
Abstract
Introduction
ADHD is a common childhood neurodevelopmental disorder with an estimated worldwide prevalence of 3.4% (Polanczyk, Salum, Sugaya, Caye, & Rodhe, 2015). It is a heterogeneous diagnosis, in which genetic, biological, and environmental factors play an important role (Larson, Russ, Kahn, & Halfon, 2011; Pressman et al., 2006; Thapar & Cooper, 2016). To meet Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) classification criteria for ADHD, a child must display six out of nine symptoms from the inattention cluster and/or six out of nine symptoms from the hyperactivity/impulsivity cluster (APA, 2013). These symptoms depend on age and sex and may vary in different life stages (Barkley & Murphy, 2006; Biederman et al., 2005; Gershon, 2002). In addition, ADHD has a high comorbidity rate, and many symptoms of comorbid disorders show an overlap with ADHD symptoms (Jensen & Steinhausen, 2014). Besides age, gender, and comorbidity, psychosocial context may shape ADHD presentation (Rutter, 2012; Thapar, Cooper, Eyre, & Langley, 2013). Diagnosing ADHD further requires symptoms to interfere with one’s social life and development, presence of symptoms before the age of 12, and no alternative explanation of symptoms by another mental disorder (APA, 2013). This makes it a challenge for clinicians to make a distinction between ADHD symptoms due to an ADHD diagnosis or due to other causes.
In 2014, the Dutch Health Council (DHC) found a fourfold increase in methylphenidate use among children over the past decade and a 30% increase in specialized health care facilities use for problems related to ADHD symptoms (Health Council of the Netherlands, 2014). To halt this increase, the DHC proposed a prominent role for primary health care in differentiating between children with ADHD symptoms who only need supportive counseling and children with serious impairment who need specialized mental health care. Therefore, the Dutch government introduced a new Child and Youth Act in 2015, which made local governments responsible for prevention, support, and treatment of developmental and psychological problems and disorders. The premise of the Act is that care must match the needs of the child and family, which should not be dictated exclusively by the diagnosis of the child. The number of children in specialized care must be decreased by increasing preventive and early intervention support and the use of social networks within the direct environment of children (Ministerie Volksgezondheid, Welzijn en Sport/ Ministry of Health and Sports, 2014). Accurate evaluation of ADHD symptoms is one of the cornerstones of success of this new Act to prevent not only overdiagnosis based on just symptoms but also underdiagnosis with the risk of complications.
Prior to the introduction of the Child and Youth Act, a wide range of data from children seen at a specialized ADHD clinic were analyzed to gain insight into characteristics of children sent to a specialized care facility. The data were analyzed at the hand of the following research questions:
Method
Participants
The database was that of children attending the Medipsy ADHD clinic (“the ADHD clinic”). The ADHD clinic is a collaboration between the Sint Jans Gasthuis Hospital (SJG), Medipsy—a primary mental health care clinic—and Metggz—a specialized child psychiatry institute, which was started in 2010. It is an outpatient clinic for children between 6 and 18 years old, located at the SJG Weert, a small hospital in a southern province of the Netherlands. All children were referred by a general practitioner or youth health care physician (school doctor) because of symptoms related to attention deficit and/or hyperactivity and impulsivity. Fifteen children had seen a psychologist at another primary health care facility prior to their visit and 14 children already used methylphenidate before referral. The ADHD clinic used only two triage criteria, namely, age (>6 and <18 years) and a referral related to ADHD symptoms. There was no triage on the severity of DSM symptoms and cross-situational impairment. The data set is based on files of children attending between September 2011 and November 2015, during the time in which there was consistent composition of, and practice by, the multidisciplinary team.
