
Abstract
Objective:
Across contexts, from social cognition to the COVID-19 pandemic response, individual variation in the regulation of interpersonal distance has typically been viewed as a voluntary choice. Here we examine the frequency of unintentional lapses in interpersonal distancing, and their relationship with childhood ADHD symptoms.
Method:
We administered a novel measure of difficulty with interpersonal distancing across three undergraduate samples (total N = 1,225), in addition to measures of recalled childhood ADHD symptoms, mind wandering, and hyperfocus.
Results:
Almost all (>97%) participants reported unintentional lapses in maintaining interpersonal distance, with 16% experiencing such lapses frequently. Thirty percent of the variance in these reports was accounted for by attentional traits: Inattentive and hyperactive/impulsive ADHD symptoms jointly predicted difficulties with interpersonal distancing, with the former relationship fully mediated by hyperfocus and spontaneous mind wandering.
Conclusion:
Both inattentive and hyperactive/impulsive ADHD symptoms confer vulnerability to frequent unintentional lapses in interpersonal distancing.
During the COVID-19 pandemic, psychological science has played a vital role in informing behavioral interventions, with investigations exploring how to best design, implement, and communicate effective behavioral measures such as social distancing. Social distancing measures include both the proactive avoidance of social situations (e.g., remaining at home when possible) and interpersonal distancing (e.g., maintaining a minimum physical interpersonal distance of 1–2 m when in social contexts; Bavel et al., 2020). These behavioral interventions will remain relevant even after the current COVID-19 pandemic, as animal-human transmission of novel viruses remains an unresolved and ongoing threat (Gray et al., 2021).
A key line of research has been the identification of barriers to compliance with social distancing measures, which has found that factors such as low empathy, low working memory capacity, and high Attention Deficit Hyperactivity Disorder (ADHD) symptoms predict greater non-compliance with measures such as mask wearing and some aspects of social distancing (e.g., avoiding crowds, remaining at home; Pfattheicher et al., 2020; Pollak et al., 2022; Xie et al., 2020). A consistent pattern across this previous research is that social distancing is conceptualized as a deliberate and motivated choice, with variation reflecting risky decision making.
Though these findings provide significant insight, they don’t address compliance with a key component of social distancing measures: The mandated 1 to 2 m distancing rule, requiring maintenance of interpersonal distance in immediate social situations. This omission is significant given the established effectiveness of these measures in reducing viral transmission (Chu et al., 2020), and their ability to be adopted on a longer-term basis than more extreme stay at home measures.
Physical distancing has been explored in other work non-specific to the pandemic distancing orders, such as the determinants of interpersonal avoidance in prejudice and anxiety (Fasoli et al., 2016; Goff et al., 2008; Perry et al., 2015); or proximity seeking in social relationships and attachment style (Kaitz et al., 2004; Sundstrom & Altman, 1976), after alcohol consumption (Gurrieri et al., 2021), or when sharing a social identity (Templeton et al., 2018). This research has conceptualized interpersonal physical distancing as a deliberate choice or behavior in line with personal values. Here we argue that (1) the maintenance of interpersonal distancing is not solely a personal choice, but may also require a “person radar” which is dependent upon available attentional capacity to monitor and maintain interpersonal distance; and (2) this “person radar” may be potentially compromised in the context of attention disorders.
The necessity of attention for successful interpersonal distancing is supported by recent evidence that cell phone use can lead to disrupted crowd movements and more frequent collisions (Murakami et al., 2021). Similar disruption to our “person radar” could conceivably come from any daily life task that is performed in busy contexts. For example, consider the multiple attentionally demanding processes that must be simultaneously performed during grocery shopping: (1) Maintain the primary goal to look for groceries; (2) recall/consult the list of specific groceries; (3) plan a route based on spatial memory; (4) maintain the secondary goal to interpersonally distance; (5) search for people nearby and encode their positions; and (6) monitor and anticipate their movements based on inferred intentions. As such, interpersonal distancing may be driven not only by voluntary factors, but also involuntary lapses resulting from the combined attentional demands of the “person radar” (i.e., steps 4–6 above) plus any concurrent task exceeding an individual’s capacity.
Present Study
Recognizing the potential contribution of involuntary lapses of attention is key to effectively understanding and predicting distancing behavior. The first aim of the present work was hence to establish the frequency with which people report experiencing unintentional lapses in the ability to monitor and maintain appropriate physical distance from others. To this end, we measured the frequency that involuntary lapses in this “person radar” occurred by developing the Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS). Using this novel scale we were then able to measure the prevalence of difficulties in three large samples. The view of interpersonal distancing as an attentionally demanding process, vulnerable to involuntary lapses, implies that individual differences in attention could impact the likelihood of such lapses (and hence the ability to comply with social distancing regulations). Our second aim was to test this possibility. Our initial study examined the relationship between DIDAS scores and symptoms of ADHD. These symptoms are thought to reflect a stable genetically determined trait distributed on a continuous spectrum throughout the population, with the clinical diagnosis of ADHD reflecting the extreme end of this spectrum (Demontis et al., 2019). ADHD symptoms are clustered into two strands, comprised of inattention and hyperactivity/impulsivity (American Psychiatric Association, 2013).
Although no study to our knowledge has examined interpersonal distancing in ADHD, evidence from road safety research suggests that ADHD has been linked to more inattentive driving (e.g., mind wandering) resulting in worse distancing from other vehicles, more collisions, and lower driving competence scores (Biederman et al., 2007; Randell et al., 2020). It appears plausible that the same inattentive symptoms might similarly predict difficulties with interpersonal distancing from people. To further illuminate the relationship between interpersonal distancing and attention, our second investigation examined the influence of trait propensity to specific inattentive behaviors which are strongly linked to ADHD, but are also widely experienced states across the population: Mind wandering and hyperfocus (Hupfeld et al., 2019; Seli, Smallwood et al., 2015). Mind wandering reflects the disengagement of attention from the external environment toward internal thoughts, and can reflect either purposeful thought (i.e., deliberate mind wandering) or uncontrolled attention to extraneous thoughts (i.e., spontaneous mind wandering; Seli, Carriere et al., 2015; Seli et al., 2016). It is well established that mind wandering can result in reduced processing of the external environment (Schooler et al., 2011), and as such might plausibly interfere with awareness of the presence and movements of people around us.
Hyperfocus, on the other hand, is the tendency to over-attend to a single external task at the expense of attending to other stimuli in the environment (Ashinoff & Abu-Akel, 2021). In our supermarket example, hyperfocus would result in focusing purely on the primary goal to find groceries at the cost of attending to those around us; conversely, mind wandering would result in the preoccupation with thoughts about ongoing concerns.
In summary, we aim to explore the prevalence of difficulties with interpersonal distancing, and the extent to which vulnerability to such difficulties is predicted by ADHD symptoms, and the ADHD-related traits of mind wandering and hyperfocus. If, as we predict, ADHD symptoms confer vulnerability to unintentional lapses in interpersonal distancing, this could represent a potential mediator of a range of negative outcomes associated with ADHD, from the increased risk of respiratory viral infection (e.g., Merzon et al., 2021) to negative social outcomes (e.g., Grygiel et al., 2018; Kofler et al., 2011). Factoring in the limited control some individuals have over interpersonal distancing will enable more effective modeling of distancing behavior in social settings, which will both allow the design of more effective interventions for the purposes of disease control, as well as understanding social cognition and outcomes associated with attention.
Study 1a and 1b
Methods
Participants
Study 1a
Initially 510 undergraduate participants took part in the online survey as part of a practical class delivered online. The sample size was based on the maximum number of students who could be recruited from this class. However, 23 participants were excluded for either not completing all the measures, reporting a near-impossible age (i.e., >99) likely indicative of false responses, or not having normal or corrected-to-normal vision. These identical exclusion criteria were applied to all subsequent studies, except Study 1b where vision was not recorded. The final sample consisted of 487 participants, the average age was 20.71 years (SD = 3.10, range = 18–48). Despite the wide range of ages, the majority of the sample were young adults with 93.63% being below the age of 25 (n = 456). Three-hundred and eighty participants identified as “female,” 103 as “male,” and 4 as "another gender". Data collection was conducted in October 2020.
