
Abstract
Introduction
The diagnostic criteria for ADHD require that patients experience not only symptoms of inattention and/or hyperactivity–impulsivity but also interference with or reduced quality of functioning in social, academic, or occupational domains (American Psychiatric Association, 2000, 2013). Based on this definition, ADHD is therefore expected to have a negative impact across multiple domains of patients’ health-related quality of life (HRQoL; Coghill & Hodgkins, 2016; Danckaerts et al., 2010). Following guidance from the European Medicines Agency that clinical efficacy trials of ADHD medications should assess both ADHD symptoms and functional impairments (European Medicines Agency, 2010), recent studies have included functional impairment and/or HRQoL measures as well as symptom-based measures (Coghill, 2011). ADHD symptoms, functional impairments, and HRQoL are hypothesized to be related, but distinct constructs, raising the question of the extent of congruence or divergence between the instruments used to assess these outcomes in clinical trials. It is therefore important that functional impairment and HRQoL instruments are able to tap into domains of impairment that are relevant to ADHD, but that they are not simply surrogate measures of ADHD symptoms (Coghill, Danckaerts, Sonuga-Barke, Sergeant, & ADHD European Guidelines Group, 2009).
Among the instruments commonly used to assess HRQoL and functional impairments in clinical trials of ADHD medications are the Child Health and Illness Profile–Child Edition: Parent Report Form (CHIP-CE:PRF) and the Weiss Functional Impairment Rating Scale–Parent (WFIRS-P), respectively (Banaschewski et al., 2014; Banaschewski et al., 2013; Coghill, 2010; Coghill et al., 2013; Danckaerts et al., 2010; Escobar, Schacht, Wehmeier, & Wagner, 2010; Hervas et al., 2014; Nagy et al., 2016). While both are parent-rated instruments intended for use in children, the CHIP-CE:PRF is a generic HRQoL instrument (not specific for any disease or disorder), whereas the WFIRS-P was designed around functional impairments that are most relevant to patients with ADHD (but not necessarily unique to ADHD).
The CHIP-CE:PRF has been psychometrically validated in population samples (Estrada et al., 2010; Riley et al., 2004) and in children and adolescents with ADHD (Riley, Coghill, et al., 2006; Schacht, Escobar, Wagner, & Wehmeier, 2011). Scores on the 76-item questionnaire are normalized to T-scores using data from a U.S. reference population for each of the five CHIP-CE:PRF domains (Achievement, Risk Avoidance, Resilience, Satisfaction, and Comfort) and 12 nested subdomains (Estrada et al., 2010; Riley et al., 2004). The Achievement domain (10 items) assesses children’s role performance at school and with peers, and comprises the subdomains of Academic Performance and Peer Relations. The Risk Avoidance domain (14 items) assesses children’s ability to refrain from behaviors that may lead to illness or injury or that may interfere with social development and comprises the subdomains of Individual Risk Avoidance and Threats to Achievement. The Resilience domain (19 items) assesses children’s family support, coping abilities, and physical activity levels, and comprises the subdomains of Family Involvement, Social Problem-Solving, and Physical Activity. The Satisfaction domain (11 items) assesses children’s well-being and self-esteem, and comprises the subdomains of Satisfaction with Health and Satisfaction with Self. The Comfort domain assesses children’s positive and negative physical and emotional symptoms and feelings and limitations in their day-to-day activities, and comprises the subdomains of Physical Comfort, Emotional Comfort, and Restricted Activity (Riley et al., 2004). The WFIRS-P has also been psychometrically validated in children and adolescents with ADHD (Dose, Hautmann, & Döpfner, 2016; Gajria et al., 2015; Tarakcioglu, Memik, Olgun, Aydemir, & Weiss, 2015). Scores from 0 to 3 on the 50-item questionnaire are reported as the mean score in total and in each of the six WFIRS-P domains: Family, Learning and School (with subdomains of Learning and Behavior), Life Skills, Child’s Self-Concept, Social Activities, and Risky Activities. The complete WFIRS-P questionnaire is available on the Canadian ADHD Resource Alliance (CADDRA; 2014) website.
Here, we use data from two recent Phase 3 clinical trials of stimulant and nonstimulant ADHD medications to investigate the relationships between symptom-based, functional impairment, and HRQoL outcomes in children and adolescents with ADHD. Both the CHIP-CE:PRF and WFIRS-P were secondary efficacy outcome measures in a placebo-controlled study of the stimulant prodrug lisdexamfetamine (LDX) that included an osmotic-release oral system methylphenidate (OROS-MPH) reference arm (study SPD489-325; Banaschewski et al., 2013; Coghill et al., 2013); and the WFIRS-P was a secondary efficacy outcome measure in a placebo-controlled study of the selective α2A adrenergic receptor agonist guanfacine extended-release (GXR) that included an atomoxetine (ATX) reference arm (study SPD503-316; Hervas et al., 2014). In concordance with the results of previous studies and meta-analyses (Cheng, Chen, Ko, & Ng, 2007; Punja et al., 2016; Storebo et al., 2015; Stuhec, Munda, Svab, & Locatelli, 2015), all four of the medications studied in these two clinical trials were significantly more effective than placebo in relieving ADHD symptoms, as assessed using the investigator-rated ADHD Rating Scale IV (ADHD-RS-IV; Coghill et al., 2013; Hervas et al., 2014). Secondary efficacy outcomes in SPD489-325 showed that LDX and OROS-MPH were significantly more effective than placebo in improving CHIP-CE:PRF T-scores in the domains of Achievement, Risk Avoidance, Resilience, and Satisfaction, and in improving WFIRS-P total scores (and WFIRS-P scores in the domains of Family, Learning and School, Social Activities, and Risky Activities for both medications, and in Life Skills and Child’s Self-Concept for OROS-MPH only; Banaschewski et al., 2013). Secondary efficacy outcomes in SPD503-316 showed that GXR and ATX were more effective than placebo in improving WFIRS-P total scores (and scores in the domains of Learning and School for both medications, and in Family and Social Activities for GXR only; Hervas et al., 2014). Safety outcomes from both studies were consistent with those of previous studies and indicated that the medications were generally well tolerated (Coghill et al., 2013; Hervas et al., 2014).
In the present post hoc analyses, we use correlational analyses to investigate the associations between changes from baseline to endpoint in ADHD-RS-IV, CHIP-CE:PRF, and WFIRS-P scores in SPD489-325, and ADHD-RS-IV and WFIRS-P scores in SPD489-316. We hypothesized that very strong correlations (Evans, 1996) with ADHD-RS-IV would be observed if the CHIP-CE:PRF and WFIRS-P instruments effectively acted as additional measures of ADHD symptoms, and that very weak or no correlations would be observed if the CHIP-CE:PRF and WFIRS-P instruments assessed impairments and HRQoL deficits that are not connected with ADHD symptoms. In contrast, moderate correlations between these outcome measures would be observed if the instruments assessed symptoms, functional impairments, and HRQoL as separable but interconnected aspects of the treatment response in patients with ADHD.
Method
Studies
The present article describes post hoc analyses of results from two separate randomized, double-blind, placebo-controlled efficacy and safety trials, one of LDX with an OROS-MPH reference arm and one of GXR with an ATX reference arm. Summaries of the published prespecified efficacy analyses are provided for context. The reference arms were included in the studies and prespecified analyses as active controls (established treatments known to be superior to placebo), rather than as direct comparators. The purpose of an active control is to aid interpretation of results if the primary endpoint is not met for the investigational product. The studies were neither designed nor powered for comparisons between active treatments.
