
Abstract
This study examined the psychometric properties of the Czech translation of the Vanderbilt ADHD Diagnostic Parent Rating Scale (VADPRS), a tool used to assess ADHD symptoms. Data was collected online from parents of school-aged children and included questions related to their child’s diagnosis or treatment. The results showed that while relying on professional judgment improved specificity and positive predictive value, it decreased negative predictive value. These findings indicate that the VADPRS scale is more accurate in identifying individuals with ADHD when professionals provide the diagnosis, but fewer true negatives are found. This is the first study attempting to describe the psychometric properties of this tool in the Czech Republic and assess its use as an additional tool for ADHD diagnosis. It is recommended that structured clinical interviews be used to increase the accuracy of ADHD diagnosis.
Introduction
ADHD is a common neurodevelopmental disorder that manifests in behavioral abnormalities associated with concentration, hyperactivity, and impulsivity. The DSM-5 divides ADHD into the following three categories based on their predominant symptoms: ADHD Inattentive (I), Hyperactive-Impulsive (HI), and Combined presentation (American Psychiatric Association, 2013).
A child psychiatrist commonly diagnoses ADHD by confirming that the patient meets all criteria for ADHD as specified in DSM-5. However, a uniform and systematic assessment method can be facilitated in clinical practice using checklists and inventories, including teacher and parent questionnaires. Vanderbilt ADHD Parent Rating Scale (VADPRS) is a widely used example of a tool used to collect symptom patterns in a specific setting, such as home or school.
VADPRS has been developed based on DSM IV criteria for ADHD. The Vanderbilt scale includes two subscales incorporating all nine inattentive and nine hyperactive-impulsive DSM ADHD symptoms and assesses ODD (eight items) and internalizing symptoms (seven items). Each item is rated on a 4-point scale (0 = never and 3 = very often; National Institute for Children’s Healthy Quality, 2002). National norms are available in the United States (Anderson et al., 2022). However, this is not the case in Czechia yet.
The internal consistency and factor structure of the original English version of VADPRS are acceptable and consistent with DSM-IV and other accepted measures of ADHD (Wolraich et al., 2003). In a more recent study, internal consistencies for parents (teachers) were: ADHD inattention α = .89 (.93), ADHD hyperactivity impulsivity α = .90 (.94), ODD α = .91 (.89), anxiety α = .77 (.82), and depression α = .84 (.80; Becker et al., 2015). VADPRS also shows good psychometric properties when translated. A Polish study revealed satisfactory results and concluded high correlations between categorial DSM-IV symptoms and VADPRS (Kądziela-Olech, 2014). Similarly, the Greek version reached high internal consistency and may be used as an accurate psychometric instrument to diagnose ADHD (Kapogiannis et al., 2022). However, limited prior research suggests that younger children may have higher total ADHD symptom scores (Anderson et al., 2022). Further, age dependence of ADHD symptom burden on the Vanderbilt scale was not found in individuals aged 7 to 12 years in the Greek study (p = .209; Kapogiannis et al., 2022). Overall, the predictive ability of VADPRS varies from acceptable to strong, as research by Silverstein et al. (2016) shows Vanderbilt alone predicted a positive ADHD decision support diagnosis 56% of the time (95% confidence interval [CI] = 45%, 67%). In the full model—including all candidate covariates—the predictive validity rose to 84% (95% CI = 52%, 99%). However, some researchers reported poor root mean square error of approximation (RMSEA; Narad et al., 2015).
Overall, VADPRS seems to be a vital tool with good psychometric properties, such as high internal consistency and acceptable ability to predict ADHD (Wolraich et al. 2013). It, therefore, can be an essential adjunct to systematic clinical assessment that confirms full criteria for ADHD are met.
In Czechia, there is an existing translation of the Vanderbilt scale by Ptáček and Ptáčková, however, its psychometric properties have not yet been validated. Therefore, this study aimed to describe the psychometric properties of the Czech translation of part of the VADPRS focused on ADHD and assessed its use as a supplementary tool for ADHD diagnosis.