Ethical approval for all studies (Study 1a, 1b, and 2) were granted by the University of Sussex Science & Technology Research Ethics Committee (approved codes: ER/SF80)/32, ER/SF280/35). All studies were in accordance with the 1964 Declaration of HELSINKI.
Study 1b
Initially 446 individuals responded to the survey link via social media advert or when contacted through an undergraduate mailing list, with 355 participants providing data beyond initial consent and demographics. Applying the exclusion criteria listed in Study 1a resulted in eight participants being excluded. Within the final sample of 347 participants the average age was 21.77 years (SD = 2.81, range = 18–44), with 218 participants identifying as “female,” 123 as “male,” 1 as “another gender,” and 5 preferring not to answer. As in Study 1a, most of the sample were young adults with 90.80% being below the age of 25 (n = 316). Data collection was conducted between October 2020 and March 2021, the sample size was based on the maximum number of participants who could be recruited during this period.
Materials
Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS)
To measure self-reported capacity to maintain social distance and monitor inter-personal range we developed an 8-item scale. The items are designed to tap into unintentional lapses in interpersonal distancing in shared spaces: For example, instances when the individual was told they had become too close after being unaware, or when lapses in monitoring social distance had manifested as physically bumping into someone. See Table 1 for all items and Cronbach’s reliability analysis.
Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS) Scale Individual Items and Parameter Estimates Calculated from Confirmatory Factor Analysis.
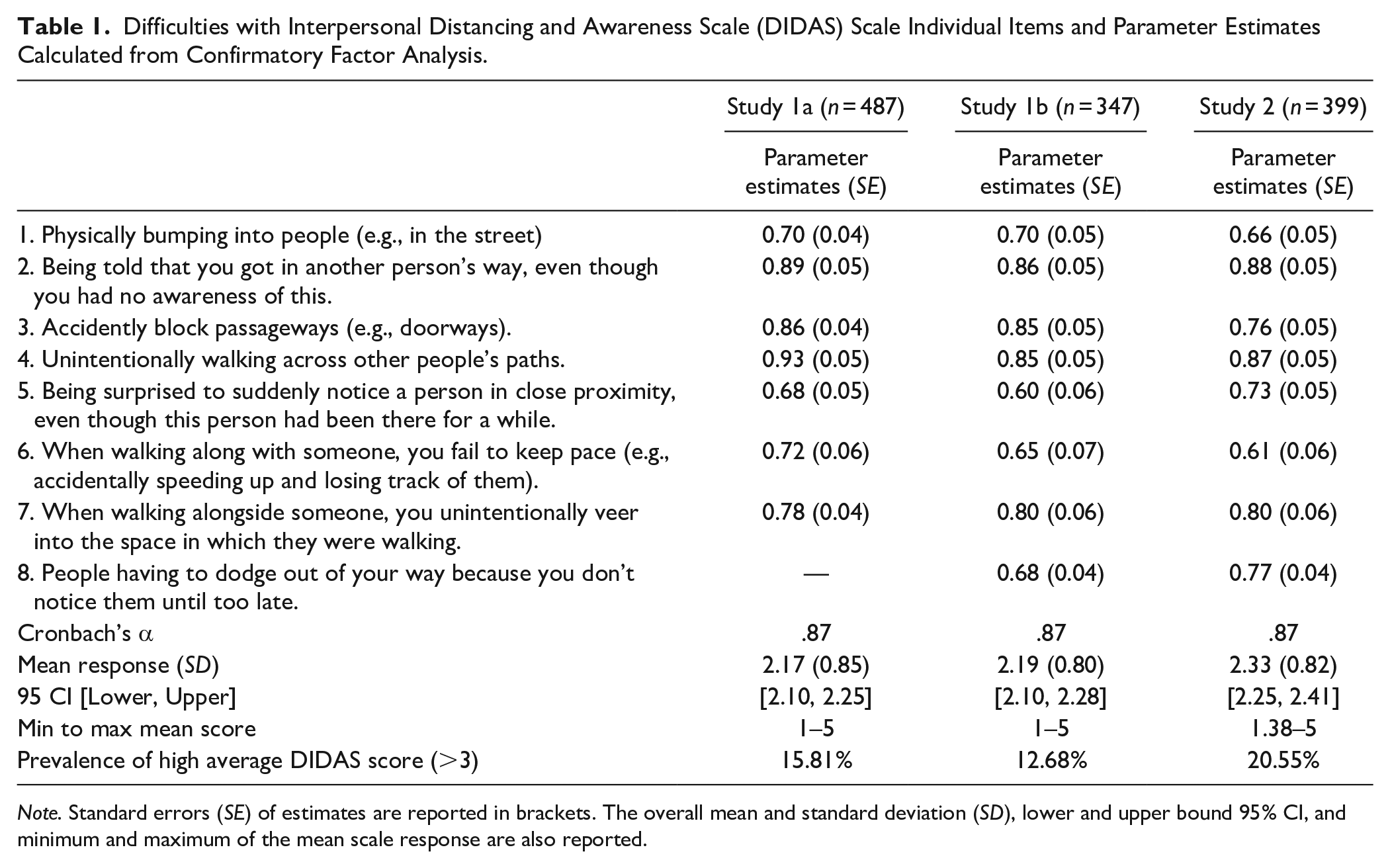
Note. Standard errors (SE) of estimates are reported in brackets. The overall mean and standard deviation (SD), lower and upper bound 95% CI, and minimum and maximum of the mean scale response are also reported.
Each item is rated along a 5-point Likert scale ranging from “Never” (1) to “Very Often” (5). The scale is prefaced with the instruction to “Considering your overall life experience rather than recent months, indicate how often do you generally experience the following situations,” thus the questionnaire was designed to measure the general difficulty with monitoring social distancing, rather than specifically adherence to COVID-19 distancing orders. The total scale consists of eight items, though within Study 1a the final item was omitted due to a programming error. We analyzed the score as the average response given across items. The final score therefore ranges between 1 and 5, with a high score reflecting greater difficulties with monitoring and maintaining interpersonal distance, and any score above 1 reflecting at least some difficulties.
Childhood ADHD Symptoms Scale
To measure ADHD symptoms, participants completed the 18-item Childhood ADHD Symptoms Scale which included two 9-item subscales (Barkley & Murphy, 1998). One subscale measures hyperactive/impulsive behaviors with items such as: “Blurted out answers before questions had been completed” and “Felt restless”; whilst the other subscale measures inattentive behaviours with items such as: “Had difficulty sustaining my attention in tasks or fun activities” and “Didn’t listen when spoken to directly.” The scale begins with the instruction to “respond by using the mouse to indicate the answer that best describes your behavior WHEN YOU WERE A CHILD AGE 5 TO 12 YEARS.” Responses were along a 4-point scale ranging from “Never or rarely” (0) to “Very often” (3).
As in Forster and Lavie (2016), childhood symptoms rather than adult symptoms were measured on the grounds that ADHD diagnosis requires symptoms to have started during childhood. Further, childhood symptoms would also be less confounded by any temporary influence of pandemic-related stress/worry on attention (Brown et al., 2022).
Spontaneous and Deliberate Mind Wandering Scales
Deliberate and spontaneous mind wandering were measured through two 4-item scales developed by Carriere et al. (2013). In these scales, spontaneous mind wandering is measured with items such as “It feels like I don’t have control over when my mind wanders”; whilst deliberate mind wandering is measured with items such as “I find mind wandering is a good way to cope with boredom.” The items are clarified with the instruction to respond in relation to “to how your mind wanders, i.e., when your mind is focused on internal thoughts.” Responses are along a 7-point scale ranging from either “rarely”/“not true at all” (1) to “a lot”/“very true” (7).
