
Abstract
This is now Thibault, Veissière, Olson, and Raz’s (2018) eighth publication making the same argument based on the consistent finding of no separation on any outcome measure when comparing so-called “genuine” neurofeedback (NFB) and sham feedback in sham-controlled trials (e.g., Thibault & Raz, 2017). The authors therefore assert that NFB operates as a placebo, all be it a powerful one, with effects commonly equivalent to optimized versions of established ADHD treatments (e.g., Pigott, 2017). In their current effort, the authors provide guidance how clinicians can ethically prescribe NFB “as a form of neurosuggestion therapy” (Thibault et al., 2018, p. 2). Our Guest Editorial deconstructs these sham-controlled studies demonstrating the fallacies of the authors’ argument. We also examine the evidence supporting neurosuggestion as a therapeutic intervention as well as that supporting NFB’s specificity, sustainability, and effectiveness when compared with stimulant medication (SM). Finally, we question why prescribe NFB as a placebo when with proper training clinicians can provide operant conditioning of the electroencephalogram (EEG) with proven sustained effects.
Learning Methodology Matters
Table 1 summarizes the methodology and findings from six sham-controlled trials treating ADHD. Although each study acknowledged NFB is based on operant learning, their methodology violated established learning science by using either automated or manually adjusted EEG reward thresholds to maintain an “about 80%” level of reward across sessions and subjects. This procedure is contrary to basic learning principles. First, operant conditioning targets a response followed by a stimulus-event to make the desired response occur more or less frequently and then plots the target response’s occurrence over time to document whether or not learning has occurred. In these studies, the target response was not consistently calculated, monitored, plotted, and presented to NFB subjects. Therefore, it is not known what response (if any) was conditioned. Second, the studies do not reference the effects of practice in the experimental process. Subjects in both groups engaged in the same set of behaviors during sessions (e.g., maintaining stillness and focus, reducing muscle and eye-movement artifacts, relaxation, posture, and breathing). If subjects did not engage in these practiced behaviors, their EEG data were riddled with artifact and worthless. Third, operant conditioning of the EEG requires that these core concepts are strictly adhered to demonstrating the operant behavior has been learned and such documentation of learning should occur before examining outcome measures of interest (Cannon, 2015).
