
Abstract
Introduction
ADHD is a neurodevelopmental disorder affecting around 5% of children and 2.5% of adults (American Psychiatric Association [APA], 2013). Individuals with ADHD often show executive function deficits—limiting an individual’s ability to function across a range of tasks and settings requiring the regulation of attention, behavior, and emotion (Barkley, 1997; Graziano & Garcia, 2016; Shaw et al., 2014; Van Cauwenberge et al., 2015). Empirical studies suggest that deficits in inhibitory control (i.e., the ability to suppress pre-potent responses) are significantly associated with ADHD (Willcutt et al., 2005) and support for this view has come from studies using a range of tasks including Stroop (e.g., Liotti et al., 2005), Go/No-Go (e.g., Bluschke et al., 2016) and Stop Signal tasks (e.g., Senderecka et al., 2012).
Around one-quarter of individuals diagnosed with ADHD also meet the diagnostic criteria for an anxiety disorder (Jarrett & Ollendick, 2008). Consistently, in the general population, the symptoms of the two conditions are often correlated (Bowen et al., 2008; Kessler et al., 2006). Anxiety symptoms have also been found to disrupt performance on tasks requiring executive control of attention. In contrast to ADHD, cognitive processing in anxiety is hypothesized to emerge most clearly in the context of perceived or actual internal (i.e., uncontrollable worry) or external threat—typically characterized as an attentional bias for threat (review by Richards et al., 2014). For example, cognitive biases have been demonstrated as enhanced attention toward threat (e.g., Fox et al., 2008), difficulty disengaging attention from threatening stimuli (such as angry faces; e.g., Pavlou et al., 2016) as well as attentional avoidance of threat (i.e., from negative scenes; Koster et al., 2006; Mogg et al., 2004). Further frameworks suggest that anxiety negatively impacts individuals’ processing efficiency on cognitive tasks, such that performance levels similar to non-anxious individuals are only achieved via increased effort or time (Eysenck et al., 2007; Eysenck & Derakshan, 2011). Several studies have found links between reduced efficiency and increased anxiety symptoms in adults, as reflected in slower saccade onsets in an antisaccade task (Hepsomali et al., 2017), as well as greater Contingent Negative Variation (CNV; reflecting greater response preparation) and increased pupillary responses indicating increased effort (Hepsomali et al., 2019).
The shared focus on executive control in theories of ADHD and anxiety—despite their different underlying putative causes and manifestations—raises the important question about how individuals with co-occurring symptoms of ADHD and anxiety will be affected by the emotional content of stimuli presented during tasks. The studies that have explored this issue to date have found inconsistent results. Some studies have shown that, rather than exacerbating executive problems in ADHD, the presence of anxiety counter-acted them—for example, improving performance on response inhibition tasks (e.g., Rodríguez et al., 2014; for a review, see Schatz & Rostain, 2006). Other studies found no impact of anxiety on ADHD inhibitory difficulties (e.g., Vloet et al., 2010). Further research has shown that according to parent and self-reported measures of executive control, comorbid anxiety exacerbated the difficulties in inhibitory control and emotion regulation (i.e., ability to control emotional responses and express emotions) in both children (Sørensen et al., 2011) and adults (Jarrett, 2016) with ADHD.
Few studies have examined attentional processes in ADHD and anxiety in the context of threat-related biases. One study, for example, found that young people with ADHD showed poorer sustained attention and inhibitory control (i.e., increased omission and commission errors in the Conners’ Continuous Performance Test-II and increased errors in a Word-Color Stoop task), relative to young people with anxiety disorders. In contrast, individuals with anxiety disorders showed greater attentional bias toward threatening (angry) faces, as reflected with slower response times and more errors in an emotional probe task (Weissman et al., 2012). These findings support more general attention-related deficits in ADHD and more threat-related attentional biases in anxiety. However, the study by Weissman et al. (2012) did not consider the effects of co-occurred ADHD and anxiety on cognitive performance in the context of threat. The current paper, therefore, extends existing research to explore the impact of social threat on attentional processing and inhibitory control in individuals with elevated symptoms of ADHD, anxiety, and their interactive effect. Attentional biases to threat-related stimuli have been suggested to be critical for the onset and maintenance of psychiatric conditions such as anxiety disorders (Van Bockstaele et al., 2014). Here, we considered dimensional measures of symptoms to capture a wider spectrum of cases within-population sample. This is important both from an educational and public health standpoint as it provides information about disrupted cognitive and emotional processing across a wider population (both young people and adults) who might experience symptoms but not necessarily have a clinical diagnosis.
In this study, we examined the impact of social threat on sustained attention and response inhibition by investigating saccadic eye-movements in an emotional Go/No-Go task in adults and children/adolescents who reported symptoms of anxiety and ADHD that fell within a typical range. 1 In this task, automatic responses are built up during the presentation of Go trials (80% of the trials) and response inhibition is measured during the presentation of No-Go trials (20% of the trials). Go trials require participants to make an eye-movement toward a peripheral target stimulus and No-Go trials to withhold an eye-movement response (i.e., maintain central fixation). Trials varied in their emotional content—with targets either being emotional (happy and angry faces) or non-emotional/neutral stimuli (colored squares). This paradigm provides two indices of sustained attention on Go trials including: (1) task efficiency or saccade onset latency (i.e., time taken to make a correct eye-movement toward a target), and (2) task effectiveness or performance as indicated by attentional lapses (as measured by the absence of a saccade to the target when one is required, i.e., an omission error). This task provides an additional measure of performance as reflected in (3) inhibitory control via the number of incorrect saccades (commission errors) to a target on No-Go trials.