Dispositional Hyperfocusing Scale
To measure the tendency to hyperfocus, participants completed the 12-item Dispositional Hyperfocusing Subscale from the Hyperfocusing Questionnaire developed by Hupfeld et al. (2019). The dispositional subscale measures the general tendency to hyperfocus across different settings and tasks, and includes items such as: “In general, when I am busy doing something I enjoy or something that I am very focused on, I can feel completely engrossed or fixated on the activity. . .” The responses are along a 6-point Likert scale relating to how often the participant entered a state of hyperfocus, ranging from “Never” (1) to “Daily” (6).
Procedure
Participants in both samples completed the surveys in Inquisit 5 software, which was downloaded onto their home computers. After providing informed consent, participants initially completed a demographic questionnaire measuring their age and gender (“Male,” “Female,” “another gender,” “prefer not to say”). In Study 1a, participants also reported whether English was their first language, and whether they had normal or corrected-to-normal vision. Alongside the key measures analyzed, demonstration versions of visual attention tasks, not calibrated for the experimental setting, were administered at the start of the session for educational purposes (for further information see the pre-registration to Study 2). Participants then completed the attentional trait measures (Study 1a: The childhood ADHD symptom self-report scale; Study 1b: Dispositional hyperfocus scale, and deliberate and spontaneous mind wandering scales), followed by the DIDAS. Finally, participants completed an unpublished 39-item scale in development and still requiring further validation (Brown et al., in preparation).
Statistical analysis
The analysis for Study 1a and 1b were all conducted using JASP software (JASP Team, 2020). To confirm that our novel measure of difficulties with interpersonal distancing reflected a single factor, we used Confirmatory Factor Analysis (CFA) on all items of the DIDAS within both Study 1a and 1b. The single factor’s fit to the data was assessed through traditional fit indices and goodness-of-fit criteria: CFI (>0.95), RMSEA (<0.08), and SRMR (<0.04; Hu & Bentler, 1999). After validating the proposed single-factor structure, we then utilized this measure to assess the prevalence of difficulties with interpersonal distancing. Specifically, we assessed the prevalence that participants reported any level of difficulty with interpersonal distancing, as reflected by scoring above the minimum possible rating (i.e., greater than 1); and the prevalence that participants reported more frequent difficulties, reflected by an average DIDAS score above the mid-line of the scale (i.e., greater than 3).
To test the hypothesis that attentional traits are associated with increased difficulties with interpersonal distancing, we correlated traits linked to inattention with the novel scale. Specifically, in Study 1a we assessed the relationship between the average DIDAS score and reported childhood ADHD symptoms; and in Study 1b we assessed the relationship between average DIDAS score and spontaneous mind wandering, deliberate mind wandering, and hyperfocus.
To further explore the unique contribution of ADHD inattentive traits to the difficulties with interpersonal distancing in Study 1a, we entered both ADHD inattentive and hyperactive/impulsive symptom subscales into a regression model. Similarly, in Study 1b, to explore the independent contribution of mind wandering and hyperfocus to difficulties with interpersonal distancing, we entered both the spontaneous and deliberate mind wandering scales, and dispositional hyperfocus scale scores, as predictors in a regression model.
Results
The analysis for Study 1a and 1b were all conducted using JASP software version 0.14.3 (JASP Team, 2020). All anonymized raw and processed data are available via the OSF: https://osf.io/wsj32/?view_only=e1da5210ed794040b82134409c7d86a5.
Prevalence of Childhood ADHD Symptoms
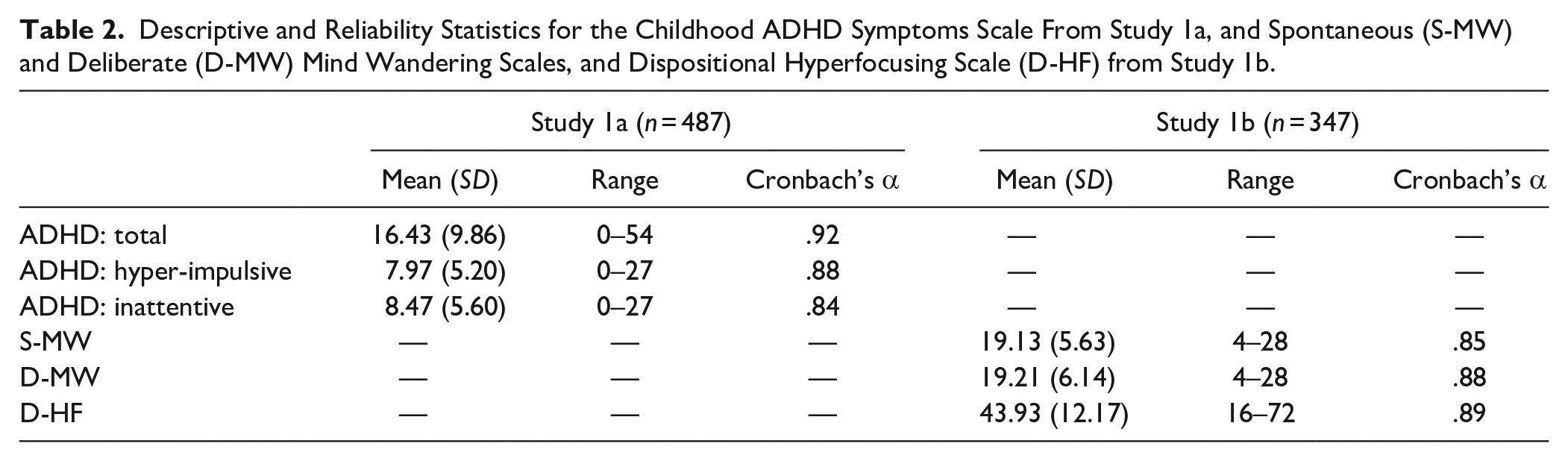
See Table 2 for the overall mean, standard deviation, range of total scores, and internal reliability of the self-reported childhood ADHD symptoms for Study 1a; and of the spontaneous and deliberate mind wandering, and hyperfocusing scale scores for Study 1b. Of those participants who completed the childhood ADHD symptoms scale in Study 1a, 5.54% (n = 27) reported a level of symptoms above the clinically significant threshold for that measure, as indicated by reporting four or more inattentive or hyperactive/impulsive symptoms, or eight or more symptoms overall, occurring “very often” (Barkley, 2011).
Descriptive and Reliability Statistics for the Childhood ADHD Symptoms Scale From Study 1a, and Spontaneous (S-MW) and Deliberate (D-MW) Mind Wandering Scales, and Dispositional Hyperfocusing Scale (D-HF) from Study 1b.
Confirmatory Factor Analysis
Due to the expected single factor structure of the DIDAS and retention of all items, CFA was conducted on both Study 1a and 1b data (see Table 1 for individual item loadings). Across all fit indices derived from the CFA there was evidence that the single factor structure was an acceptable fit to the data with 7-items in Study 1a, Χ2(14) = 60.80, p < .001, CFI = 0.97; RMSEA = 0.08, 90 CI [0.06, 0.11]; SRMR = 0.03 (Hair et al., 1998; 2006), as well as with the full 8-item scale in Study 1b, Χ2(20) = 67.46, p < .001, CFI = 0.96; RMSEA = 0.08, 90 CI [0.06, 0.11]; SRMR = 0.04. Assessment of the scale with Cronbach’s alpha also showed good internal reliability across both Study 1a and 1b (α = .87; see Table 1).
Prevalence of Difficulties With Interpersonal Distancing
In both Study 1a and 1b, the mean DIDAS scores were 2.17 and 2.19, respectively, indicating that, on average, difficulties with interpersonal distancing and awareness were clustered on the lower end (see Table 1 for further descriptive statistics). Examining the distribution of the scores revealed, however, that participants were represented across the full range of the scale from minimum (1) to maximum (5) scores. Importantly, almost all participants reported experiencing some level of difficulty with distancing, with only less than 5% (Study 1a: 4.1%; 1b: 3.5%) of participants reporting never experiencing any difficulties (i.e., scoring exactly 1). A smaller subset reported experiencing relatively frequent difficulties across the DIDAS items, as reflected by the average score being greater than the mid-line of the scale (i.e., greater than 3). Approximately one in six participants fell into this category (Study 1a: 15.81%; Study 1b: 12.68%). The distribution of scores therefore revealed that difficulties with distancing were a common occurrence across the samples, but were experienced more frequently by some participants than others.