Study SPD489-325 (ClinicalTrials.gov NCT00763971) was a randomized, double-blind, placebo-controlled, Phase 3 trial of the efficacy and safety of LDX in children and adolescents with ADHD in Europe (48 sites in 10 countries). OROS-MPH was included as a reference treatment. Details of the study design, results, and previous post hoc analyses are published (Banaschewski et al., 2013; Coghill et al., 2013; Coghill et al., 2014; Soutullo et al., 2013).
Study SPD503-316 (ClinicalTrials.gov NCT01244490) was a randomized, double-blind, placebo-controlled, Phase 3 trial of the efficacy and safety of GXR in children and adolescents with ADHD in Europe (45 sites in 11 countries), the United States (11 sites), and Canada (two sites). ATX was included as a reference treatment. Details of the study design, results, and previous post hoc analyses are published (Hervas et al., 2014; Huss et al., 2016).
Study Populations and Designs
Both studies enrolled male and female children (aged 6-12 years) and adolescents (aged 13-17 years) with a Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnosis of ADHD and an ADHD-RS-IV total score of at least 28 (LDX study SPD489-325) or at least 32 (GXR study SPD503-316). Children and adolescents were excluded from the study if they had a comorbid psychiatric diagnosis (except oppositional defiant disorder) or if their current ADHD medication provided effective control of symptoms with acceptable tolerability (Coghill et al., 2013; Hervas et al., 2014). In the LDX study, children and adolescents were excluded if there had been a failed response to previous OROS-MPH treatment (Coghill et al., 2013).
Following screening and washout, enrolled participants were randomized (1:1:1) to receive LDX, placebo, or the OROS-MPH reference treatment for a double-blind treatment period of 7 weeks in SPD489-325; or to receive GXR, placebo, or the ATX reference treatment for a double-blind treatment period of 10 weeks for children or 13 weeks for adolescents in SPD503-316. In both studies, recruitment management ensured that about 25% of those enrolled were adolescents, and randomization was stratified by country and age group (children or adolescents; Coghill et al., 2013; Hervas et al., 2014). For regulatory reasons, at least 70% of enrolled participants in the GXR study were to be recruited in Europe (Hervas et al., 2014).
Study Drug Administration
In SPD489-325, doses were optimized to LDX 30, 50, or 70 mg/day or OROS-MPH 18, 36, or 54 mg/day from Week 0 to Week 4, and these doses were maintained for the remainder of the 7-week double-blind treatment period. Dose alterations (weekly stepwise increases or a single decrease) were permitted during dose optimization but not dose maintenance (Coghill et al., 2013). OROS-MPH 54 mg/day is the maximum dose approved in Europe.
In SPD503-316, doses were optimized to GXR 1 to 7 mg/day (up to a maximum of 4, 5, 6, or 7 mg/day depending on age and body weight as previously described), or ATX 0.5 or 1.2 mg/kg/day (for patients weighing <70 kg; maximum 1.4 mg/kg/day) or 40, 80, or 100 mg/day (for patients weighing ≥70 kg) from Week 0 to Week 4 (for children) or to Week 7 (for adolescents), and these doses were maintained for the remainder of the 10-week (for children) or 13-week (for adolescents) double-blind treatment period (Hervas et al., 2014). Dose alterations (weekly stepwise increases or a single decrease) were permitted during dose optimization but not dose maintenance (Hervas et al., 2014). ATX was titrated in accordance with the European marketing authorization.
Study Assessments
The primary efficacy outcome in both studies was the change in ADHD-RS-IV total score from baseline to endpoint (defined as the last on-treatment assessment with valid data, excluding baseline; Coghill et al., 2013; Hervas et al., 2014). Both studies included the WFIRS-P, and the LDX study also included the CHIP-CE:PRF among other secondary efficacy outcome measures (Banaschewski et al., 2013; Coghill et al., 2013; Coghill et al., 2014; Hervas et al., 2014; Huss et al., 2016; Soutullo et al., 2013). In the LDX study, the CHIP-CE:PRF Achievement domain was prespecified as the primary HRQoL outcome (Banaschewski et al., 2013); in the GXR study, the WFIRS-P Learning and School domain and Family domain were prespecified as key secondary efficacy outcomes. Safety was assessed as previously described (Coghill et al., 2013; Hervas et al., 2014).
Investigators completed the ADHD-RS-IV at baseline and at each weekly study visit in the double-blind period of both studies, based on all available information at each assessment. Participants’ parents (or legally authorized representatives) completed the CHIP-CE:PRF and WFIRS-P at baseline, Week 4 (for participants enrolled after a protocol amendment), Week 7, and/or at early termination in the LDX study. Participants’ parents (or legally authorized representative) completed the WFIRS-P at baseline, Week 4, Week 7, Week 10, Week 13 (for adolescents only), and/or at early termination in the GXR study (Banaschewski et al., 2013; Hervas et al., 2014).
Prespecified Statistical Analyses
In both studies, efficacy analyses were based on the full analysis set, defined as participants who were randomized and took at least one dose of study drug. The full analysis set in the LDX study excluded 15 patients from one site where there were violations of good clinical practice; and the full analysis set in the GXR study excluded one patient who was randomized to GXR but was lost to follow-up before receiving treatment (Coghill et al., 2013; Hervas et al., 2014). The “last observation carried forward” approach to missing data was used in both studies for all outcome measures (Banaschewski et al., 2013; Coghill et al., 2013; Hervas et al., 2014). The methods for determining sample sizes have been previously described (Coghill et al., 2013; Hervas et al., 2014). Prespecified analyses used ANCOVA models of the difference in least squares (LS) mean changes from baseline for each study treatment group compared with placebo (α = .05) in ADHD-RS-IV and WFIRS-P scores in both studies and also for CHIP-CE:PRF T-scores in the LDX study (Banaschewski et al., 2013; Coghill et al., 2013; Hervas et al., 2014). Effect sizes were calculated as the difference in LS means between each active drug and placebo, divided by the root mean square error from the ANCOVA models. Effect sizes calculated using this method are similar to Cohen’s d and are conventionally interpreted as large (>0.8), medium (0.5-<0.8), or small (0.2-<0.5; Cohen, 1992).
Both studies used a prespecified hierarchical testing algorithm to control Type I error. The primary efficacy outcome was tested first, followed in rank order by each key secondary outcome. Statistical significance was only declared for an outcome if the p value was below .05 and the previous outcome in the algorithm was also declared significant. This means that p values below .05 reported in this article are statistically significant only for the primary efficacy outcome and the key HRQoL outcome in the LDX group of SPD489-325 (change from baseline to endpoint in ADHD-RS-IV total score and CHIP-CE:PRF Achievement domain T-score, respectively) and for the primary efficacy outcome and key secondary efficacy outcomes in the GXR group of SPD503-316 (change from baseline to endpoint in ADHD-RS-IV total score and WFIRS-P Learning and School domain and Family domain scores, respectively). Analyses of all other outcomes were not included in the hierarchical testing algorithm, so they are not controlled for multiplicity and their associated p values are descriptive and noninferential.