Sham-Controlled NFB Studies.
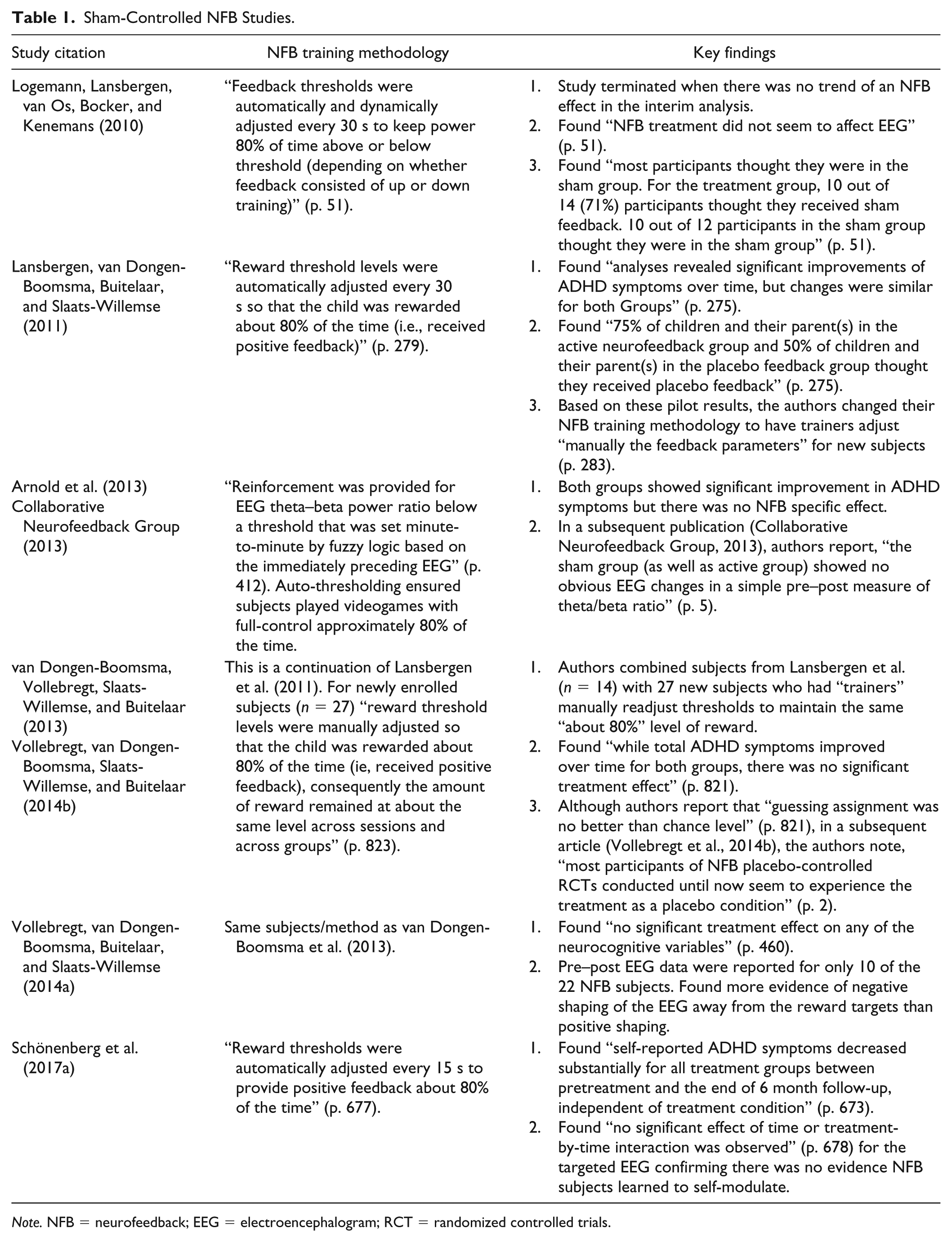
Note. NFB = neurofeedback; EEG = electroencephalogram; RCT = randomized controlled trials.
In these studies, every reset of the EEG reward threshold delivered operant consequences to subjects’ brains antithetical to the goal of training. As Pigott and colleagues (2017) note if the targeted EEG was strengthening, reinforcement was withdrawn and reset down to 80% thereby punishing participants for learning to self-modulate. Conversely, if the targeted EEG was decreasing, participants were reinforced up to 80% thereby rewarding them for decreasing its strength. (p. 897)
At every reset of the reward threshold, NFB subjects therefore were either rewarded for not learning to self-modulate the targeted EEG or administered a Type 2 punishment for the beginnings of success.
Given their flawed methodology, it is not surprising that all six studies found:
No evidence NFB subjects learned to self-modulate the targeted EEG;
No separation between NFB and sham feedback on any outcome measure; and
When assessed, the vast majority (71% to 75%) of NFB subjects thought they received sham-feedback—correctly determining the NFB they received was often false.
Intriguingly, four of the studies also found significant improvement in both groups, leading Thibault and colleagues among many others to argue that these beneficial effects are due to placebo phenomena versus any specific effects from NFB. Two points in response below:
First, flawed methodology prevented NFB subjects from learning to self-modulate the targeted EEG and therefore no specific effects should be expected since each study compared two forms of false-feedback. Second, both groups participated in an active intervention. Ninaus and colleagues (2013) found multiple cortical regions of the brain are activated when blinded subjects were told to focus and try to control randomly moving bars during five 20-s rounds. In contrast, no such changes occurred when subjects were instructed to merely watch the moving bars. Subjects in sham-controlled trials are commonly instructed to sit still, focus, and use their brains to increase positive feedback. Similar cortical regions therefore likely underwent a vigorous workout during subjects’ 30+ sessions sitting still and trying to control that which was uncontrollable. This is hardly a “placebo” intervention as traditionally understood and likely only had positive effects because subjects were deceived into believing they had a 50% chance of receiving accurate EEG feedback. Transparency eliminated the brain activation found by Ninaus et al. as it likely would in all false-feedback trials.