Attentional Traits Correlate With Difficulties With Interpersonal Distancing
In both Study 1a and 1b, zero order correlations revealed significant positive relationships between the DIDAS and all inattentive traits (see Table 3, and Figure 1). DIDAS score was positively correlated with both ADHD hyperactive/impulsive and inattentive subscales in Study 1a; and both spontaneous and deliberate mind wandering, as well as dispositional hyperfocus in Study 1b.
Zero-Order Correlations Between the Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS) Score, the Total Childhood ADHD Symptom Score, as Well as the Scores from the ADHD Hyperactive/Impulsive (Hyper-Impulsive) and Inattentive Subscales in Study 1a (n = 487), and Spontaneous (S-MW) and Deliberate (D-MW) Mind Wandering Scales, and Dispositional Hyperfocusing Scale (D-HF) in Study 1b (n = 347).
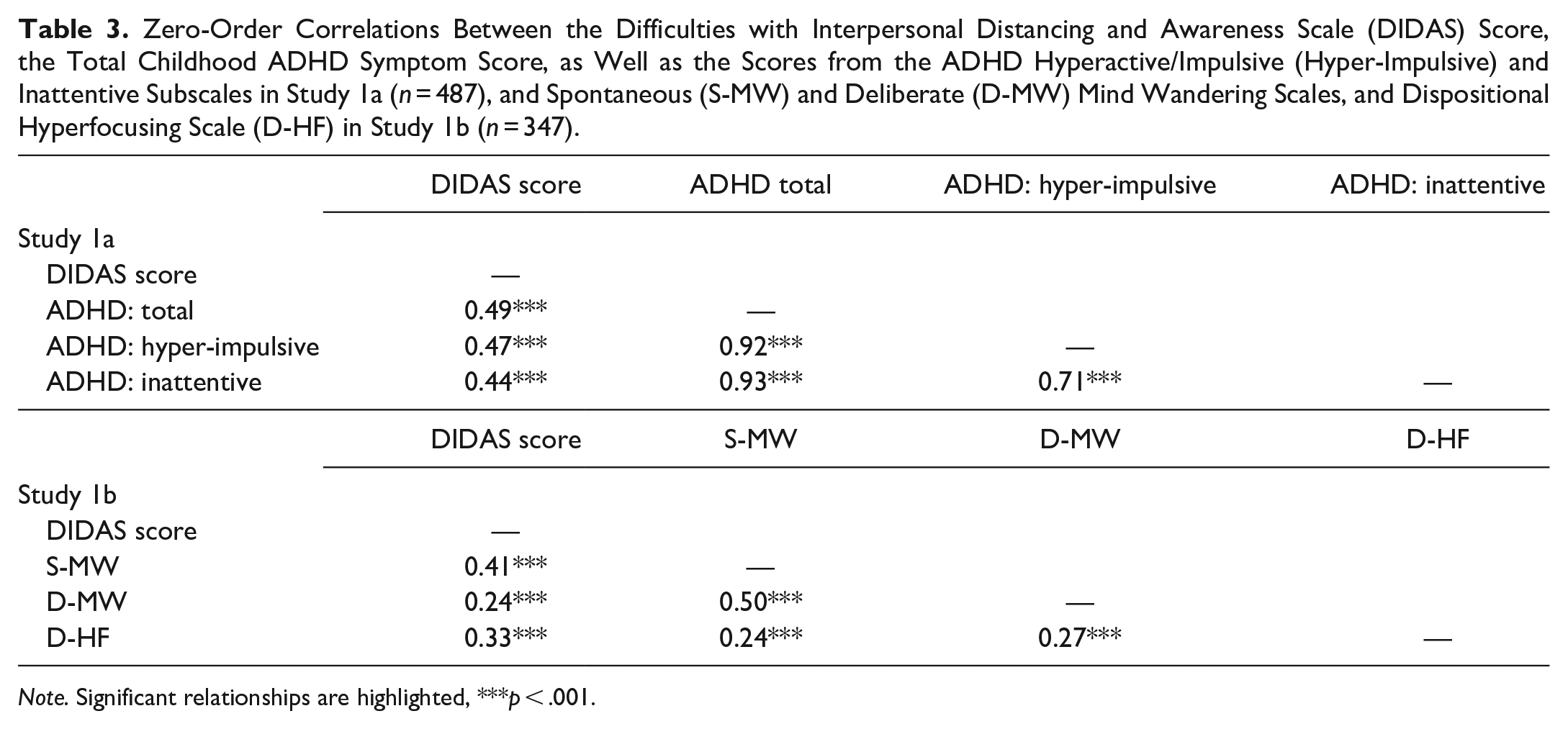
Note. Significant relationships are highlighted, ***p < .001.
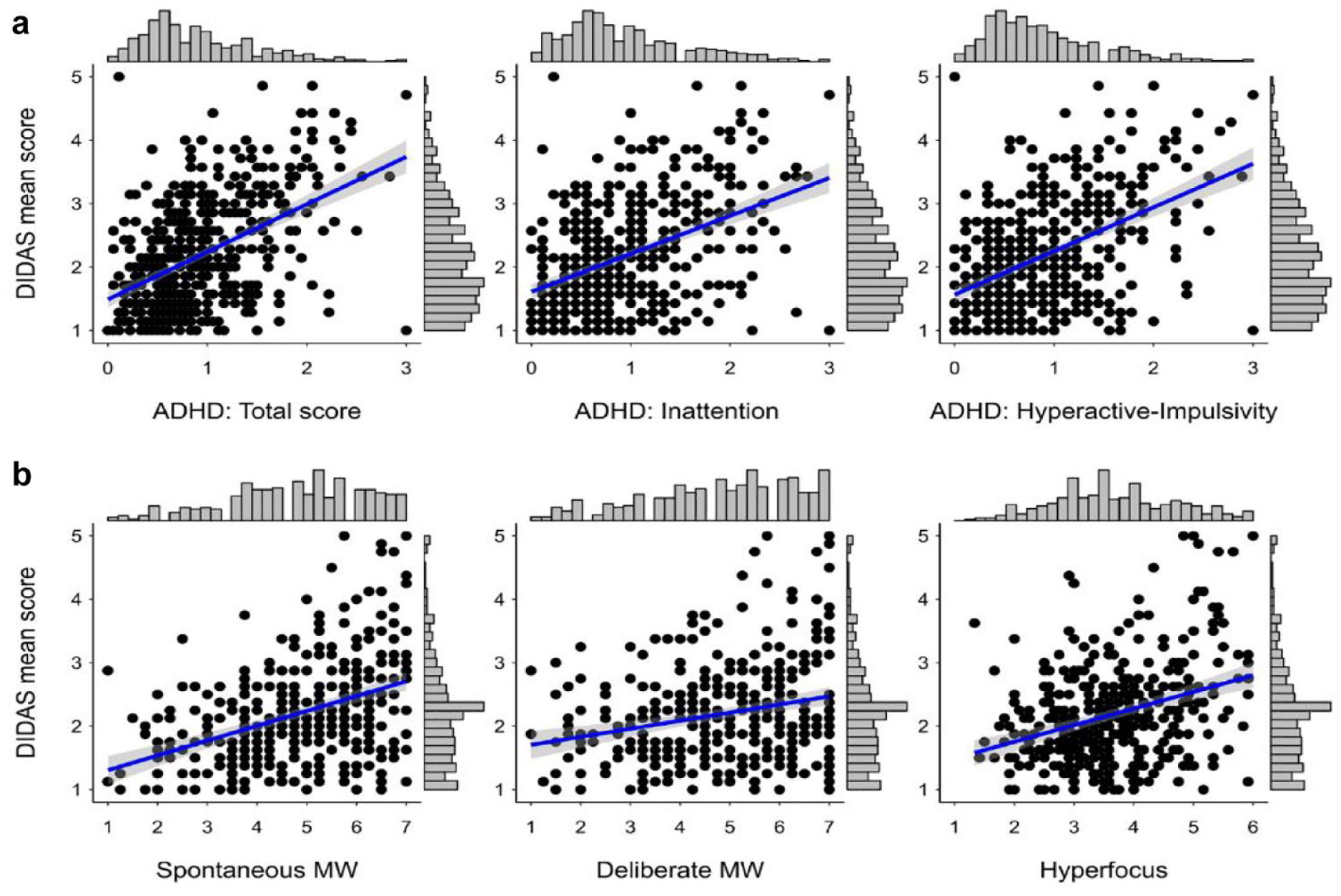
Scatterplot presenting the relationship between the mean self-reported Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS) score and mean self-reported childhood hyperactive/impulsive and inattentive childhood ADHD symptoms in Study 1a (a), and mean Spontaneous and Deliberate Mind Wandering (MW), and Dispositional Hyperfocus scores in Study 1b (b). The regression line is presented with a 95% confidence band. Frequency distributions for each variable are presented on the opposing axis.