First, we predicted that individuals with elevated levels of ADHD would show generalized deficits in sustained attention and inhibitory control independent of the emotional content of trials (i.e., slower saccade latencies and more attentional lapses via increased omission errors), and more commission errors, indicating difficulty suppressing reflexive saccades to a target. In contrast, we predicted that elevated levels of anxiety would be most associated with threat specific effects on attention and inhibition. In particular, we anticipated that increased anxiety symptoms would be associated with disrupted processing of angry face (vs. happy and non-face) stimuli. Following previous research (e.g., Pavlou et al., 2016) we expected that elevated anxiety would manifest in the current task as slower disengagement, that is, slower saccade onset latencies on angry Go trials and fewer saccadic commission errors in response to centrally presented angry No-Go trials. Finally, we anticipated that elevated levels of anxiety would exacerbate the negative impact of ADHD symptoms on cognitive processing on threat trials (with deficits on all performance indices being most evident for angry compared with happy and non-face cues).
We explored these effects in both children/adolescents and adults, to examine potential age differences. We anticipated that performance would be reflected in increased accuracy (i.e., fewer saccade errors) and efficiency (i.e., shorter saccade onset latency) in adults compared to children. With regards to the individual differences, very few studies have examined age-dependent cognitive performance in ADHD and anxiety. Some studies, for example, found that impulsive behavior in ADHD attenuates with age (Biederman, 2000; Spencer et al., 2007), and since inhibitory control varies with impulsiveness (such that highly impulsive individuals show poorer inhibitory control due to slower information processing), in both clinical (Metin et al., 2013) and non-clinical samples (Logan et al., 1997), we expected that associations between inhibitory control and symptoms of ADHD to be less evident in adults.
Method
Participants
Fifty-four participants, including 27 adults (12 males) aged between 18 and 34 years old (M = 21.44, SD = 3.93) and 27 children and adolescents (12 males) aged between 8 and 15 years old (M = 11.84, SD = 2.22) participated in the current study. The young people who participated in this study were pooled from a larger mixed sample of clinical (i.e., withADHD, anxiety, and co-morbid ADHD/anxiety diagnoses) and community cases of children and adolescents (N = 71; 38 males). Because the focus was on cognitive processing in the non-clinical range we excluded children and adolescents who met the diagnostic criteria (symptom and criterion count) for ADHD (inattention and hyperactivity/impulsivity subscales) or anxiety disorder (specific phobia, social phobia, separation anxiety disorder, panic disorder, generalized anxiety disorder) scales of the Diagnostic Interview Schedule for Children (DISC-IV; Shaffer et al., 2000). We also excluded participants who met the symptom threshold for depressive disorder, oppositional defiant disorder (ODD), and conduct disorder (CD) on the parent-reported Conners Comprehensive Behavior Rating Scale (CBRS-P; Conners, 2008; across both symptom count and standardized T-score 2 ). Exclusion criteria also included taking psychoactive medication and the recognition of severe learning difficulties or special educational needs. Young people were also required to be able to speak and understand English. Young people gave written assent to participate and a parent or legal guardian provided a written consent to participate.
Adult volunteers were recruited via study adverts that were placed around the University campus. Adults undertook a short structured mini neuropsychiatric interview based on the DSM-IV criteria (Mini International Neuropsychiatric Interview, MINI; Sheehan et al., 1998) and were screened for depression, mania, anxiety, obsessive-compulsive disorder, and post-traumatic stress disorder, addiction to drugs and alcohol and strong family history of mood disorder, including panic disorder or panic attacks. No participant met any of these criteria.
Questionnaires
Trait anxiety
We used the State-Trait Anxiety Inventory for children (STAIC; Spielberger, 1973) and adults (STAI; Spielberger et al., 1983) to measure symptoms of trait anxiety. The trait anxiety scale includes 20 items and each item is rated on a 3-point Likert response scale for the child version and a 4-point Likert scale for adults. The scale is based on how individuals “usually feel” (e.g., “I worry too much. . . hardly ever/sometimes/often” (child scale) or “almost never/sometimes/often/almost always” (adult scale) and possible score ranges are 20–60 and 20–80, respectively). Child participant trait anxiety scores ranged from 23 to 46 (M = 32.90, SD = 7.17). Adult participants’ trait anxiety scores ranged from 20 to 48 (M = 33.85, SD = 6.58).
ADHD symptoms
Child and adolescent symptoms of ADHD were measured using the parent-reported Diagnostic Interview Scale for Children—Fourth Edition (DISC-IV; Shaffer et al., 2000). The DISC is a structured diagnostic interview designed to assess psychiatric disorders (based on the Diagnostic and Statistical Manual [DSM-IV], 1994) and symptoms in children and adolescents aged 6–17 years old. Most of the questions are recorded and coded as “yes” (1), “no” (0), “not applicable” (8), or “don’t know” (9). The DISC has moderate to good diagnostic reliability and validity for the parent interview (Schwab-Stone et al., 1996). Test–retest diagnostic reliability of the DISC-parent report for ADHD is 0.60 for and for any anxiety disorder 0.56 (κ-statistics). The ADHD-combined symptom count for young people was taken from both the ADHD-Inattention and Hyperactivity/Impulsivity scales of the DISC-IV, with the potential score ranging between 0 and 23. The total score of the symptoms in the current sample ranged between 0 and 20 (M = 6.10, SD = 6.24).
We used the Current Symptoms Scale (CSS; Barkley & Murphy, 2006) to measure ADHD symptoms in adults. The scale has two sections. The participant filled out the first part and an additional informant, known to the participant (i.e., friend or relative), filled out the second part, 3 in order to reduce self-report bias. The latter was not used for the main analyses. The scale is based on DSM-IV criteria for ADHD and measures the number of symptoms experienced in the last 6 months. It includes 18-items and each asks the participant to endorse a symptom via a four-point Likert scale (never or rarely (0), sometimes (1), often (2), and, very often (3), making a potential score range from 0 to 54). Items are equally divided into inattentive and hyperactive/impulsive subscales. Only items rated as “often” or “more” counted as an indicator of DSM-IV symptom count and included in the total symptom count with scores ranging from 0 to 9 (M = 2.03, SD = 2.79).
