
Abstract
Objective:
In this review, we examined if there is a deficit in facial recognition of emotion (FER) in children, adolescents, and adults with attention deficit hyperactivity disorder (ADHD).
Background:
Emotional regulation is impaired in ADHD. Although a facial emotion recognition deficit has been described in this condition, the underlying causal mechanisms remain unclear.
Methods:
The search was performed in six databases in September 2022. Studies assessing children, adolescents, or adults with isolated or comorbid ADHD that evaluated participants using a FER task were included.
Results:
Twelve studies out of 385 were selected, with participants ranging in age from 6 to 37.1 years. A deficit in FER specific to ADHD, or secondary to comorbid autism spectrum disorder, anxiety, and oppositional symptoms, was found.
Conclusions:
There is a FER deficit in patients with ADHD. Adults showed improved recognition accuracy, reflecting partial compensation. ADHD symptoms and comorbidities appear to influence FER deficits.
Background
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by an inappropriate and persistent pattern of inattention, hyperactivity, and impulsivity (Christiansen et al., 2019; Dan, 2020). The global prevalence of ADHD is approximately 5% in the pediatric population and 2.5% in adults, making it one of the most prevalent disorders in the pediatric population (Christiansen et al., 2019). According to the DSM-V criteria, children who qualify for an ADHD diagnosis present six out of nine symptoms for at least 6 months, and the symptoms must occur globally, that is, they are present in at least two different settings (Austerman, 2015; Levelink et al., 2020). In the revised DSM-V-TR, ADHD is divided into predominant inattention, hyperactivity-impulsivity, and combined subtypes (Austerman, 2015).
The strategies designed to assess ADHD include the Vanderbilt ADHD rating scale, the Conners scale, the Diagnostic Interview for Children and Adolescents, and the Behavior Assessment System for Children (Christiansen et al., 2019; Zhou et al., 2018). However, an accurate assessment can be challenging in that many ADHD symptoms overlap with those of comorbid disorders.
Children with ADHD often have reduced working memory, response inhibition, and planning ability, and are less able to adapt to change compared with those without ADHD (Hilger et al., 2020). Moreover, emotional regulation deficits have been described in children and adolescents with this condition (Romani et al., 2018). This may manifest as altered facial emotion recognition (FER), which has also been described in individuals with borderline personality disorder, autism spectrum disorders (ASD), Parkinson’s disease, and schizophrenia (Romani et al., 2018; Villanueva-Valle et al., 2021).
Specific brain regions are known to be crucial for facial processing. These include the posterior occipital area, which detects specific areas of the face, the ventral medial prefrontal cortex, which directs attention to the eyes, the temporal lobe, which identifies familiar and unfamiliar faces, and the right posterior superior temporal sulcus and amygdala, which are responsible for the recognition of facial expressions (Romani et al., 2018).
Emotions can be divided into positive emotions such as surprise and happiness, negative emotions such as madness, sadness, fear, and disgust, and neutral facial expressions (Greco et al., 2021). Emotional deficits have been examined according to changes in emotional vocalizations as well as changes in biological parameters such as heart rate, which are related to autonomic responses (Villanueva-Valle et al., 2021).
Despite the publication of several reviews about FER in individuals with ADHD, there are conflicting data. For instance, some authors have proposed that children with externalizing behaviors exhibit a primary deficit in FER (Cooper et al., 2020) while others have suggested that altered FER is secondary to cognitive alterations in different age groups with ADHD (Borhani & Nejati, 2018), but yet no conclusion has been reached. Furthermore, no direct causality has been described regarding abnormal FER in individuals with ADHD, and
Methods
Study Design
This study was a systematic review of the literature following the PRISMA 2020 criteria for systematic reviews (Page et al., 2021). The protocol was registered under the PROSPERO ID CRD42022345250.
Search Strategy
An online search was performed in September 2022 using PubMed, Scopus, ScienceDirect, Embase for published literature, and Medrxiv and Google Scholar for gray literature. We used the MeSH terms: (“Attention Deficit Disorder with Hyperactivity”) AND ((“Facial Expression”) OR (“Facial Recognition”)) AND (“Emotions”). Moreover, a manual search was performed on the references of the articles selected for full-text screening. The search results were limited to the last 5 years (2017–2022). The last systematic reviews performed on children with diagnosed ADHD had search strategies performed until 2017, with inconclusive results (Borhani & Nejati, 2018; Romani et al., 2018). Therefore, this review intends to update the evidence since that year, discussing whether there is a primary or secondary facial emotion recognition deficit in people with ADHD with the newly generated information.