In Study 1a, to further explore the unique contribution of ADHD inattentive traits to the difficulties with interpersonal distancing, we entered both ADHD inattentive and hyperactive/impulsive symptom subscales into a regression model. This analysis revealed that both ADHD subscales independently predicted the self-reported lower ability to maintain interpersonally distance, R2 = 0.24, F(2, 484) = 77.41, p < .001. Both the hyperactive/impulsive subscale, β = .32, t = 5.65, p < .001, and 95 CI [0.21, 0.43] and the inattentive subscale, β = .21, t = 3.82, p < .001, and 95 CI [0.10, 0.32], positively correlated with the average DIDAS score.
Similarly, to explore the independent contribution of mind wandering and hyperfocus to difficulties with interpersonal distancing, we entered both the spontaneous and deliberate mind wandering scales, and dispositional hyperfocus scale scores as predictors in a regression model for Study 1b. This revealed a significant overall model predictive of self-reported difficulties with interpersonal distancing, R2 = .22, F(3, 343) = 33.06, p < .001. The individual coefficients revealed that spontaneous mind wandering was a significant predictor of higher DIDAS score, β = .35, t = 6.27, p < .001, and 95 CI [0.34, 0.46], but not the deliberate mind wandering, β < .01, t = 0.07, p = .949, and 95 CI [−0.11, 0.11]. Reported dispositional hyperfocus was also independently related to higher DIDAS score, β = .25, t = 4.93, p < .001, and 95 CI [0.15, 0.34].
Study 2
Study 1 established the novel DIDAS, and using this measure established two key findings: First, more than 95% of people report experience involuntary lapses in interpersonal distancing at least occasionally, with 12% to 15% reporting frequent lapses. Second, approximately 23% of this inter-individual variance was accounted for by attentional traits. Study 2 sought to conduct a pre-registered replication of the findings of Study 1, while further examining the interplay between the attentional traits in predicting difficulty in interpersonal distancing. Given that both mind wandering and hyperfocus are associated with ADHD (Hupfeld et al., 2019; Seli, Smallwood et al., 2015), a key question is the extent to which the relationship between DIDAS and ADHD (as revealed in Study 1a) was mediated by the relationship between DIDAS and mind wandering and/or hyperfocus (Study 1b). As these relationships were demonstrated in separate samples in Study 1, this could not be tested. Study 2 therefore included pre-registered path-analysis testing this question.
Methods
Participants
For Study 2, we pre-registered recruitment strategy, exclusion criteria, all measures, and planned analysis on the OSF https://osf.io/vks47/?view_only=9072bdef9f0148a8a308aa6a9eba2d82). Initially, 436 individuals responded to the survey link as part of a practical class on campus, with 429 individuals providing data beyond initial consent and demographics. Preregistered exclusion criteria (see Study 1a exclusion criteria) were then applied with the addition of the maximum age limit, resulting in a final sample of 399 participants of which 310 identified as “female,” 80 as “male,” and 7 who identified as “another gender,” and 2 who preferred not to answer. The average age of the sample was 20.69 years (SD = 3.44; range = 18–49). The majority of the participants were young adults with 94.49% being below the age of 25 (n = 377). Data collection was conducted in October 2021.
Our sample size was based on the maximum number of participants who could be recruited from this practical class, though we pre-registered a minimum sample size of 300 participants. This would provide the necessary power to detect a significant predictive model where R2 = .05 (F-test power analysis, three predictors, α = .05, β = .90, calculated with G*power; Faul et al., 2009). The sample was therefore well powered to detect the expected effect based on the results of Study 1b (R2 = 0.22).
Materials and procedure
The procedure was similar to Study 1a, however, participants completed Study 2 in a computer laboratory, in practical class groups of approximately 30 to 40 students, using Inquisit 5 software. After providing informed consent, participants completed the childhood ADHD symptoms questionnaire, followed by the DIDAS, hyperfocus questionnaire, and spontaneous and deliberate mind wandering questionnaire in a random order. The testing session also included a demonstration version of a visual attention task for educational purposes only (see pre-registration: https://osf.io/vks47/?view_only=9072bdef9f0148a8a308aa6a9eba2d82).
Statistical analysis
As in Study 1a and 1b, we further tested the single-factor structure of the DIDAS using CFA with all eight items; and assessed the prevalence of participants scoring greater than the minimum value, reflecting any lapses in distancing, and above the mid-point of the scale, reflecting frequent lapses in distancing. The overall pattern of relationships was also explored with zero-order correlations.
As hyperfocus and spontaneous mind wandering are associated with ADHD, our pre-registered hypothesis was that that these variables would mediate the relationship between the capacity to interpersonally distance and childhood ADHD symptoms. Using the Lavaan R package for structural equation modeling (Rosseel, 2012), we therefore ran a pre-registered mediation analysis with the total ADHD score as the predictor and average DIDAS score as the outcome variable in the model. Both the spontaneous mind wandering and dispositional hyperfocus scales were entered as mediators with their non-directional covariance included in the model. As pre-registered, the deliberate mind wandering scale scores were left out of the model due to accounting for no unique variance independent of spontaneous mind wandering in Study 1b.
Additionally, to explore the separate contributions of inattentive and hyperactive/impulsive childhood ADHD symptoms to the DIDAS score, when mediated through dispositional hyperfocus and spontaneous mind wandering, we conducted a pre-registered follow-up mediation analysis with both ADHD subscales (hyperactive/impulsive and inattentive) as independent but covarying predictors.
Results
Prevalence of Childhood ADHD Symptoms
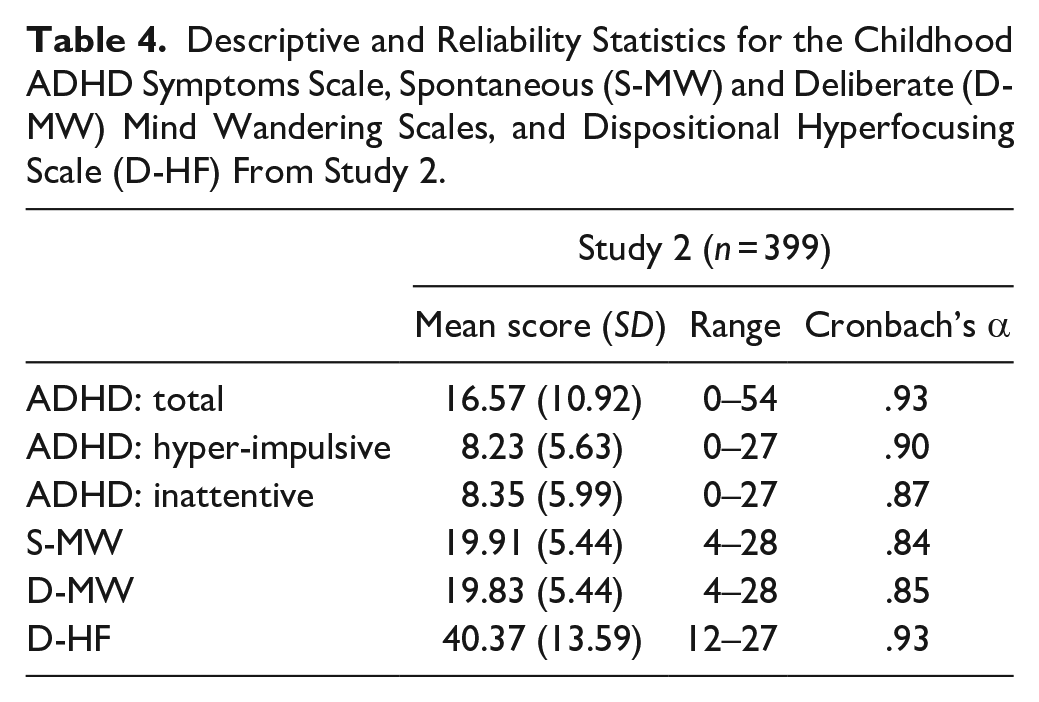
The mean, standard deviation, range of total scores, and internal reliability of the recalled childhood ADHD symptoms scale, mind wandering scales, and hyperfocusing scale scores from Study 2 are reported in Table 4. As in Study 1a, we also assessed the sample for clinically relevant levels of childhood ADHD symptoms, based on the same criteria as Study 1a (Barkley, 2011). This revealed that 6.52% (n = 26) of participants in Study 2 reported symptoms above the clinically relevant threshold.