Thibault and colleagues’ (2018) claim that NFB is a placebo is not supported by the referenced data. Their referenced studies compared two forms of false-feedback—not operant conditioning of the EEG. NFB has a 75+ year history of scientific inquiry documenting operant conditioning of the EEG in cats (e.g., Wyrwicka & Sterman, 1968), primates (e.g., Schafer & Moore, 2011), and people (e.g., Jasper & Shagass, 1941), including a 40-year history of research treating ADHD children (Lubar & Shouse, 1976; Shouse & Lubar, 1979). The authors though dismiss this extensive research history asserting that “Following the results from recent double-blind studies, we can now add EEG-nf for ADHD to this list of placebo therapies that masquerade under other biomedical labels” (p. 2). In contrast, it is our assessment that it is these double-blind studies themselves that are the masquerade since they did not compare operant conditioning of the EEG with a sham-control but rather two forms of false-feedback.
Bad Science Begets More Bad Science
In their introductions, each of these sham-controlled studies states something similar to “neurofeedback is based on the assumption that deviant brain activity patterns can be voluntarily modulated by operant learning strategies” (Schönenberg et al., 2017a, p. 674) and yet then used a methodology antithetical to operant learning. When we challenged Schönenberg and colleagues to either “acknowledge that their neurofeedback methodology violates the very essence of operant conditioning or explain the errors in our analysis” (Pigott et al., 2017, p. 897), these authors stated that they used a “previously established protocol” (Schönenberg et al., 2017b, p. 897) and then made additional points unrelated to our analysis.
This is the problem. Bad science begets more bad science until it is corrected. Each of these studies cited one or more of their predecessors and appears more focused on single/double/triple blinding and empirical rigor than ensuring competence in administering the independent variable, in this case operant conditioning of the EEG. True scientific rigor demands a higher level of adherence to learning principles when evaluating treatments based on operant conditioning.
Unfortunately, the impact factors of the journals publishing these six studies ranged from 2.5 to 11.6 placing them in the mid-to-top tier of behavioral health journals. These studies therefore have had a nefarious impact on the scientific literature as they are highly cited in research and review articles, meta-analyses, editorials, and authoritative practice guidelines (e.g., AACAP, 2011) as well as by insurance companies when denying coverage since these studies are presumed to demonstrate that NFB has no specific effects when rigorously evaluated and therefore does not meet evidence-based treatment standards. This contaminated scientific literature has harmed the public by limiting access to a treatment with a long history of using operant conditioning to improve lives by teaching children and adults how to self-modulate targeted neuronal activity.
Neurosuggestion, Specificity, and Comparative Effectiveness
Thibault and colleagues (2018) argue it is the efficacy of suggestion and the placebo effect that drives behavioral change from NFB—nothing specific to NFB itself—and if transparent, clinicians can ethically prescribe NFB as a placebo treatment “with an eye for amplifying the psychosocial mechanisms of suggestion rather than grasping at the elusive neural signatures many practitioners speciously assign as the cause of ADHD” (p. 709). To buttress their argument, the authors cite an unpublished, uncontrolled, open-label feasibility study they presented at a hypnosis conference (Veissière, Olson, & Raz, 2017). In this study, the authors used a decommissioned magnetic resonance imaging (MRI) machine as a prop with nine ADHD children. They told the children it was an inactive “brain machine” and the authors would “use it as a suggestion” to “help their brain heal itself.” While in the MRI, the authors “gave the children positive verbal suggestions to promote relaxation, focus, and confidence.” They report that in follow-up interviews, parents of two children “reported near complete remission of symptoms, and six reported improvements in areas such as confidence, self-control, and social skills” (p. 709) The authors then claim that “In essence, this study provided neurofeedback-like treatment, but instead of focusing on a specific physiological mechanism, we emphasized suggestion-based healing” (Thibault et al., 2018, p. 708, 709). Four points in response below:
First, besides the inherent potential for multiple biases in an unpublished, uncontrolled, open-label hypnosis study, we have no evidence of functional deficits or improvements in ADHD symptoms using standardized measures for such deficits in the children themselves. Instead, just post-treatment “qualitative” interviews conducted by the authors with the children’s parents of domains unrelated to ADHD’s core symptoms (e.g., “confidence, self-control, and social skills”). Furthermore, we have no data indicating the diagnoses were correct. One would assume an accurate differential diagnosis was conducted at some point in these children’s evaluation procedures; however, this is not clear given the lack of information available. Finally, this is a hypnosis feasibility study using an MRI machine as a prop, not “neurofeedback-like treatment.” It is hard to see how this study provides anything more than anecdotal support for a new experimental treatment.
