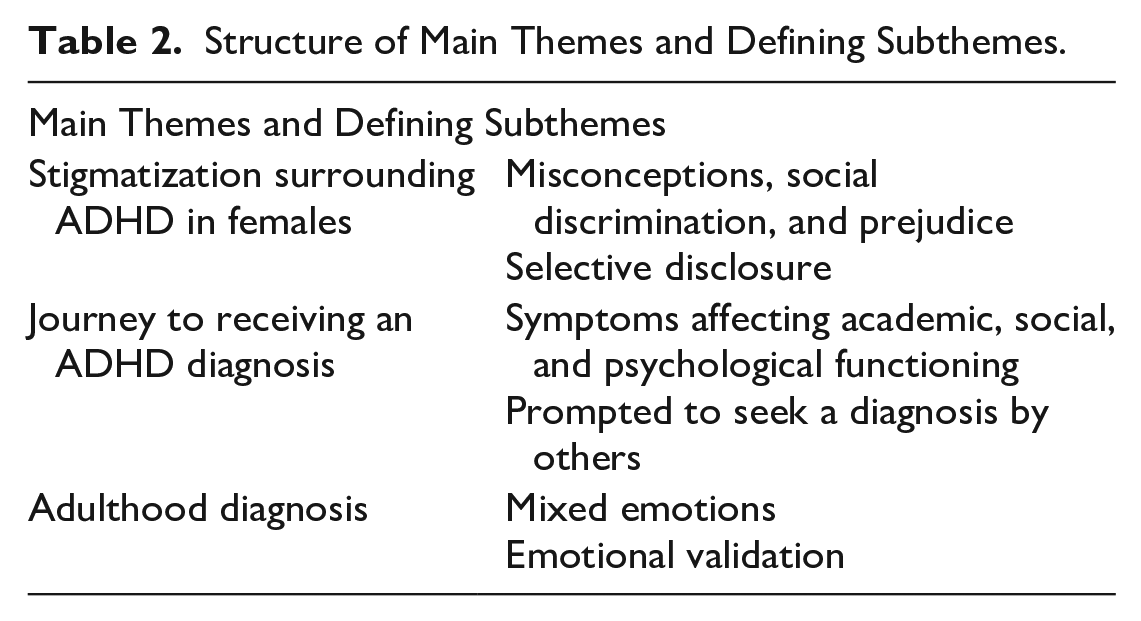
Mean scores and standard deviations (SD) for each of the subscales of the General Health Questionnaire-28 (GHQ-28) are outlined in Table 1. Participants scored higher in domains of anxiety/insomnia, and social dysfunction, compared to the other subscales, arguably due to the nature of ADHD and comorbid conditions. However, overall, the scores do not indicate high levels of psychological distress amongst participants. Therefore, it is unlikely that the subscales of the GHQ-28 would have acted as significant confounding factors in the experiences being investigated. Thematic analysis of the raw data identified three core themes and six sub-themes. Derived from the coding framework, the themes and sub-themes provide insight into participants’ experiences of ADHD as a female university student in the UK. The three core themes, which guide the order of presentation of the findings, include “stigmatization 11 surrounding ADHD in females,” “journey to receiving an ADHD diagnosis” and “adulthood diagnosis.” The structure of the core themes and defining subthemes are described in Table 2.
Mean Scores and Standard Deviations of the Subscales of the General Health Questionnaire 28.
Structure of Main Themes and Defining Subthemes.
Theme 1—Stigmatization Surrounding ADHD in Females
Misconceptions, Social Discrimination, and Prejudice
Female adults suffering with ADHD are at a high risk of being confronted with stigmatization due to the lack of disorder-related understanding and male stereotypes surrounding ADHD, amongst other factors (Mueller et al., 2012). Topics of stigma, public misconception, prejudice, and discrimination recurred throughout participants’ experiences. Most participants commented on the general lack of understanding and public awareness of ADHD, particularly surrounding the differences between ADHD in males and females. Participants acknowledged that ADHD is often perceived as a disorder that affects hyperactive teenage boys. One participant experienced prejudice during their assessment for ADHD as their symptoms did not align with the male stereotype of the disorder.