Post Hoc Statistical Analyses
Pearson correlation coefficients (r) were calculated post hoc for the change in scores from baseline to endpoint in the following: ADHD-RS-IV total score versus T-scores in each of the five CHIP-CE:PRF domains (in the LDX study only), ADHD-RS-IV total score versus WFIRS-P total score and scores in each of the six WFIRS-P domains (in both studies), and T-scores in each of the five CHIP-CE:PRF domains versus WFIRS-P total score and in scores in each of the six WFIRS-P domains (in the LDX study only). Data for each treatment group were analyzed separately (results for the placebo group are not reported). Values of r were not compared statistically with one another across instruments, domains, or treatment groups. These exploratory analyses were not corrected for multiple comparisons, and p values are descriptive and noninferential. Pearson’s r is a measure of the strength of a positive or negative linear relationship between paired data, and may be interpreted as indicating very weak (r < .2), weak (.2-<.4), moderate (.4-<.6), strong (.6-<.8), or very strong (.8-<1.0) correlations (Evans, 1996).
Results
Participant Characteristics and Disposition
In the LDX study (Banaschewski et al., 2013; Coghill et al., 2013), 336 participants were randomized and 317 were included in the full analysis set, of whom 77/104, 42/106, and 72/107 in the LDX, placebo, and OROS-MPH groups, respectively, completed the study. The principal reason for study discontinuation was lack of efficacy. Baseline demographics and disease characteristics were similar across treatment groups. The mean age of participants in the full analysis set was 10.9 years (SD = 2.70), and 72.2% were children aged 6 to 12 years.
In the GXR study (Hervas et al., 2014), 338 participants were randomized and 337 were included in the full analysis set, of whom 91/114, 89/112, and 92/111 in the GXR, placebo, and ATX groups, respectively, completed the double-blind period of the study. Of the 338 randomized participants, 77.5% were enrolled in Europe. The principal reason for study discontinuation was lack of efficacy. Baseline demographics and disease characteristics were similar across treatment groups. The mean age of participants in the full analysis set was 10.8 years (SD = 2.77), and 71.8% were children aged 6 to 12 years.
ADHD-RS-IV, CHIP-CE:PRF, and WFIRS-P Outcomes: Change From Baseline to Endpoint
In the LDX study, mean improvements in ADHD-RS-IV total score from baseline to endpoint were significantly greater for LDX and the OROS-MPH reference treatment than for placebo, with effect sizes of 1.80 and 1.26, respectively (Table 1; Coghill et al., 2013). Improvements in CHIP-CE:PRF T-scores were significantly greater for LDX and OROS-MPH than for placebo in four of the five domains, with large effect sizes in Achievement and Risk Avoidance, small effect sizes in Resilience and Satisfaction, and no significant effect in Comfort (Table 1; Banaschewski et al., 2013). Improvement in WFIRS-P total score was significantly greater for LDX and OROS-MPH than for placebo, with a large effect size for LDX and a medium effect size for OROS-MPH. In four of the six WFIRS-P domains, improvements were significantly greater for LDX and OROS-MPH than for placebo: Learning and School (large effect sizes for both treatments), Family and Social Activities (medium effect sizes for both treatments), and Risky Activities (medium effect size for LDX, small effect size for OROS-MPH; Table 1). OROS-MPH also had a significantly greater effect than placebo in Life Skills and Child’s Self-Concept, with small effect sizes (Banaschewski et al., 2013).
Summary of Efficacy Outcomes in the LDX Study (SPD489-325).
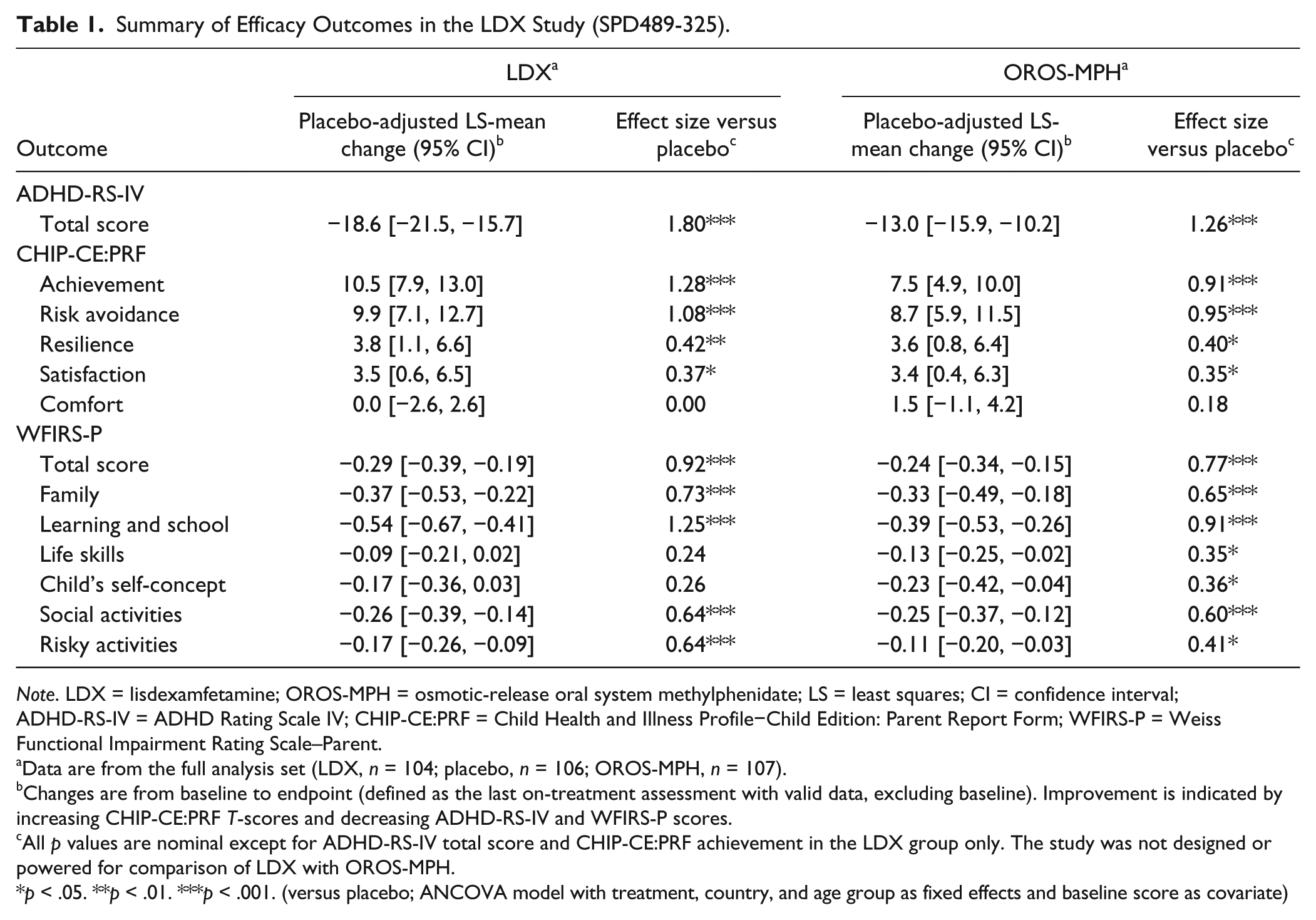
Note. LDX = lisdexamfetamine; OROS-MPH = osmotic-release oral system methylphenidate; LS = least squares; CI = confidence interval; ADHD-RS-IV = ADHD Rating Scale IV; CHIP-CE:PRF = Child Health and Illness Profile−Child Edition: Parent Report Form; WFIRS-P = Weiss Functional Impairment Rating Scale–Parent.