Second, Thibault and colleagues ignore the evidence suggestive of NFB’s specificity and effectiveness in treating the “neural signatures” of ADHD. For example, in their double-blinded within-subject reversal design studies, Lubar and Shouse (Lubar & Shouse, 1976; Shouse & Lubar, 1979) demonstrated both (a) the functional relationship between the sensory motor rhythm (SMR) and manifestation of hyperkinetic behaviors and (b) that through real-time SMR feedback paired with operant conditioning, ADHD children could learn to self-regulate SMR with the resulting improvements or worsening in their hyperkinetic behaviors based on whether they were reinforced to increase or decrease SMR. In their clinical utility of EEG article, Loo and Barkley (2005) state, “To demonstrate that EEG changes are responsible for treatment effects, reporting of actual EEG changes and correlation with treatment outcome must be shown” (p. 72). Four studies have met this challenge by correlating the extent of NFB subjects’ learning to self-modulate the targeted EEG with treatment outcome and found that those subjects demonstrating the greatest learning experience the most improvement on ADHD outcome measures (Drechsler et al., 2007; Gevensleben et al., 2009; Janssen et al., 2016; Lubar, Swartwood, Swartwood, & O’Donnell, 1995). These findings provide further evidence that enhancing EEG self-regulation is the mechanism of change from NFB treatment versus “neurosuggestion” or other placebo effects. Furthermore, two randomized controlled trials (RCT) have compared electromyographic (EMG) biofeedback with NFB to control for both nonspecific effects and the effects of self-regulation training (Bakhshayesh, Hansch, Wyschkon, Rezai, & Esser, 2011; Strehl et al., 2017). Both of these studies found that subjects learned to self-modulate the targeted physiological mechanism (either EMG or EEG) with NFB demonstrating significant superiority over EMG in reducing ADHD symptoms and this despite the fact that EMG subjects demonstrated more pronounced learning to self-regulate. Finally, in one RCT SM combined with NFB was found superior in multiple outcome domains at the end of treatment and 6-month follow-up to SM combined with attention training that used the identical instructions and game sequences as NFB except that the feedback was not based on subjects’ EEG thereby suggesting a specific effect for NFB as an augmentation to SM (Li, Yang, Zhuo, & Wang, 2013). Lia and colleagues also found that the combined SM/NFB subjects used significantly lower doses of SM during follow-up and reported fewer adverse side effects.
Third, the authors fail to acknowledge that in eight head-to-head comparisons with SM (see Table 2), NFB resulted in essentially equivalent improvement in treating ADHD’s core symptoms (Duric, Assmus, Gundersen, & Elegen, 2012; Flisiak-Antonijczuk, Adamowska, Chładzińska-Kiejna, Kalinowski, & Adamowski, 2015; Fuchs, Birbaumer, Lutzenberger, Gruzelier, & Kaiser, 2003; Gelade et al., 2017; Meisel, Servera, Garcia-Banda, Cardo, & Moreno, 2013; Moreno-García, Meneres-Sancho, Camacho-Vara de Rey, & Servera, 2019; Rossiter, 2004; Rossiter & La Vaque, 1995). These eight studies comprised 581 subjects and in only one head-to-head comparison (n = 32) has SM been found superior to NFB (Ogrim & Hestad, 2013). These comparative effectiveness studies provide strong evidence that NFB is an evidence-based treatment for ADHD.