“I felt like I wasn’t taken seriously during my assessment. . .because I arrived really early, which the person assessing me kept bringing up, like, well you arrived on time so obviously that’s not a problem for you. And they were making comments like I wasn’t fidgeting enough, at least in their eyes. And those kind of comments knocked my confidence and I felt like I wasn’t being believed”
Similarly, one participant was told that she was depressed during her initial ADHD assessment as she was overwhelmed and visibly emotional. The participant knew that she was not depressed, and so felt that her feelings and experiences were being dismissed by the GP. Young et al. (2020) highlighted that it is not uncommon for adults with ADHD to be treated for depression in the first instance, as affective symptoms, such as emotional dysregulation, are often misattributed to depressive disorders. One participant reported experiencing discrimination at work, which had a serious impact on her mental health and resulted in leaving her job.
“People [at work] were making comments and I was getting into trouble for things that I now realise were symptoms [of ADHD] . . .and I felt like it was really unfair, and it was messing with my head a little bit”
Furthermore, several participants also described experiencing negative attitudes towards ADHD, from family members and academic staff. Participants expressed shock over the stigma surrounding ADHD that they faced.
“I had one tutor at university who didn’t believe in ADHD and dyslexia and that, she just believed it was a lazy excuse for not going to school”
“When I told my auntie [about my diagnosis], she was really unsupportive, and I was really shocked. She says she knows a lot of kids with ADHD and autism and says it is brought on by their diet and that makes them go crazy when their parents give them processed food”
One participant explained that they did not wish that they had their diagnosis sooner, as they felt that they would have faced even greater public misconception. Overall, participants remarked that the lack of understanding and awareness of ADHD in females is what led to their ADHD being undiagnosed throughout their childhood. However, some participants did acknowledge that awareness of ADHD in females is improving, but there is still a long way to go.
Selective Disclosure
As a result of the stigmatization and negative misconceptions surrounding ADHD, some participants avoided telling close friends, family, and colleagues about their diagnosis. Participants described that they felt like they would be judged and perceived differently for having ADHD.
“Even now, I don’t tell many people in my personal life about my diagnosis. I am a bit more open about it at university, but I am worried about what some family members and close friends will think of me if I tell them about it” “Now, like I don’t really tell people [about my diagnosis], like I tell my close friends and family, but for work, it’s very much a need to know basis, because I think, if you’re female, most people will just go right well you don’t have ADHD and you can’t be bothered explaining yourself really, so there’s just no point”
Theme 2—Journey to Receiving an ADHD Diagnosis
Symptoms Affecting Academic, Social, and Psychological Functioning
Prior to receiving a diagnosis, participants described struggling with various aspects of daily life, without realizing that their struggles were consistent with symptoms of ADHD. For many participants, these problems were most prevalent in an academic setting, primarily due to the inability to focus and maintain concentration. It has been widely documented in the literature that inattention, a core symptom of ADHD, is associated with poor academic functioning (Sedgwick, 2018). Several participants remarked that, although they did not do badly at school, they struggled with motivation, particularly in subjects that they did not enjoy.
“I was great in the subjects that I was good at, which was usually the more creative ones like, you know, the more practical subjects like PE, drama, and art, and I did really well in those. And it’s not to say I did really badly in other subjects, I was capable of doing it, but I just couldn’t focus to do it, so I refused to do the work”
Furthermore, most participants described having problems with time management and procrastination, and struggling to organize their thoughts, which acted as a barrier to performing well academically. Before receiving a diagnosis, many participants described that they felt that these symptoms were part of their personality and felt that they were “simply just not academic.” Though, not all participants struggled with academic performance; one participant described being a perfectionist and seeking a lot of self-worth and validation from her academic work, which led to overworking herself at school from a young age.
“If I didn’t do well on a test at school, I would completely have a meltdown, for me it was like the end of the world. . .I remember being at a parents evening when I was 11 years old, and the teacher told my parents that I was on the verge of burnout if I kept working as much as I was, which, you know, should not be happening to an 11 year old”
Consistent with the literature on ADHD, a recurring theme throughout all women’s experiences was suffering with low self-esteem, which had a profound impact on participants’ social, academic, and psychological functioning (Trzesniewski et al., 2006). Many participants described comparing themselves to other people around them, which left them feeling like “there is something wrong with me.”
“I really felt myself being inferior to other people, I suppose, and I always had a feeling that I wasn’t good enough. You know, you’re thinking what is wrong with me? Why can’t I do that? Why can’t I be as organised as other people? How do they do it?”
One participant described believing that “people had to put up with me, instead of enjoying my company, and I felt like I had to apologise for the way that I was,” which had a huge impact on their self-perception. Fifteen Linked to low self-esteem, many participants also described issues specifically related to their social functioning, including problems creating and maintaining friendships. For example, one participant described having “lots of acquaintances, but not very many close friends” as they struggled to hold onto close friendship groups, and often found that they would neglect friendships and relationships when they were busy or stressed. Some participants also described having problems with emotional dysregulation, which had a large impact on their social functioning.