A single author performed the database search. The screening of titles, abstracts, and full texts was performed by pairs of authors. In case of discrepancy, a third author was called in order to reach a consensus for article inclusion.
Eligibility Criteria
The inclusion criteria were as follows: studies about pediatric, adolescent, or adult patients with isolated ADHD or with comorbidities, the presence of a control group without ADHD, and the evaluation of participants using a FER task, published between 2017 and 2022 in English or Spanish. The exclusion criteria were as follows: systematic reviews, editorial letters, book chapters, and evaluation of participants using tasks unrelated to FER.
Quality and Risk of Bias Assessment
All authors conducted a quality assessment of the selected studies using the Joanna Briggs Institute Critical Appraisal tools for cross-sectional analytic designs. Critical appraisal was also done through paired assessment of the studies. In case of discrepancy or doubts, a third author was called in order to reach a consensus for article inclusion.
Data Extraction
Relevant data were extracted by two researchers (M.O. and O.V.). The items extracted from each study included the author names, publication year, country, design, mean age and age range of the patients, sample size, types of comorbidities, instruments used to assess ADHD symptoms, subtypes of ADHD, use of medication, characteristics of the FER task used, and performance in the emotion recognition task.
Results
The selection process is shown in the PRISMA chart in Figure 1, and the data extraction is in Table 1. A total of 385 studies were found using the aforementioned search strategy in the regular databases and gray literature. There were 278 studies after eliminating the duplicates, of which 14 were included in the analysis (Figure 1). The data extraction showed that the measurements were not comparable owing to the absence of original data and standard measures for accuracy and response times. Some studies measured the mean number while others mean percentage, mean z score, median or accuracy percentage of correct responses, and mean error rates in different emotions. With respect to response times, some of the studies registered mean z score or mean reaction time in milliseconds while others did not report them. For these reasons, a meta-analysis could not be performed.
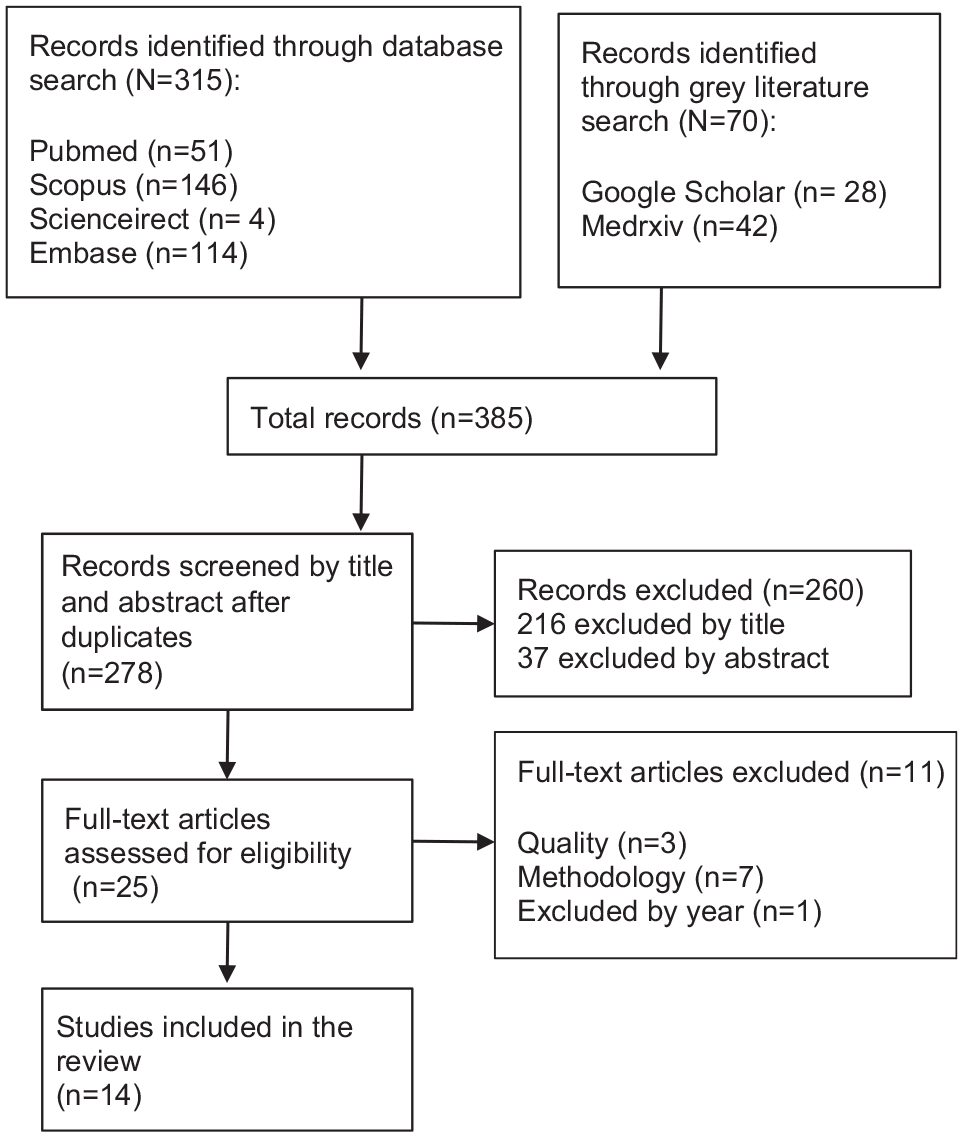
PRISMA algorithm for selection of the studies.