Wilcoxon signed ranked tests revealed no group differences (between adults and young people) for both trait anxiety scores (p = .90), and ADHD symptom scores (p = .97).
Experimental Go/No-Go Task
The Go/No-Go task comprised four blocks including two blocks using non-face stimuli (blue and orange squares represented Go and No-Go cues thatwere reversed between two blocks) and two blocks using facial emotional stimuli (happy and angry faces that represented Go and No-Go trials that were reversed between two blocks). Emotional face stimuli were modelled by two (one male and one female) individuals from the NimStim face set (Tottenham et al., 2009). In order to reduce variations between images and prevent unwanted effects of chromatic and differently illuminated images, image pre-processing was carried out using Adobe Photoshop CS6. Images were converted to grayscale, face size was rescaled by keeping a constant aspect ratio for each face, head orientations were adjusted to horizontal plane and centering, hair was removed and intensity was adjusted to obtain images with stable contrast and illumination. Each experimental block consisted of 200 trials (80% Go trials and 20% No-Go trials presented in random order), with each block preceded by 15 practice trials.
In each trial sequence, participants saw an initial presentation of a black fixation cross that appeared at the center of the screen (2,000 ms). This fixation cross was followed by either a Go or a No-Go cue, along with an eccentric target (a white square) that was presented at 8° eccentricity either to the left or to the right of fixation (600 ms). Participants were instructed to look at the central fixation cross until they saw a Go cue, during which they had to move their eyes toward the eccentric white square as quickly as possible and then bring their eyes back to the center after the central fixation cross appeared once more. Participants were also asked to maintain central fixation in the presence of No-Go cues. A randomized inter-trial interval (ITI) of 1,500 to 2,500 ms was added between the initial fixation cross and the target screen. An automatic recalibration was added every 25 trials throughout each block. This was added to minimize data loss due to the continuous presentation of the trial sequences. 4 The colored squares subtended 3 × 3 degrees of visual angle, whereas the targets (white squares) subtended 1.5 × 1.5 degrees of visual angle. The faces subtended 4.2° horizontally and 6.5° vertically (Figure 1).
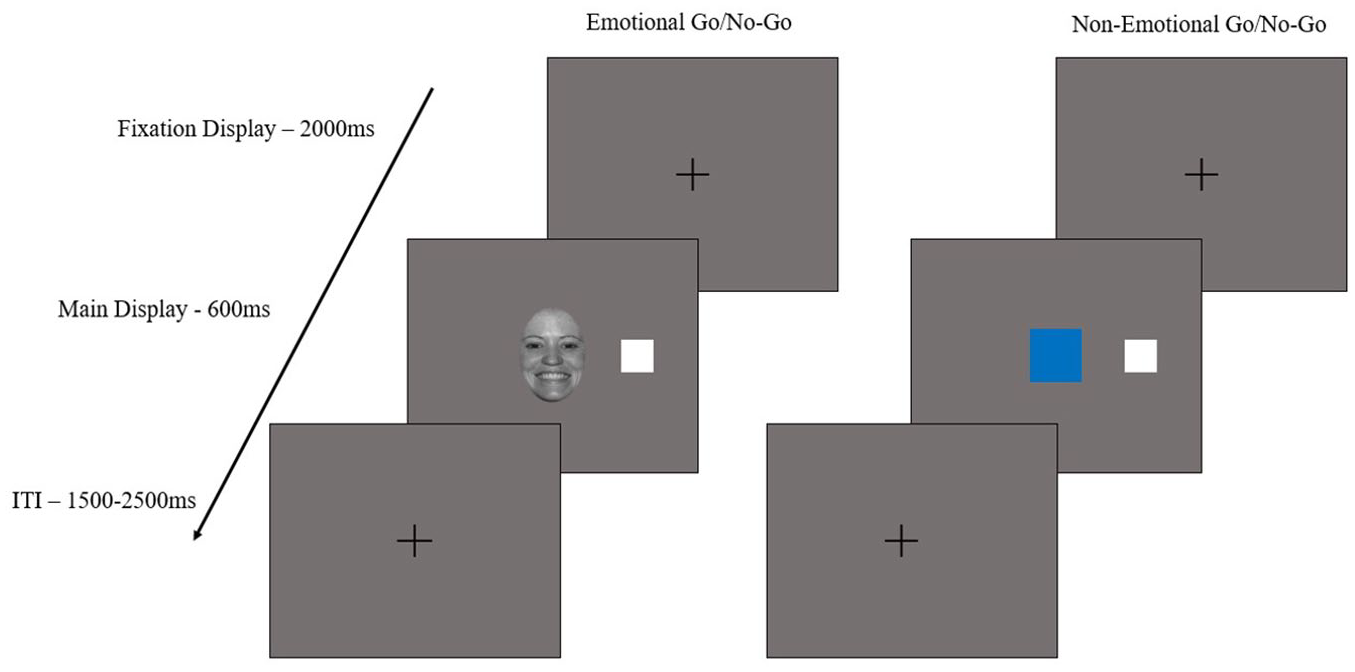
Trial sequence of the Go/No-Go task for face/emotional and non-face/non-emotional stimuli.
Eye movements were recorded using an EyeLink 1000 Plus Desk Mount eye-tracking system (SR Research Ltd) housed in a department research laboratory. The experiments were created and implemented using Experiment Builder software (SR Research Ltd) and presented on a 23-inch monitor (1,920 × 1,080 resolution). Although viewing was binocular, the vertical and horizontal movements of the right eye were sampled monocularly at a rate of 1,000 Hz. The eye-movement data were extracted as saccadic reports using the EyeLink Data Viewer software (SR Research Ltd).