Data are from the full analysis set (LDX, n = 104; placebo, n = 106; OROS-MPH, n = 107).
Changes are from baseline to endpoint (defined as the last on-treatment assessment with valid data, excluding baseline). Improvement is indicated by increasing CHIP-CE:PRF T-scores and decreasing ADHD-RS-IV and WFIRS-P scores.
All p values are nominal except for ADHD-RS-IV total score and CHIP-CE:PRF achievement in the LDX group only. The study was not designed or powered for comparison of LDX with OROS-MPH.
p < .05. **p < .01. ***p < .001. (versus placebo; ANCOVA model with treatment, country, and age group as fixed effects and baseline score as covariate)
In the GXR study, mean improvements in ADHD-RS-IV total score from baseline to endpoint were significantly greater for GXR and the ATX reference treatment than for placebo, with effect sizes of 0.76 and 0.32, respectively (Table 2; Hervas et al., 2014). Improvements in WFIRS-P total score were significantly greater for GXR and ATX than for placebo, with small effect sizes. In the six WFIRS-P domains, improvements were significantly greater for GXR and ATX than for placebo in Learning and School, with small effect sizes, and for GXR only in Family and Social Activities, with small effect sizes (Table 2; Hervas et al., 2014).
Summary of Efficacy Outcomes in the GXR Study (SPD503-316).
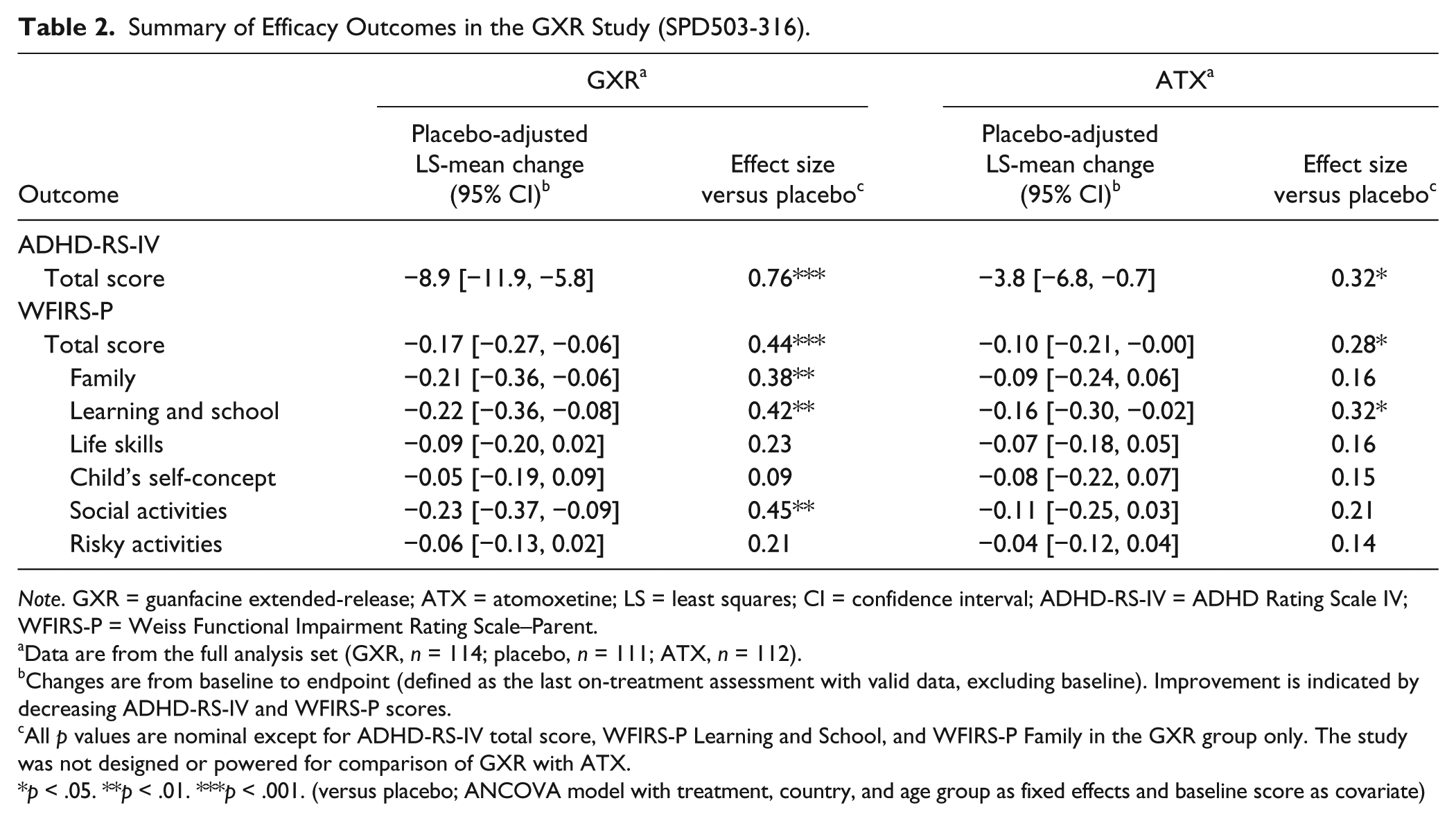
Note. GXR = guanfacine extended-release; ATX = atomoxetine; LS = least squares; CI = confidence interval; ADHD-RS-IV = ADHD Rating Scale IV; WFIRS-P = Weiss Functional Impairment Rating Scale–Parent.
Data are from the full analysis set (GXR, n = 114; placebo, n = 111; ATX, n = 112).
Changes are from baseline to endpoint (defined as the last on-treatment assessment with valid data, excluding baseline). Improvement is indicated by decreasing ADHD-RS-IV and WFIRS-P scores.
All p values are nominal except for ADHD-RS-IV total score, WFIRS-P Learning and School, and WFIRS-P Family in the GXR group only. The study was not designed or powered for comparison of GXR with ATX.
p < .05. **p < .01. ***p < .001. (versus placebo; ANCOVA model with treatment, country, and age group as fixed effects and baseline score as covariate)
Correlation of Change in ADHD-RS-IV Score With Change in CHIP-CE:PRF T-Scores
In the LDX and OROS-MPH groups, changes in ADHD-RS-IV total score from baseline to endpoint in SPD489-325 correlated most moderately with changes in CHIP-CE:PRF domain T-scores (Figure 1). The strongest nominally significant correlations for both active treatments were with changes in the Risk Avoidance domain (LDX, r = −.44; OROS-MPH, r = −.42) and the Achievement domain (LDX, r = −.36; OROS-MPH r = −.48). For changes in the remaining three domains, correlations were weak but significant for both active treatments in Satisfaction and Comfort and for LDX in Resilience, and were very weak and not significant for OROS-MPH in Resilience (Figure 1).