“One of the biggest things that affected me was my emotional sensitivity, and like fear of rejection, like if a friend didn’t text me back, I thought they hated me. . .I think I would have benefited when I was younger knowing about that emotional side, as that really had a huge impact on my friendships and relationships which was pretty difficult”
Emotional dysregulation is a very common symptom of ADHD, often more severe amongst females (P. Shaw et al., 2014; Young et al., 2020). An aspect of emotional dysregulation, called rejection sensitive dysphoria (RSD), was described by several participants. RSD causes individuals to feel intense emotional pain from feeling as if you have failed to meet your own or other’s expectations (Bedrossian, 2021). RSD, though not widely recognized, is estimated to affect 99% of adults with ADHD (Bedrossian, 2021). Despite the social issues that participants faced, most participants described having a strong support network of family and friends with whom they could share their experiences and seek emotional help.
Prompted to Seek a Diagnosis by Others
Many participants described that they were prompted to seek a diagnosis by a member of their support network, such as a friend, family member, or colleague, who had recognized that they were presenting with some of the symptoms of ADHD. Despite acknowledging that they were struggling with certain aspects of their life, most participants commented that they did not realize that this could have been due to ADHD, as they were not aware of many of the symptoms of ADHD, particularly in females. A couple of participants reported that they had their suspicions that they might have ADHD but chose not to act on it. For 16 several participants, ADHD had been mentioned in their childhood, but, at the time, it was not taken seriously enough to seek professional help.
“I’ve got a friend who has ADHD, and she noticed a lot of similarities between us, and said it seemed like something I should follow up with. I sort of had a suspicion [that it might be ADHD], but I didn’t bother following up with it because it seemed like a lot of work, and at the time, I didn’t think it was impacting my life that much”
Some participants also disclosed that they had a comorbid condition, including dyslexia, autism spectrum disorder, or anxiety, and a history of issues with self-harm and eating disorders. Comorbidities were highlighted by several participants as a possible reason why they never realized that they also had ADHD. The presence of comorbidities in this sample are consistent with the literature, highlighting that comorbid disorders present possible overlapping symptoms with ADHD which can create challenges for diagnosis (Katzman et al., 2017). Seven out of eight participants referred themselves for a diagnosis after they researched more about ADHD and realized that they would benefit from seeking professional help.
Theme 3—Adulthood diagnosis
All participants received a diagnosis of ADHD in adulthood. For some participants, the diagnosis process was relatively quick and easy and lasted a matter of 3 months, however, for others, it took up to 2 years.
Mixed Emotions
After receiving a diagnosis, participants reported very mixed emotions. Most participants described feelings of relief and recognition. One participant described feeling like “a weight had been lifted off their shoulders,” as they felt that there was an explanation for why they had been struggling in many areas of their life.
“For me, there was a lot of relief. I mean, I had spent my whole adult life thinking that I just wasn’t good enough, and I kept falling short in a lot of areas of my life, I 17 thought I was lazy, I thought I was useless. . .so hearing that it wasn’t just me and there is something else going on, I guess, yeah, it was a huge relief”
However, not all participants felt a sense of relief following diagnosis. Despite acknowledging that diagnosis was a positive thing which meant that they would be able to get support, one participant commented that they “didn’t feel anything.”
Emotional Validation
Although there were mixed emotions initially, all participants described feelings of validation once they had time to think about their diagnosis. Participants were able to understand themselves better and noted that looking back, their behaviour “made sense.” Validated feelings and experiences improved participants’ self-esteem, and many participants reported being kinder and more compassionate to themselves following diagnosis. Furthermore, many participants implemented appropriate management strategies, such as seeking professional support and using good organization. For many participants, stimulant medication had been the most useful management strategy. Likewise, having a better understanding of their strengths and weaknesses meant that participants felt they had better control over their lives.
“Having a diagnosis has changed the way I approach lots of things, I plan things differently, I’m aware that I might struggle with certain things, and I don’t beat myself up if I can’t do things”
Since diagnosis, many participants returned to full-time education and started university, as they were able to approach things differently this time round. Participants generally reported receiving lots of support from their university, which made the experience of returning to education much easier for them. Some participants reported feeling like they needed to prove to themselves, and others, that they can do it. Participants described a need to fulfil their potential by going to university, and pursuing the career that they always wanted, but felt they were unable to achieve prior to being diagnosed with ADHD.