Data Analyses
We performed linear mixed effects models (LMMs) using the lmer function from the lme4 package (Bates et al., 2015) in R (R Development Core Team, 2017) to examine the effects of anxiety and ADHD symptoms and age group (children vs. adults) on saccade onset latency in the presence of emotional and non-emotional stimuli. The saccade onset latency was measured on correct Go trials and it was defined as the time elapsed from the presentation of the Go cue until the first correct saccade landed to the interest area of the target. Saccade latencies below 80 ms were excluded from the dataset (approximately 1% of the data).
We performed generalized linear mixed effects models (gLMMs) using the glmer function from the lme4 package in R to examine the effects of anxiety and ADHD symptoms in saccadic accuracy (saccadic error rates; binary variables: 1 = error, 0 = no error) in the presence of emotional and non-emotional stimuli between children and adults. Saccadic accuracy was considered in relation to (1) omission errors, defined as the number of misses (absence of a saccade when one is required) in the presence of a Go cue, and (2) commission errors, defined as the number of incorrect saccades executed in the presence of a No-Go cue. Analyses revealed a low number of saccadic omission errors (<10%), therefore the results are only reported for saccade latencies and saccadic commission errors.
The participants’ age group (adults vs. children), the cue condition (happy face, angry face, and non-face stimuli), anxiety, and ADHD symptoms (continuous variables) were fixed factors across all the analyses. We considered two- and three-way interactions among ADHD symptoms, anxiety symptoms, cue condition, and age group.
The random effect of the models resolves the non-independence that stems from having multiple responses by the same participant and multiple trials across each experimental block. Therefore, participant and trial number were used as random factors in a maximal random structure including random intercepts and slopes for the cue condition. The models were trimmed in a top–down method until convergence (Barr et al., 2013). In this case, the random structure of the first model was reduced first by removing the correlations, then the interactions between the slopes and then the random effects explaining the least variance until the maximal converging model was identified. The random structure of the final model used for saccade latency and commission errors included different intercepts and slopes for the cue condition for the random effect of participants and trials. The saccade latencies were log-transformed to ensure normal distribution. The continuous variables were mean centered to reduce collinearity between main effects and interactions.
Results
There were significant effects of cue condition (Table 1). Non-face cues elicited shorter saccade latencies and more commission errors, compared to face cues. Angry faces elicited slower saccade latencies (i.e., slower stimulus disengagement) and fewer commission errors (with a marginal effect, p = .08) than happy faces. There was no main effect of sex (p’s > .10). There was a significant effect of age (adults vs. children/adolescents), with adults showing shorter saccade latencies and fewer saccadic commission errors compared to children (Tables 1 and 2).
Estimated Marginal Means (ms) for Saccade Latency and Estimated Marginal Probabilities for Commission Errors in Children and Adults for Each Cue Condition.
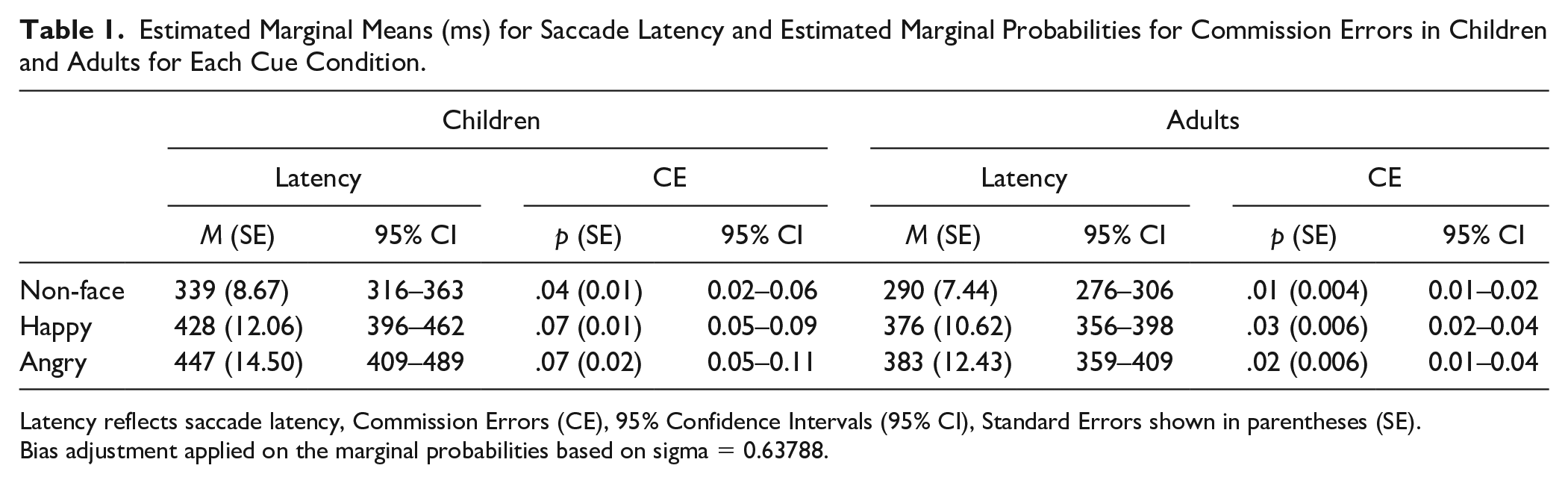
Latency reflects saccade latency, Commission Errors (CE), 95% Confidence Intervals (95% CI), Standard Errors shown in parentheses (SE).
Bias adjustment applied on the marginal probabilities based on sigma = 0.63788.
LMMs of Group, Cue Condition, ADHD and Anxiety, and Interactions on Saccade Latency and GLMMs on Saccade Accuracy of Commission Errors.