Data Extraction of Studies Evaluating FER in ADHD.
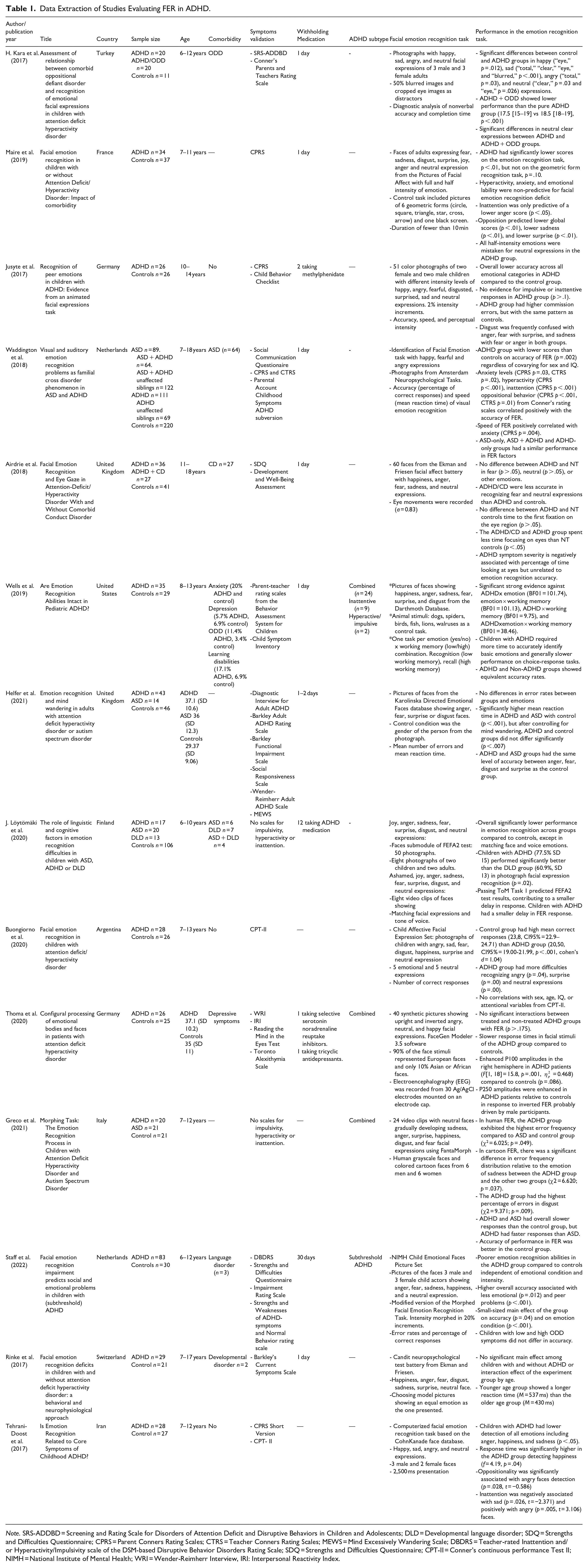
Note. SRS-ADDBD = Screening and Rating Scale for Disorders of Attention Deficit and Disruptive Behaviors in Children and Adolescents; DLD = Developmental language disorder; SDQ = Strengths and Difficulties Questionnaire; CPRS = Parent Conners Rating Scales; CTRS = Teacher Conners Rating Scales; MEWS = Mind Excessively Wandering Scale; DBDRS = Teacher-rated Inattention and/or Hyperactivity/Impulsivity scale of the DSM-based Disruptive Behavior Disorders Rating Scale; SDQ = Strengths and Difficulties Questionnaire; CPT-II = Conner’s continuous performance Test II; NIMH = National Institute of Mental Health; WRI = Wender-Reimherr Interview, IRI: Interpersonal Reactivity Index.