Procedure
The multidisciplinary team of the ADHD clinic consisted of a psychologist, a nurse specialist, a staff member from the child psychiatric center, and a pediatrician. Prior to the visit, all screening rating scales, an open questionnaire for the teacher, and a demographic form were completed by both parents and teacher. During the clinical visit, the child and parents were extensively interviewed by the psychologist concerning different aspects of ADHD and comorbidities. Parents were always asked who took the initiative for referral to an ADHD clinic (e.g., parents, teacher, or both parents and teacher). Subsequently, a medical consultation took place. Besides medical history and complete physical examination, the pediatrician discussed the prefilled demographic form, which also contained questions about early development of the child. The next step was for the ADHD multidisciplinary team to discuss the collected data. Diagnoses were made by team consensus, taking into account information from the interview, Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria, developmental history and somatic comorbidity, thresholds on rating scales, and information from the teacher open questionnaire. Only children who met criteria for ADHD diagnosis without suspected comorbidity received a same-day ADHD diagnosis. All others were either referred to a specialized child psychiatric center for additional diagnostics or referred to adequate primary care, for example, Youth Care or school counseling team.
Measures
Child Behavior Checklist (CBCL), Teacher Report Form (TRF), and Youth Self-Report (YSR)
The CBCL is a component in the Achenbach System of Empirically Based Assessment (ASEBA) developed by Thomas M. Achenbach (Achenbach & Rescorla, 2001). The ASEBA uses different checklists for teachers (TRF), and children older than 11 can fill in their own checklist (YSR). We used the Dutch school age version from 2001 by Verhulst (Verhulst, Koot, Akkerhuis, & Veerman, 1990). These sets of questionnaires offer a standardized way to quantify behavioral and emotional problems and skills in children. Both attention problem scores and total scores were used during the evaluation of the child; total scores were used to determine the need for specialized mental health care. T-scores between 65 and 70 were described as subclinical scores and above 70 as clinical scores. In 2013, the Dutch Committee on Tests and Testing (Commissie testaangelegenheden, COTAN) assessed the Dutch version as insufficient in terms of reliability but sufficient in terms of validity, the one that made this rating scale useful for our seccond research question. In this study, parents, the teacher, and children older than 11 completed the form.
ADHD Vragen Lijst (AVL; ADHD questionnaire)
AVL is a Dutch behavioral questionnaire for children aged 4 to 18 years that is based on the Conners’ Rating Scale for ADHD and developed by Van der Ploeg and Scholte (2001). It determines whether there are behavioral symptoms of ADHD, and if so, to what extent symptoms of inattention, hyperactivity, and impulsivity play a role. The AVL is based on the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) and describes 18 behavioral symptoms. The COTAN assessed the test reliability as good and the validity as sufficient. At the ADHD clinic, the teacher and both parents filled in the AVL.
Open questionnaire for the teacher
This open questionnaire for teachers was designed by the ADHD clinic based on the Conners’ Rating Scale for ADHD. It consists of 13 general questions about functioning at school and psychosocial development, and 18 questions describing behavior based on the DSM-IV diagnostic criteria for ADHD.
Demographic form
This open questionnaire for parents was also designed by the ADHD clinic and consisted of questions concerning legal matters of parenthood, family situation, education level and employment of both parents, birth and early development of the child, prior interventions, and family history.
Data Analysis
All data used in this study were uploaded in SPSS (Version 22) for analysis. To answer the research questions, the outcome at the end of the diagnostic process was divided into two groups: Group A with ADHD and/or other psychiatric symptoms with special need due to serious impairment in need of specialized mental health care, and Group B with ADHD without comorbidity requiring supportive counseling eventually combined with methylphenidate at a primary care clinic or other problems requiring primary or supportive care.
First, the demographic characteristics of Groups A and B were analyzed; in Group B (need for primary care), a distinction was made between those who were diagnosed with ADHD and those who did not receive a diagnosis. In addition, crosstabs were used to analyze if demographic variables and outcome of rating scales were associated with first initiative for referral. Logistic regression in a univariable model with Group A and Group B was used to identify significant factors differentiating between primary and specialized mental health care. In the logistic regression, positive family history for ADHD was combined with positive family history for other psychiatric diagnosis. Variables from this univariable logistic regression with a p value ≤.01 were combined in a multivariable logistic regression to assess independence of each other on the outcome.