Descriptive and Reliability Statistics for the Childhood ADHD Symptoms Scale, Spontaneous (S-MW) and Deliberate (D-MW) Mind Wandering Scales, and Dispositional Hyperfocusing Scale (D-HF) From Study 2.
Confirmatory Factor Analysis
Running CFA on the Study 2 data replicated the single factor model, which showed good fit to the data, Χ2(20) = 52.16, p < .001, CFI = 0.98; RMSEA = 0.06, 90 CI [0.04, 0.09]; SRMR = 0.03. Additionally, the model showed good internal validity again (see Table 1 for full analysis). All measures of attentional traits were positively correlated with the reported difficulties with interpersonal distancing, replicating the earlier findings, whilst being positively correlated amongst themselves (see Table 5).
Study 2. Zero-Order Correlations Between the Difficulties with Interpersonal Distancing and Awareness Scale (DIDAS) Score and ADHD Hyperactive/Impulsive (Hyper-Impulsive) and Inattentive Subscales, and the Total of These Scales, Spontaneous (S-MW) and Deliberate Mind Wandering (D-MW), and Dispositional Hyperfocusing Scale (D-HF).
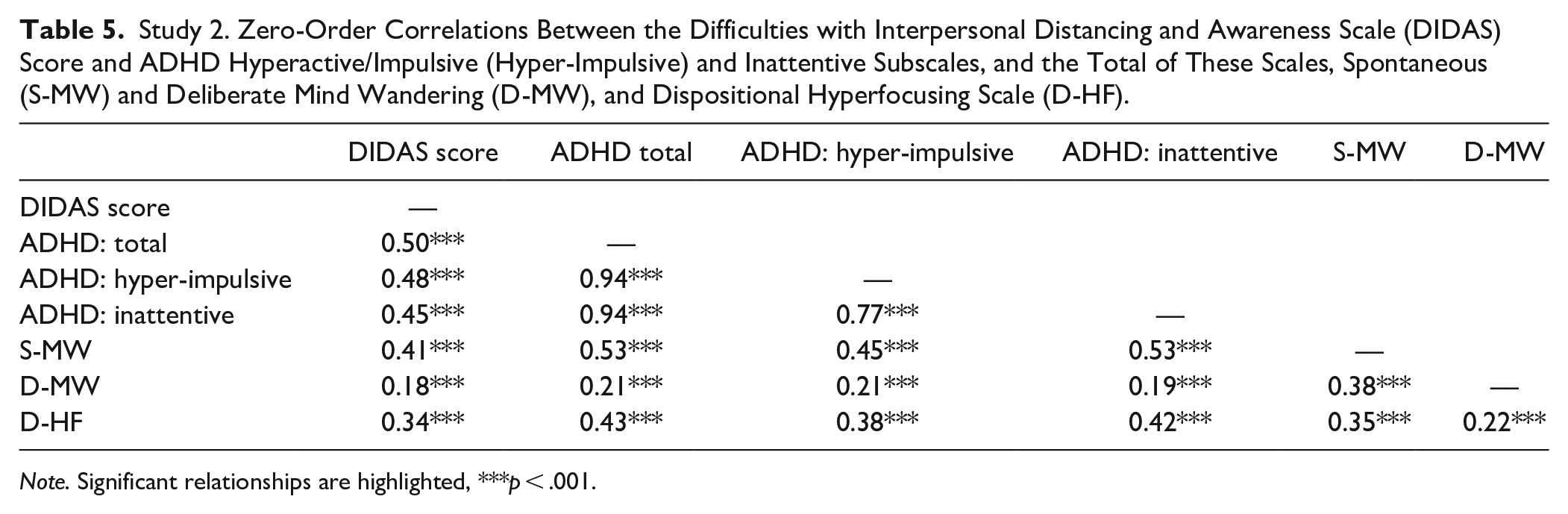
Note. Significant relationships are highlighted, ***p < .001.
Prevalence of Difficulties With Interpersonal Distancing
In Study 2, the mean DIDAS score was 2.33 (SD = 0.82; see Table 1 for further descriptive statistics). Across the sample all participants reported at least some difficulty with interpersonal distancing (i.e., DIDAS score >1), and 20.6% scored above 3, reflecting relatively frequent difficulties.
Mediation Analysis
We first examined the potential mediating role of spontaneous mind wandering and hyperfocus in the relationship between childhood ADHD symptoms and DIDAS. As hyperfocus and spontaneous mind wandering are associated with ADHD, we hypothesized that these variables would mediate the reduced capacity to socially distancing in those with more recalled childhood ADHD symptoms. Using the Lavaan R package for structural equation modeling, we ran a mediation analysis (Rosseel, 2012). We entered the total ADHD score as the predictor and average DIDAS score as the outcome variable in the model. Both the spontaneous mind wandering and dispositional hyperfocus scales were entered as mediators with their non-directional covariance included in the model. As pre-registered, the deliberate mind wandering scale scores were left out of the model due to accounting for no unique variance independent of spontaneous mind wandering in Study 1b.
The overall model accounted for a substantial portion of the variance, R2 = 0.29, in DIDAS score. As hypothesized in our pre-registration, the relationship between ADHD and DIDAS score was indirectly mediated through both spontaneous mind wandering, β = .10, SE = 0.03, Z = 3.48, p = .001, and 95 CI [0.04, 0.15], and dispositional hyperfocus, independently, β = .06, SE = 0.02, Z = 2.67, p = .008, and 95 CI [0.02, 0.10]. This significant pattern reflected ADHD correlating with higher spontaneous mind wandering and dispositional hyperfocus scores, and these independently predicting higher DIDAS score. There was no significant difference in the magnitude of these indirect paths, β = .04, SE = 0.04, Z = 1.07, p = .287, and 95 CI [−0.03, 0.11], with both spontaneous mind wandering and dispositional hyperfocus scale scores being equally strong mediators of ADHD inattention. Interestingly, the total ADHD score remained a significant direct predictor of higher DIDAS score, β = .34, SE = 0.05, Z = 6.59, p < .001, and 95 CI [0.24, 0.45], above the influence of spontaneous mind wandering and hyperfocus. Thus, the results suggest that these attentional traits only partially mediated the influence of overall childhood ADHD symptoms.
To further explore whether this direct relationship reflected the different contributions of inattentive and hyperactive/impulsive ADHD symptoms, we conducted a pre-registered follow-up parallel mediation analysis with both ADHD subscales as independent predictors. Again, the overall model accounted for a substantial portion of the variance, R2 = .30. The path analysis (reported in full in Table 6) revealed that both spontaneous mind wandering and hyperfocus fully mediated the positive relationship between ADHD inattentive symptoms and DIDAS score, with both indirect paths being independently significant. Conversely, the ADHD hyperactive/impulsive symptoms directly correlated with greater difficulties with interpersonal distancing, and neither indirect effect reached significance, p > .095. See Figure 2 for full pattern of significant paths.