The studies encompassed a wide range of ages in the samples that were evaluated. Age varied from six (Kara et al., 2017; Löytömäki et al., 2020; Staff et al., 2022) to 37.1 (standard deviation, SD = 10.2) years (Helfer et al., 2021). Among these, one article included children (Löytömäki et al., 2020), two included adolescents (Airdrie et al., 2018; Jusyte et al., 2017), eight combined children and adolescents (Buongiorno et al., 2020; Greco et al., 2021; Jusyte et al., 2017; Kara et al., 2017; Maire et al., 2019; Staff et al., 2022; Waddington et al., 2018; Wells et al., 2019), and two included adults (Helfer et al., 2021; Thoma et al., 2020).
ADHD has been associated with particular comorbidities that were described in some of the studies. This included conduct disorder (n = 2) (Airdrie et al., 2018; Staff et al., 2022), anxiety (n = 1) (Wells et al., 2019), depression (n = 2) (Thoma et al., 2020; Wells et al., 2019), oppositional defiant disorder (ODD) (n = 2) (Kara et al., 2017; Wells et al., 2019), learning disabilities (n = 1) (Wells et al., 2019), language disorder (n = 2) (Löytömäki et al., 2020; Staff et al., 2022), ASD (n = 3) (Löytömäki et al., 2020; Thoma et al., 2020; Waddington et al., 2018), obsessive-compulsive disorder (n = 1) (Thoma et al., 2020), bipolar disorder (n = 1) (Thoma et al., 2020), and alcohol use disorder (n = 1) (Thoma et al., 2020).
Medication may be considered as another factor that can influence the obtained results in the included studies. Regarding the use of medication among the study participants, psycho-stimulant drugs were suspended 24 hr before the test in six studies (Airdrie et al., 2018; Helfer et al., 2021; Kara et al., 2017; Rinke et al., 2017; Waddington et al., 2018; Wells et al., 2019), while one study suspended medication in the prior month (Staff et al., 2022), three studies included people actively taking ADHD medication and antidepressants (Jusyte et al., 2017; Löytömäki et al., 2020; Maire et al., 2019), and one study suspended ADHD medication the day before the experiment but permitted continued antidepressant treatment in the patient group (Thoma et al., 2020).
Different positive and negative emotions were assessed in the studies, including sad, happy, angry, fearful, surprised, disgusted, shameful, and neutral expressions. Some studies used test batteries such as Ekman and Friesen’s facial affect battery (Airdrie et al., 2018; Rinke et al., 2017), the Child Affective Facial Expression Set (Buongiorno et al., 2020), the facial emotion task from the Amsterdam Neuropsychological Tasks (Waddington et al., 2018), the faces submodule of the Frankfurt Test and Training of Facial Affect Recognition second edition (FEFA2) (Löytömäki et al., 2020), the National Institute of Mental Health Child Emotional Faces Picture Set (Staff et al., 2022), and the Bochum Emotional Stimulus Set (Thoma et al., 2020). Other studies used facial emotion pictures from databases such as The Karolinska Directed Emotional Faces database (Helfer et al., 2021), the Cohn Kanade database (Tehrani-Doost et al., 2017), and the Dartmouth database (Wells et al., 2019). Finally, some authors employed morphing programs (Greco et al., 2021; Jusyte et al., 2017; Maire et al., 2019; Staff et al., 2022) in FER tasks.
Performance in Facial Emotion Recognition Tasks
Regarding FER task performance in ADHD patients and controls, three different possible outcomes were found. Some studies produced evidence for an intrinsic deficit in FER in individuals with ADHD, others supported the notion of abnormal FER as a secondary deficit in ADHD patients, and the third group indicated that there was no deficit in the participant group.