Methodology
Data were collected in cooperation with the STEM/MARK agency, which has a national panel of respondents. Data was collected online as the internet penetration was high enough to reach a representative number of participants. Parents of school-aged children were asked to complete a questionnaire that included the VADPRS and supplementary questions regarding their child’s diagnosis or treatment. We did not have access to medical databases, and thus medication information was not collected. Answers to the first 18 questions of the VADPRS were analyzed. For crosstabulation, VADPRS symptom patterns consistent with DSM combined presentation were used (threshold of six symptoms in both the inattentive and impulsive-hyperactive subscales). This was chosen because in Czechia ICD 10 is still utilised, and the criteria for hyperkinetic disorder most resemble the DSM combined presentation criteria. Furthermore, we calculated internal consistency, ROC curves, and diagnostic capabilities. For this analysis, VADPRS symptom thresholds that met current symptom criteria for all three forms of ADHD were included and analyzed - inattentive, impulsive hyperactive, and combined type. Data were analyzed using the R software (R Core Team, 2021).
Results
We collected data from 810 parents, 403 boys (49.75%) with a mean age of 8.19 years and 407 girls (50.25%) with a mean age of 8.17 years. The overall mean age was 8.18 years (min = 6 years; max = 10 years). Ninety-four parents (11.6%) reported that their child had previously been diagnosed with ADHD. Of these previously reported subjects, 63 were boys, and 31 were girls. 15.63% of the boys have been diagnosed with ADHD compared to 7.62% of the girls. The mean age for diagnosis was 6.06 years. The Czech version of the VADPRS was presented to parents to assess the ADHD symptomatology of their children. Since this is a screening tool, for the first 18 questions, answers “Often” and “Very Often” were counted (according to the advice of the American Academy of Pediatrics). We then investigated how many children met the symptom criteria threshold of 6 or more symptoms that would be required to be diagnosed with Inattentive ADHD presentation or Hyperactive-Impulsive ADHD presentation and how many fell into both categories as required to be diagnosed with Combined Type ADHD presentation. Results are presented in Table 1.
Vanderbilt Scale Parent Report ADHD Symptom Criteria Patterns by Sex and Age.
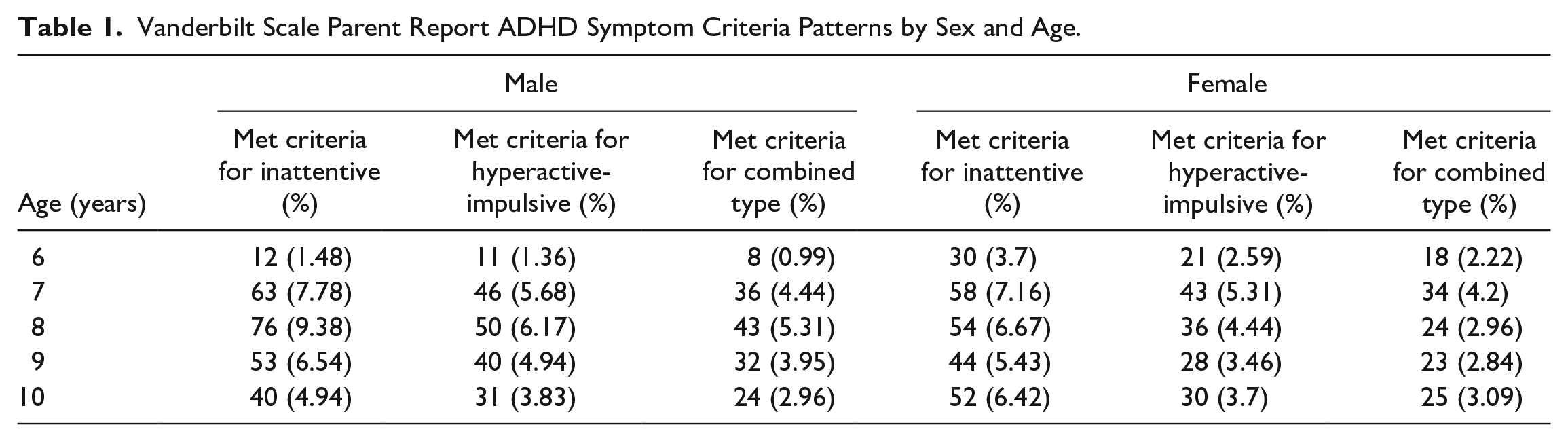
As can be seen, 33% of the sample scored above the thresholds consistent with sufficient current symptom burden to have Combined Type ADHD presentation (Table 1). If these individuals presented to clinical care with concerns about these symptoms, they, therefore, would be eligible for further assessment to diagnose or rule out ADHD diagnosis. We, therefore, investigated how many of these children were reported to have received the diagnosis as part of whatever clinical care they had received. Crosstabulation is shown in Table 2.