Results
Sample Characteristics and Study Flow Diagram
Files of 261 children were analyzed (see Figure 1, and Tables 1 and 2). Mean age was 10 years (SD = 2.87), 72.8% was male. In 258 cases, a clear answer on the question “who took the first initiative for referral to an ADHD clinic for the inattention and/or hyperactive problems?” was present. Most children (50.8%) were referred by both parents and school. Initiative of referral was not significantly associated with the need for specialized care; the percentage of children in need of specialized mental health care was only slightly higher when both parents and teacher - initiated the referral. “ADHD and/or other psychiatric symptoms with special need due to serious impairment in need of specialized mental health care” was the outcome in 82 children (31.4%). Besides marital status of the parents, there were no demographic differences between Group A and Group B (Table 1). Distribution of these demographic factors over the three referral groups (i.e., referral by teacher, parents, or both) only showed significantly more boys than girls in the school referral group (Table 2). Scores on general symptom severity by mothers and teacher on the CBCL and TRF were higher in the group that was found to be in need of specialized health care. Scores on ADHD symptoms by both parents and teacher on ADHD rating scale (AVL) were the highest in Group B, that is, children diagnosed with ADHD in absence of comorbidity. Rating scales only partly reflected the initiative for referral by school or parents.
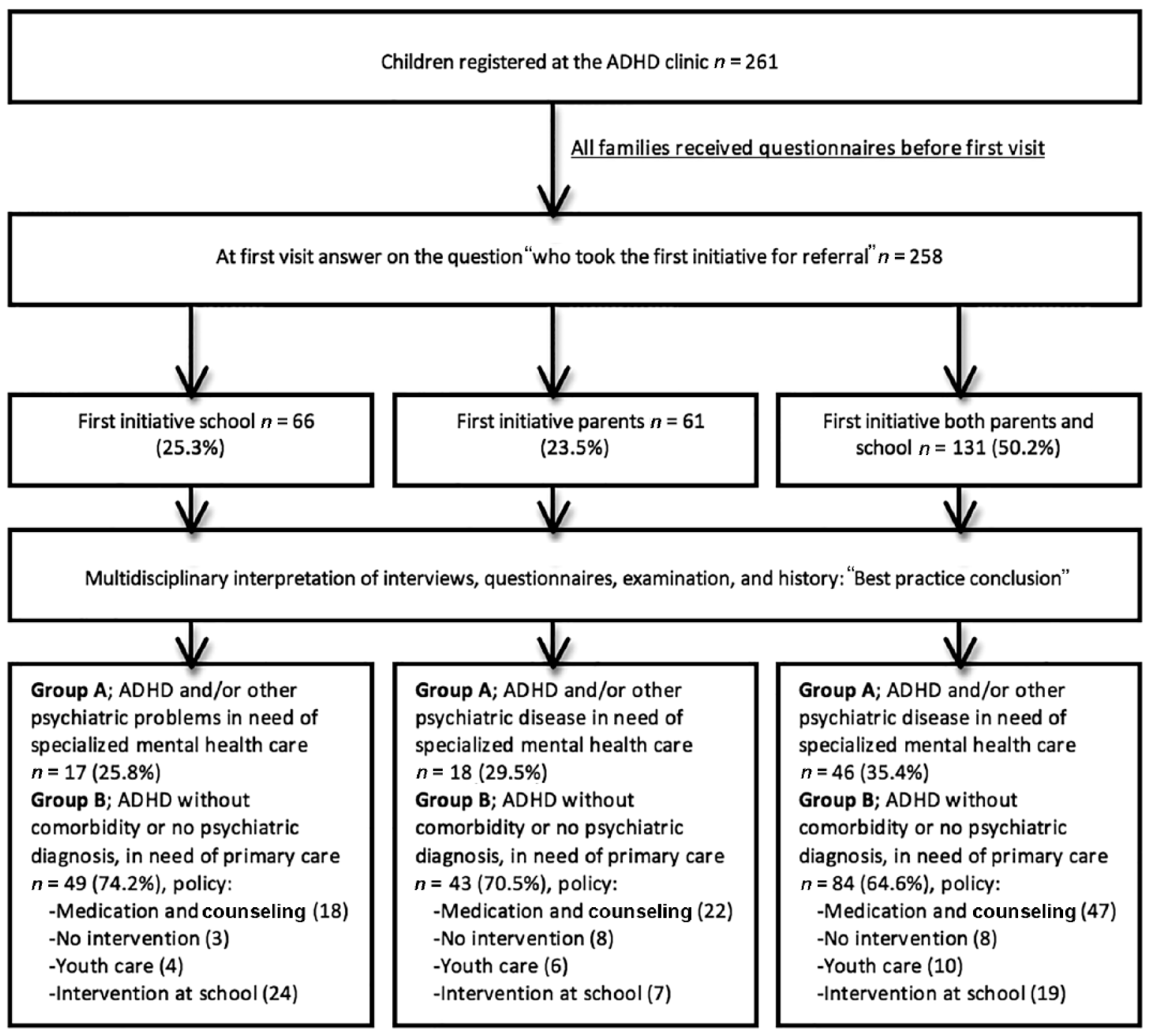
Study flow diagram. Number in parenthesis refer to number of children.