Evidence for Abnormal FER as a Primary Deficit in ADHD Patients
Many studies reported significantly higher FER performance in control groups compared with that in children and adolescents with confirmed (Buongiorno et al., 2020; Greco et al., 2021; Jusyte et al., 2017; Kara et al., 2017; Löytömäki et al., 2020; Maire et al., 2019; Tehrani-Doost et al., 2017; Waddington et al., 2018) and subthreshold ADHD (Staff et al., 2022). Some authors reported that the difference remained significant after controlling for disruptive behavior scores (Kara et al., 2017) and ODD symptoms (p = .463) (Staff et al., 2022), and that there was no correlation with impulsive or inattentive behavior (Jusyte et al., 2017), attention-related variables (Buongiorno et al., 2020), hyperactivity (Maire et al., 2019), or IQ (Buongiorno et al., 2020; Waddington et al., 2018).
Staff et al. (2022) found that higher FER task accuracy scores were associated with fewer emotional problems (p = .012) and decreased challenges with peer interactions (p < .001). Moreover, Jusyte et al. (2017) suggested that children with ADHD might exhibit a developmental delay rooted in unclear boundaries between emotional categories, while Maire et al. (2019) suggested that emotional development might be delayed in individuals with ADHD.
Evidence for Abnormal FER as a Secondary Deficit in ADHD Patients
In contrast, other studies found that inattention was correlated with FER accuracy (Conner’s Parent Rating Scale p < .001) (Waddington et al., 2018) in children and adolescents, and that it predicted lower anger recognition scores in children (ß = −.05, p < .05) (Maire et al., 2019; Tehrani-Doost et al., 2017). Moreover, inattention was negatively associated with sad face recognition (p = .026, t = −2.371) (Tehrani-Doost et al., 2017) in children. Hyperactivity (Conner Parent Rating Scale p < .001) (Waddington et al., 2018) and oppositional behavior were also correlated with FER accuracy in children and adolescents (Conner’s Parent Rating Scale p < .001; Conner’s Teacher Rating Scale p < .01) (Waddington et al., 2018), (ß = −.31, p < .01) (Maire et al., 2019). The latter was related to decreased recognition of sad (ß = −.05, p < .01)(Maire et al., 2019) and surprised faces (ß = −.04, p < .01)(Maire et al., 2019), suggesting that oppositional symptoms may negatively impact emotion recognition abilities in children (Maire et al., 2019; Tehrani-Doost et al., 2017).
In terms of the recognition of fearful and neutral expressions, Airdrie et al. (2018) only found FER differences in adolescents with ADHD and conduct disorder compared with the findings in controls (p < .05). This supports the idea that emotion recognition deficits in individuals with ADHD are specifically related to symptoms of conduct disorder. Additionally, anxiety symptoms were correlated with both the accuracy (CPRS p = .03, CTRS p = .02) and speed of FER in children (CPRS p = .004) (Waddington et al., 2018).
Löytömäki et al. (2020) suggested that the first-order theory of mind could predict delayed FER in children, evaluated using photographs (FEFA2). Similar to that in participants in ADHD, emotion recognition task performance was significantly lower in developmental language disorder (DLD) and ASD groups, compared with that in controls. This suggests the presence of shared difficulties in emotion recognition between these conditions. However, the ADHD group performed better than the DLD group (p = .02) (Löytömäki et al., 2020). Waddington et al. (2018) described similar FER performance in children with ADHD, those with ASD, and a comorbid ASD + ADHD group. Deficits in FER may be an overlapping feature of children with ADHD and ASD, as suggested by Greco et al. (2021).
Airdrie et al. (2018) simultaneously assessed eye movements during a FER task and found that adolescents with ADHD and conduct disorder symptoms spent less time focusing on the eye region of the face than controls. However, they found no differences between control groups and ADHD patients without conduct disorder symptoms.
Although Rinke et al. (2017) did not report significant differences between children with ADHD and controls in their study, the authors state that the deficit may be secondary and only occur with certain ADHD subtypes and emotions.
Evidence Against a FER Deficit in ADHD Patients
Airdrie et al. (2018), Helfer et al. (2021), Wells et al. (2019), Rinke et al. (2017), and Thoma et al. (2020) reported no significant differences in FER accuracy between ADHD groups and controls. However, in these studies, the FER speed in children with ADHD was slower than that in controls (Greco et al., 2021; Helfer et al., 2021; Wells et al., 2019). Wells et al. (2019) proposed that working memory affects the speed of recognition of basic emotions, which was consistent with their finding that individuals with ADHD exhibited slower performance in choice response tasks.