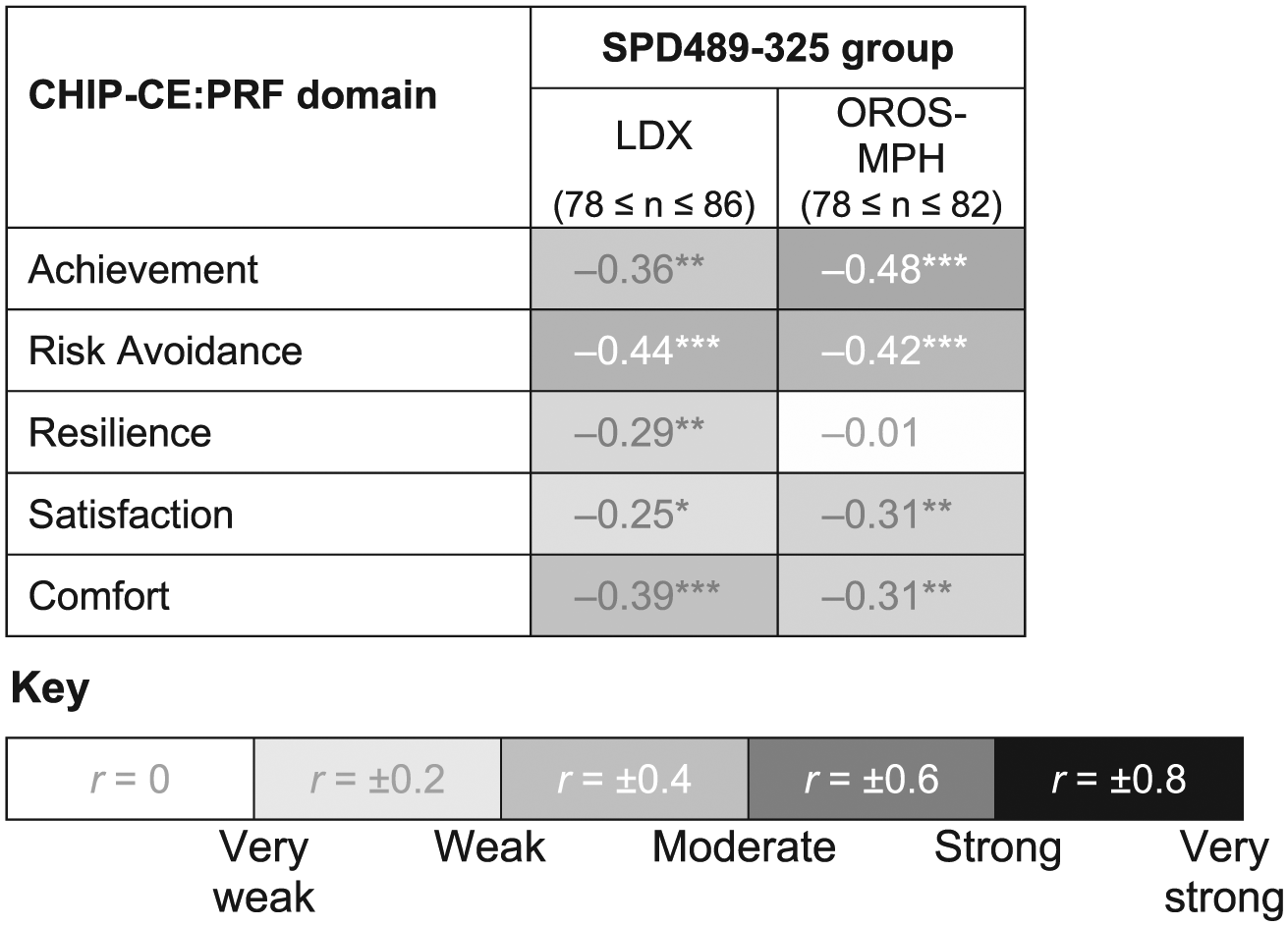
Pearson correlation coefficients for change in ADHD-RS-IV total score versus change in CHIP-CE:PRF T-score in the LDX study (SPD489-325).
Correlation of Change in ADHD-RS-IV Score With Change in WFIRS-P Scores
Changes in ADHD-RS-IV total score from baseline to endpoint correlated moderately and nominally significantly with changes in WFIRS-P total score in the LDX and OROS-MPH groups in SPD489-325 and the GXR group in SPD503-316, with r values of .51, .49, and .56, respectively (Figure 2). The correlation of change in ADHD-RS-IV with change in WFIRS-P total score was weak but nominally significant in the ATX group (r = .38). In the WFIRS-P domains, correlations of change in all six domains with change in ADHD-RS-IV total score were nominally significant, and were strongest for the Family domain in the LDX and OROS-MPH groups of SDP489-325 and the GXR group of SPD503-316 (r > .5). Moderate correlations with change in ADHD-RS-IV total score were also observed for changes in Learning and School and Risky Activities (LDX group and GXR group only) and Child’s Self-Concept and Social Activities (GXR group only) domain scores. All other correlations were weak but nominally significant (including all domains in the ATX group).
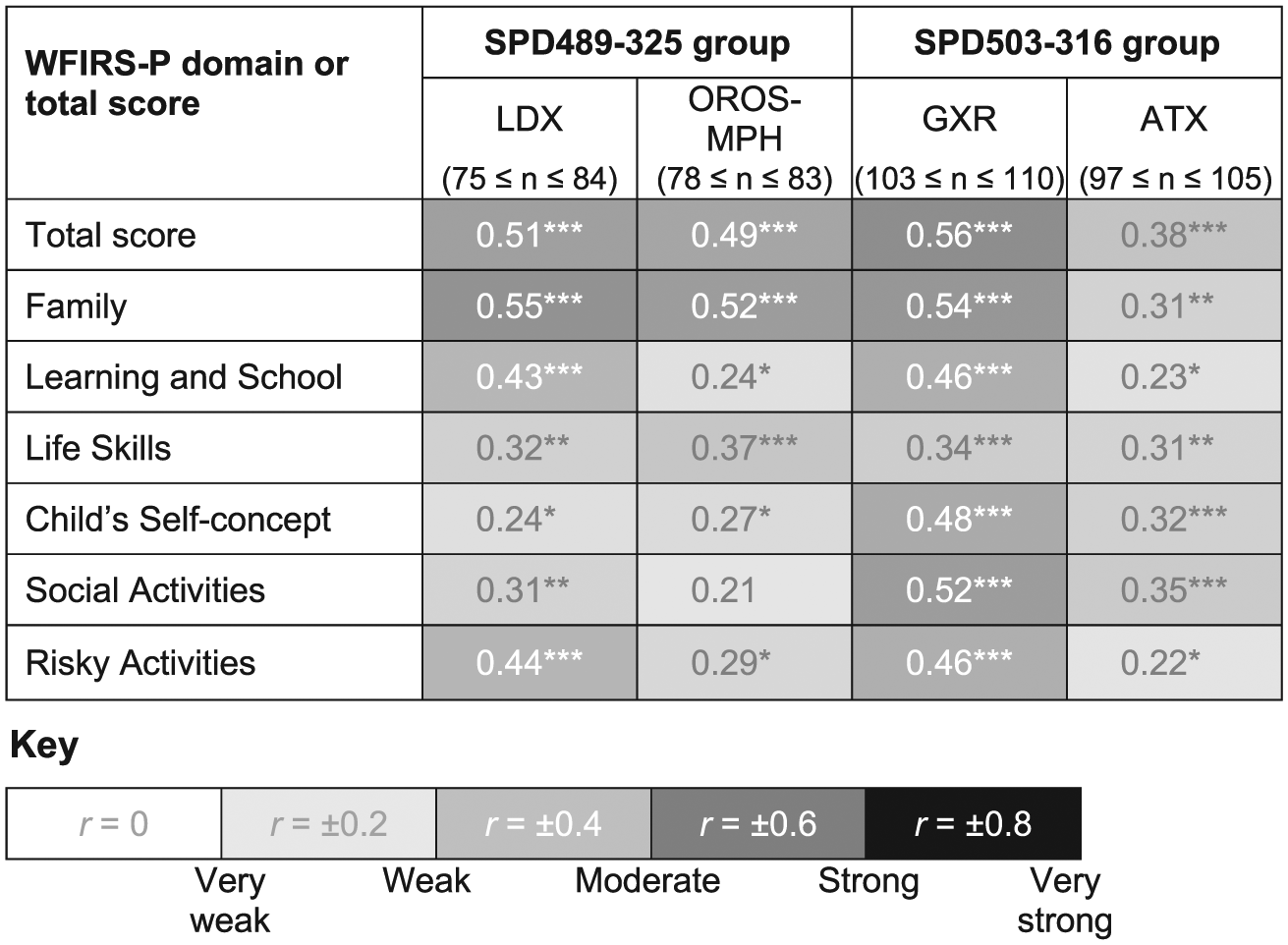
Pearson correlation coefficients for change in ADHD-RS-IV total score versus change in WFIRS-P total and domain scores in studies SPD489-325 and SPD503-316.