Studies Comparing NFB With SM in Treating ADHD’s Core Symptoms.
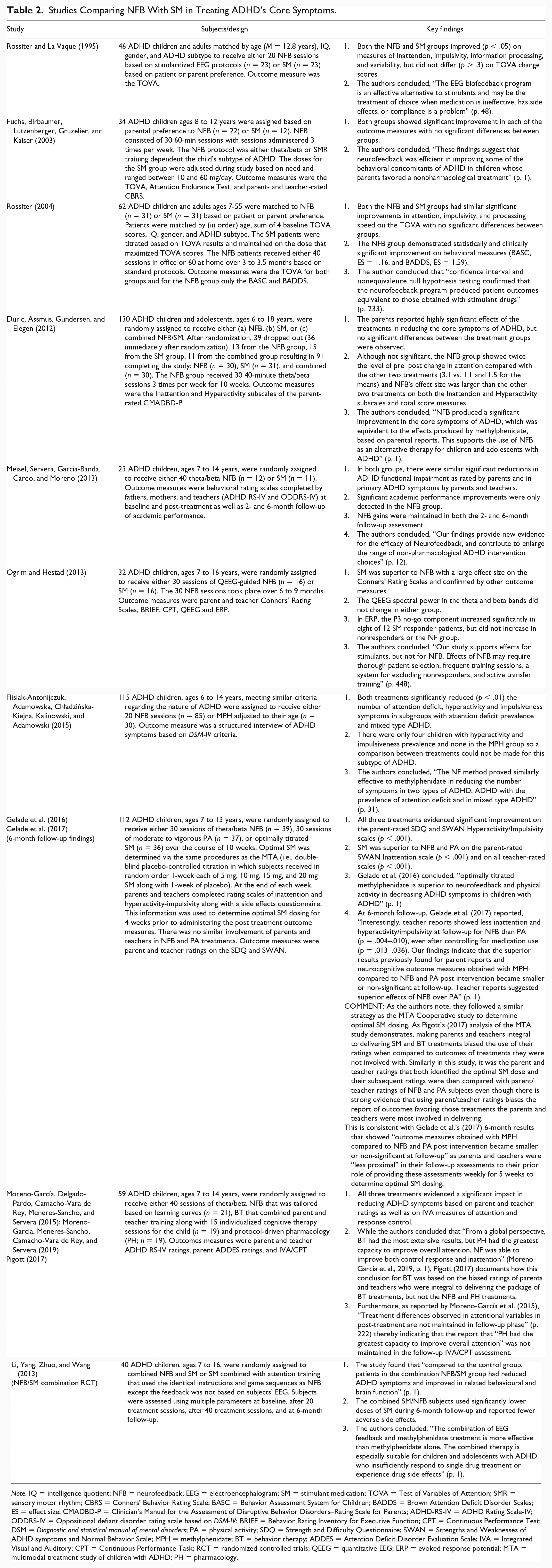
Note. IQ = intelligence quotient; NFB = neurofeedback; EEG = electroencephalogram; SM = stimulant medication; TOVA = Test of Variables of Attention; SMR = sensory motor rhythm; CBRS = Conners’ Behavior Rating Scale; BASC = Behavior Assessment System for Children; BADDS = Brown Attention Deficit Disorder Scales; ES = effect size; CMADBD-P = Clinician’s Manual for the Assessment of Disruptive Behavior Disorders–Rating Scale for Parents; ADHD-RS-IV = ADHD Rating Scale-IV; ODDRS-IV = Oppositional defiant disorder rating scale based on DSM-IV; BRIEF = Behavior Rating Inventory for Executive Function; CPT = Continuous Performance Test; DSM = Diagnostic and statistical manual of mental disorders; PA = physical activity; SDQ = Strength and Difficulty Questionnaire; SWAN = Strengths and Weaknesses of ADHD symptoms and Normal Behavior Scale; MPH = methylphenidate; BT = behavior therapy; ADDES = Attention Deficit Disorder Evaluation Scale; IVA = Integrated Visual and Auditory; CPT = Continuous Performance Task; RCT = randomized controlled trials; QEEG = quantitative EEG; ERP = evoked response potential; MTA = multimodal treatment study of children with ADHD; PH = pharmacology.