Crosstabulation of VADPRS Combined Type Symptom Criteria and Prior Reported Diagnosis.
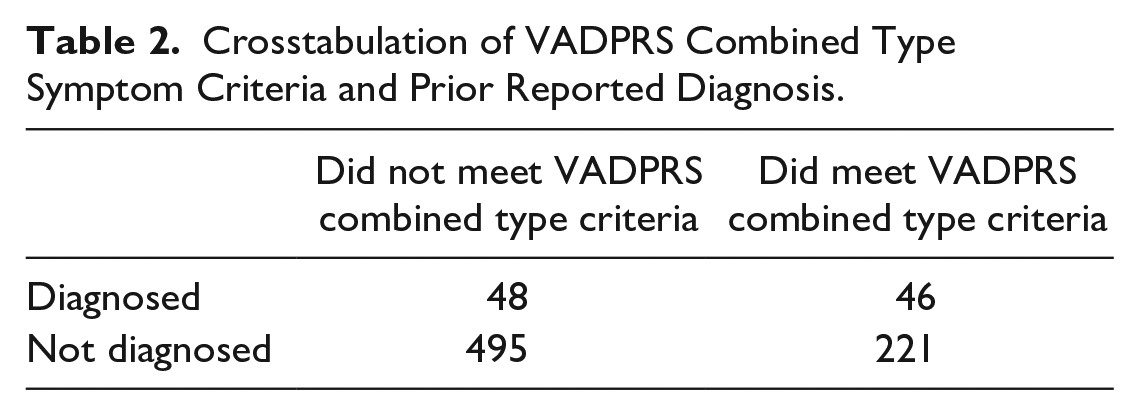
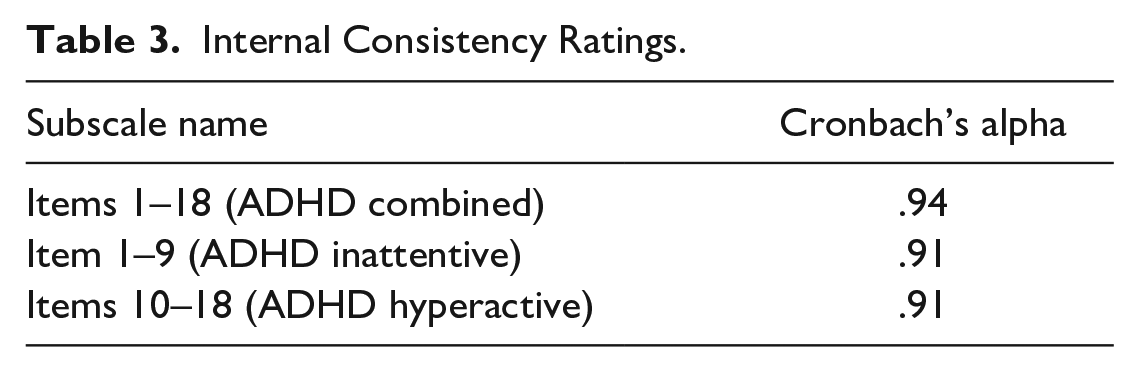
Table 2 shows that 48.94% of children with previous diagnoses also met the threshold for Combined Type diagnosis on the Vanderbilt scale. However, it is also important to note that only 17.23% of children who passed the threshold on the Vanderbilt scale have received the diagnosis. While this could be an appropriate proportion of Combined Type ADHD, it could reflect possible problems with the diagnostic accuracy of the translated Vanderbilt scale. Consequently, we checked the internal consistency of the scale. Table 3 shows the results and evidence of good internal consistency of subscales and total scale.