Correlation of CHIP-CE:PRF Outcomes With WFIRS-P Outcomes
Changes in CHIP-CE:PRF Achievement domain and Risk Avoidance domain T-scores correlated strongly and nominally significantly with changes in WFIRS-P total score in the active treatment groups of study SPD489-325, with r values of −.65 and −.62 in the LDX group and −.59 and −.62 in the OROS-MPH group, respectively (Figure 3). Nominally significant correlations with change in WFIRS-P total score were moderate for changes in the remaining CHIP-CE:PRF domains of Satisfaction (LDX, r = −.50; OROS-MPH, r = −.44), and weak to moderate for Resilience and Comfort (LDX, r = −.37 and −.42; OROS-MPH, r = −.24 and −.33, respectively).
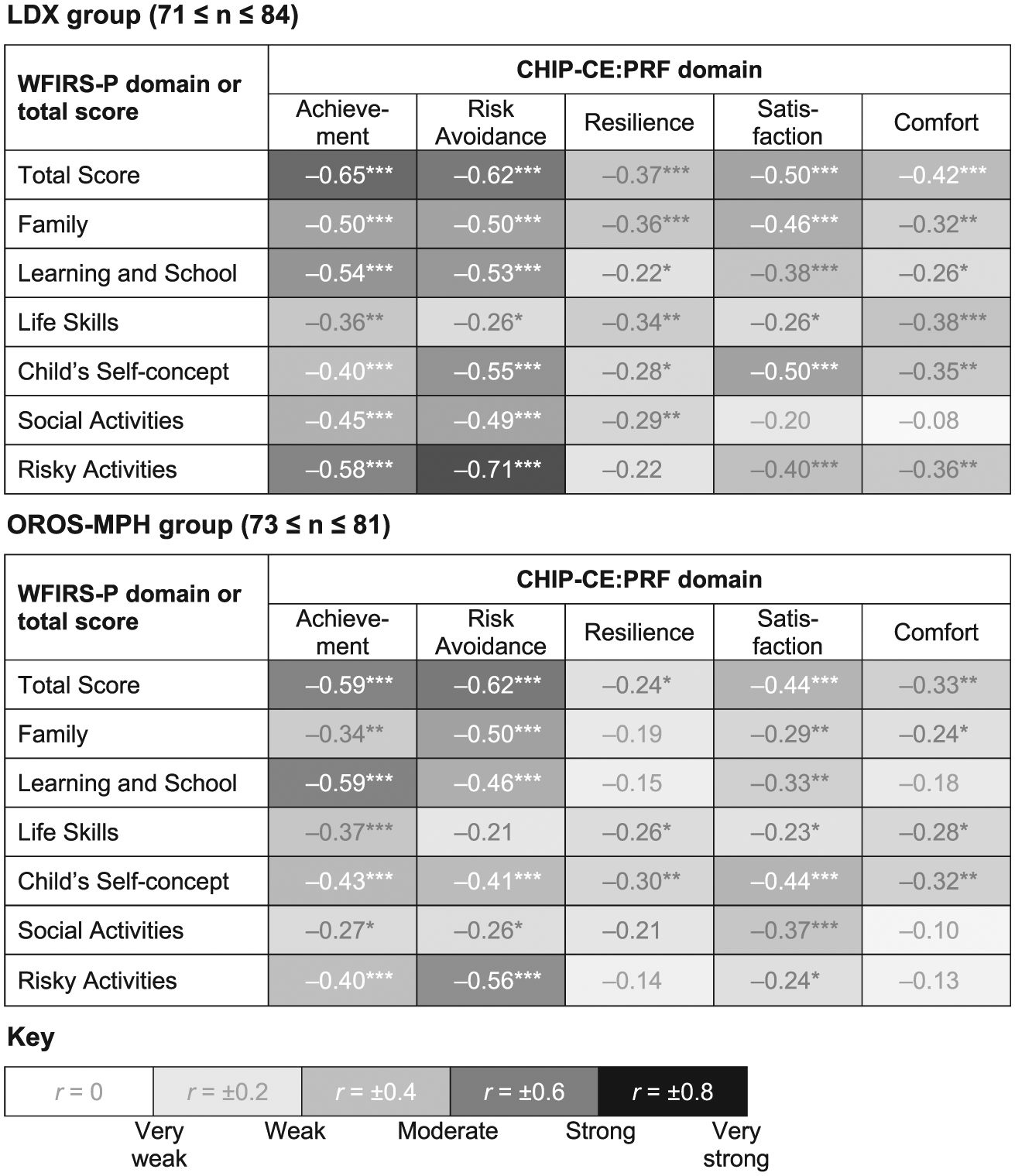
Pearson correlation coefficients for change in WFIRS-P scores versus change in CHIP-CE:PRF T-scores in study SPD489-325 in the LDX and OROS-MPH groups.