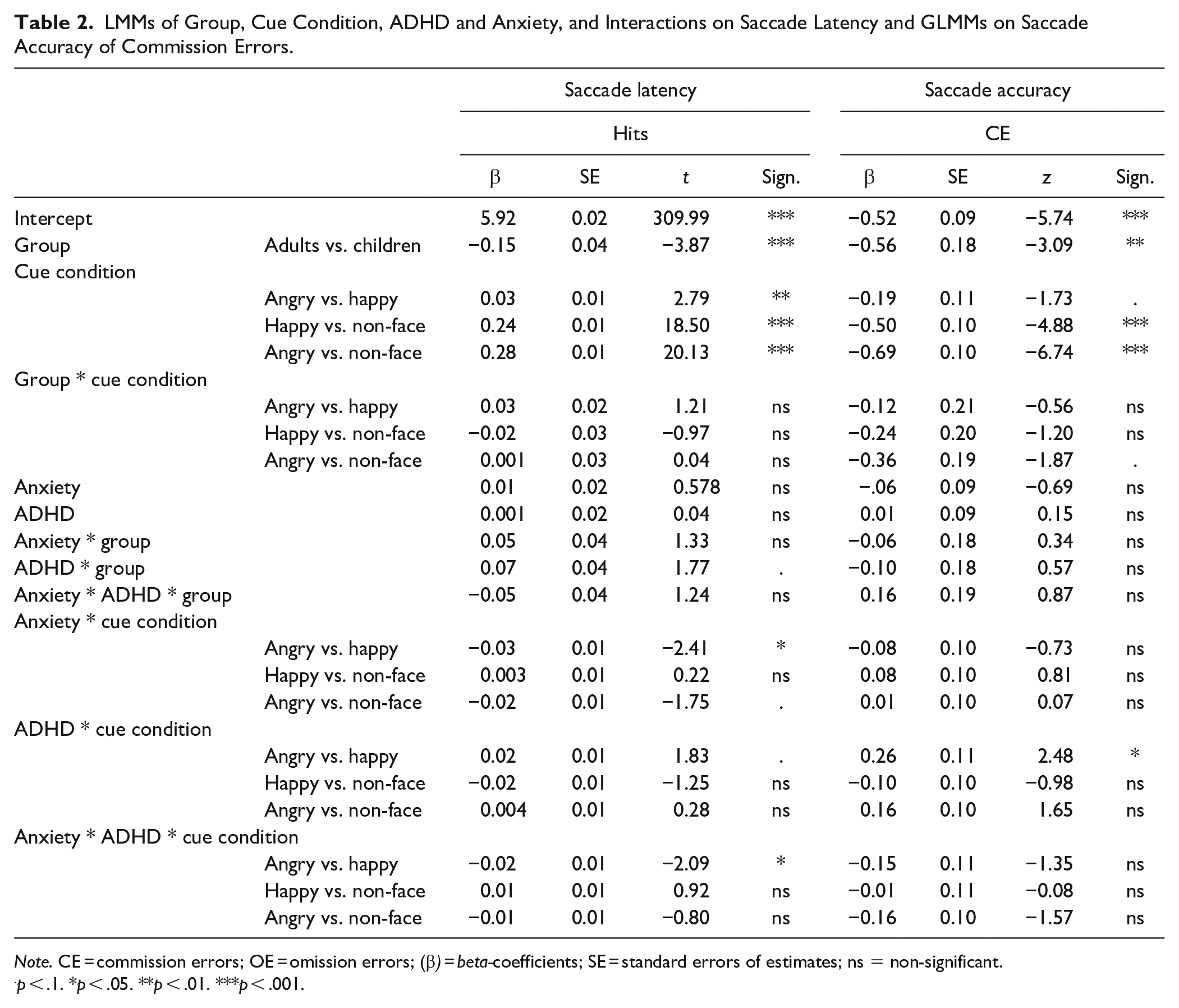
Note. CE = commission errors; OE = omission errors; (β) = beta-coefficients; SE = standard errors of estimates; ns = non-significant.
p < .1. *p < .05. **p < .01. ***p < .001.
Effects of ADHD Symptoms
There was no main effect of ADHD symptoms on either outcome (saccade latency and commission errors). There was no significant two-way interaction between ADHD and age. There was a significant interaction between ADHD and cue condition (Table 1), suggesting that ADHD target processing was disrupted in the context of angry (vs. happy) faces. Individuals with elevated levels of ADHD symptoms made more saccadic commission errors for angry relative to happy faces (No-Go trials; β = 0.26, SE = 0.11, z = −2.48, p < .05; Figure 2). Individuals with elevated ADHD symptoms also showed slower latencies for angry (vs. happy) faces on Go trials—with the effect approaching significance (β = 0.02, SE = 0.01, t = 1.83, p = .07); Figure 3). Contrast comparisons showed no significant interactions between ADHD symptoms and either happy/non-face and angry/non-face stimuli on saccade latency and commission errors (Table 1). There was no significant three-way interaction between ADHD symptoms, age group and cue condition.