FER Performance According to Age Group
Most of the studies that reported significant deficits in FER accuracy in ADHD patients evaluated children and adolescents (Buongiorno et al., 2020; Greco et al., 2021; Jusyte et al., 2017; Kara et al., 2017; Löytömäki et al., 2020; Maire et al., 2019; Tehrani-Doost et al., 2017; Waddington et al., 2018), with the exception of Airdrie et al. (2018), Rinke et al. (2017) and Wells et al. (2019). In contrast, the studies performed on adults only reported slower response times without a deficit in the accuracy of the identified emotions (Helfer et al., 2021; Thoma et al., 2020). Yet, younger age groups (M = 537 ms) have higher response times than older age groups (M = 430 ms) regarding whether having ADHD condition is present or not (Rinke et al., 2017)
Happiness
Like Airdrie et al. (2018) and Buongiorno et al. (2020), Kara et al. (2017) found no statistically significant decrease in task performance for faces with happy facial expressions in children and adolescents with ADHD. Maire et al. (2019) reported similar results, with non-significant differences in the recognition of happy faces with expressions at half (p = .95) and full intensity (p = .08). However, children with ADHD showed lower task performance than controls for cropped eye images (“eye” p = .012) of happiness in the study of Kara et al. (2017), as well as a higher response time for happiness detection in the study of Tehrani-Doost et al. (2017).
Sadness
Kara et al. (2017) reported significant differences in sad facial expression recognition as well as eye expressions (p < .001) in children with ADHD. Greco et al. (2021) assessed recognition using cartoon faces and found a higher error frequency in children with ADHD (p = .037) compared with that in the control group. Like Airdrie et al. (2018) and Buongiorno et al. (2020), Maire et al. (2019) reported no statistically significant differences in sad FER in children with ADHD compared with that in a control group (p < .01). However, opposition symptoms predicted lower sadness recognition in children (p < .01) (Maire et al., 2019) and lower sadness recognition was also significantly related to inattention symptoms in Conner’s parent rating scales for ADHD (Tehrani-Doost et al., 2017).
Anger
Maire et al. (2019) found that inattention predicted lower anger performance (p < .05), but reported no statistically significant differences in children with pure ADHD for faces with half (p = .81) or full emotional expression intensity (p = .17) compared to the control group. This was consistent with the results of Kara et al. (2017) (p = .03) in children and Airdrie et al. (2018) in adolescents (p > .05). In contrast, Buongiorno et al. (2020) found that children with ADHD exhibited more difficulty recognizing angry facial expressions (p = .04) compared with controls. Tehrani-Doost et al. (2017) found that oppositional symptoms were associated with lower angry face detection in children as well.
Disgust
Greco et al. (2021) found that children with ADHD had a higher percentage of error when asked to evaluate disgust in cartoon faces (p = .009) compared to the control group—they were more likely to confuse disgust with anger (p = .035). However, Maire et al. (2019) did not find statistically significant differences in disgust recognition in ADHD patients for faces with half (p = .50) or full emotional expression intensity (p = .91) in children. These findings were similar to those of Buongiorno et al. (2020).
Fear
Airdrie et al. (2018) reported that adolescents with ADHD group had less accurate FER for fearful faces compared with controls (p < .01), while participants with ADHD and conduct disorder were less accurate than those with pure ADHD and controls (p < .001). Maire et al. (2019) found no statistically significant differences in fear recognition in children with ADHD for facial expressions with half (p = .43) or full intensity (p = .99). These findings were similar to those of Buongiorno et al. (2020).
Surprise
Maire et al. (2019) found no statistically significant differences in surprise recognition in children with ADHD for faces with half (p = .99) or full emotional intensity (p = .82), however, the presence of oppositional behaviors predicted poorer recognition (p < .01). In contrast, Buongiorno et al. (2020) reported that children with ADHD exhibited more difficulty in surprise recognition (p = .00). This was supported by Greco et al. (2021), who found that children with ADHD had a higher percentage of error recognition for surprised human faces compared with controls (p = .049)
Neutral Expressions
Airdrie et al. (2018) reported significantly lower accuracy in identifying neutral facial expressions in adolescents with ADHD compared with that in control participants (p < .5). This was consistent with the results of children assessed by Kara et al. (2017) (clear face emotions, p = .03; cropped eye emotions p = .026) and Buongiorno et al. (2020) (p = .00). Difficulty recognizing neutral facial expressions was accentuated in individuals with both ADHD and conduct disorder (p < .001) (Airdrie et al., 2018).