Characteristics of Children in Need of Specialized Care (Group A: “ADHD or Other Psychiatric Symptoms With Serious Impairment in Need of Specialized Mental Health Care”) and of Children in Need of Primary Care (Group B1: “ADHD Without Comorbidity Requiring Supportive Counseling Eventually Combined With Methylphenidate at Primary Care Clinic” and Group B2: “Other Problems Requiring Primary Care”).
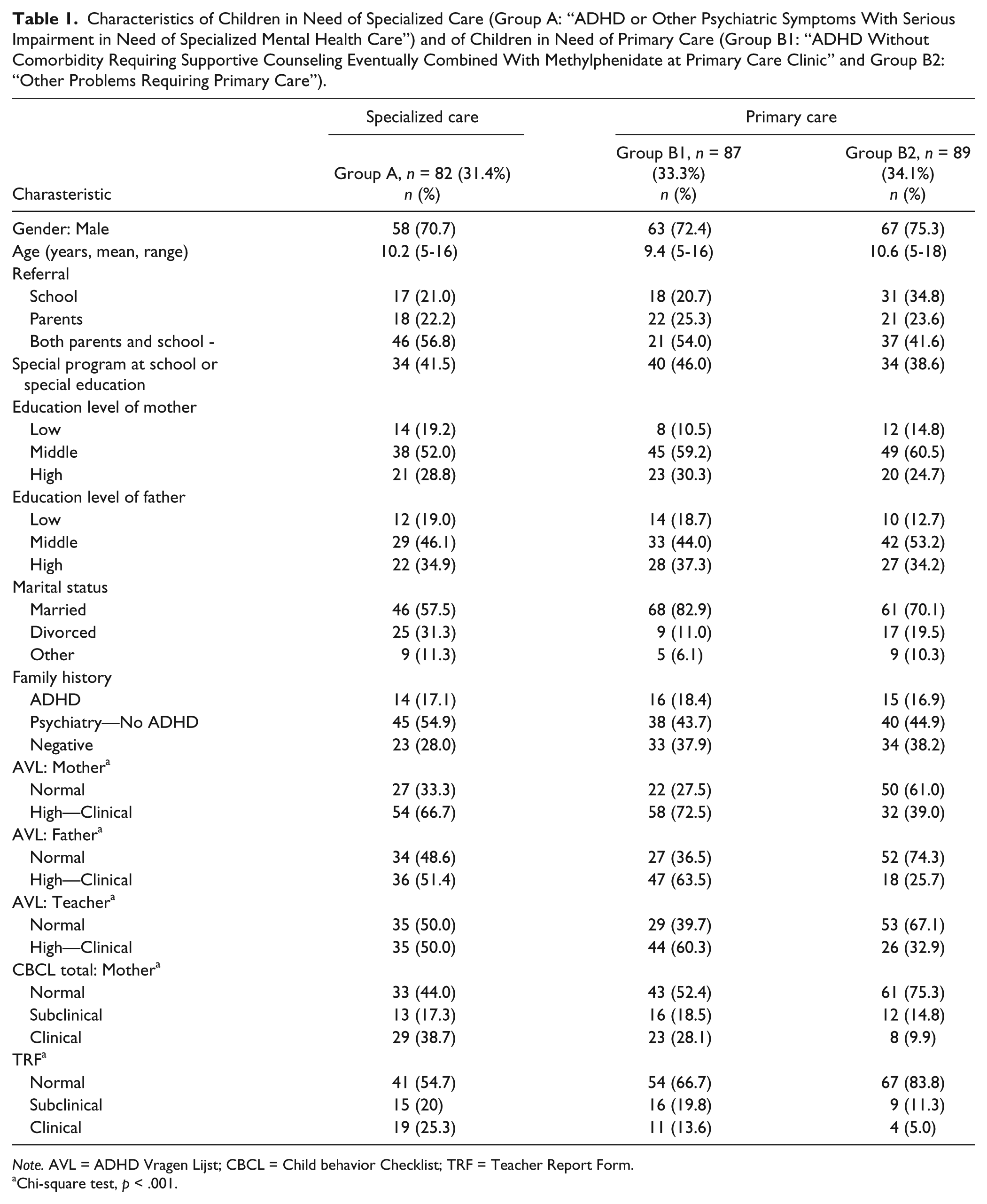
Note. AVL = ADHD Vragen Lijst; CBCL = Child behavior Checklist; TRF = Teacher Report Form.