In pairwise correlations of change in the five CHIP-CE:PRF domains with change in each of the six WFIRS-P domains (Figure 3), change in CHIP-CE:PRF Risk Avoidance correlated most strongly with change in WFIRS-P Risky Activities (LDX, r = −.71; OROS-MPH, r = −.56), but also moderately and nominally significantly with change in Family, Learning and School, and Child’s Self-Concept in both groups (LDX, r = −.50, −.53, and −.55; OROS-MPH, r = −.50, −.46, and −.41, respectively) and Social Activities in the LDX group (r = −.49). Change in CHIP-CE:PRF Achievement correlated most strongly with change in WFIRS-P Learning and School (LDX, r = −.54; OROS-MPH, r = −.59) and Risky Activities (LDX, r = −.58; OROS-MPH, r = −.40), but also moderately and nominally significantly with change in Family and Social Activities in the LDX group (r = −.50 and −.45, respectively) and Child’s Self-Concept in both groups (LDX, r = −.40; OROS-MPH, r = −.43). Changes in CHIP-CE:PRF Resilience, Satisfaction, and Comfort correlated weakly or very weakly with changes in the WFIRS-P domains, except for the moderate correlations of change in CHIP-CE:PRF Satisfaction with change in WFIRS-P Child’s Self-Concept in both groups (LDX, r = −.50; OROS-MPH, r = −.44) and with WFIRS-P Family in the LDX group (r = −.46; Figure 3)
Discussion
These post hoc analyses investigated the associations between different symptom-based and non-symptom-based outcomes in two recent clinical trials involving four different medications in children and adolescents with ADHD. The results are consistent with the hypothesis that the ADHD-RS-IV, CHIP-CE:PRF, and WFIRS-P instruments assess partially intersecting but distinct aspects of the response to pharmacological treatment. Changes in CHIP-CE:PRF and WFIRS-P scores correlated significantly, but at most moderately, with changes in ADHD-RS-IV total score (r weaker than ± .6); the strongest relationships were with the CHIP-CE:PRF Achievement and Risk Avoidance domains (r in the range −.36 to −.48) and the WFIRS-P total score and Family domain (r in the range .31-.56). Correlations of the CHIP-CE:PRF Achievement and Risk Avoidance domains with WFIRS-P total score were stronger than those of either instrument with the ADHD-RS-IV, but were still generally only of moderate strength (r in the range −.59 to −.65 for WFIRS-P). These results suggest not only that control of ADHD symptoms was associated with improved functioning and HRQoL in children and adolescents with ADHD in these studies, but also that the symptom-based scale may not have captured a complete picture of the treatment response. From a clinical perspective, this conclusion indicates that a focus on monitoring improvements in ADHD symptoms during treatment remains important, but that reliance solely on assessment of patients’ symptoms may fail to recognize continuing problems with functioning and HRQoL that require additional support.
Many interventional and observational studies in children and adolescents with ADHD have included the CHIP-CE:PRF as an outcome measure (Banaschewski et al., 2014; Banaschewski et al., 2013; Coghill & Hodgkins, 2016; Dell’Agnello et al., 2009; Escobar et al., 2009; Escobar et al., 2010; Hodgkins et al., 2017; Prasad et al., 2007; Preuss et al., 2006; Riley, Spiel, et al., 2006; Svanborg et al., 2009). As a generic HRQoL instrument, the CHIP-CE:PRF contains some items that are likely to be adversely affected by ADHD (e.g., academic performance) and other items that are not (e.g., physical activities). In clinical studies, the largest placebo-adjusted effect sizes of stimulant medications and ATX in children and adolescents with ADHD are seen in the CHIP-CE:PRF domains with the most pronounced baseline HRQoL deficits, namely, the Achievement and Risk Avoidance domains (Banaschewski et al., 2014; Banaschewski et al., 2013; Coghill & Hodgkins, 2016; Escobar et al., 2010; Riley, Spiel, et al., 2006). In the present analyses, changes in these domains inversely correlated most strongly with changes in ADHD-RS-IV symptom scores in the LDX and OROS-MPH groups of study SPD489-325, consistent with the results of similar analyses of other studies (Coghill & Hodgkins, 2016; Escobar et al., 2010; Riley, Coghill, et al., 2006). The large placebo-adjusted effect sizes of LDX and OROS-MPH in these CHIP-CE:PRF domains were nearly as large as they were for the ADHD-RS-IV outcome (Table 1). LDX and OROS-MPH also had small but nominally significant placebo-adjusted effect sizes in the CHIP-CE:PRF domains of Resilience and Satisfaction, but not Comfort (Table 1); yet these three domains all correlated weakly with ADHD-RS-IV, with weaker correlations in Resilience and Satisfaction than in Comfort (Figure 1). Taken together, these findings suggest that stimulant medications could have a proximal effect on HRQoL in domains where the impact of ADHD is both strong and direct (Achievement and Risk Avoidance), a more distal effect in domains where the impact is less strong and seems likely to occur via a less direct pathway (Resilience and Satisfaction), and little or no effect in domains that are hardly affected all by ADHD (Comfort).
The WFIRS-P has been less extensively used in studies in children and adolescents with ADHD than the CHIP-CE:PRF (Banaschewski et al., 2014; Banaschewski et al., 2013; Hervas et al., 2014; Hodgkins et al., 2017; Maziade et al., 2009; Nagy et al., 2016; Stein et al., 2015; Wilens et al., 2015). Unlike the CHIP-CE:PRF, the WFIRS-P was designed to focus on areas of impairment that are most problematic in patients with ADHD. This means that all six WFIRS-P domains contain items deemed to be characteristic of ADHD and that may represent important treatment targets (although these are not necessarily unique to ADHD). The design of the WFIRS-P is such that children and adolescents with ADHD may therefore have severe and clinically significant impairments in only a small number of salient WFIRS-P items. Furthermore, the lack of normative data means that the severity of baseline impairments and the magnitude of treatment-associated improvements in WFIRS-P domain scores cannot be interpreted in the same way as CHIP-CE:PRF domain T-scores. The absolute value of a mean WFIRS-P domain score does not necessarily reflect its clinical impact. For example, estimates of minimum difference that parents perceive as important are larger for the WFIRS-P Learning and School domain and Family domain than for the Risky Activities domain (Hodgkins et al., 2017). Despite these considerations, mean baseline WFIRS-P scores in children and adolescents with ADHD tend to indicate greater impairment in the Family domain and the Learning and School domain than in the other domains (Banaschewski et al., 2014; Banaschewski et al., 2013; Hervas et al., 2014; Hodgkins et al., 2017; Nagy et al., 2016; Stein et al., 2015; Wilens et al., 2015). In SPD489-325, placebo-adjusted effect sizes of LDX and OROS-MPH were largest in these domains, and changes in the same domains (plus Risky Activities) correlated most strongly with ADHD-RS-IV changes, in agreement with the results of previous studies (Gajria et al., 2015; Stein et al., 2015; Tarakcioglu et al., 2015). In contrast, in the GXR group of SPD503-316, placebo-adjusted effect sizes were largest in the Social Activities and Learning and School domains, and changes in the same domains (plus Family) correlated most strongly with ADHD-RS-IV changes. This possible difference between GXR and stimulants in the two studies may have multiple potential explanations. First, participants’ disease severity and characteristics, including types of functional impairment, may differ between studies of stimulants and nonstimulants. Second, the effects of different medications, with different modes of action and pharmacodynamic profiles, may vary over time and across domains of functional impairment. Third, patients may experience functional improvement in different parent-reported questionnaire items, which may vary in the proximity of their relationship to improvement in ADHD symptoms. Further studies would be needed to investigate whether particular medications are more or less suitable for patients with particular functional impairments.
In pairwise correlations of treatment-associated changes in study SPD489-325, each of the five CHIP-CE:PRF domains did not generally correspond to any particular WFIRS-P domain. Although CHIP-CE:PRF Risk Avoidance inversely correlated moderately to strongly with WFIRS-P Risky Activities, the CHIP-CE:PRF Achievement and Risk Avoidance domains inversely correlated at least moderately with all of the WFIRS-P domains except Life Skills. For the remaining three CHIP-CE:PRF domains, correlations with WFIRS-P domains were generally weak, except for CHIP-CE:PRF Satisfaction with WFIRS-P Child’s Self-Concept. These results provide further indications that the CHIP-CE:PRF Achievement and Risk Avoidance domains may be more proximally related to ADHD than the other domains. In contrast, a wider range of WFIRS-P domains than CHIP-CE:PRF domains may be proximally related to ADHD, possibly because the disorder may be expressed as particular types of parent-rated functional impairment in each individual child or adolescent. However, the WFIRS-P Child’s Self-Concept domain may be more distally related to ADHD than other domains.