“I’ve spent my whole life thinking that I wasn’t capable [of going to university], and now I’ve finally got the belief and motivation behind me to do it. It’s almost like I’m 18 trying to prove something just to myself and everybody else that’s doubted my ability”
All participants benefited from receiving a diagnosis. However, there are still daily challenges that they face with ADHD. Participants explained that they have good and bad days, and with each day, they are constantly learning new things about themselves.
Discussion
The personal experiences of female students with ADHD explored in this qualitative study are rich and insightful, highlighting the profound impact of ADHD on social, academic, and psychological functioning.
The themes and sub-themes identified in this study overlap with previous literature surrounding females with ADHD. Many of the symptoms which affected participants academic functioning correspond with the literature review of ADHD in university students presented by Sedgwick (2018), including inability to focus, easily distracted, boredom, and lack of motivation. However, despite struggling with these symptoms and despite the wealth of literature which suggests that ADHD is associated with poor educational outcomes (Arnold et al., 2020; Daley & Birchwood, 2010; Sedgwick-Müller et al., 2022), most participants stated that they did not perform badly when they were at school (ages 5–16). As mentioned previously, one participant described that she was a perfectionist from a young age, driven by the validation of receiving good grades. This is in line with the research presented by Quinn (2005), highlighting that not all females with ADHD struggle with academic performance at school, as they often work harder to compensate for their symptoms and meet parent/teacher expectations. Greater challenges may present when an individual goes to university, as it becomes harder to cope with the struggles of ADHD amongst other lifestyle changes, such as moving away from home and having greater personal responsibilities (Quinn, 2005; Sedgwick-Müller et al., 2022). At the time of interviewing, all participants were at least 1 year into an undergraduate university degree, some even studying at master’s or doctorate level. With appropriate recognition, support, and management for their ADHD, participants were able to perform well academically and achieve their long-term goals by going to university. However, participants explained that they would often receive comments such as “you have a degree; you can’t have ADHD,” amongst other false claims that individuals with ADHD do not perform well academically. This highlights that, despite the literature and common perceptions, which often overlooks females, ADHD is not solely characterized by poor academic performance and poor educational outcomes.
Intense feelings of low self-esteem resonated throughout participants’ experiences. Poor self-esteem is very common amongst females with ADHD (Holthe & Langvik, 2017; Quinn, 2005), triggered by feelings of failure and “not being good enough.” Feelings of 20 inadequacy are exacerbated by other’s perceptions and expectations and ultimately, by an absence of an ADHD diagnosis throughout childhood. Low self-esteem has a knock-on effect on an individual’s social, academic, and psychological functioning. Participants explained that having low self-esteem negatively impacted many different aspects of their life, including body image, eating habits, confidence at school, romantic relationships, and close friendships. As outlined in the sub-theme of “emotional validation,” participants’ self-esteem improved significantly following diagnosis, as participants reported understanding themselves and their needs better, which allowed them to feel much more in control of their lives. It is evident that receiving a later diagnosis in adulthood had a profound negative impact on participant’s wellbeing throughout their childhood. This emphasizes the importance of earlier recognition and diagnosis of ADHD in females.
In accordance with the literature, participants also faced problems forming and maintaining friendships, particularly at school (Sedgwick, 2018). Despite this, most participants described having a strong support group formed of close friends and family members whom they could rely on for social and emotional help. A strong support group was further evidenced by the subtheme of “prompted to seek a diagnosis by others,” in which, for most participants, the possibility of having ADHD was first raised by someone within their support group. This further highlights the importance of disorder-related understanding, as with greater and more widespread understanding of ADHD in females comes greater recognition and diagnosis for those who need it.
The aim of the research was to explore the impact of ADHD on participants’ social, academic, and psychological functioning, as discussed in the themes of “journey to receiving an ADHD diagnosis” and “adulthood diagnosis.” However, following data analysis, the theme of “stigmatization surrounding ADHD in females” emerged from the data and became a highly influential element in participants’ experiences of ADHD. Most participants described at least one personal experience of public misconception, social discrimination, or prejudice. Stigmatizing attitudes towards both children and adults with ADHD are very common (Mueller et al., 2012). As a disorder, ADHD is vulnerable to stigmatization due to its largely unknown aetiology; there is not a single causal factor, nor a single diagnostic test used to identify ADHD. As a result, there are many public misconceptions about the origins of the disorder, including myths that ADHD occurs in children who eat too much sugar, or that it is caused by poor parenting (Mueller et al., 2012). These public misconceptions and stigmatizations are strengthened by a lack of disorder-related knowledge.