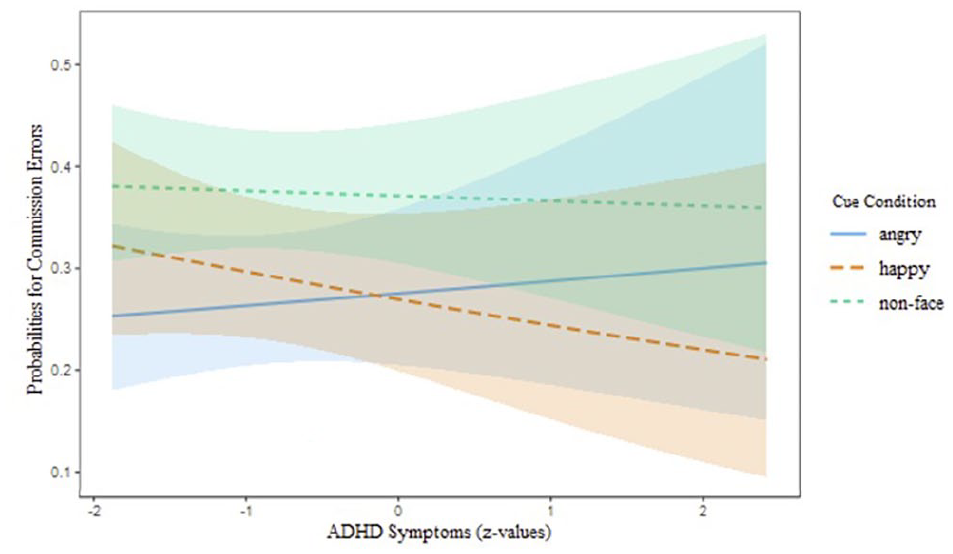
Probabilities for commission errors as a function of ADHD symptoms and cue condition (angry faces, happy faces, and non-face stimuli) on No-Go trials. Shaded bands represent 95% confidence intervals.
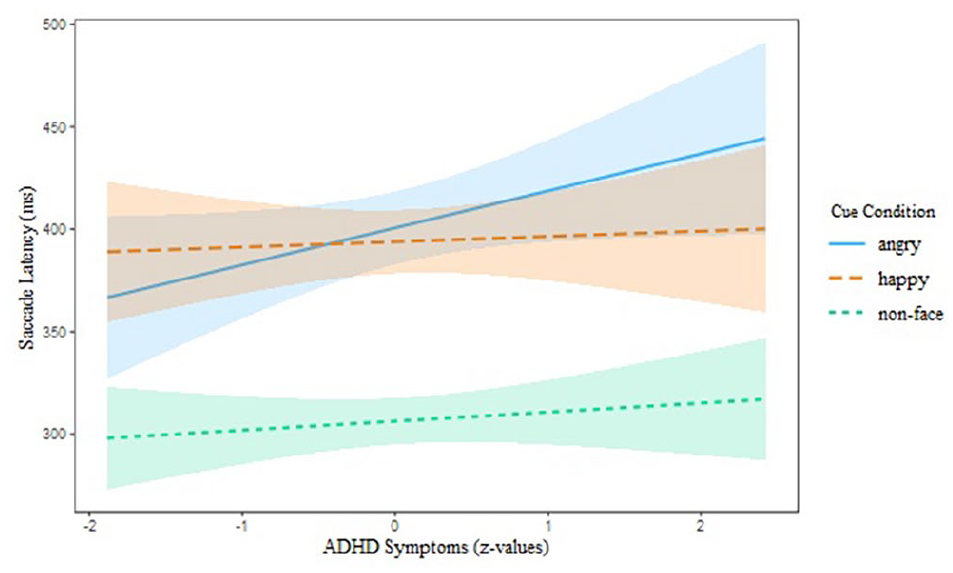
Saccade latency as a function of ADHD symptoms and cue condition (angry faces, happy faces, and non-face stimuli) on Go trials. Shaded bands represent 95% confidence intervals.
Effects of Anxiety Symptoms
There was no significant main effect of anxiety on any index of task performance. There was a significant interaction between anxiety symptoms and cue condition with regards to saccade latency, suggesting that attentional processing was affected by the presence of angry faces. Elevated anxiety levels were associated with shorter saccade latencies for angry face cues compared to happy face cues (β = −0.03, SE = 0.01, t = −2.41, p < .05), but numerically slower saccade latencies when compared to non-face stimuli (this latter effect was not statistically significant, β = −0.02, SE = 0.01, z = −1.75, p = .09); Figure 4).
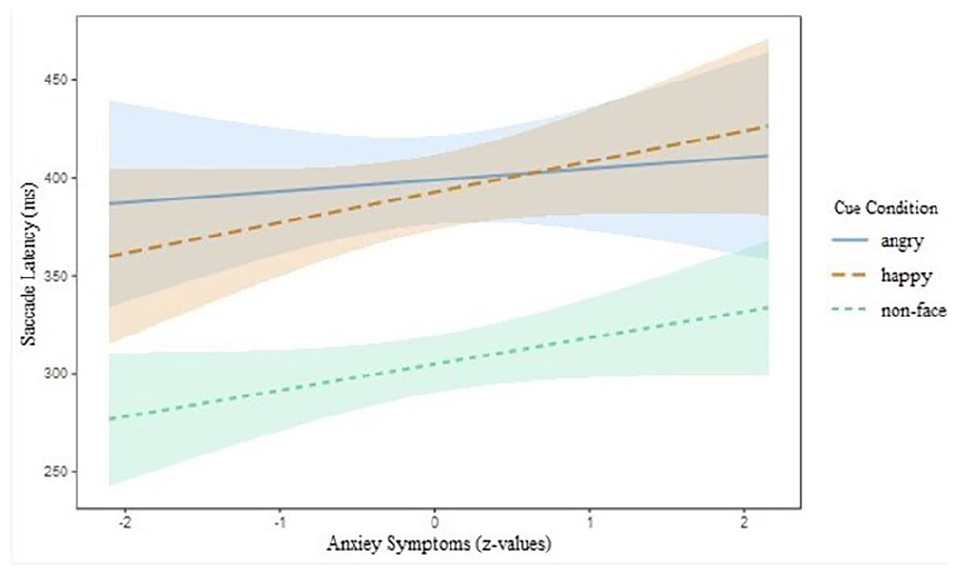
Saccade latency as a function of anxiety and cue condition (angry faces, happy faces, and non-face stimuli) on Go trials. Shaded bands represent 95% confidence intervals.