Chi-square test, p < .001.
Characteristics of Children Based on First Initiative for Referral (i.e., First Initiative for Referral Taken by School, Parents, or Both Parents and School).
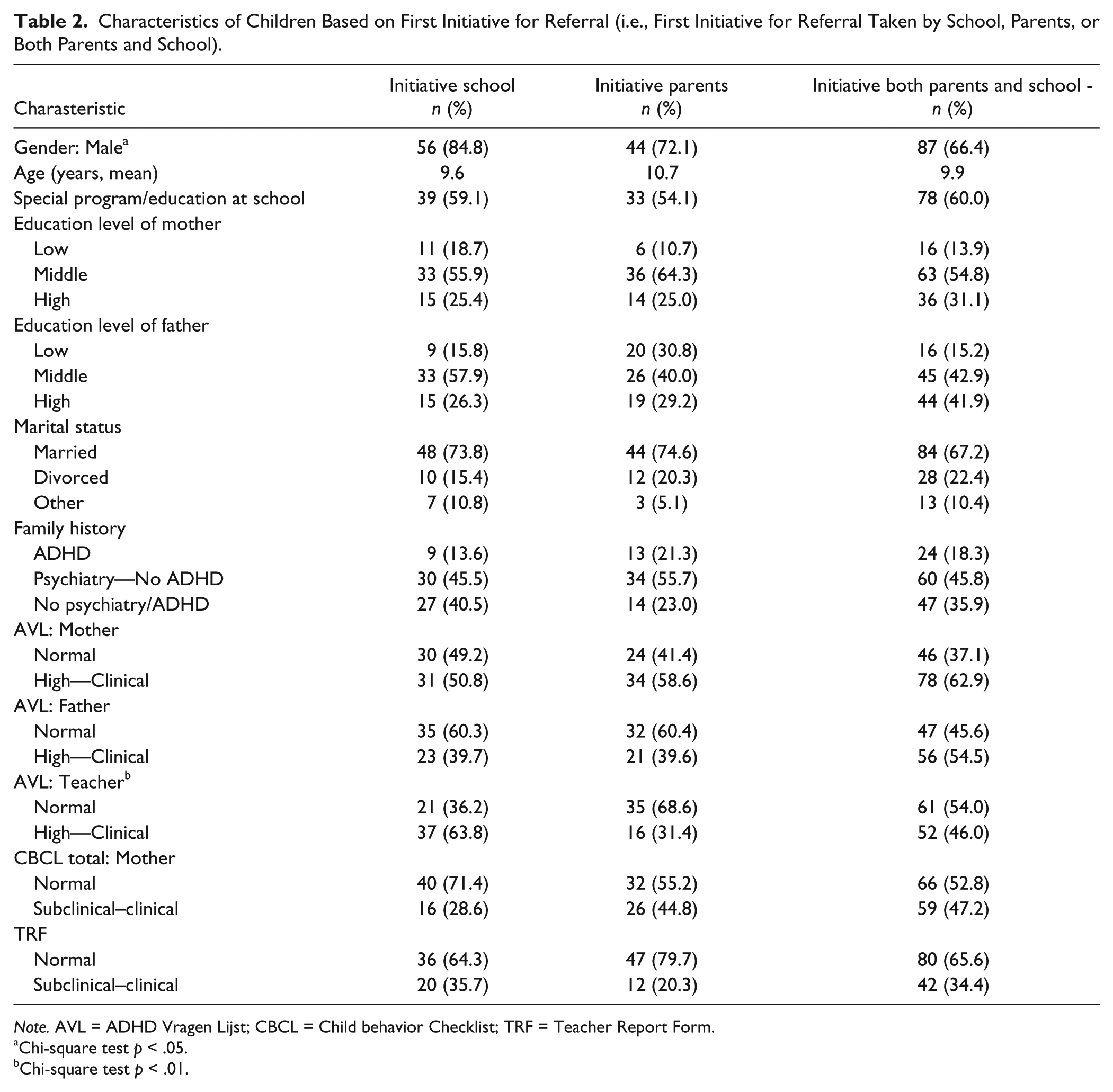
Note. AVL = ADHD Vragen Lijst; CBCL = Child behavior Checklist; TRF = Teacher Report Form.