Jusyte et al. (2017) reported that overall, children with ADHD had lower FER for anger, happiness, fear, disgust, sadness, and surprise, compared with a control group. This was similar to the findings of Staff et al. (2022) (p = 0.611), except that they did not evaluate disgust or surprise, and similar to the findings of Tehrani-Doost et al. (2017) which evaluated only anger, happiness, and sadness in children. In contrast, Wells et al. (2019) described equivalent accuracy rates among the evaluated emotions in children with and without ADHD. Similarly, Helfer et al. (2021) reported similar levels of accuracy for facial expressions showing anger, fear, disgust, and surprise in controls and adults with ADHD.
Discussion
We hypothesized that individuals with ADHD might have a specific deficit in FER. The high heterogeneity of the results indicates that additional factors, yet to be elucidated, influence FER deficits among children and adults with ADHD. This review examined the influence of different factors such as age, ADHD symptoms, and comorbidities.
Age
As mentioned above, all except three of the included studies favored a FER deficit in children and adolescents with ADHD compared with the findings in controls (Airdrie et al., 2018; Rinke et al., 2017; Wells et al., 2019). This is consistent with previous studies indicating that these patients have emotional recognition deficits related to emotional expression, regulation, and understanding (Borhani & Nejati, 2018). Rodrigo-Ruiz et al. (2017) suggested that children with ADHD exhibit impaired FER as a primary deficit and that this results from reduced emotional intelligence and emotional perception accuracy.
Contrary to Borhani and Nejati (2018) and Lindholm et al. (2019), the other studies included in this review show that FER deficits in children with ADHD were alleviated across development and that, although adults with ADHD had a higher response time, they showed no deficits in FER accuracy (Helfer et al., 2021; Thoma et al., 2020). Likewise, the effects of age were observed in the mean reaction time of emotion recognition, being shorter in older children, and having more accurate anger recognition despite having or not having the ADHD condition (Rinke et al., 2017). This reflects that age is one of the intervening factors in FER tasks.
Overall, happiness was the emotion that has better recognition across different age groups, as supported by Rodger et al. (2015) who found that happiness has the lowest recognition threshold. In the same study, the response of facial expression recognition for fear also remains stable across development. This explains why fear was reported with a less accurate response in both, ADHD children and adolescents in the studies included in this review.
Tsurumi et al. (2019) conducted several experiments and reported that 7 to 8-month-old infants were capable of correctly identifying a face. However, the identification of emotion in a face is a more complex process. Kujawa et al. (2014) found that emotion identification accuracy develops throughout childhood and adolescence and that the identification of basic emotions (happiness and sadness) appears at approximately 5 years of age. More elaborate emotions (fear, disgust, anger, and neutral emotions) emerge at 11 years old, at which this ability is comparable to that of an adult (Kujawa et al., 2014).
Thoma et al. (2020) suggested that the enhancement of event-related potentials at 250 ms component might indicate disrupted or delayed maturation in these systems, reflecting compensation for poorer inhibition of incorrect stimulus representations and categorization of stimuli. This is supported by functional Magnetic Resonance Imaging findings regarding activity in regions associated with emotional regulation and behavior, which led Dan (2020) to suggest that individuals might compensate for emotional recognition deficits after facing social challenges in daily life. Compensation might occur via changes in the structure of the inferior occipital and fusiform regions that integrate visual information, which matures by late adolescence and adulthood (Leppänen & Nelson, 2009).
This review included studies that examined different age groups. We found varied results for specific emotion recognition abilities, even within the same age groups, except for adults (both with and without pure ADHD), who had more accurate FER in general compared with children (Helfer et al., 2021; Thoma et al., 2020). This indicates that there are other factors involved in FER deficits in addition to age.
The Effect of ADHD Symptoms or Comorbidities on FER Deficits
In this review, while some authors found that ADHD symptoms and comorbidities such as inattention, hyperactivity, oppositional behavior, conduct disorder, and anxiety were related to FER deficits, others presented contrasting evidence or even found no evidence of FER deficits.
The emotional symptoms associated with ADHD are characteristic of a range of comorbid psychiatric disorders. Thus, these symptoms may be explained by the phenomenon of comorbidity (Faraone et al., 2019).
Inattention
Inattention has been previously proposed to influence FER deficits in children without a diagnosis of ADHD (Cooper et al., 2020). Muszkat et al. (2015) suggested that FER deficits might be attributed to poor allocation of attention to specific cues (Muszkat et al., 2015). Consistent with this, some authors have proposed that deficits in sustained attention and visual processing play a role in FER, as supported by the observation of increased gamma oscillations in occipital regions during the early stages of facial emotion processing (Sarraf Razavi et al., 2017). Additionally, more robust functional connectivity has been observed in the frontal lobes of children with ADHD, which may indicate the abnormal transfer of information from the occipital lobe to the frontal lobe, that is, from the visual to the emotional processing center (Ansari Nasab et al., 2022).