ADHD × Anxiety Interaction
There were no two-way interactions between anxiety and ADHD symptoms for any outcomes. The results did, however, show a significant three-way interaction between symptoms of ADHD, anxiety and cue condition, indicating that the presence of high levels of anxiety and ADHD symptoms were associated with shorter saccade latencies for angry (vs. happy) face cues, when compared to elevated ADHD and fewer anxiety symptoms (β = −0.02, SE = 0.01, t = −2.09, p < .05; Figure 5). No other effects were significant (Table 1).
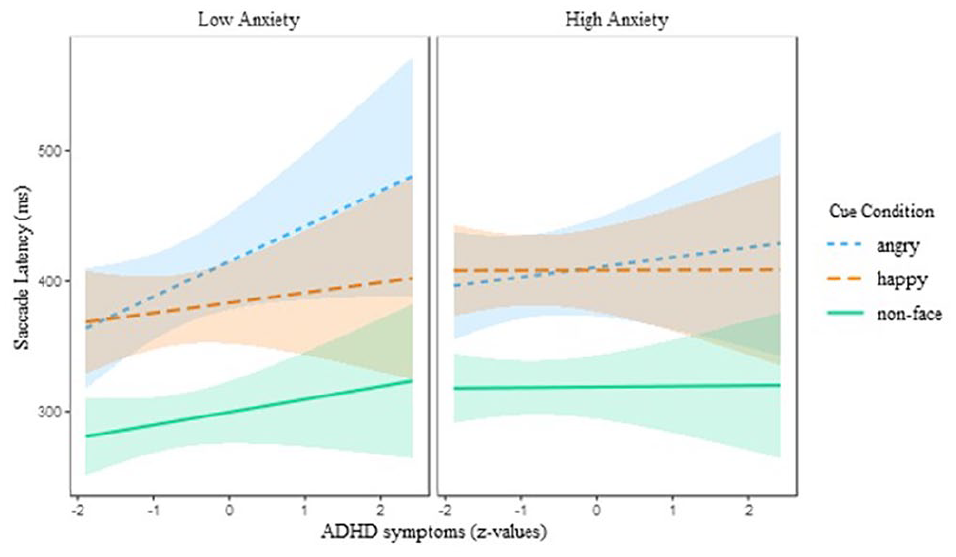
Saccade latency as a function of ADHD, anxiety, and cue condition (angry faces, happy faces, and non-face stimuli) on Go trials. For better visualization anxiety symptoms were divided into low and high groups based on −1 and +1 standard deviation. Shaded bands represent 95% confidence intervals.
Discussion
This study examined the effects of anxiety and ADHD symptoms on sustained attention and inhibitory control in children and adults using emotionally-loaded (happy and angry faces) and non-emotional/non-face stimuli. In general, adults made faster saccades and fewer commission errors compared with children/adolescents. Elevated ADHD symptoms were associated with an increased impairment in inhibitory control (as reflected in more saccadic commission errors for angry faces) and reduced sustained attention (as reflected in slower saccade latencies for angry face cues) when processing threat. In contrast, increased levels of anxiety were associated with shorter saccade latencies in response to angry (vs. happy) face cues. Moreover, when both anxiety and ADHD symptoms were elevated the effect of elevated anxiety symptoms on shorter saccade latency for angry versus happy faces remained, while those associated with symptoms of ADHD were no longer evident.
Individuals who reported increased ADHD symptoms showed reduced ability to suppress reflexive saccades on No-Go trials, specifically in the context of angry (compared to happy) faces. Contrary to our expectations, the results did not support a generalized inhibitory-control deficit for high ADHD. Lowered inhibitory control in response to angry (vs. happy and neutral) faces, has been previously accompanied by reduced right parietal ERP (event-related potential) amplitudes in both children (Kochel et al., 2013) and adults (Köchel et al., 2012) with ADHD, suggesting reduced processing of negative emotional stimuli relative to positive or neutral stimuli. Furthermore, other studies have found reduced ventrolateral prefrontal activation in adolescents with ADHD when negative words were used in an emotional Stroop task, highlighting reduced attentional engagement in the presence of negative stimuli (Passarotti et al., 2010a). Further studies have found that children with ADHD showed reduced prefrontal activity (i.e., in ventrolateral, orbitofrontal, and medial prefrontal cortices) when angry (vs. neutral) faces were used in a 2-back working memory task and increased prefrontal activity in the presence of happy (vs. neutral) faces when compared to healthy controls (Passarotti et al., 2010b). Together these findings support the claim that executive function difficulties in ADHD are modulated by the emotional valence of the stimuli. The current study showed similar findings with regards to disrupted inhibitory control in ADHD that were evident specifically in the presence of negative compared to positive emotional faces.
In the current study, disrupted performance to angry faces in individuals with higher ADHD was also supported by less efficient processing (i.e., slower saccade latencies) in response to angry (vs. happy) face cues. Interestingly, this effect suggests that increased ADHD symptoms were associated with difficulties disengaging from angry faces (slowing a required response to move the eyes away from an angry face). In support, disrupted processing of angry (but not happy) faces in ADHD were previously shown with reduced hemodynamic response during recognition of angry faces and typical (increased) response during recognition of happy faces (Ichikawa et al., 2014). Other studies, have also shown that challenges with emotion identification in ADHD are specific to negative stimuli (including anger, sadness, and fear; e.g., Pelc et al., 2006; Singh et al., 1998; Williams et al., 2008). Recent functional imaging evidence showed hyperresponsivity in the dorsal and ventral anterior cingulate cortex during passive viewing of negative (vs. neutral) pictures in adults with ADHD compared with typical controls (Materna et al., 2019). These findings support a differential implicit processing of negative emotional stimuli in ADHD. Hyperactivation in limbic and paralimbic brain regions was also found in other psychiatric conditions such as autism and associated with atypical emotional-face processing (Aoki et al., 2015). Overall, the current findings support a threat-specific attentional and inhibitory control disruption in high ADHD found also in previous research.