Chi-square test p < .05.
Chi-square test p < .01.
Characteristics of Children Associated With Need of Specialized Care
In the univariable analysis, marital status of parents, the CBCL filled in by the mother, and the TRF were associated with increased odds for the need of specialized mental health care (Table 3). In the multivariable logistic regression analysis, all these three variables remained significant, with the TRF in particular (p = .007; CBCL, p = .02; marital status, p = .02). The effect of the TRF and CBCL was even more obvious when analysis was done with clinical scores only.
Univariable and Multivariable Logistic Regression Identifying Risk Factors for Children With ADHD With Serious Impairment and/or Other Psychiatric Symptoms in Need of Specialized Mental Health Care (Group A).
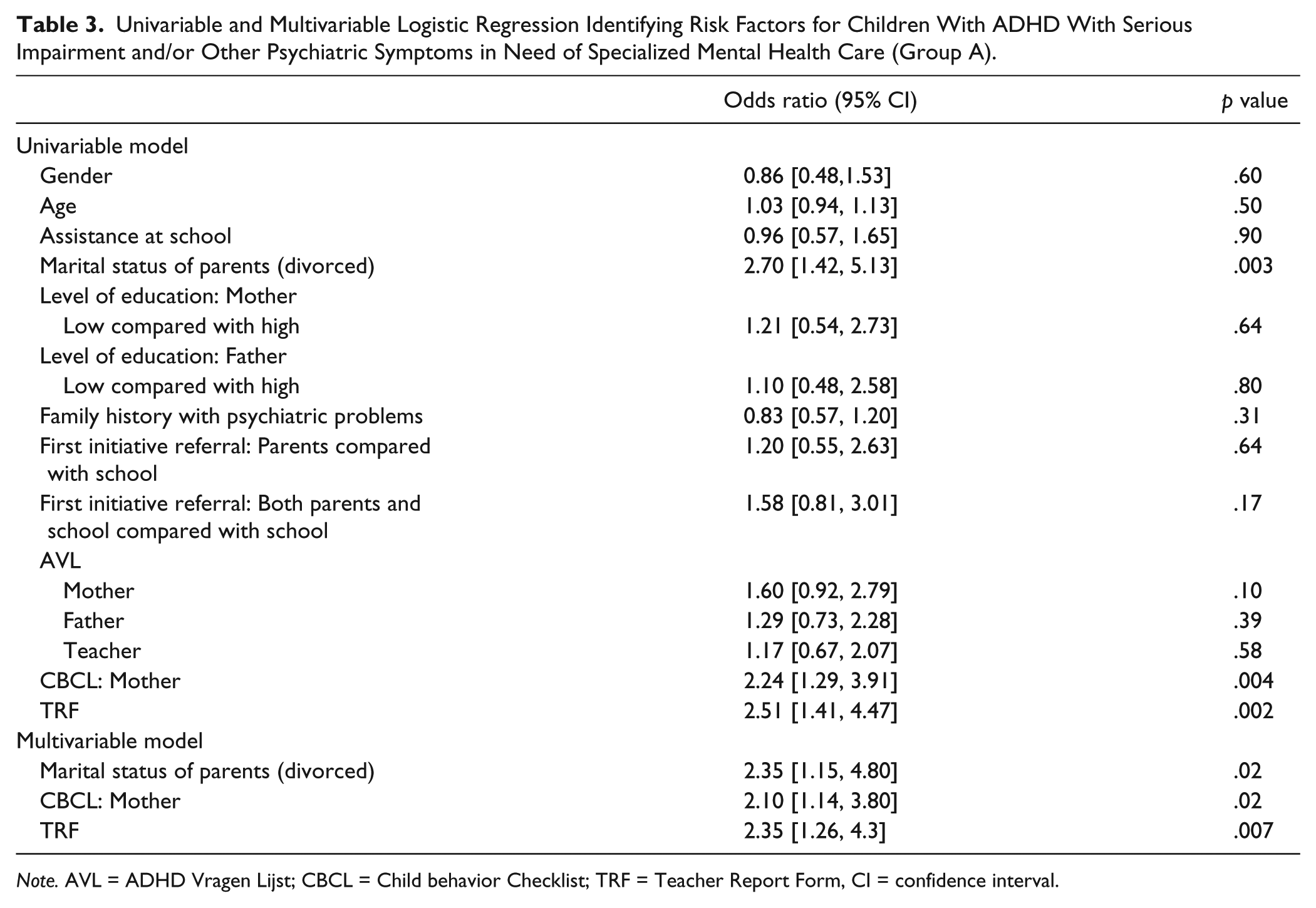
Note. AVL = ADHD Vragen Lijst; CBCL = Child behavior Checklist; TRF = Teacher Report Form, CI = confidence interval.
Discussion
The Committee on Psychosocial Aspects of Child and Family Health and Task Force on Mental Health (2009) wrote a policy statement in which they described mental health competencies for pediatric primary care. The statement focused on treatment of children with mental problems in absence of a diagnosis by pediatric primary care. Until 2015, these children were treated by specialized mental and pediatric health care facilities in the Netherlands; the new Dutch Child and Youth Act must shift the care of these children to primary (health) care facilities. This is also true for the support and treatment of children with ADHD without severe impairment and/or comorbidity. Primary health care for children in the Netherlands involves a diverse group, including general practitioners, youth health care physicians, social workers, psychologists, and coaches. In addition, the government wants to create a formal role for teachers and family members.