There is even greater stigmatization towards females with ADHD, in comparison to males, as it is publicly recognized as a disorder that predominantly affects boys. Schmitz et al. (2003) observed that the stereotypical profile of an individual with ADHD is described as “a young, white, middle-class boy suffering with hyperactivity.” Due to this common misperception, participants were often told that “they can’t have ADHD” or that “they aren’t hyperactive enough.” Furthermore, as confirmed by several participants in this study, females with ADHD often experience prejudice and social discrimination. For females, their disorder is often not taken seriously enough and they “feel like they aren’t being believed” by those whom they share their diagnosis with. McKeague et al. (2015) investigated experiences of stigma in young people with ADHD and observed that stigmatization from others results in negativity towards the self, called “self-stigma.” Self-stigma is an individual’s recognition that others hold prejudice and will discriminate towards them due to their disorder, which can severely affect one’s self-esteem and psychological wellbeing (Corrigan & Rao, 2012). Consequently, many participants reported that they are selective with whom they share details of their diagnosis with, in fear of being judged or perceived differently, or because they “don’t want to have to explain themselves.” This finding is in line with the findings of Holthe and Langvik (2017), who also identified the theme of “to tell or not to tell: selective disclosure” in their thematic analysis of adult women’s experiences with ADHD. This demonstrates that it is common amongst females with ADHD to withhold their diagnosis of ADHD from others, primarily due to the stigmatization and public misconceptions surrounding ADHD in females.
Overall, the women’s experiences discussed in this qualitative study draw attention to the complexity of ADHD. The heterogeneity of symptom presentation presents many challenges in recognizing and diagnosing ADHD in females. However, the overarching theme amongst all participant’s experiences is a clear lack of understanding of ADHD in females. Even amongst health professionals, there is a lack of appreciation of the differences in symptom presentation between males and females with ADHD, and an overwhelming existence of stigmatization. This lack of disorder-related knowledge, 22 alongside the presence of comorbidities, plays a key role in females receiving a late diagnosis of ADHD.
Limitations
This research responds to gaps in the literature by exploring several rich and detailed accounts of first-hand experiences of ADHD in adult female university students in the UK. However, there are number of caveats with the sample used in this study. Firstly, given that females with ADHD are largely underdiagnosed in the general population, the sample of formally diagnosed females used in this study may not be fully representative of females with ADHD in the wider population (Lynch & Davison, 2022). It is likely that many females in the general population have ADHD that is undiagnosed, possibly due to having less severe symptoms, or have reduced access to support, in comparison to the females in this sample. Additionally, as the participants used in this study were diagnosed during adulthood, their experiences will likely differ from those who received a diagnosis in childhood (Lynch & Davison, 2022).
Another caveat of the sample used in this study is the exclusion of participants who have comorbid diagnoses of another serious mental health disorder, such as a depressive disorder or personality disorder. This presents a severe limitation to the research as there is a high incidence of depression, amongst other psychiatric disorders, in females with ADHD (Solberg et al., 2018). Therefore, the results of this study are not representative of the entire population of females with ADHD. Possibly linked to the exclusion of participants with a serious mental health disorder, the results of the GHQ-28 identified that the participants in this sample were all in relatively good physical and psychological health. Thus, participants’ experiences will likely differ from those who are suffering with their health. Overall, the results of this study do not provide a complete picture of females with ADHD and should not be generalized to all contexts.
Implications and Directions for Future Research
Despite the addressed limitations, this research provides meaningful insight into the experiences of women with ADHD. Today, many women with ADHD experience stigmatization and social discrimination. Therefore, the clear take-home message of this study is the need for greater public understanding and appreciation of ADHD in females. Twenty-three Improving public knowledge of ADHD is important moving forwards to reduce stigmatization and debunk stereotypes of ADHD as a disorder that predominantly affects males.
Furthermore, greater understanding of ADHD is particularly important in allowing for earlier diagnosis of the disorder. Earlier diagnosis allows individuals with ADHD to develop effective management strategies, which in turn improves their social, academic, and psychological functioning. Greater public understanding of ADHD in females can be achieved through education. Moving forwards, particularly amongst health professionals and teachers, ADHD should be treated as a disorder that affects both males and females, and attention should be drawn to potential differences in symptomatic presentation between males and females.
However, ADHD in females should not be treated as separate to ADHD in males, as this can feed into further stereotypes. The findings of this study identify the need for larger scale research surrounding ADHD in females, to strengthen the validity of this research. In conclusion, the results of this qualitative study provide significant insight into the complex and challenging nature of ADHD amongst female university students in the UK.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.