The Standardized Coefficients and Standard Error of Coefficients, p-Values, and Upper and Lower Bounds of 95% CI for All Direct and Indirect Paths, Whilst Controlling for All Other Variables in the Model.
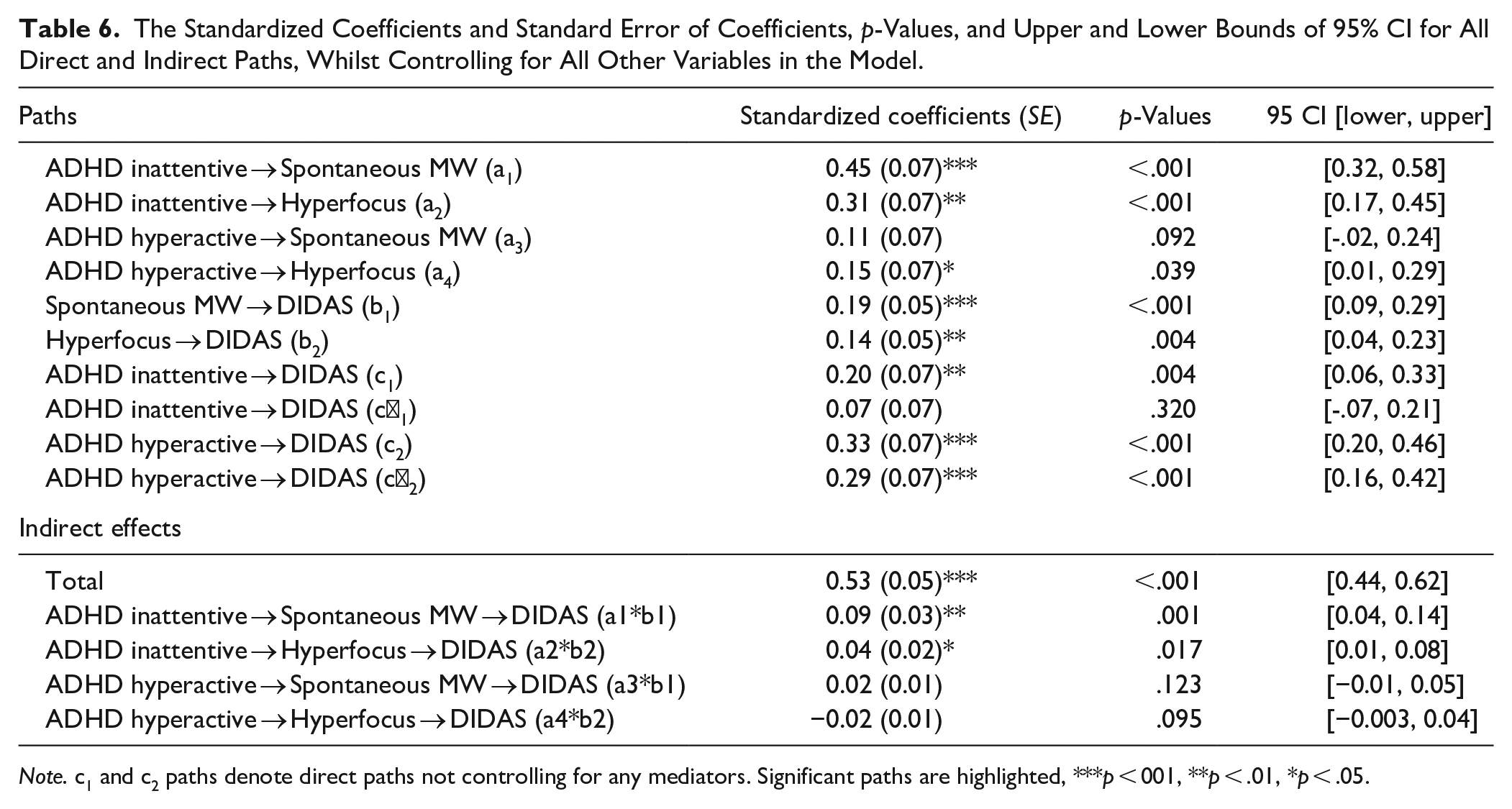
Note. c1 and c2 paths denote direct paths not controlling for any mediators. Significant paths are highlighted, ***p < 001, **p < .01, *p < .05.
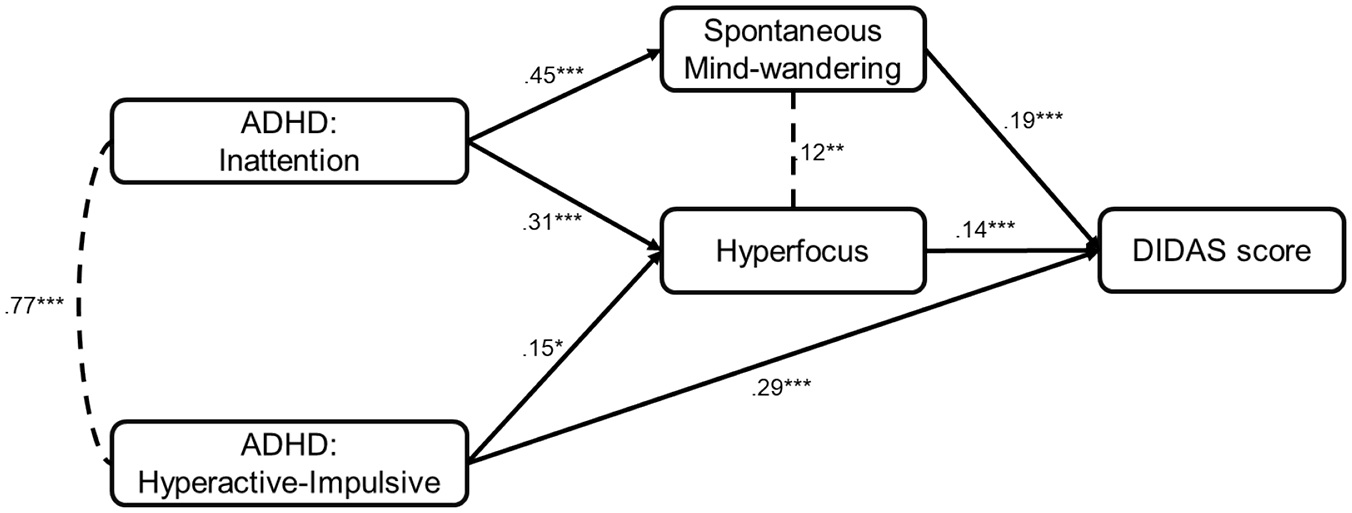
Path analysis model with all significant directional paths (p < .05) highlighted with directional arrows, and covariances presented as dashed non-directional lines. The magnitude of these paths is reported as standardized coefficients. Non-significant paths have been omitted for clarity.
The contrast between the magnitude of the two indirect effects through hyperfocus versus spontaneous mind wandering revealed no significant difference, β = .04, SE = 0.03, Z = 1.38, p = .168, and 95 CI [−0.02, 0.11], with both mediating the positive relationship between ADHD inattentive symptoms and DIDAS score to a similar degree.
General Discussion
Using a new measure, we established the prevalence of involuntary lapses in interpersonal distancing. Across three studies we found that such lapses had been experienced by 97.4% of participants, and approximately one in six participants reported relatively frequent difficulties with distancing. The second key finding was that inattentive traits accounted for 22.4% and 29.51% of the variance in these difficulties across samples. More specifically, we established that a stable and genetically determined attentional trait (childhood ADHD symptomology) strongly predicted the measure of difficulties with interpersonal distancing; and that the positive relationship between ADHD inattentive symptoms and this measure was fully mediated by two distinct inattentive behaviors: spontaneous mind wandering and hyperfocus.