Angry faces impacted attentional processing in individuals with elevated levels of anxiety in a different way to that of ADHD. Increased anxiety was associated with shorter saccade latencies for angry relative to happy facial expressions. In this study, faces were central to task goals and behavior. Previous evidence has shown that threatening stimuli presented peripherally capture attention, as reflected in faster response times (see the review by Cisler & Koster, 2010), in individuals who reported high trait anxiety (Bradley et al., 2000) and those diagnosed with clinical anxiety (Chen et al., 2002). Further studies have suggested that over extended periods, anxiety is linked to increased avoidance of threatening stimuli (Mogg et al., 2004). Other studies have also shown that anxiety is associated with attentional disengagement difficulties in relation to negative stimuli in children and adults (Ladouceur et al., 2009; Pavlou et al., 2016; Richards et al., 2012). However, in these studies, all threatening stimuli acted as distractors and were irrelevant to the task goals, suggesting that the mixed findings across studies related to threat-related attentional biases in anxiety, may be attributed to the different task requirements and methodological manipulations (i.e., task-relevant and irrelevant stimuli and presentation duration of stimuli). Future studies should consider investigating task-relevant compared to task-irrelevant stimuli on emotional processing, to allow the disentanglement of attentional engagement and disengagement processes in anxiety research.
Our results showed that the presence of increased anxiety symptoms in ADHD did not impact the number of inhibitory control errors (i.e., the absence of an interactive effect), but counteracted the effects of ADHD on sustained attention in the emotional context. In other words, the slower processing to move attention away from angry faces in ADHD was no longer evident when both anxiety and ADHD symptoms were elevated. The former finding was supported by previous studies that examined inhibitory control using symbolic stimuli and found that anxiety symptoms had no impact on ADHD inhibitory difficulties (e.g., Vloet et al., 2010). This finding, however, contradicts other studies showing that the presence of anxiety in ADHD was associated with improved response inhibition in ADHD (e.g., Manassis et al., 2000; Rodríguez et al., 2014). More recently, a meta-analysis has found that clinical anxiety did not have a negative impact on attention and working memory and improved response inhibition in children with ADHD (Maric et al., 2018), highlighting that anxiety attenuates executive function deficits associated with ADHD. However, these findings were only focused on tasks using emotionally neutral stimuli. In the current study, the counteracting effects of anxiety on sustained attention in ADHD were specific to emotional stimuli. Previous evidence has shown a similar effect, with anxiety moderating impairments in emotion recognition in children with comorbid conduct disorder (CD; Short et al., 2016). In this study, Short et al. (2016) examined emotion recognition of anger, fear, happiness, sadness, and disgust using a five-alternative-forced-choice task in adolescents diagnosed with CD, anxiety, comorbid CD/anxiety, and typical controls. The results showed that young people with CD showed larger impairments in the recognition of fear, anger, and disgust, whereas young people with anxiety did not differ from controls. Emotion recognition (across all emotions) of comorbid CD/anxiety was similar to that of the control group, suggesting that emotion processing in anxiety counteracted the impairments associated with CD. Consistently, the findings from the current study support that rather than exacerbating, the effects of anxiety on emotional processing counteracted those of ADHD. Previous studies found that ADHD and CD share neuropsychological impairments including slower inhibitory responses and increased reaction variability (Hobson et al., 2011; Oosterlaan et al., 1998) as well as common functional responses in the neural networks mediating interference inhibition and attention allocation (Rubia et al., 2009). More recently, theoretical frameworks suggested that individuals with ADHD and CD share dimensional traits of emotion dysregulation (Petrovic & Castellanos, 2016).
In summary, the current study used saccadic eye-movement measurements to examine the synergistic effects of ADHD and anxiety symptoms on inhibitory control and sustained attention for processing emotional and non-emotional (symbolic) stimuli. The results showed that cognitive deficits associated with elevated ADHD symptoms were specific to the emotional content of the stimuli, thus not supporting more generalized attention deficits. ADHD symptoms were associated with reduced inhibitory control and less efficient sustained attention in response to angry (compared with happy faces). In contrast, increased anxiety symptoms were linked to faster processing of angry face relative to happy face cues. The interaction between ADHD and anxiety showed that the effect of anxiety symptoms prevailed over those associated with ADHD, indicating a reduction of the effect of ADHD symptoms on sustained attention and inhibitory control during the processing of threat stimuli. The current findings might likely stimulate future research to further investigate the interaction between cognition and emotion across a wider spectrum of ADHD and anxiety symptoms including clinical levels.
This research enables the disentanglement of the psychological challenges associated with ADHD from those underpinning comorbid disorders (i.e., anxiety) and has implications on interventional approaches related to attentional training and threat biases. For example, emerging evidence on attentional training and especially those focusing on bias modifications (ABM; attention bias modification), aim to reduce clinical symptoms (i.e., of anxiety) by reducing negative attentional biases through attention training that involves processes such as orienting attention away from threatening or toward non-threatening stimuli (e.g., Mogg & Bradley, 2016, 2018). This interventional approach has been mainly adapted for anxiety, but evidence from meta-analytic data showed only small effect sizes (Mogoaşe et al., 2014). Related theoretical frameworks have suggested that future studies should consider methodological approaches related to cognitive control training that is focused attention-search for positive/nonthreat information rather than threat avoidance. The effects of individual characteristics of anxiety should also consider comorbid symptoms and their severity (Mogg & Bradley, 2016). Our findings suggest that the ABM approach could be extended to individuals with elevated ADHD symptoms with and without anxiety that was found to be associated with attentional disruptions specific to threat contexts.
Footnotes
Acknowledgements
The study was undertaken at the Centre for Innovation in Mental Health-Developmental Laboratory and the Centre for Vision and Cognition, at the University of Southampton. We would like to thank all the participants and their families that kindly volunteered in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by the University of Southampton’s Vice Chancellor Scholarship and the Solent NHS Trust.