Internal Consistency Ratings.
We next conducted a confirmatory factor analysis. Since the items are scores from never to very often, they were treated as continuous. The model was fitted into the expected two-factor model, where items from first to ninth constitute ADHD predominantly inattentive type, and items 10 to 19 compose ADHD predominantly hyperactive-impulsive type. The overall model fit indices were slightly inconsistent, as expected. Chi-square (134) = 987.71, p = 0 was significant, most likely due to the sample size being more prominent than 200. A more robust indicator, such as CFI = 0.9 and SRMR = 0.05, showed quite a good fit. However, another often used index, RMSEA = 0.09, showed poor fit. Similarly, poor RMSEA has been reported for core scales of the VADPRS (Narad et al., 2015), while in other reports, better fit properties are reported (Bard et al., 2013.). Individual loadings are shown in Figure 1; all were significant at p < .001.
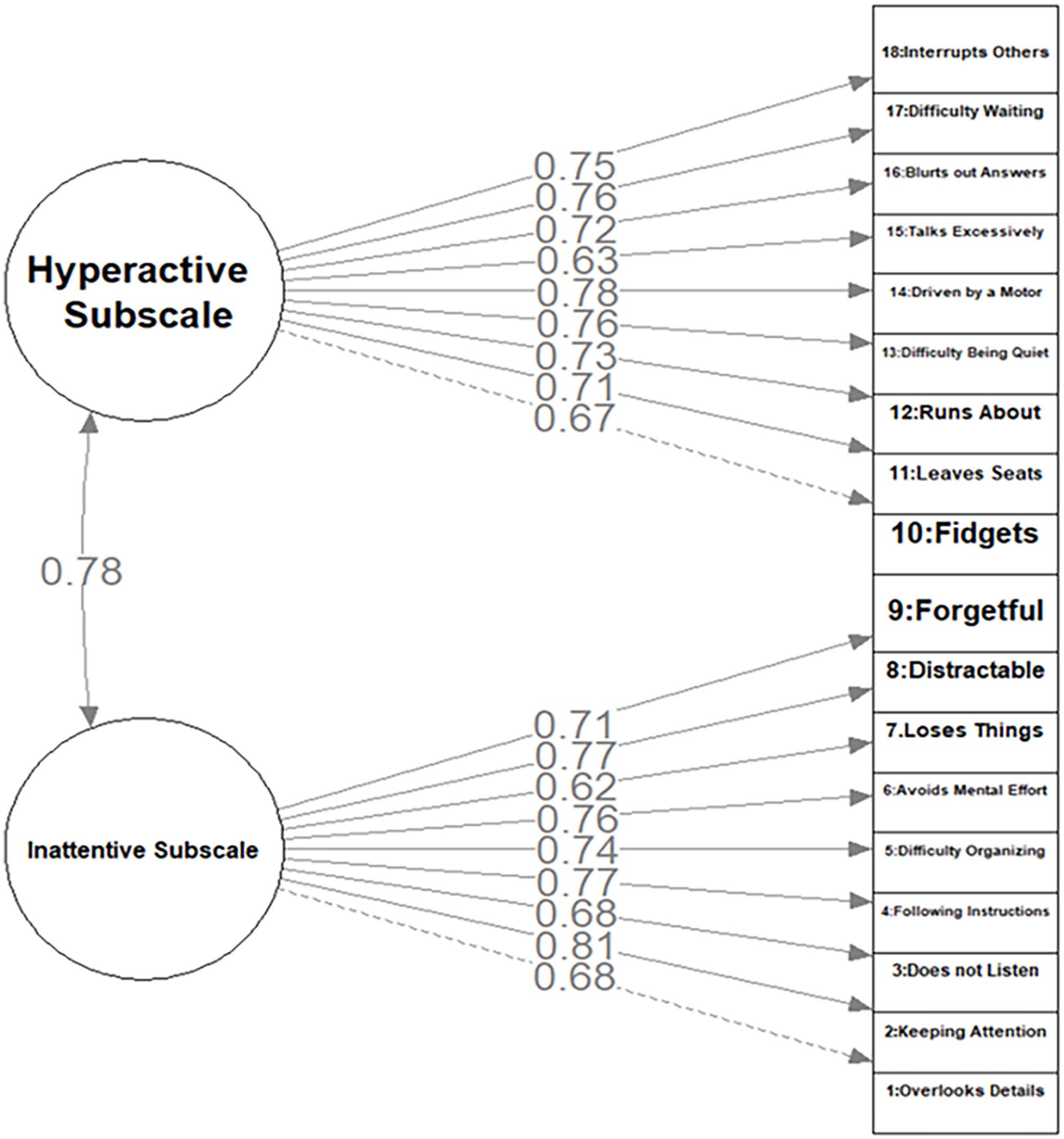
CFA factor loadings.