In clinical trials, parent-rated HRQoL questionnaires like the CHIP-CE:PRF are used rather than self-rated questionnaires because children aged below 10 to 12 years may lack the conceptual grasp to evaluate their HRQoL accurately. This involves judgment of the extent to which ill-health affects their “perception of their position in life, in the context of culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns,” according to the World Health Organization definition of quality of life (World Health Organization, 1995, p. 1403). If HRQoL is narrowly defined as being perceptible only by individuals themselves, then the parent-rated CHIP-CE:PRF might be considered more as a measure of functional impairments than of HRQoL. Scores on self-rated HRQoL instruments have been reported to correlate significantly but only weakly to moderately with scores on parent-rated HRQoL instruments, including comparisons of the self-rated CHIP-CE: Self-Report Form (CHIP-CE:SRF) with the CHIP-CE:PRF (Coghill & Hodgkins, 2016; Estrada et al., 2010). In the present study, using parent-rated instruments, changes in CHIP-CE:PRF correlated more strongly, but far from perfectly, with WFIRS-P changes than with ADHD-RS-IV changes. This suggests that the CHIP-CE:PRF and WFIRS-P do capture different conceptual aspects of the difficulties faced by children and adolescents with ADHD, even though the CHIP-CE:PRF does not necessarily capture their own views. Furthermore, the imperfect correlation observed between the CHIP-CE:PRF and WFIRS-P instruments is consistent with the possibility that poor HRQoL in children and adolescents with ADHD may arise from their functional impairment as well as from their ADHD symptoms.
The strengths and weaknesses of the present post hoc analyses include those of the two published studies on which they were based (Banaschewski et al., 2013; Coghill et al., 2013; Hervas et al., 2014). One of the main limitations of the present analyses is the inclusion of the CHIP-CE:PRF in the LDX study but not the GXR study. Also, both included studies were short-term trials, and did not collect data on potential functional or HRQoL improvements beyond the end of the study. Improvements in some domains of functional impairment or HRQoL may develop or become apparent over a longer period of time than the double-blind treatment period of these short-term Phase 3 studies, especially if some domains are more distally related to ADHD symptoms than others. However, in an extension to the LDX study, most of the improvement in participants’ CHIP-CE:PRF and WFIRS-P scores occurred during the first 8 weeks of a 6-month open-label LDX treatment period (Banaschewski et al., 2014) and continued treatment was required to maintain CHIP-CE:PRF and WFIRS-P improvements with LDX and to maintain WFIRS-P improvements with GXR in long-term randomized-withdrawal studies (Banaschewski et al., 2014; Newcorn et al., 2016). Another limitation is that the entry criteria of the two studies did not require participants to have functional impairments or HRQoL deficits, although evidence of functional impairments is essential for the diagnosis of ADHD. In contrast, ADHD symptoms of at least moderate severity were required for entry in both studies (in addition to an ADHD diagnosis). As a result, the variance in ADHD-RS-IV total scores at baseline may have been constrained by the requirement for a minimum score at study entry. For this reason, we did not correlate baseline ADHD-RS-IV scores with baseline CHIP-CE:PRF or WFIRS-P scores. Another limitation of the present analyses is that the ADHD-RS-IV was completed by investigators, but that the CHIP-CE:PRF and WFIRS-P were completed by parents. Different results may have been obtained with a parent-rated ADHD symptom instrument. Finally, the present analyses were confined to two clinical trials and did not include other studies that have used the CHIP-CE:PRF and WFIRS-P in patients with ADHD.
A strength of the present correlational analyses is the focus on changes during treatment rather than baseline impairments. However, the inclusion criteria may also have allowed greater scope for change in the primary efficacy outcome measure than in secondary efficacy outcome measures. The treatment groups were not pooled for these correlative analyses. This approach might have increased statistical power, but would not have allowed possible treatment-specific effects to be discerned. Results for the placebo groups in the present analyses are not reported because correlation coefficients were low, presumably due to the smaller changes in scores on outcome measures than those observed in the active treatment groups. Although placebo-adjusted effect sizes of ATX in SPD503-316 were similar to those reported in other studies (Cheng et al., 2007; Escobar et al., 2010), the magnitude of changes and the number of participants may also not have been large enough to enable relationships between outcomes to be assessed adequately. We did not test statistically whether values of Pearson’s r differed from one another, so conclusions about differences in the strength of relationships between outcomes and treatment groups remain suggestive. Finally, the analyses were not corrected for multiplicity, so p values should be interpreted as descriptive, not inferential.
The present study suggests potential areas for future research. In particular, a study investigating the relationship between parent-rated symptom outcomes with parent-rated functional impairment and HRQoL outcomes may provide further insight into the relationships between these constructs in children with ADHD. Similarly, an investigation of the relationship between patient-rated symptoms and functional impairment or HRQoL may provide further insight into the relationships between these constructs in adolescents or adults with ADHD. Finally, the question of whether particular medications may have similar efficacy in providing symptomatic relief but subtly different effects in particular domains of functional impairment or HRQoL remains to be investigated.
In conclusion, the findings of these post hoc analyses suggest that relief of ADHD symptoms during short-term treatment with ADHD medication is generally associated with reduced functional impairments and improved HRQoL. This should provide further incentive for physicians to aim for optimal control of ADHD symptoms with a well-tolerated medication. At the same time, these findings also suggest that factors other than reductions in ADHD symptom scores also influence improvements in functioning and HRQoL. This should encourage physicians to explore potential benefits of therapeutic interventions that fall outside of those captured by conventional ADHD symptom scales. Finally, the findings also support the inclusion of functional impairment and HRQoL measures as outcomes of clinical trials in patients with ADHD and highlight the need for further development and improved understanding of the available instruments, on the grounds that they do appear to sample different, but partially intersecting, aspects of the treatment response, beyond relief of ADHD symptoms.
Footnotes
Acknowledgements
We thank the participants and investigators involved in both studies. We thank Antonia Panayi of Shire International GmbH for her contribution to discussions of this work. Under the direction of the authors, and funded by Shire International GmbH, Dr. M. G. Cottingham of Oxford PharmaGenesis provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy editing, and fact checking was also provided by Oxford PharmaGenesis. A Panayi from Shire International GmbH reviewed and edited the article for scientific accuracy. Although employees of the sponsor were involved in study design, data collection, analysis and interpretation, and fact checking of information, the content of this article, the interpretation of the data, and the decision to submit the article for publication in Journal of Attention Disorders were made by the authors independently.
Authors’ Note
Vanja Sikirica is currently at GlaxoSmithKline, Philadelphia, PA, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Shire develops and markets treatments for ADHD, including LDX and GXR. Alain Joseph and Caleb Bliss are employees of Shire and own stock or stock options. Vanja Sikirica is a former employee of Shire. Mark Kosinski is an employee of QualityMetric, which received funding from Shire for performing statistical analyses reported in this article. The following authors have received compensation for serving as consultants or speakers for, or they or the institutions they work for have received research support or royalties from, the companies or organizations indicated: David R. Coghill (Eli Lilly, Janssen-Cilag, Medice, Novartis, Oxford University Press, Shire, and Vifor Pharma); Michael Huss (Actelion, Eli Lilly, Engelhard Arzneimittel, Janssen-Cilag, Medice, Novartis, Shire, and Steiner Arzneimittel).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This post hoc analysis and the two original studies were funded by the sponsor, Shire Development LLC.