Fourth, Thibault and colleagues fail to acknowledge the extensive evidence from NFB studies whose training methodology mirror the best practices of operant conditioning. These studies consistently find NFB subjects learn to self-modulate the targeted EEG, this learning is associated with improvements on a wide variety of ADHD outcome measures of interest, and both are sustained at follow-up (e.g., Leins et al., 2007; Strehl et al., 2017; Strehl et al., 2006) even up to 2 years later (Gani, Birbaumer, & Strehl, 2008). These findings demonstrating the sustained ability to self-modulate the targeted EEG during follow-up with ongoing symptomatic improvement are unlike anything in the placebo literature. Findings further buttressed by Doren et al.’s (2018) recent meta-analysis documenting the sustained effects on ADHD outcomes for NFB subjects in RCTs.
The NFB Field Shares the Blame
Although NFB’s origins are based in the science of learning, the field has been negligent at ensuring that clinicians, researchers, and device manufactures adhere to this science. Examples include the following:
Monitoring within-session learning curves is not standard practice for NFB clinicians, and in fact it is our observation that most clinicians do not assess for evidence of learning.
The vast majority of NFB studies do not assess for evidence of learning even though this is the presumed mechanism of change. It is only recently that this is required for publication in the industry-sponsored journal NeuroRegulation when authors claim to provide operant conditioning of the EEG.
Virtually all device manufacturers include an auto-thresholding option despite Sherlin and colleagues (2011) clarion call that such systems violate learning science and “could effectively train in the opposite direction and result in an increase in aberrant and negative (EEG) behaviors” (p. 299). Unfortunately, this option is used by many, if not most, clinicians, particularly those who oversee multiple “NFB” sessions at a time.
As with any form of operant conditioning, there are learners and nonlearners. The same is true with NFB and it is learners who experience the most improvement on ADHD outcome measures. Given this fact, it is an indictment of the field that there are no studies comparing strategies to identify those practices that best promote subjects’ learning to self-modulate the targeted EEG. Consequently, there is no empirical guidance to determine which operant training methodologies are most effective in maximizing learning—and this in a field with a 75+ year history of basic and applied research.
Finally, the NFB field and its detractors continue to conduct research that violates behavioral principles, and both sides cite such substandard research when it supports their viewpoint. This practice must stop. Evidence of learning trumps all, and if there is no evidence of learning, operant conditioning of the EEG did not occur.
Conclusion
There is plenty of blame to go around, yet if the field is to evolve and progress, we must demand training methodologies that follow learning principles and proof that learning occurred from all who claim to perform NFB. Hence, our critique of Thibault and colleagues, and the sham-controlled studies on which their argument is based, is also a plea to NFB researchers and clinicians to demonstrate that their methods are consistent with the best practices in behavioral learning. If both sides can agree to this rigor, it will promote clarity and consistency in the NFB literature that is not present today and provide guidance to necessary steps for advancing it forward.
Most importantly, we hope our Guest Editorial conveys the truth that learning methodology matters. With this caveat, we strongly recommend operant conditioning of the EEG for the treatment of ADHD, either as a standalone treatment or augmentation to other evidence-based treatments. As for prescribing “neurosuggestion therapy” for the treatment of ADHD, more research is required since its underlying premise is unproven and evidentiary base anecdotal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.E.P. is board certified in neurofeedback and has consulted for Amen Clinics, Brain Resources, CNS Response, and the International Society of Neurofeedback and Research. He is also on the scientific advisory board of Narbis, a neurofeedback technology company. R.C. is board certified in neurofeedback and Editor-in-Chief of the journal NeuroRegulation. M.T. is board certified in neurofeedback.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Society of Neurofeedback and Research, Biofeedback Certification International Alliance, and Association of Applied Psychophysiology and Biofeedback contributed equally to the open access publication fees with our deep gratitude.