Impulsivity
Regarding the contribution of impulsivity symptoms to FER deficits, Cortez-Carbonell and Cerić (2017) stated that ADHD groups showed faster responses to a stimulus but had higher error rates, indicating that they may have been acting with higher impulsivity (Cortez-Carbonell & Cerić, 2017). Faraone et al. (2019) suggested that individuals with ADHD might have emotional management difficulties related to the consequences of impulsivity. These difficulties could first manifest as impaired self-regulation and then evolve into deficient emotional self-regulation.
Hyperactivity
The correlation between hyperactivity symptoms and FER deficits proposed by some of the included studies was supported by previous studies that related hyperactivity not only to lower recognition of happy and angry expressions, but also to that of angry, happy, and sad vocal expressions (Chronaki et al., 2015).
Anxiety
Stoddard et al. (2017) reported that high levels of anxiety were associated with increased connectivity in the amygdala and medial prefrontal cortex during FER in children and adolescents without ADHD, which may be a possible mechanism of the impact of anxiety on FER.
Autism Spectrum Disorder
The included studies reported similar FER deficits in individuals with ADHD and ASD. This is supported by other studies demonstrating shared neural processing of happy and angry emotional faces between neurodevelopmental disorders, particularly in the occipital and temporal regions (Vandewouw et al., 2020).
Medication
An infrared imaging study in children with ADHD found an increased hemodynamic response in the left inferior occipital region after methylphenidate administration for angry faces only (Kobayashi et al., 2020). However, the FER deficits reported in the included studies did not vary on the time scale of the methylphenidate suspension prior to task evaluation. Supporting these previous findings, Moukhtarian et al. (2017) reported that pharmacotherapy (methylphenidate or atomoxetine) minimally impacted emotion dysregulation in comparison with core ADHD symptoms.
Some of the included studies found no differences in FER accuracy between individuals with ADHD and controls (Basile et al., 2021). This might be partially explained by the findings of Rinke et al. (2017), who stated that FER accuracy is age-dependent such that older children display better FER accuracy regardless of ADHD condition (Rinke et al., 2017). However, this does not explain why adults and adolescents with ADHD still exhibited delayed FER response times.
Limitations
The included studies did not have a standardized methodology as some FER tasks used the faces of adults while others used children’s faces, there were different colors of the faces displayed (full color or gray-scale), different ethnicities, and different emotions which may have affected the results. Furthermore, we only considered studies with FER tasks, but there are other tasks such as emotional prosody recognition and emotional response registered as functional brain activation, and changes in heart frequency, among others, that were mentioned but not included in this review. Those studies can provide additional valuable evidence about the mechanisms of emotional response.
All the studies have evaluated emotions as a specific task either on a screen, on a card, or on paper. More studies are needed that recreate a natural scenario of social interaction for emotion recognition, interpretation, and response, to evaluate if the deficit occurs in more than one of the mentioned phases and if it also commits the emotional response of people with ADHD.
The results of this review also suggest that the FER deficit is a shared deficit with other neurodevelopmental comorbidities, which may have implications as a clinical marker that remain to be explored.
Conclusion
There is evidence for a FER deficit in children and adults with ADHD, as indicated by prolonged response latencies of emotion recognition. Regarding the type of deficit, most studies demonstrated overall better recognition of happy facial expressions in children and adults with and without ADHD. Moreover, adults with ADHD showed improved recognition accuracy compared to children with ADHD, reflecting partial compensation of the deficit. Some factors, such as the use of medication for ADHD, did not impact FER outcomes. However, other factors such as the characteristics of ADHD and its comorbidities appear to influence FER deficits. These remain to be elucidated.
Footnotes
Acknowledgements
We thank Sydney Koke, MFA, from Edanz for editing a draft of this manuscript.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of Universidad del Rosario.
Author Contributions
AV- VM, CT-G, and MD-OG conceived the idea and design of the study. CT-G and AV-VM corrected and revised the methodological design. MD-OG performed the search. All authors performed the critical appraisal and full-text selection of the articles filtered the articles by title and abstract, and read and edited the initial draft of the manuscript. MD-OG and OA-VC were responsible for writing the initial draft of the manuscript. All authors read and approved the final version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report was supported by Universidad del Rosario.
Ethics Approval
This review was approved by the Research Ethical Committee of the School of Medicine and Health Sciences of the Universidad del Rosario.