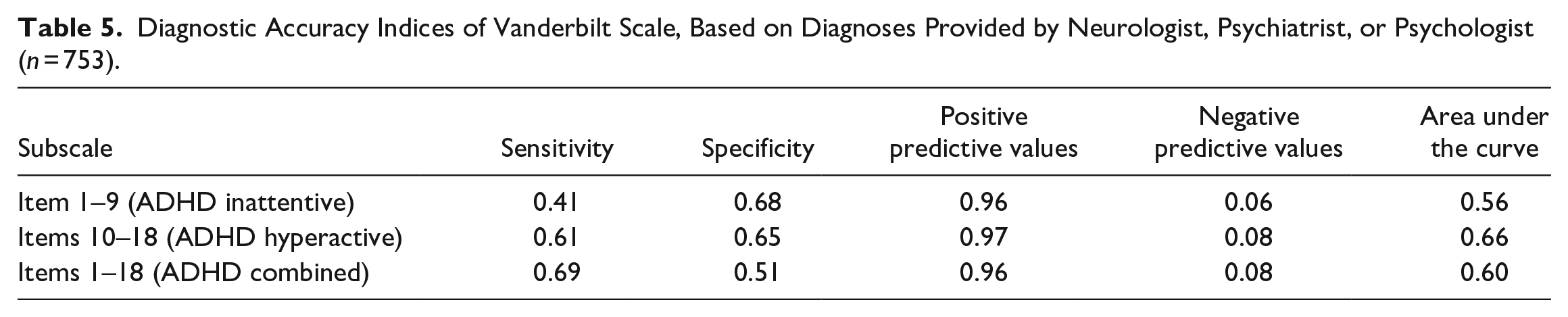
The last step of the questionnaire validation was calculating diagnostic accuracy using sensitivity, specificity, positive and negative predictive values (PPV and NPV), and area under the curve (AUC). These indices were calculated for two versions of the sample. Firstly for the whole sample, the diagnosis was given by either neurologist, psychiatrist, psychologist, pedagogic consultation, or someone else (Table 4). Then, due to the questionable expertise of pedagogic consultants and the inability to verify the expertise of other professions, the same indices were calculated only for trained professionals (Table 5). The analysis showed that while reliance only on professional judgment slightly improved specificity, PPV, and AUC of the Vanderbilt scale, it also decreased NPV. This shows that the Vanderbilt scale is more accurate in identifying individuals with ADHD when professionals provide the diagnosis;however, in such circumstances the proportion of true negative results (i.e. not scoring above the threshold when there is no diagnosis) to all negative results is smaller.
Diagnostic Accuracy Indices of Vanderbilt Scale, Based on Diagnoses Provided by Any Professional (n = 810).

Diagnostic Accuracy Indices of Vanderbilt Scale, Based on Diagnoses Provided by Neurologist, Psychiatrist, or Psychologist (n = 753).