This study analyzed data from children seen at a specialized ADHD clinic before introduction of the new Child and Youth Act to identify characteristics that can be used to differentiate between children who require primary care and children with serious impairment in need of specialized mental health care. Of the children referred to this ADHD clinic, 34.1% displayed ADHD symptoms but did not receive a specific mental diagnosis; they were referred to primary (health) care. In addition, 33.3% were diagnosed with ADHD in absence of comorbidity. The demographic characteristics of children both in need of primary and specialized care were heterogeneous, and there were no demographic differences between the groups -except for the marital status of the parents—In the group of children referred to specialized care, more parents were divorced. Recently, Brown et al. (2017, p. 349) concluded that “there is a significant association between adverse childhood experiences (ACE) score and ADHD” and they advised routinely evaluating for ACE to improve ADHD management. This study did not examine why more children from divorced parents were referred to specialized care (e.g., severity of ADHD symptoms, family problems), but this result does fit with the advice to evaluate for ACE. No significance was found for a positive psychiatric family history to distinguish between levels of care, which may be explained by the fact that parents with mental health problems tend to use more services (Sayal, Mills, White, Merrell, & Tymms, 2015).
A striking observation was that almost half of the children referred only by school or only by the parents received a diagnosis of ADHD or were in need of specialized mental health care. Other studies have shown that concordance among teachers’ and parents’ perceptions of ADHD symptoms could differ due to reference framework, difference in salience, and/or variations in children’s behavior in different settings, which could be caused by differing situational demands (Efstratopoulou, Simons, & Janssen, 2012). A one-dimensional measurement of the initiative of referral can therefore not be used as screening criterion to differentiate between levels of care, as it does not adequately capture the presence of symptoms and/or impairment in a different setting.