Mind wandering is already well established to involve a decoupling from the external environment, resulting in negative impacts on a range of tasks such as driving or reading (Unsworth & McMillan, 2013; Yanko & Spalek, 2014). Our findings extend this literature by suggesting that mind wandering may also undermine the ability to interpersonally distance. Hyperfocus has received less empirical investigation, but our results raise the possibility that over-allocating attention to external tasks can have a similarly disruptive effect. Taken together with prior evidence, our findings are consistent with the view that operating an ongoing “person radar” during everyday tasks requires attention, and as such may be undermined when attentional capacity is occupied by internal thoughts (i.e., mind wandering) or deeply engaged in external tasks.
By highlighting the involuntary aspects of interpersonal distancing, our data have implications for the effective implementation of public health measures to reduce the transmission of airborne viruses. Specifically, these measures must mitigate potential negative consequences of involuntary lapses in distancing. For instance, structural changes such as increased ventilation would be less effected by lapses. Another consideration is whether attentional demands of interpersonal distancing could potentially detract from the performance of other tasks. While this remains to be directly tested, this possibility cautions that over-reliance on distancing in settings such as workplaces (e.g., hospitals) could potentially come with a performance cost.
Beyond the pandemic, variation in interpersonal distance has been found to influence a wide range of social behaviors, including salesperson persuasiveness (Otterbring et al., 2021), tipping behavior (Jacob & Guéguen, 2012), the emotional reaction to personal space violations (Kennedy et al., 2009), anxiety in social settings (Perry et al., 2015), perceived liking of strangers (Schiffenbauer & Steven Schiavo, 1976), effort in co-operative group tasks (Halberstadt et al., 2016), and crowd safety at large events (Johansson et al., 2008). Our findings raise the possibility that attentional traits might also influence social outcomes and crowd behavior. For instance, by varying the speed and decision making of individual agents to reflect psychological factors (e.g., stress), a recent investigation was able to computationally simulate crowding behaviors during an evacuation scenario (Şahin et al., 2019). Inattentive traits which could disrupt crowd movements could similarly be accounted for when modeling crowd dynamics, which can then inform the design of shared spaces (e.g., airports, schools) to allow for safer crowd movements.
While the present investigation focused on stable attentional traits, both mind wandering and hyperfocus fluctuate across contexts. For instance, mind wandering is heightened under anxiety and stress, or boredom (Danckert & Merrifield, 2018; Seli et al., 2019); whereas self-reported hyperfocus is higher during screen-based activities than other tasks such as academic work (Hupfeld et al., 2019). We therefore predict that temporary increases in these states would predict increased lapses in interpersonal distancing, independent of ADHD inattentive traits.
Future research could test this hypothesis using experimental manipulations of concurrent tasks or states, which would also allow an important causal test of the proposed effects of inattentive states (i.e., mind wandering and hyperfocus) on interpersonal distancing. The latter is particularly important in the light of the present work’s use of a cross-sectional and correlational design, which cannot test causality. Though the current hypothesized model of inattentive traits’ influence on interpersonal distancing is theoretically grounded, this causal assumption still requires empirical confirmation.
Another important step for future research would be to further validate our novel measure—the DIDAS—using objective or other-informant measures. In addition to the standard concerns that apply to any subjective measure, it might specifically be argued that individuals high in inattentive traits would be less aware of lapses in distancing, and hence less able to recall and report them. Though this concern is plausible, prior research has demonstrated that individuals with ADHD may still be accurate at recalling and reporting impairments from ADHD symptoms, as demonstrated by the relatively high correlation between self and other informant reports of impairment in daily life from ADHD symptoms (e.g., r = .68; Barkley et al., 2011). Additionally, the fact that inattentive symptoms were associated with more, rather than fewer, reports of lapses in distancing is inconsistent with this concern; although, it remains possible that any inaccurate reports on our measure could have resulted in the underestimation of an even stronger relationship between ADHD symptoms and difficulty in distancing. A prudent step for future research would be to establish the correlation between self-report and other informant report versions of the DIDAS. In addition, behavioral observation of distancing behavior in a laboratory or real-world setting could be used to provide further objective corroboration of our self-report measure, while also providing a conceptual replication of the proposed relationship between inattentive traits and lapses in distancing.
Though our a priori hypotheses were related to inattentive behaviors, hyperactive/impulsive childhood ADHD symptoms also predicted difficulties with interpersonal distancing. While unexpected, this extends previous evidence by highlighting that impulsivity may influence not only voluntary adherence to public health measures, as previously suggested (e.g., Pollak et al., 2022), but also the capacity to follow such measures. Future research could clarify potential mediators of this relationship; and whether it extends to conditions related or overlapping with ADHD (e.g., sluggish-cognitive-tempo; Barkley, 2014). For instance, motor-coordination or intolerance of delay could be potential mechanisms by which hyperactivity/impulsivity predicts poorer distancing ability (Kaiser et al., 2015; Sjöwall et al., 2013)
An important step for future research will be to test whether the patterns seen here are at the clinical end of the ADHD symptom spectrum. Such a finding would have ramifications for the implementation of population-level public health interventions (e.g., social distancing), which may not only be less effective for some neurodivergent groups, but could unfairly stigmatize these groups for non-adherence. Indeed, difficulty in following public health measures has been proposed as a potential explanation for the higher COVID-19 infection rate in untreated ADHD (Merzon et al., 2021); our findings are compatible with such suggestions. Future research could also consider the potential role of interpersonal distancing in mediating vulnerability to other negative outcomes associated with ADHD (e.g., in social contexts; Kofler et al., 2011). The DIDAS could be adopted for this purpose, especially as this validated measure would allow for efficient data collection compared to resource-intensive observational studies.
It is important to note that the generalizability of our findings is limited by our use of a sample that is lacking diversity in age and level of education and from a “WEIRD” (Western, educated, industrialized, rich, and democratic) society, the latter of which represents only 12% of the global population (see Henrich et al., 2010). As such our results cannot be assumed to generalize more broadly across different age groups (e.g., children or older adults), cultures, or levels of education or socioeconomic status until they are directly established in future research. Although our sample was also biased toward female participants, our large sample size did allow us to conduct a basic exploratory analysis considering the role of gender. Reassuringly, this analysis found no evidence of a difference in DIDAS score between male and female participants, and the same pattern of correlations between inattentive traits and DIDAS score was found in both groups (see Supplemental Materials for full analysis).
In summary, the present investigation highlights, for the first time, the variation in the ability to monitor and maintain interpersonal distance, and reveals its relationship with both inattentive and hyperactive/impulsive childhood ADHD symptoms. Whilst interpersonal distancing is directly relevant to the COVID-19 pandemic, the ability to distance is required for effective everyday functioning. Future research is now needed to assess how limited attentional capacity influences how people navigate social spaces and the real-world consequences of this ability.
Supplemental Material
sj-docx-1-jad-10.1177_10870547221149200 – Supplemental material for Lapses in the Person Radar: ADHD Symptoms Predict Difficulty in Interpersonal Distancing
Supplemental material, sj-docx-1-jad-10.1177_10870547221149200 for Lapses in the Person Radar: ADHD Symptoms Predict Difficulty in Interpersonal Distancing by Chris R. H. Brown and Sophie Forster in Journal of Attention Disorders
Footnotes
Acknowledgements
We would like to thank Rachel Fricker for her assistance generating items for the novel measure of interpersonal distancing and her comments on an earlier version of the draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open Practices Statement
The study materials, data, and scripts for analyses for all studies are publicly accessible via the Open Science Framework (OSF), access code: https://osf.io/wsj32/?view_only=e1da5210ed794040b82134409c7d86a5. Study 1a and 1b were not pre-registered, Study 2 was pre-registered via the OSF, and can be accessed via using the following OSF pre-registration doi: https://osf.io/vks47/?view_only=9072bdef9f0148a8a308aa6a9eba2d82. OSF open data link: https://osf.io/wsj32/?view_only=68501cdc881c49d094bcf9ecbe90291f. Pre-registration OSF doi: ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.