Discussion
Considering that the commonly reported worldwide ADHD prevalence according to the DSM-5 is 5%, our results might suggest over-diagnosing of ADHD in early school-age children in the Czech Republic, given that 11.6% of the parents in our sample reported their child had received ADHD diagnosis in the past. Furthermore, it is essential to note that the diagnoses originated from diverse sources, many of whom were clinical professionals who are not routinely trained in the diagnostics and the differential diagnostics of neurodevelopmental disorders. Therefore, the psychometric properties presented might not necessarily reflect those of the VADPRS but rather the quality of the assessment procedure performed by differently trained professionals. Nonetheless, our report highlights the potential utility of implementing structured and standardized diagnostic tools such as the VADPRS to assess ADHD. Furthermore, the high rate of ADHD diagnosis suggests a need for precise regulation and specification regarding the qualification and authority/responsibility in diagnosing ADHD. The diagnosis must be solely reserved for fully trained medical professionals. We demonstrated that by relying only on parent assessment tools, we face the danger of inaccurately diagnosing ADHD. When combining parental assessment and clinical evaluation impression of diagnosis, we obtained better positive predictive values.
Nonetheless, further research must confirm and specify the prevalence of ADHD diagnosis globally. When looking at the results of the parent report scale only, an even higher rate of cases of ADHD in children is suggested. This would correspond with the previous findings that ADHD tends to be over-reported by parents. However, when combining the sources and looking at kids having received an ADHD diagnoses by a professional and a high score in symptomatology on parents’ ratings for combined presentation, we are looking at an overall prevalence of 5.68 %, which corresponds more closely to the majority reported in the DSM-5. Interestingly the biological gender pattern of combined type ADHD diagnosis was similar to prior studies. The ratio was 2:1 (male: female).
One of the limitations of our research is that the VADPRS teacher rating scale, clinical interview, and impairment measure were not incorporated into our analysis. In future studies, these measures should also be integrated because data from the Vanderbilt parent scale is insufficient to indicate the clinical diagnosis of ADHD. Further, we anchored symptom pattern assessment in the combined type presentation; therefore, our diagnostic results need to be interpreted cautiously.
However, overall, the Vanderbilt scale showed good properties at best. One of the reasons for its poor performance may be that as this scale was developed for DMS IV, it might need to be updated since DSM 5 is already being used. Furthermore, the Czech population may need different thresholds than are currently set. Notably, in the Czech version, the language indicating "sometimes" and "often" is not distinguishable. Thus the Czech version may measure symptom patterns differently.
To our knowledge, this is the first study to describe the psychometric properties of the Czech translation of the VADPRS elements focused on ADHD and assess its use as a supplementary tool for ADHD diagnosis in the Czech Republic. We implemented parent assessment tools and the participants’ history of diagnoses to uncover how these numbers correspond to the globally reported prevalence of the disorder. Although 11.6% of children have received an ADHD diagnosis in the past, 5.68 % of this was consistent with a combined type diagnosis by the parents’ assessment - a larger-than-expected proportion. For future research, we recommend that structured clinical interviews that review the full criteria for ADHD be used to ground ADHD case definition. To conclude, we demonstrated an urgent need for a more uniform and homogenous approach toward a reliable diagnosis and the need for professionals to work with children more closely to achieve this goal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Craig Surman, MD has received, in his lifetime, consulting fees from Eisai, Mcneil, Neurocentria, NLS Pharma, Nutricia, Pfizer, Adlon/Purdue, Rhodes, Shire, Somaxon, Sunovion, Supernus, Takeda, and Teva. He has also received payments for lectures for Alcobra, Arbor, McNeil, Janssen, Janssen-Ortho, Novartis, Shire, and Reed/MGH Academy (funded by multiple companies) as well as GME CME (funded by multiple companies). Royalties have been given to Dr. Surman from Berkeley/Penguin for Fast Minds: How to Thrive If You Have ADHD (or Think You Might) and from Humana/Springer for ADHD in Adults: A Practical Guide to Evaluation and Management. Additionally, Dr. Surman has conducted clinical research at Massachusetts General Hospital supported by The National Institutes of Health, Abbot, Cephalon, the Hilda and Preston Davis Foundation, Eli Lilly, Magceutics, Jazz/Axsome, Johnson & Johnson/McNeil, Lundbeck, Merck, Nordic Naturals, Shire, and Takeda.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Charles University institutional funding: Cooperatio program 207038 research area: Neurosciences, Psychology.