To objectivize the presence of ADHD symptoms, rating scales can be used. Efron, Bryson, Lycett, and Sciberras (2016) recently showed that rating scales of teachers are useful regarding ADHD symptoms, which was also reflected in this study. Need for specialized mental health care was not reflected in ADHD rating scales, but in the total scores of the CBCL and TRF. This corresponds with the fact that these children suffer from serious impairment and/or comorbidities, which may give symptoms other than attention deficit and/or hyperactivity and impulsivity. Despite the fact that CBCL and TRF were statistically significant in differentiating between specialized or primary care, exclusive reliance on these questionnaires is a pitfall for clinical practice. Of the children in need of specialized care, 56% and 45% scored subclinical or clinical on the CBCL and TRF, respectively, and positive predictive value was low. Overall, there were few questionnaires with a symptom score in the clinical range. Like we know from literature, also in this study, the cross-informant scores between teacher, father, and mother on all rating scales varied (Rescorla et al., 2014). To obtain a clear picture of symptoms and impairment, this study used contextual information during the interviews as a guide together with the questionnaires and the rating scales, as suggested in a meta-analysis concerning the multi-informant (De Los Reyes et al., 2015; Korsch & Petermann, 2013). Studies by Gordon et al. (2006) and Gathje, Lewandowski, and Gordon (2008) showed the impact of using the impairment criterion along with symptoms on clinical decision making. Their studies found that impairment combined with symptoms can lower diagnoses. This study not only showed the same but also found the reverse—low symptom scores on questionnaires but impairment during the interview. This can have several causes; most noticeable was the difference between teacher’s AVL and TRF questionnaires (low scores) and the open questionnaire for teachers, which did show impairment many times. This shows the importance of good cross-sectional analysis, not only through rating scales but also through interviews with, for example, teachers. Differentiation between levels of care was only possible through comprehensive interpretation of all data.
A key finding was that more than half of the children referred with attention problems received no additional support at school before referral. Regarding the goal of the Dutch government, this raises opportunities for early intervention by school-based programs.
These results have several limitations. First, results are based on data collected from a group referred to a specialized ADHD clinic in a specific region in the Netherlands. Little is known about regional differences regarding ways of referral and use of different services for ADHD. Although the various participant characteristics like sex and age are in line with other populations and studies, we cannot assume that the demographics of patient populations seen by other clinics are identical or even similar. The clinic studied here is situated in a hospital; it is therefore possible that children with more comorbidity and social problems are directly referred to specialized mental health care. Second, it could be that some referred children did not register at the clinic, which may cause bias in the data set. Other studies find teacher referral rates from 30% to 38% (Sayal et al., 2015; Visser, Zablotsky, Holbrook, Danielson, & Bitsko, 2015). In this group, teacher referral rates were slightly lower (25.6%). This difference could be explained by the fact that some children (e.g., girls) referred by the teacher did not go to the ADHD clinic. Several factors can influence the likelihood of parents seeking help for attention deficit problems—and thereby influence referral outcome, such as parent education, unclearness of the referral route, or the availability of services in a region (Yamauchi, Fujiwara, & Okuyama, 2014). Third, ADHD diagnosis is a best practice diagnosis. There is no gold standard for a diagnosis of ADHD, and it is difficult to discriminate between ADHD symptoms without mental diagnosis and a diagnosis of ADHD. There are no data on the uniformity of the diagnostic path in different centers. Due to interrater reliability, impairment can be weighed differently and change outcome (Epstein et al., 2014). Further research into ways of clinical decision making is important for better interpretation and generalization of data.
Clinical Implications and Conclusion
These findings shed light on the complexity of triaging children with ADHD symptoms—by implication, the viability of the Dutch government’s goal to shift the care for children with ADHD symptoms to primary health care facilities. Children who seek help for their attention problems and/or hyperactivity form a heterogeneous group, and despite the fact that clinical scores on CBCL and TRF gave direction to the need of specialized care, only clinical decision making by the multidisciplinary team was decisive. Every child needs extensive comprehensive evaluation to gain insight in the origin of the symptoms, the presence of ACEs, and to evaluate the degree of impairment. It is important to determine which options primary care has to evaluate symptoms of attention deficit and/or hyperactivity, to prevent under- and/or overdiagnosis, and to make the new Dutch policy a success. By developing consultative structures and relationships between primary and specialized health care, proper critical assessment of every child can be done.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.